
The Effectiveness of Interventions Delivered Using Digital Food Environments to Encourage Healthy Food Choices: A Systematic Review and Meta-Analysis

 , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Selection Criteria
2.1.1. Types of Studies
2.1.2. Type of Participants
2.1.3. Types of Interventions
- The intervention was delivered primarily via an online food ordering system (i.e., >50% of the intervention strategies were delivered via the online food ordering system). Online food ordering systems of interest included (but were not limited to) online supermarkets and grocery stores, online restaurants, cafes and canteens; and online food and meal delivery services.
- The intervention aimed to encourage the purchase of healthier foods/beverages and/or reduce the purchase of less-healthy foods/beverages via strategies employed within the online food ordering platform.
- The intervention involved an actual online transaction, where money or equivalent (i.e., credit/voucher) was directly or indirectly (i.e., in the form of free or subsidized meal programs) exchanged for foods or beverages. This was to ensure that the consumer purchasing behaviors were generalizable to real-world contexts.
- Translating information: translating existing, decision-relevant information by changing the format or presentation of the information, but not the context.
- Making information visible: making external information, that is normally invisible, visible (e.g., daily calories allowances).
- Providing a social reference point: role modelling, or referring to the behavior of peer groups.
- Changing choice defaults: setting no-action defaults, or the use of prompted choice (e.g., nudge).
- Changing option related effort: changing the physical or financial effort to encourage or discourage certain choices.
- Changing the range or composition of options: changing categories or changing the grouping of options.
- Changing option consequences: changing the social consequences of certain decisions, or connecting decisions to benefits or costs (e.g., price promotions or discounts).
- Providing decision assistance: providing reminders, or facilitating commitment (e.g., self or public commitment).
2.1.4. Types of Comparison
2.1.5. Types of Outcomes
- The contents of food/beverage purchases according to food groups (e.g., servings of fruits and vegetables), food categories (e.g., the proportion of ‘healthy’ items and ‘less healthy’ items), or the presence of target items (e.g., sugar sweetened beverages).
- The macronutrient and micronutrient content of food/beverage purchases (e.g., mean energy, saturated fat, total sugar or sodium; or % energy contributed from fat or sugar; or energy density).
2.2. Search Strategy
2.3. Data Collection and Analysis
2.3.1. Selection of Studies
2.3.2. Data Extraction and Management
- Study characteristics: first author, publication year, country, study design, study aim, funding source and sample size.
- Participant characteristics: age, gender and ethnicity.
