
Identifying Low Value Malnutrition Care Activities for De-Implementation and Systematised, Interdisciplinary Alternatives—A Multi-Site, Nominal Group Technique Approach


Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Demographics
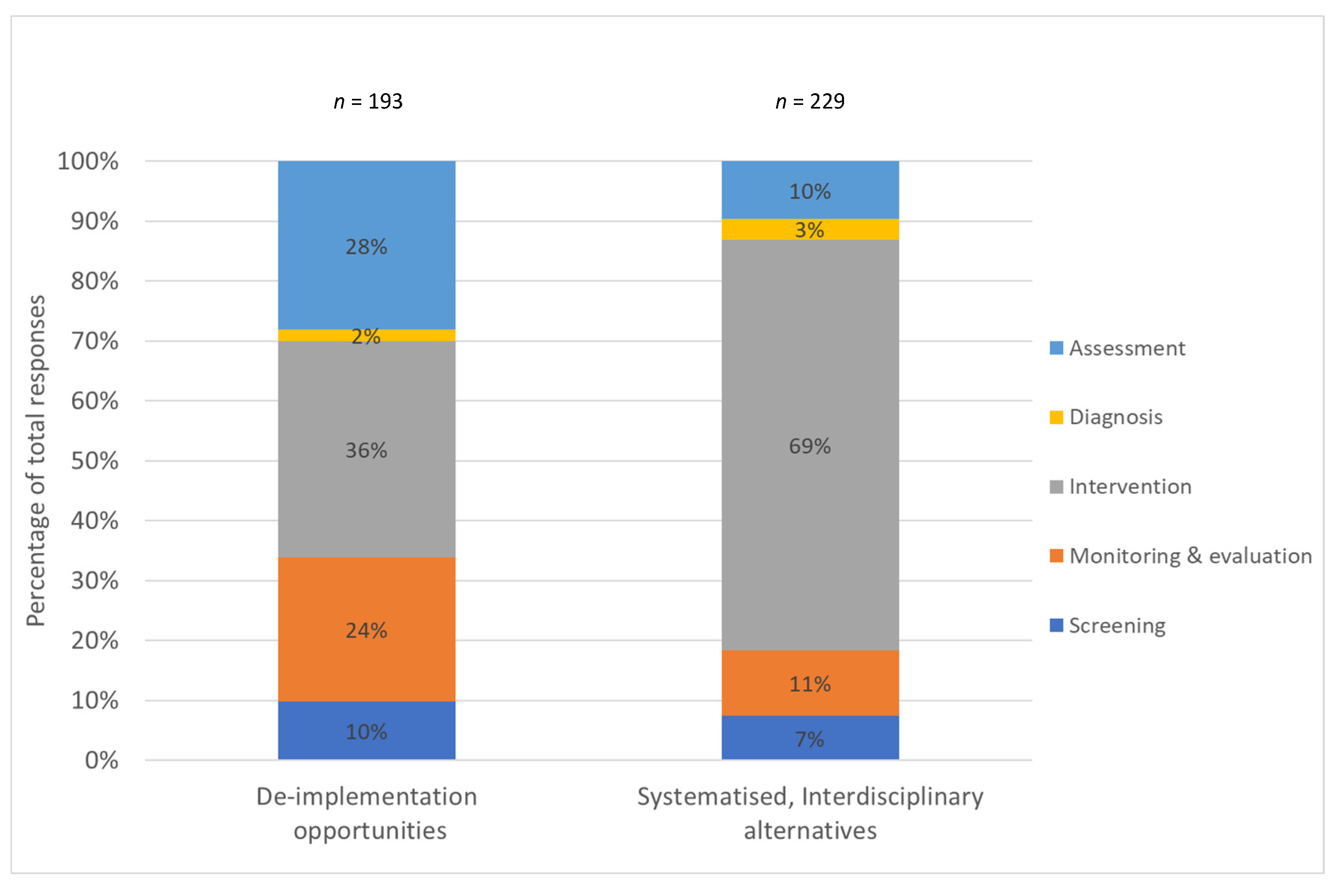
3.2. Low-Value Nutrition Care Activities for De-Implementation
3.2.1. Screening Activities for De-Implementation
3.2.2. Assessment Activities for De-Implementation
3.2.3. Diagnosis Activities for De-Implementation
3.2.4. Intervention Activities for De-Implementation
3.2.5. Monitoring and Evaluation Activities for De-Implementation
3.3. Systematised, Interdisciplinary Alternatives
3.3.1. Screening Alternatives
3.3.2. Assessment Alternatives
3.3.3. Diagnosis Alternatives
3.3.4. Intervention Alternatives
3.3.5. Monitoring and Evaluation Alternatives
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

- Identify a facilitator.