- Intervention characteristics: provider of the online food ordering platform, food ordering environment (e.g., school canteen, restaurant, or supermarket), intervention description, intervention strategies (as per Mȕnscher et al. [29] Choice architecture taxonomy), duration and intensity of the intervention.
- Outcome characteristics: definitions, methods of outcome assessment, and time points of outcome measurements.
- Study results relevant to the review primary outcome: e.g., food and beverage purchases/selection.
- Study results relevant to the review secondary outcomes: e.g., unintended adverse events, economic data/evaluation.
- Conflict of interest: using the Tool for Addressing Conflicts of Interest in Trials (https://tacit.one/, accessed on 7 August 2020).
2.3.3. Study Risk of Bias Assessment
2.3.4. Data Synthesis
3. Results
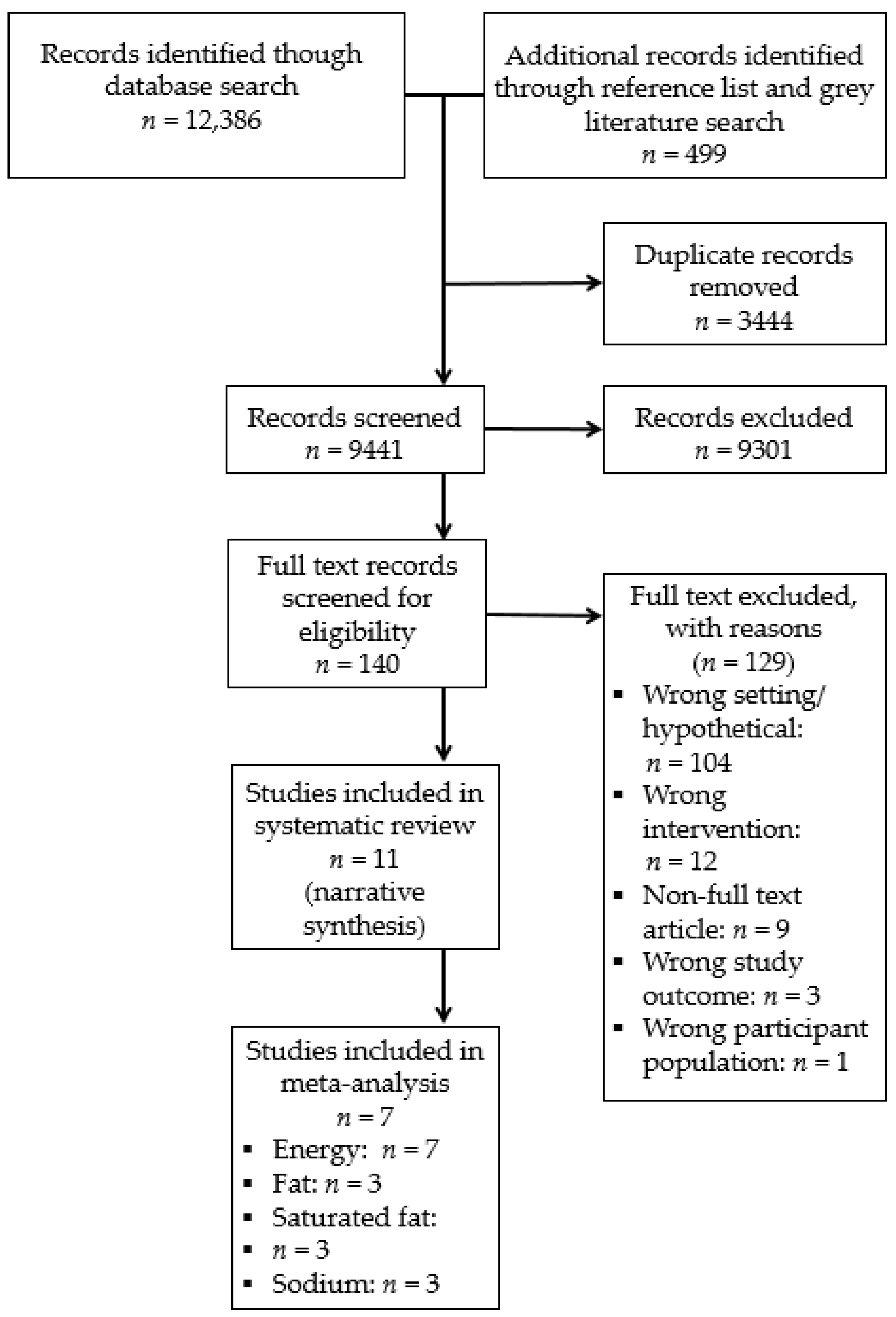
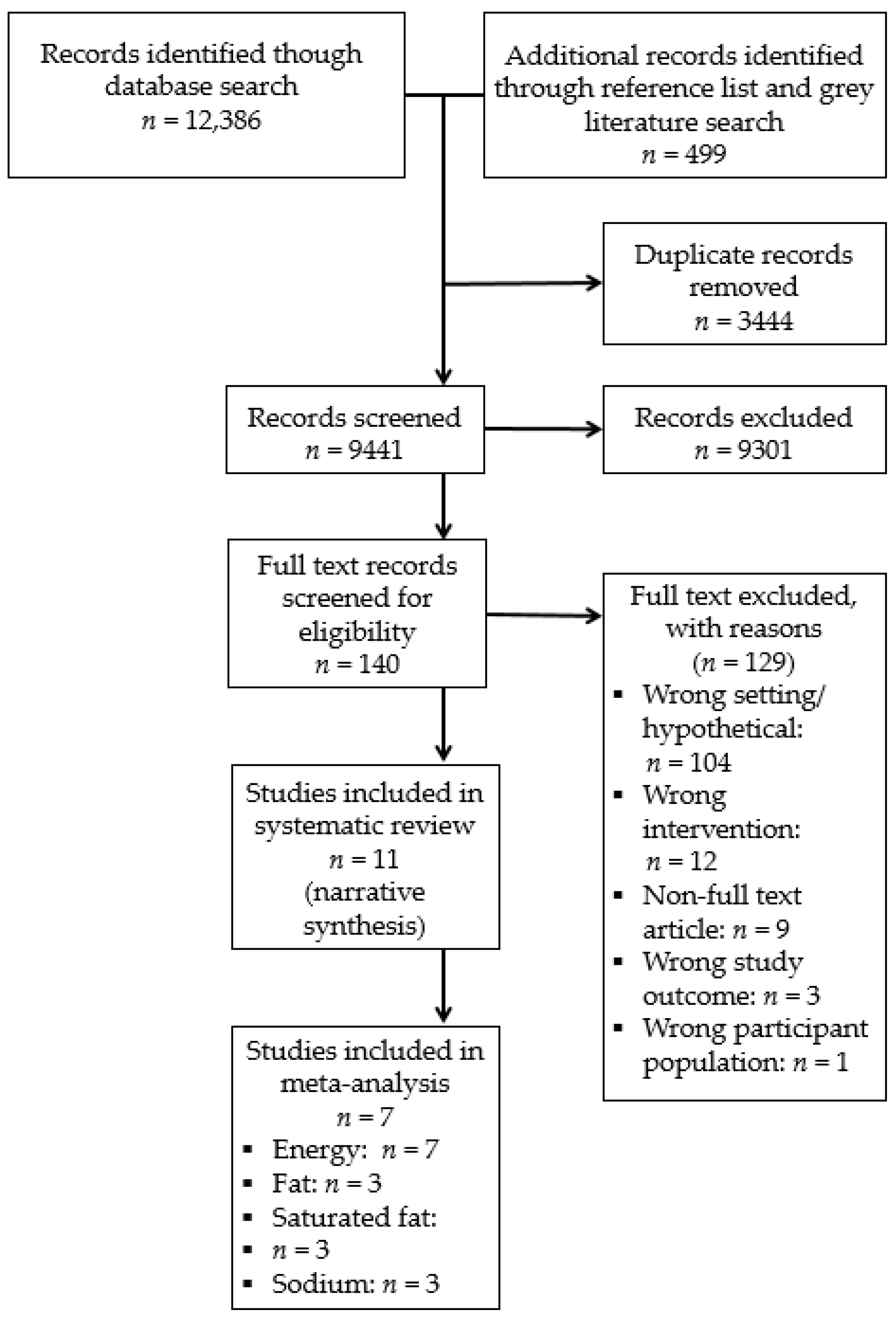
3.1. Study Selection
3.2. Study Characteristics
3.2.1. Design
3.2.2. Setting
3.2.3. Participants
3.2.4. Interventions
3.2.5. Comparison Group
3.2.6. Primary Outcomes
3.2.7. Secondary Outcomes
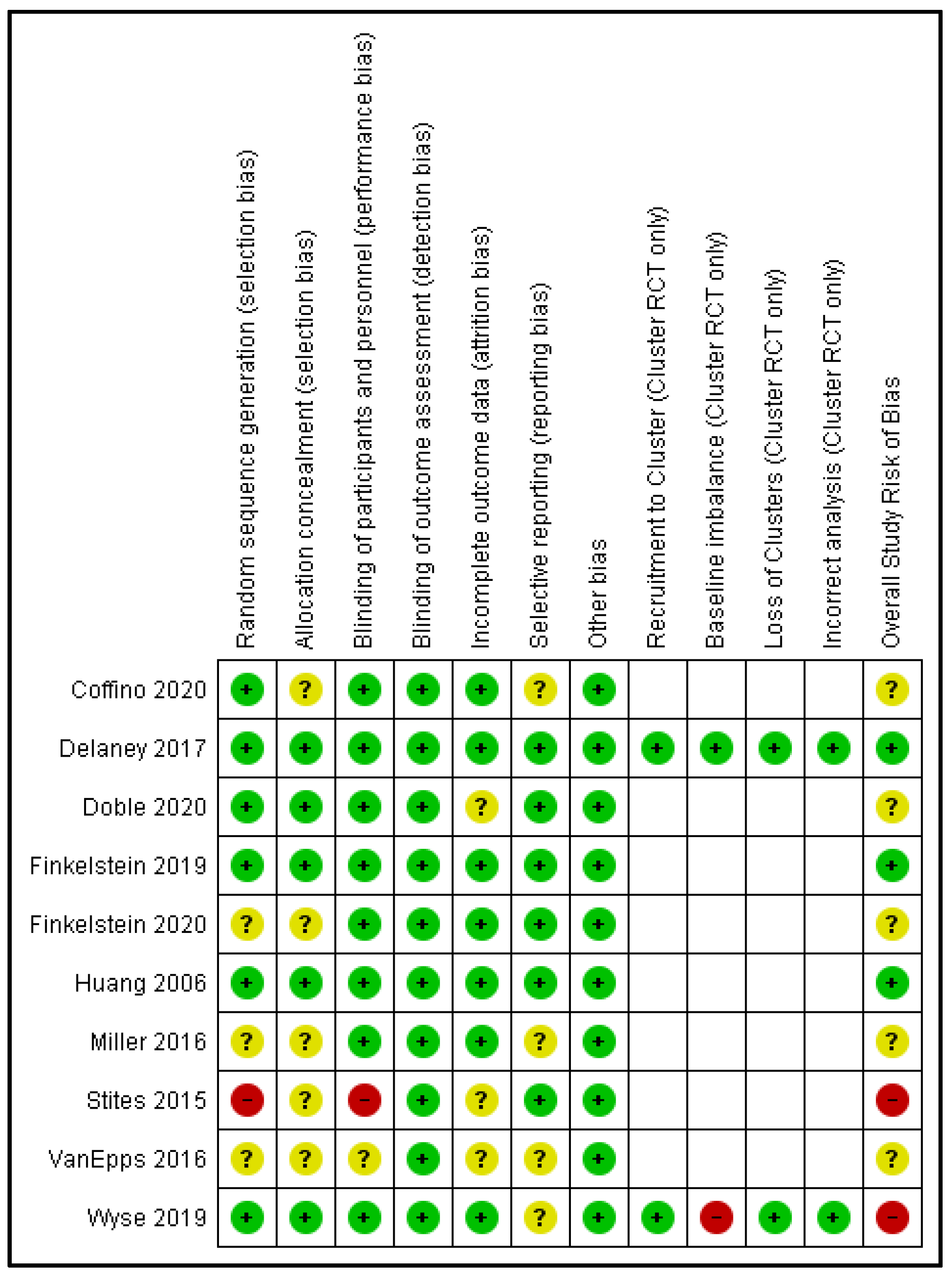
3.3. Risk of Bias
3.4. Intervention Effects: Meta-Analysis
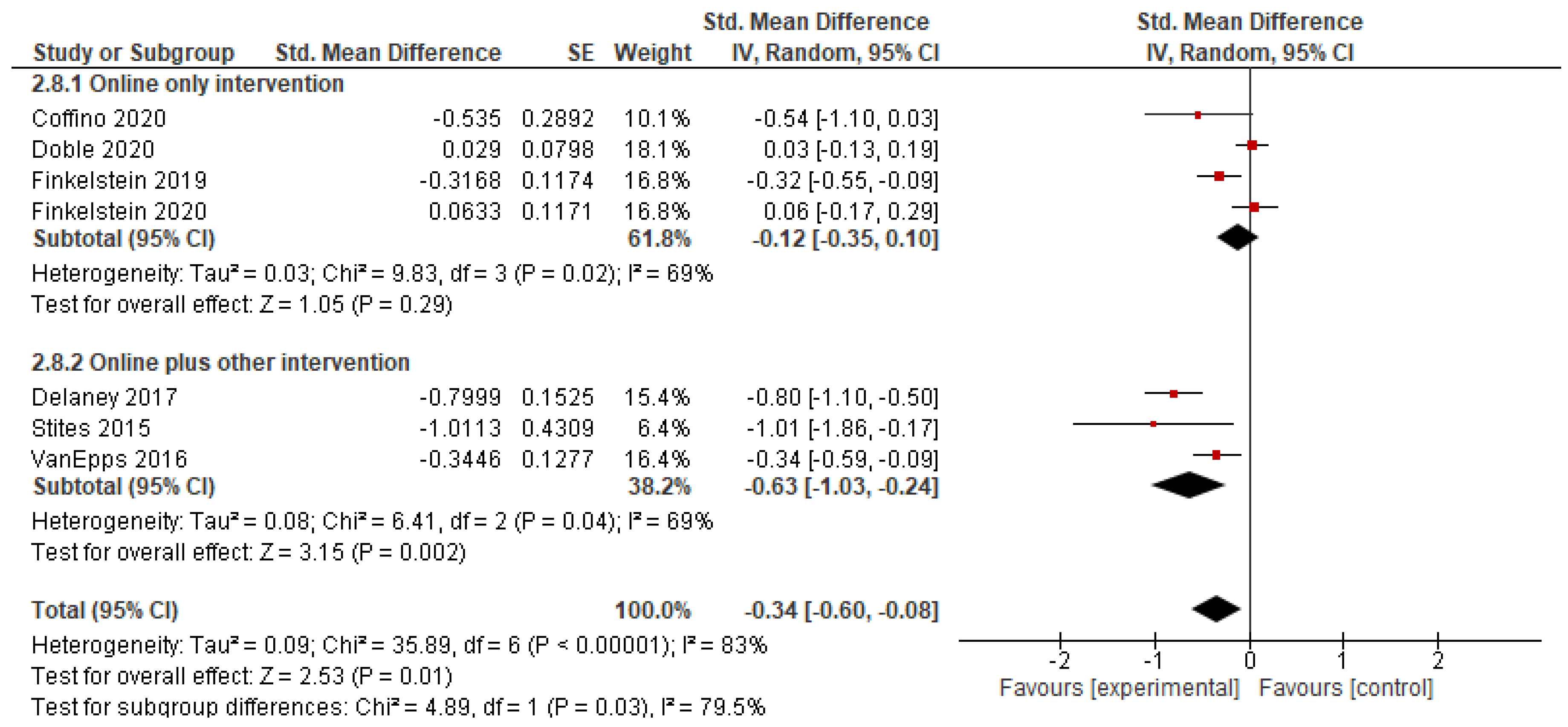
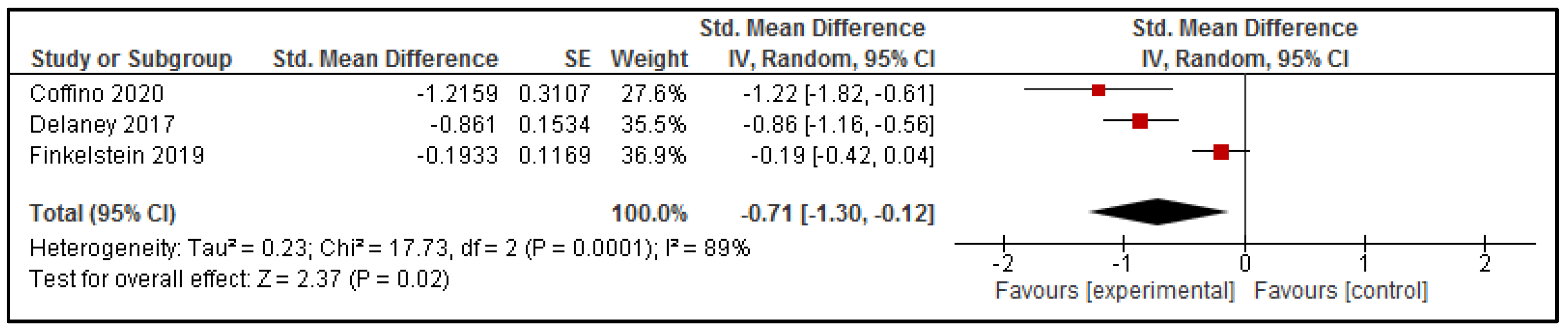
3.4.1. Energy Content of Purchases
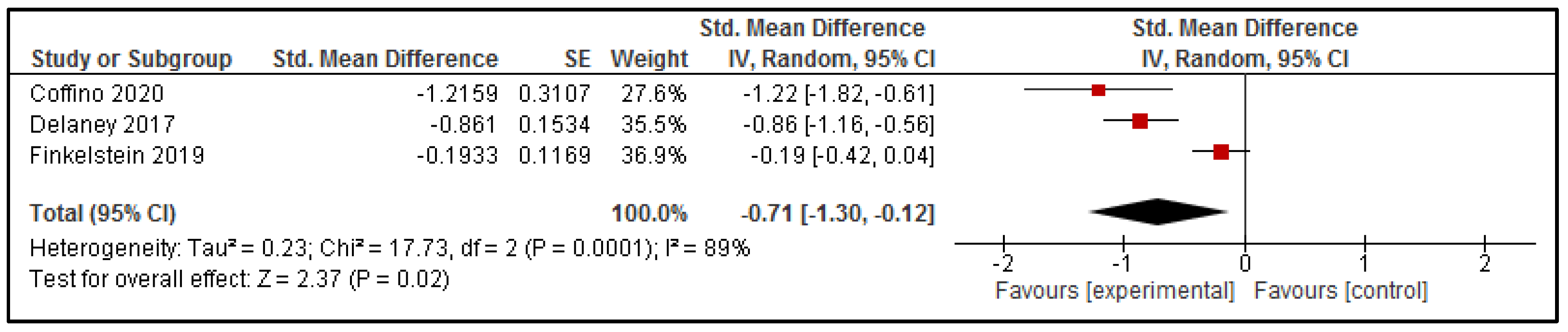
3.4.2. Total Fat and Saturated Fat Content of Purchases
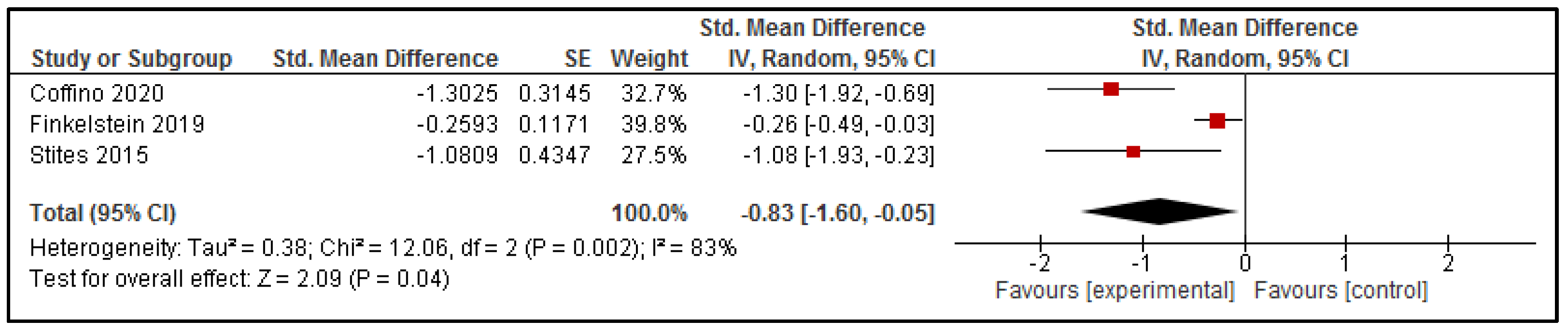
3.4.3. Sodium Content of Purchases
3.5. Intervention Effects: Narrative Synthesis
3.5.1. ‘Other’ Nutrient Content of Purchases
3.5.2. ‘Healthiness’ or ‘Nutritional Quality’ of Purchases
3.5.3. Cost of Interventions Delivered via Online Food Ordering Systems
3.5.4. Unintended Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Collaborators, G.D. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2017, 393, 1958–1972. [Google Scholar]
- Murray, C.J.; Aravkin, A.Y.; Zheng, P.; Abbafati, C.; Abbas, K.M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abdelalim, A.; Abdollahi, M.; Abdollahpour, I. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef]
- Eurostat Statistics Explained. Fruit and Vegetable Consumption Statistics. 2018. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php/Fruit_and_vegetable_consumption_statistics#Consumption_of_fruit_and_vegetables (accessed on 5 March 2021).
- NHS Digital. Health Survey for England 2019: Fruit & Vegetables. 2019. Available online: http://healthsurvey.hscic.gov.uk/data-visualisation/data-visualisation/explore-the-trends/fruit-vegetables.aspx (accessed on 4 March 2021).
- United Health Foundation. America’s Health Rankings. National Fruit and Vegetable Consumption. 2021. Available online: https://www.americashealthrankings.org/explore/annual/measure/fvcombo/state/U.S (accessed on 4 March 2021).
- Australian Institute of Health and Welfare. Australia’s Health 2018. Fruit and Vegetable Intake; AIHW: Canberra, Australia, 2018.