- Organise room and supplies as per the CDC guideline:
- Pre-distributed SIMPLE infographic, summary, and pathway.
- Local data for presentation (delegation survey graphs and dietetic survey results).
- -
- Current practice (DTN individually delivering, AHA individually delivering);
- -
- Time to provide individualised malnutrition care for ALL malnourished/at risk of malnutrition + other tasks (Q7 on DTN delegation survey);
- -
- Full scope perception.
- Attendance sheet (demographics of attendees).
- Q1 and Q2 answer sheets for step 1.
- Large butchers paper flip chart: 3 pages (food and nutrient, education, coordination of care).
- Markers.
- Dot stickers for step 4 (5 per person).
- Food/drinks.
- Because we think you can help us to identify better ways to improve malnutrition care provided patients in hospital, every day; and
- SIMPLE implementation will impact on your day-to-day activities.
- What highly individualised malnutrition care activities do you think we could replace with SIMPLE malnutrition care?
- What SIMPLE opportunities do you think we should do instead to provide more effective and efficient nutrition care in our ward/hospital?
| |
| |
Appendix B
- 1 h ax of MST 2.
- All outpatients without a screening/triaging process.
- Assistant staff “solo” meal rounds.
- “At risk” staying in “supporting”.
- Biochem data (scaffolded) by DNs.
- Blanket referrals (dependent on area -> consider locally where likely not adding value).
- Blanket referrals to Dietitian (vs, e.g., system or interdisciplinary).
- BMIs >40 individualised DN.
- Completing full assessments for pts not for enteral feeding (RACF, chronic disease, etc., frequent flyers, PEG feeds).
- Day 1 enteral tube feeding r/v.
- Detailed handovers by DNs where unlikely to add value.
- Diet restrictions.
- Dietitian (re)educations HPHE by DNs, d/c educations by DNs, f/u wound educations.
- Dietitian ax for referrals for incomplete MSTs/unsures/2s and/or spending lots of time on these.
- Dietitian SGAs/diagnosis (malnutrition).
- Director from doing HENs a/c, DNs doing HENs registration.
- Discharge referral process (e.g., PACs) for pts at risk of malnutrition/or malnourished who? Requires specialised nutrition care.
- Discharge summaries.
- Diverticulitis or HPHE counselling or other basic educations.
- DN basic malnutrition educations (but ensuring DN gives diagnosis).
- DN doing all of assessment/diagnostic, e.g., SGAs.
- DN HPHE education.
- DN individualised RACF handover.
- DN must see (at risk) for all, e.g., Pus, etc.
- DN nutrition screening in paediatrics wards.
- DN r/vs (or news for known or non-compliant) that might not change outcomes substantially.
- DN requirement for diet changes (e.g., manually putting on HPHE by DN).
- DN solo scripting.
- DN specific mealtime support.
- DN/NA having to chase weights/other ax data, weekly MST et.
- DNs and NA ongoing full r/v for “not for tube feeding”.
- DNs chasing up weights/weighing patients.
- DNs doing Ax of low risk/MST 2s, e.g., malnutrition management, oral nutrition support, educations, food charts, med pass, etc.
- DNs doing HPHE education.
- DNs doing reviews where low value unless escalated nutrition support is requested.
- DNs doing supply and distribution.
- DNs required for HP diets, etc.
- DNs spending + time on PFM triaging/new referrals, etc. for day/screening patients to be delegated.
- DN prescribing SAM.
- (Excessively) long chart entries/documentation/assessment.
- Education for other, e.g., diverticular and gout disease.
- Education of patients where does not require specialist DN education skills.
- EN/PN DN required to start.
- Excess reviews where unlikely to add benefit/no new action to do.
- Extended individual inpatient malnutrition care (e.g., 45+ min).
- Feeling bad if chart r/v not perfect.
- Flavour change/preference checks.
- Food chart and intake r/vs.
- Food intake monitoring/record charts.
- Food/flavour preferences by Dietitian.
- Foodservice complaints or issues by DNs.
- Full ax and intervention for frequent flyers.
- General HPHE educations.
- Going to [site name removed for confidentiality].
- Highly individualised enteral feed (r/vs) by DNs.
- HPHE education by DNs on low risk.
- Inappropriate referrals through PFM.
- Individualised DN care when this might be achieved using protocols or pathways or asking for DN before systems in place and applied.
- Intake and weight ax data by dietitians for non-specialised patients.
- Interventions where the outcomes does not matter to pt or is unlikely to influence outcomes.
- Lifestyle education on discharge.
- Long stay stable pts (regardless of nutrition status), e.g., palliative care.
- Low value d/c coordination for “at risk” but not specialised.
- Low value reviews by DN.
- MDT education (e.g., doctors) re malnutrition status.
- Medical round.
- Missing care (across care process) to some of the at risk.
- Monitoring setup/meal assistance.
- Monthly MST audit.
- MST “unsures”.
- MST 2 being seen by dietitian.
- MST 2 care by dietitians.
- MST 2 DN ax.
- MST 2 patients.
- MST screening by DAs.
- Multiple professions/other screening, e.g., nurses, assistants, etc.
- NA MSTs.
- NA preference checks.
- NAFLD in OPDs.
- NAs and nurses doing duplicate screens on all pts.
- Nursing home d/c reports.
- Ongoing r/vs while waiting for change, e.g., diet upgrade to the upgrade progression to tube feeds.
- Oral nutrition supplement reviews.
- Other educations by DNs on low risk.
- Over-reviews without purpose by DNs.
- Preference checks by DNs.
- Pt preferences/tolerances by DNs.
- Pump education.
- R/Vs for anthropometry/see above.
- Rechecking biochem for at risk of refeeding.
- Referrals for inappropriate weight gain.
- Reliance on D/N to prescribe SAM.
- Reliance on DN initiated MEDPASS/SAM.
- Relying on AHA/DN initiation of food charts.
- Reviewing and triaging MST scores.
- Shifting long r/v to supportive care (stop multiple individual dietetic reviews instead do supportive).
- Supplements trolley being done by a DA.
- Support reviews/preference checks by DNs.
- Thickened fluid education.
- Waiting for education by DN for MST 2+.
- Weighing patients.
| Ax = Assessment |
| d/c = Discharge |
| DA = Dietitian assistant |
| DN = Dietitian |
| EN = Enteral nutrition |
| f/u = Follow-up |
| HENS = Home enteral nutrition support |
| HPHE = High protein high energy |
| MDT = Multi-disciplinary team |
| MST = Malnutrition screening tool |
| MST 2 = Malnutrition screening tool score of 2 |
| NA = Nutrition Assistant |
| NAFLD = Non-alcoholic fatty liver disease |
| OPD = Outpatient department |
| PACS = Post-acute care service |
| PEG = Percutaneous endoscopic gastrostomy |
| PFM = Patient flow manager |
| PN = Parenteral nutrition |
| Pt = Patient |
| PU = Pressure ulcer |
| r/v = Review |
| RACF = Residential aged care facility |
| SAM = Supplements as medicine |
| SGA = Subjective global assessment |
Appendix C
- AHA [intake and weight ax data for non-specialised patients] with intervention plan.
- AHA audit of what care people are getting.
- AHA educations.
- AHA ensuring all at risk are getting a food and nutrition treatment.
- AHA follow-up post discharge (although may have funding issues).
- AHA HENS orders.
- AHA malnutrition education for home.
- AHA mealtime audits.
- AHA systematised HP for at risk, e.g., 7+ days.
- AHAs to see MST 2s.
- “Allowing” other HPs to provide an intervention.
- Applied protocols for enteral feeds, eating disorders, etc.
- Appropriate screening including blanket referral.
- Assistant data collection (any ax data, e.g., biochem, anthropometry, intake, audit/monitoring).
- Assistant facilitated—SGAs (+training).
- Assisted mealtimes.
- Assisted SGAs.
- Auto nutrition support cart.
- Automated d/c summary for RACF pts.
- Automated process/referral for specialised care (multiple criteria required).