- World Health Organization. Diet, Nutrition, and the Prevention of Chronic Diseases: Report of a Joint WHO/FAO Expert Consultation; World Health Organization: Geneva, Switzerland, 2003; Volume 916. [Google Scholar]
- Eilander, A.; Harika, R.K.; Zock, P.L. Intake and sources of dietary fatty acids in Europe: Are current population intakes of fats aligned with dietary recommendations? Eur. J. Lipid Sci. Technol. 2015, 117, 1370–1377. [Google Scholar] [CrossRef] [Green Version]
- Lei, L.; Rangan, A.; Flood, V.M.; Louie, J.C.Y. Dietary intake and food sources of added sugar in the Australian population. Br. J. Nutr. 2016, 115, 868–877. [Google Scholar] [CrossRef] [Green Version]
- Brown, I.J.; Tzoulaki, I.; Candeias, V.; Elliott, P. Salt intakes around the world: Implications for public health. Int. J. Epidemiol. 2009, 38, 791–813. [Google Scholar] [CrossRef] [Green Version]
- Hawkes, C.; Jewell, J.; Allen, K. A food policy package for healthy diets and the prevention of obesity and diet-related non-communicable diseases: The NOURISHING framework. Obes. Rev. 2013, 14, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Pineda, E. The Evolving Virtual Food Environment: Impact on Food Retailers, Consumers, and Health; Imperial College London: London, UK, 2020. [Google Scholar]
- Li, C.; Mirosa, M.; Bremer, P. Review of Online Food Delivery Platforms and their Impacts on Sustainability. Sustainability 2020, 12, 5528. [Google Scholar] [CrossRef]
- Granheim, S.I.; Opheim, E.; Terragni, L.; Torheim, L.E.; Thurston, M. Mapping the digital food environment: A scoping review protocol. BMJ Open 2020, 10, e036241. [Google Scholar] [CrossRef] [Green Version]
- Bates, S.; Reeve, B.; Trevena, H. A narrative review of online food delivery in Australia: Challenges and opportunities for public health nutrition policy. Public Health Nutr. 2020, 1–11. [Google Scholar] [CrossRef]
- Resendes, S. 31 Online Ordering Statistics Every Restauranteur Should Know in 2020. Available online: https://upserve.com/restaurant-insider/online-ordering-statistics/ (accessed on 21 August 2020).
- Keyes, D. The Online Grocery Report: Coronavirus Is Accelerating US Online Grocery Shopping Adoption—Here Are the market Stats, Trends and Companies to Know. 2021. Available online: https://www.businessinsider.com/online-grocery-report-2020?r=AU&IR=T (accessed on 4 March 2021).
- Dalgleish, R. How the COVID-19 Pandemic Has Accelerated the Shift to Online Spending. 2020. Available online: https://blog.ons.gov.uk/2020/09/18/how-the-covid-19-pandemic-has-accelerated-the-shift-to-online-spending/ (accessed on 4 March 2021).
- Pitt, E.; Gallegos, D.; Comans, T.; Cameron, C.; Thornton, L. Exploring the influence of local food environments on food behaviours: A systematic review of qualitative literature. Public Health Nutr. 2017, 20, 2393–2405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thorndike, A.N.; Sunstein, C.R. Obesity Prevention in the Supermarket-Choice Architecture and the Supplemental Nutrition Assistance Program. Am. J. Public Health 2017, 107, 1582–1583. [Google Scholar] [CrossRef]
- Thorndike, A.N.; Sonnenberg, L.; Riis, J.; Barraclough, S.; Levy, D.E. A 2-Phase Labeling and Choice Architecture Intervention to Improve Healthy Food and Beverage Choices. Am. J. Public Health 2012, 102, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Bucher, T.; Collins, C.; Rollo, M.E.; McCaffrey, T.A.; De Vlieger, N.; Van der Bend, D.; Truby, H.; Perez-Cueto, F.J. Nudging consumers towards healthier choices: A systematic review of positional influences on food choice. Br. J. Nutr. 2016, 115, 2252–2263. [Google Scholar] [CrossRef] [PubMed]
- Cameron, A.J.; Charlton, E.; Ngan, W.W.; Sacks, G. A systematic review of the effectiveness of supermarket-based interventions involving product, promotion, or place on the healthiness of consumer purchases. Curr. Nutr. Rep. 2016, 5, 129–138. [Google Scholar] [CrossRef]
- Delaney, T.; Wyse, R.; Wolfenden, L. Online Food Delivery Systems & Their Potential to Improve Public Health Nutrition: A Response to ‘A Narrative Review of Online Food Delivery in Australia. Public Health Nutr. 2021, 18, 1–5. [Google Scholar]
- Indig, D.; Lee, K.; Grunseit, A.; Milat, A.; Bauman, A. Pathways for scaling up public health interventions. BMC Public Health 2018, 18, 68. [Google Scholar] [CrossRef] [Green Version]
- Milat, A.J.; Bauman, A.; Redman, S. Narrative review of models and success factors for scaling up public health interventions. Implement. Sci. 2015, 10, 113. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred Reporting Items for Systematic Reviews and Meta Analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 6. [Google Scholar] [CrossRef] [Green Version]
- Wyse, R.; Jackson, J.; Grady, A.; Delaney, T.; Stacey, F.; Wolfenden, L.; Yoong, S. The Effectiveness of Interventions Delivered via Online Food Ordering Systems Targeting Dietary Behaviours: A Systematic Review Protocol. Available online: Osf.io/85fup (accessed on 28 September 2020).