- Better feeding assistance.
- Better handover, e.g., to GPs for at risk.
- Better identification of “at risk” pts (e.g., red folder/electronic/etc.)—including what is in place/could be done by team.
- Better screening beyond just MST, e.g., for ICU, #NOF, etc.
- Blanket “HP” for at risk.
- Blanket interventions [by IDT], e.g., HP or whatever, rather than waiting for DN under blanket DN.
- Clear, e.g., WPI to escalate pts who are for tube feeds, and when we are not going to come back unless they are for tube feeds.
- Clearer expectations for who could receive “supportive” vs specialist (DN) care + better referral criteria.
- DA (+ NA if can get time)—re-screening high risk (e.g., on PFM) + 7-day re-screen + repeat MST.
- DA/NA basic education.
- DA/NA chase assessment data.
- DA/NA home follow up/see if want a referral.
- DA/NA NEMO sheet and d/c planning.
- DA/NA place on HP +/- food chart.
- DA/medical/nursing/students full scope SIMPLE for MST 2/at risk (data collection, e.g., weighing, chart audit, diagnosis—PG-SGA/SGA, data collection and assisted diagnosis, HPHE education, auditing of interventions, organising food/nutrition and supplements, systematised. Not call to dietitian).
- Decrease inpatient time to allow out of hospital care or other higher value activities.
- Default HPHE (SAM) for at risk.
- Delegating or automatically generated d/c summaries.
- Delegation/escalation/discharge criteria.
- Delegation at risk direct to DAs/delegation from DN to DAs (re-escalation).
- DN and AHA team support processes (MDT meeting, board rounds, ward rounds, case conferences).
- Education + training—inservices (including local data feedback, e.g., SIMPLE audits), for interdisciplinary teams/DAs.
- Education by MDT, including d/c planning (Nursing, AHA, medical, students, other Allied Health).
- Engaging pts in care and evaluation of care (+ not wasting time when not engaged)
- Expand nutrition cart.
- External facilitator and NA together [RACF handover].
- Feeding assistance/mealtime assistance coordinator.
- Food chart + intake r/v by NA with escalation criteria.
- Foodservice staff doing food preferences/menu choices and complaints.
- Full scope DA role.
- Group based nutrition interventions with MDT like group morning teas.
- Group education for malnutrition (and/or student led).
- Guilty until innocent approach for high-risk population, e.g., NOF, oncology, respiratory.
- HENS.
- HPHE educations SIMPLE messages by IDT/AHA.
- IDT/AHA? To order drinks/supplements and other, e.g., HP diets.
- Immediate education (e.g., nurse or NA or Doctor) e.g using you are at malnutrition risk sheet.
- Imprest system/or selective mid-meal trolley/medpass.
- Initial assessment [ADIME on first time seeing pt] template for “at risk” patients (i.e., short case).
- Initial adult risk ax = add in refused DN, seen by DN in community.
- Interdisciplinary mealtime assistance and/or champions (AHA/nurses/other).
- Interdisciplinary prescription with clear guidelines.
- Interdisciplinary SIMPLE malnutrition messaging.
- It’s ok not to keep individually seeing this pt WPI.
- “It’s ok not to r/v this pt if not for tube feeding” WPI.
- “It’s ok not to see this pt anymore unless you tube feed them” standardised chart entry (i.e., we are doing everything already).
- Leverage off eat/walk/engage.
- Leverage off student workforce for SIMPLE orange.
- Local interdisciplinary or delegated process to let DN know.
- Malnutrition new:r/v ratio.
- Malnutrition prevention/prehab.
- MDT or nursing assistance with supportive care at time of risk screening (education, weekly weighs, intake monitoring, mealtime assistance).
- Meal support for pts with eating disorders by NAs.
- Medical malnutrition diagnosis.
- MST triaging and confirmation of risk.
- Multimedia standard educations.
- NA advising re d/c plan, e.g., discuss with GP.
- NA assistance post d/c scripting.
- NA HPHE education.
- NA pre assessment data.
- NAs doing d/c planning under guidelines.
- NAs or nurses for preference checks/flavours.
- NEMO therapeutic diet educations.
- Nurse records estimated intake.
- Nursing/AHA/interdisciplinary to commence SIMPLE malnutrition strategies on risk ax.