- Münscher, R.; Vetter, M.; Scheuerle, T. A review and taxonomy of choice architecture techniques. J. Behav. Decis. Mak. 2016, 29, 511–524. [Google Scholar] [CrossRef]
- Higgins, J.P.; Savović, J.; Page, M.J.; Elbers, R.G.; Sterne, J.A. Assessing risk of bias in a randomized trial. In Cochrane Handbook for Systematic Reviews of Interventions; Cochrane: London, UK, 2019; pp. 205–228. [Google Scholar]
- Sterne, J.; Higgins, J.; Elbers, R.; Reeves, B. The Development Group for ROBINS-I Risk of Bias in Non-Randomized Studies of Interventions (ROBINS-I): Detailed Guidance; Cochrane Bias Methods Group: Bristol, UK, 2016. [Google Scholar]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Deeks, J.J.; Higgins, J.P.; Altman, D.G.; Group, C.S.M. Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions; Cochrane: London, UK, 2019; pp. 241–284. [Google Scholar]
- Coffino, J.A.; Udo, T.; Hormes, J.M. Nudging while online grocery shopping: A randomized feasibility trial to enhance nutrition in individuals with food insecurity. Appetite 2020, 152, 104714. [Google Scholar] [CrossRef]
- Doble, B.; Ler, F.A.J.; Finkelstein, E.A. The effect of implicit and explicit taxes on the purchasing of ‘high-in-calorie’products: A randomized controlled trial. Econ. Hum. Biol. 2020, 37, 100860. [Google Scholar] [CrossRef]
- Huang, A.; Barzi, F.; Huxley, R.; Denyer, G.; Rohrlach, B.; Jayne, K.; Neal, B. The effects on saturated fat purchases of providing internet shoppers with purchase-specific dietary advice: A randomised trial. PLoS Clin. Trials 2006, 1, e22. [Google Scholar] [CrossRef]
- Miller, G.F.; Gupta, S.; Kropp, J.D.; Grogan, K.A.; Mathews, A. The effects of pre-ordering and behavioral nudges on National School Lunch Program participants’ food item selection. J. Econ. Psychol. 2016, 55, 4–16. [Google Scholar] [CrossRef]
- Stites, S.D.; Singletary, S.B.; Menasha, A.; Cooblall, C.; Hantula, D.; Axelrod, S.; Figueredo, V.M.; Phipps, E.J. Pre-ordering lunch at work. Results of the what to eat for lunch study. Appetite 2015, 84, 88–97. [Google Scholar] [CrossRef]
- VanEpps, E.M.; Downs, J.S.; Loewenstein, G. Calorie label formats: Using numeric and traffic light calorie labels to reduce lunch calories. J. Public Policy Mark. 2016, 35, 26–36. [Google Scholar] [CrossRef] [Green Version]
- Finkelstein, E.A.; Ang, F.J.L.; Doble, B. Randomized trial evaluating the effectiveness of within versus across-category front-of-package lower-calorie labelling on food demand. BMC Public Health 2020, 20, 1–10. [Google Scholar] [CrossRef]
- Finkelstein, E.A.; Ang, F.J.L.; Doble, B.; Wong, W.H.M.; van Dam, R.M. A randomized controlled trial evaluating the relative effectiveness of the Multiple Traffic Light and Nutri-Score front of package nutrition labels. Nutrients 2019, 11, 2236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delaney, T.; Wyse, R.; Yoong, S.L.; Sutherland, R.; Wiggers, J.; Ball, K.; Campbell, K.; Rissel, C.; Lecathelinais, C.; Wolfenden, L. Cluster randomized controlled trial of a consumer behavior intervention to improve healthy food purchases from online canteens. Am. J. Clin. Nutr. 2017, 106, 1311–1320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wyse, R.; Gabrielyan, G.; Wolfenden, L.; Yoong, S.; Swigert, J.; Delaney, T.; Lecathelinais, C.; Ooi, J.Y.; Pinfold, J.; Just, D. Can changing the position of online menu items increase selection of fruit and vegetable snacks? A cluster randomized trial within an online canteen ordering system in Australian primary schools. Am. J. Clin. Nutr. 2019, 109, 1422–1430. [Google Scholar] [CrossRef] [PubMed]
- Sacks, G.; Tikellis, K.; Millar, L.; Swinburn, B. Impact of ‘traffic-light’nutrition information on online food purchases in Australia. Aust. N. Z. J. Public Health 2011, 35, 122–126. [Google Scholar] [CrossRef]
- Blüher, M. Obesity: Global epidemiology and pathogenesis. Nat. Rev. Endocrinol. 2019, 15, 288–298. [Google Scholar] [CrossRef]
- Clifton, P.; Keogh, J. A systematic review of the effect of dietary saturated and polyunsaturated fat on heart disease. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 1060–1080. [Google Scholar] [CrossRef] [PubMed]
- Grillo, A.; Salvi, L.; Coruzzi, P.; Salvi, P.; Parati, G. Sodium intake and hypertension. Nutrients 2019, 11, 1970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skov, L.R.; Lourenco, S.; Hansen, G.L.; Mikkelsen, B.E.; Schofield, C. Choice architecture as a means to change eating behaviour in self-service settings: A systematic review. Obes. Rev. 2013, 14, 187–196. [Google Scholar] [CrossRef]
- Metcalfe, J.J.; Ellison, B.; Hamdi, N.; Richardson, R.; Prescott, M.P. A systematic review of school meal nudge interventions to improve youth food behaviors. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 1–19. [Google Scholar] [CrossRef]
- Wilson, A.L.; Buckley, E.; Buckley, J.D.; Bogomolova, S. Nudging healthier food and beverage choices through salience and priming. Evidence from a systematic review. Food Qual. Prefer. 2016, 51, 47–64. [Google Scholar] [CrossRef]
- Pulker, C.E.; Farquhar, H.R.; Pollard, C.M.; Scott, J.A. The nutritional quality of supermarket own brand chilled convenience foods: An Australian cross-sectional study reveals limitations of the Health Star Rating. Public Health Nutr. 2020, 23, 2068–2077. [Google Scholar] [CrossRef] [PubMed]
- Vehmas, K.; Lavrusheva, O.; Seisto, A.; Poutanen, K.; Nordlund, E. Consumer insight on a snack machine producing healthy and customized foods at point of consumption. Br. Food J. 2019. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year; Study Design, Country | Online Food Ordering Environment; Participant Characteristics | Sample Size * | Intervention Description [Choice Architecture Strategies] † | Duration of Intervention | Control Description | Dietary Outcomes Assessed: Primary Outcomes | Adverse Events/Costs: Secondary Outcomes |
|---|---|---|---|---|---|---|---|
| Coffino [34], 2020; RCT, US | Online supermarket; Adults (mean age 46.6 years; 76% male) with food insecurity from a single-person household | n = 50 | Participants were presented with a prefilled online grocery shopping cart containing groceries selected to meet nutrition requirements based on participant sex and age. [Changing choice defaults]. Participants were free to delete, add, exchange or keep items in their cart prior to finalizing their purchase. [Changing option-related effort]. | Participants exposed to intervention in a single online grocery shop | Alternative intervention: Participants read nutrition education handout prior to completing their purchase. | Average daily food and nutrient content of purchases: Wholegrain (serves/d); Fruit (serves/d); Vegetable (serves/d); Calories (kCal/d); Fat (g/d); Saturated Fat (g/d); Sodium (mg/d); Cholesterol (mg/d); Fibre (mg/d) | Nil |