- Nursing/medical/AH malnutrition diagnoses.
- Nursing or DA blood monitoring/outpatients.
- Nutrition Assistant—rescreen, basic educations, assisted diagnosis (with DN sign off), e.g., on ward round.
- Overlearning repeat basic nutrition [messages].
- Patient centred care.
- Point of risk screen interdisciplinary education including discharge planning, e.g., talk to your GP.
- Power form diagnosis auto generates medical d/c summary 1 liner.
- Process for documentation and alternative care [to individualised DN care]/simple management.
- Process to support this [DNs stopping doing reviews where low value unless escalate nutrition support is requested].
- Pt reported experience measures.
- R/v referral + triage process.
- Re-referral criteria (ok to d/c) back to supportive.
- Reviewing MDT input/opportunities/low value meetings.
- Reviews or monitoring by non-dietitians.
- Room service.
- Seeing higher priority pts, e.g., using priority tool.
- Short/abbreviated assessments for at risk/malnourished (e.g., on mealtime monitoring).
- Short case for malnutrition.
- Short cases for malnutrition.
- Short malnutrition care WPI and/or cognitively impaired malnutrition pathway.
- SIMPLE audits.
- Standardised chart entry template, e.g., for new/review.
- Standardised protocols with templates with criteria.
- Systematised intake monitoring using CBORD [food service software] and NAs for intake monitoring.
- Systematised tube feeding/algorithms.
- Telehealth to [site removed for confidentiality] with assistant.
- Using TREND [workforce planning and workload management system], using DAs, etc, to streamline intake/prioritisation/reviews.
- Utilising procedures, protocols and pathways.
| ADIME = Process of Assessment, Diagnosis, Intervention, and Monitoring/Evaluation |
| AH = Allied health |
| AHA = Allied health assistant |
| Ax = Assessment |
| d/c = Discharge |
| DA = Dietitian assistant |
| DN = Dietitian |
| GP = General practitioner |
| HENS = Home enteral nutrition support |
| HP = Health practitioner |
| HPHE = High protein high energy |
| IDT = Interdisciplinary team |
| MDT = Multi-disciplinary team |
| MST = Malnutrition screening tool |
| MST 2 = Malnutrition screening tool score of 2 |
| NA = Nutrition Assistant |
| NEMO = Nutrition education materials online |
| PFM = Patient flow manager |
| PG-SGA = Patient generated subjective global assessment |
| Pt = Patient |
| r/v = Review |
| RACF = Residential aged care facility |
| SAM = Supplements as medicine |
| SGA = Subjective global assessment |
| SIMPLE = Systematised interdisciplinary malnutrition program for implementation and evaluation |
| WPI = Workplace instruction |
References
- Adams, N.E.; Bowie, A.J.; Simmance, N.; Murray, M.; Crowe, T.C. Recognition by medical and nursing professionals of malnutrition and risk of malnutrition in elderly hospitalised patients. Nutr. Diet. 2008, 65, 144–150. [Google Scholar] [CrossRef]
- Agarwal, E.; Ferguson, M.; Banks, M.; Bauer, J.; Capra, S.; Isenring, E. Nutritional status and dietary intake of acute care patients: Results from the Nutrition Care Day Survey 2010. Clin. Nutr. 2012, 31, 41–47. [Google Scholar] [CrossRef]
- Barker, L.A.; Gout, B.S.; Crowe, T.C. Hospital Malnutrition: Prevalence, Identification and Impact on Patients and the Healthcare System. Int. J. Environ. Res. Public Health 2011, 8, 514–527. [Google Scholar] [CrossRef]
- Correia, M.I.T.D.; Waitzberg, D.L. The impact of malnutrition on morbidity, mortality, length of hospital stay and costs evaluated through a multivariate model analysis. Clin. Nutr. 2003, 22, 235–239. [Google Scholar] [CrossRef]