| Doble [35], 2020; RCT, Singapore | Online supermarket; Adults (mean age 35.6 years, 49% male), and were Singapore residents. | n = 941 | 20% of products with the highest calories per serving (excluding fruit and vegetables) had a price rise of 20%. There were 3 intervention arms: (1) Implicit Tax: High calorie products labelled with ‘raised price’ only (no explaination) (2) Fake tax: Shows price pre and post the price rise and falsely indicates that the product will incur a 20% price rise due to high calorie content (3) Explicit tax: Shows the same label as fake tax group, but the 20% price rise is actually applied. [Changing option consequences; Making information visible] | Participants exposed to intervention in a single online grocery shop | True control: No labels or price manipulation strategy applied | The proportion of taxed (i.e., high calorie) products purchased; The kCal per serve purchased; The Alternative Healthy Eating Index Score of purchases. The kCal per $ spent. | The average total cost per shop. |
| Finkelstein [40], 2020; Crossover RCT, Singapore | Online supermarket; Adults (mean age 35 years, 21% male), who were the primary shopper for their household and were a registered shopper with RedMart (the online food ordering platform provider) | n = 146 | For each shop participants could spend between SG$50–250, and asked to complete a typical weekly grocery shop for 3 weeks (3 shops in total). 2 online labelling intervention arms, both applied a ‘Lower calorie’ label: [Making information visible]. (1) Within category labels applied: 20% of products within each product category that were lowest in calories per serve were labelled * (2) Across category labels applied: 20% of all products that were lowest in calories per serve were labelled. | Participants shopped once a week for 3 weeks (exposed to a different intervention group each week in random order). | True control: no online intervention applied to online supermarket. | The proportion of low calorie products purchased per shop. The total calories (kCal) per serve purchased; total calories (kCal) purchased per shop; and total calories purchased per $ spent | Total cost of the shop |
| Finkelstein [41], 2019; Crossover RCT, Singapore | Online supermarket; Adults (mean age 34.7 years, 31% male), who were Singapore residents and were a registered shopper with RedMart (the online food ordering platform provider) | n = 147 | For each shop participants could spend between SG$50–100, and asked to complete a typical weekly grocery shop for 3 weeks (3 shops in total). 2 online labelling intervention arms: [Making information visible] (1) Multiple Traffic Light (MTL) labels were applied to all products * (2) Nutri-score (NS) labels were applied to all products. Prior to each shopping trip, a 60 s video briefly explained how to use the labels that had been applied (MTL or NS). [Translating information] | Participants shopped once a week for 3 weeks (exposed to a different intervention group each week in random order). | True control: no online intervention applied to online supermarket. | Diet quality per shopping trip using the AHEI-2010. Average Nutri-Score of the shopping basket, weighted by serve size. The total calories, saturated fat, total fat, sodium and sugar per serve purchased. Calories per $ spent. | Total cost of the shop |
| Sacks [44], 2011; CCT, Australia | Online supermarket; Customers of online supermarket (participant demographics not further specified) | NA | A set of four traffic light labels to show relative levels of fat, saturated fat, sugar and sodium, were applied to products of the retailer’s own brand (including, milk, bread, breakfast cereals, biscuits and frozen meals) [Making information visible], as there were commercial constrains around labelling branded products. On the home page of the intervention store, and on each of the selected category and product pages, a link was provided to a page providing information about the trial, an explanation of the traffic light indicators, how to interpret them, and general nutrition advice (e.g., Australian dietary guidelines). | Intervention was active for 10 weeks. | True control: no nutrition information was provided on the comparison store site during the trial period. | Change in sales by healthiness of products. | Nil |
| Huang [36], 2006; RCT, Australia | Online supermarket; Adult (mean age 40 years, 12% male) customers of an online supermarket service. | n = 456 | 383 commonly purchased pre-packaged food items that contained >1% saturated fat were selected, and a suitable lower-fat alternative was identified for each (524 foods were identified). Participants assigned to the intervention received advice tailored to the food items they had selected for purchased. This was done automatically by a computer program, and for each items that had >1% saturated fat, participants were presented with the opportunity to retain or swap the item for an alternative, lower saturated fat item (using a side by side comparison of the products). [Making information visible, Changing choice defaults/Prompted choice] | Participants were offered the same form of advice each time that they used the online supermarket during the 5 month recruitment and follow-up period. | Alternative intervention: Participants directed to the National Heart Foundation webpage, then prompted to make changes to their purchases. | Mean % saturated fat in the purchased items among the 524 foods studied. | The mean cost per 100 g for the swapped items. |
| Wyse [43], 2019; C-RCT, Australia | Online School Canteen; Primary schools students (kindergarten to grade 6) attending government schools with an online canteen ordering system. Online canteen user might include parents of schools students | 6 schools, and 1903 students | Online canteen menus were redesigned so that fruit and vegetable snack items were positioned first and last on the menu [Changing the range or composition of options]. Target items included fruit or vegetable items (fresh, frozen, tinned or dried) that the children could consume as a snack. Target items were grouped together in a single category titled “fruit and veggie snacks”, which were displayed in 2 places, first and last categories on the online menu. Within this category, items were listed in the following order: whole fresh fruit, cut-up fresh fruit, frozen fruit, tinned fruit, dried fruit, fruit with accompaniments, fresh salad vegetable, cooked vegetables, vegetables with accompaniments. | 4 week intervention | True control: no changes were made to the online menus. | The proportion of all online orders that contained at least one fruit or vegetable snack food. The proportion of all individual items within all online lunch orders that are a fruit or vegetable snack food. | Average lunch time weekly revenue |
| Delaney [42], 2017; C-RCT, Australia | Online School Canteen; Primary schools students (kindergarten to grade 6) attending included government schools. Online canteen user might include parents of schools students. | 10 schools, and 2371 students. | Intervention schools were provided a canteen menu feedback report to improve the availability of healthy foods (strategy not delivered online). Menu labels (traffic light labels) were applied to online menu items. [Making information visible]. Healthy menu items were listed in the main website display, while users had to click and explore the less healthy menu items. [Changing option related effort]. When users chose unhealthy items, they were prompted to add a healthy item. [Prompted choice]. Healthy items were displayed in bold font, image and positive food prompt “this is a good choice”, [Changing option consequence]. | 2 month intervention | True control: Schools with online canteen did not receive any of the interventions strategies. | The mean energy (kj); saturated fat (g), sugar (g), and sodium (mg) content of student online lunch orders. The mean % energy of student online lunch orders derived from saturated fat and sugar. The mean % of student online lunch orders that were classified as “high nutritional value” and “low nutritional value”. | Canteen weekly revenue |
| Miller [37], 2016; RCT, US | Online school food service; Elementary or middle school students (5th–6th grade), receiving the National School Lunch Program. | n = 71 | While pre-ordering lunch online, students received nudges if their meal did not contain all five meal components (i.e., meat/alternative, grain, fruit, vegetables, and dairy). The nudge, “Your meal does not look like a balanced meal” would appear, and a plate was shown as a visual representation and highlight areas of the meal that the student had not selected, and were provided the option to change their orders [Making information visible]. Nudges were primarily provided for fruit, vegetable and/or dairy. Students who selected all 5 components received positive feedback consisting of a smiley face and message “You have ordered a balanced meal”. If a meal remained unbalanced after receiving the nudge, students received a message stating “Please select a fruit, vegetable or dairy. Otherwise you will be charged for each item separately”. Students that did not select these 3 components were charged for each item separately. [Changing option consequence] | Intervention was delivered to students for 2 weeks. | True control: Students pre-ordered lunch online, and did not receive nudges. If they had not selected fruit, vegetable or dairy they received: “Please select a fruit, vegetable or dairy. Otherwise you will be charged for each item separately”. | The % of vegetables, fruit and low fat dairy in meals ordered. | Nil. |
| VanEpps [39], 2016; RCT, US | Online workplace cafeteria; Adults (mean age 40 years, 39% male) employed at a large health care company, and placed at least one online order during the intervention period. | n = 249 | Using an online based system, participants were required to select exactly one meal for lunch, and had the option to add as many drinks, snacks and desserts that they wanted. There were 13 meal, 23 snack/dessert and 30 drink options. Participants were assigned to 1 of 3 menu labelling options: [Making information visible]. (1) Traffic light labels (green, yellow, red: based on calorie content); (2) Calorie information appeared next to each menu item. (3) Combined Traffic light and calorie labelling On Monday and Wednesday morning, participants received an email reminding them of the study, and the discount (providing in a link to the website). | 4 week intervention | True control: no online menu labels | Total lunch calories purchased. | Nil. |
| Stites [38], 2015; RCT, US | Online workplace (hospital) food service; Adult (mean age 44.9 years, 11.5% male) employees who worked full-time at the study hospital and were overweight (BMI > 25 kg/m2). | n = 26 | An online pre-ordering system was developed, to allow participants to order their lunches and view the nutrient content of their choices (calorie and fat content, plus ingredients) [Making information visible]. The system selected the version of the food selected with the least calories and fat by default [Changing choice defaults]. This intervention included Mindful eating training (90 min session) that was delivered offline. 20 × US$1.25 lunch order vouchers were provided to all participants (intervention and control), to encourage the use of the online ordering system. | 4 week intervention | Delayed intervention group | Average kilocalories and grams of fat in purchased meals. | Nil. |
| Cost of the Intervention to the Consumer | |
| Huang, 2006 | Mean cost per 100 g of foods purchased: Intervention: AUD $0.63 [0.58–0.68]/100 g Control: AUD $0.62 [0.58–0.067]/100 g |
| Finkelstein, 2019 | Difference in mean total expenditure per shop vs. control: Nutri-Score labels: S$0.90 [SE: 0.98] Multi-Traffic-Light labels: S$1.13 [SE: 1.06] |
| Finkelstein, 2020 | Difference in mean total expenditure per shop vs. control: Within-category labels: S$0.11 [−0.40, 0.63] Across-category labels: S$0.18 [−0.33, 0.70] |
| Doble, 2020 | Difference in mean total expenditure per shop vs. control: Implicit tax: S$1.86 [−1.38, 5.39] Fake tax: −S$0.32 [−3.40, 2.82] Explicit tax: −S$0.79 [−3.83, 2.34] |
| Cost of the Intervention to the Foodservice | |
| Wyse, 2019 | Weekly revenue per school (Relative Mean Difference): AUD $180 [−16, 376], p = 0.07 |
| Delaney, 2017 | Weekly revenue per school (Relative Mean Difference): AUD −$62.33 [−212.36, 87.68], p = 0.41 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wyse, R.; Jackson, J.K.; Delaney, T.; Grady, A.; Stacey, F.; Wolfenden, L.; Barnes, C.; McLaughlin, M.; Yoong, S.L. The Effectiveness of Interventions Delivered Using Digital Food Environments to Encourage Healthy Food Choices: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 2255. https://doi.org/10.3390/nu13072255
Wyse R, Jackson JK, Delaney T, Grady A, Stacey F, Wolfenden L, Barnes C, McLaughlin M, Yoong SL. The Effectiveness of Interventions Delivered Using Digital Food Environments to Encourage Healthy Food Choices: A Systematic Review and Meta-Analysis. Nutrients. 2021; 13(7):2255. https://doi.org/10.3390/nu13072255
Chicago/Turabian StyleWyse, Rebecca, Jacklyn Kay Jackson, Tessa Delaney, Alice Grady, Fiona Stacey, Luke Wolfenden, Courtney Barnes, Matthew McLaughlin, and Sze Lin Yoong. 2021. "The Effectiveness of Interventions Delivered Using Digital Food Environments to Encourage Healthy Food Choices: A Systematic Review and Meta-Analysis" Nutrients 13, no. 7: 2255. https://doi.org/10.3390/nu13072255
APA StyleWyse, R., Jackson, J. K., Delaney, T., Grady, A., Stacey, F., Wolfenden, L., Barnes, C., McLaughlin, M., & Yoong, S. L. (2021). The Effectiveness of Interventions Delivered Using Digital Food Environments to Encourage Healthy Food Choices: A Systematic Review and Meta-Analysis. Nutrients, 13(7), 2255. https://doi.org/10.3390/nu13072255