- Lim, S.L.; Ong, K.C.B.; Chan, Y.H.; Loke, W.C.; Ferguson, M.; Daniels, L. Malnutrition and its impact on cost of hospitalization, length of stay, readmission and 3-year mortality. Clin. Nutr. 2012, 31, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Bell, J.J.; Young, A.; Hill, J.; Banks, M.; Comans, T.; Barnes, R.; Keller, H.H. Rationale and developmental methodology for the SIMPLE approach: A Systematised, Interdisciplinary Malnutrition Pathway for impLementation and Evaluation in hospitals. Nutr. Diet. 2018, 75, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Bell, J.; Bauer, J.; Capra, S.; Pulle, C.R. Barriers to nutritional intake in patients with acute hip fracture: Time to treat malnutrition as a disease and food as a medicine? Can. J. Physiol. Pharmacol. 2013, 91, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Hand, K.R.; Abram, J.K. Describing the Roles and Responsibilities of Nutrition Staff and Nutrition Care Policies in Acute Care Facilities. Top. Clin. Nutr. 2017, 32, 176–183. [Google Scholar] [CrossRef]
- Keller, H.H.; McCullough, J.; Davidson, B.; Vesnaver, E.; Laporte, M.; Gramlich, L.; Allard, J.; Bernier, P.; Duerksen, D.; Jeejeebhoy, K. The Integrated Nutrition Pathway for Acute Care (INPAC): Building consensus with a modified Delphi. Nutr. J. 2015, 14, 63. [Google Scholar] [CrossRef]
- Porter, J.; Jamieson, R. Triaging in dietetics: Do we prioritise the right patients? Nutr. Diet. 2012, 70, 21–26. [Google Scholar] [CrossRef]
- Swan, W.I.; Vivanti, A.; Hakel-Smith, N.A.; Hotson, B.; Orrevall, Y.; Trostler, N.; Howarter, K.B.; Papoutsakis, C. Nutrition Care Process and Model Update: Toward Realizing People-Centered Care and Outcomes Management. J. Acad. Nutr. Diet. 2017, 117, 2003–2014. [Google Scholar] [CrossRef]
- Tappenden, K.A.; Quatrara, B.; Parkhurst, M.L.; Malone, A.M.; Fanjiang, G.; Ziegler, T.R. Critical role of nutrition in improving quality of care: An interdisciplinary call to action to address adult hospital malnutrition. JPEN J. Parenter. Enteral Nutr. 2013, 37, 482–497. [Google Scholar] [CrossRef]
- Bell, J.J.; Young, A.M.; Hill, J.M.; Banks, M.D.; Comans, T.A.; Barnes, R.; Keller, H.H. Systematised, Interdisciplinary Malnutrition Program for impLementation and Evaluation delivers improved hospital nutrition care processes and patient reported experiences—An implementation study. Nutr. Diet. 2021. [Google Scholar] [CrossRef] [PubMed]
- Value-Based Healthcare—Shifting from Volume to Value. Queensland Clinical Senate [Meeting Report]. April 2016. Available online: https://www.health.qld.gov.au/__data/assets/pdf_file/0028/442693/qcs-meeting-report-201603.pdf (accessed on 6 January 2019).
- Bell, J.J.; Geirsdóttir, Ó.G.; Hertz, K.; Santy-Tomlinson, J.; Skúladóttir, S.S.; Eleuteri, S.; Johansen, A. Nutritional Care of the Older Patient with Fragility Fracture: Opportunities for Systematised, Interdisciplinary Approaches Across Acute Care, Rehabilitation and Secondary Prevention Settings. In Orthogeriatrics: The Management of Older Patients with Fragility Fractures; Falaschi, P., Marsh, D., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 311–329. [Google Scholar]
- Prasad, V.; Ioannidis, J.P. Evidence-based de-implementation for contradicted, unproven, and aspiring healthcare practices. Implement. Sci. 2014, 9, 1. [Google Scholar] [CrossRef]
- Upvall, M.J.; Bourgault, A.M. De-implementation: A concept analysis. Nurs. Forum 2018, 53, 376–382. [Google Scholar] [CrossRef] [PubMed]
- van Bodegom-Vos, L.; Davidoff, F. Marang-van de Mheen, P.J. Implementation and de-implementation: Two sides of the same coin? BMJ Qual. Saf. 2017, 26, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Norton, W.E.; Kennedy, A.E.; Chambers, D.A. Studying de-implementation in health: An analysis of funded research grants. Implement. Sci. 2017, 12, 144. [Google Scholar] [CrossRef] [PubMed]
- Norton, W.E.; Chambers, D.A. Unpacking the complexities of de-implementing inappropriate health interventions. Implement. Sci. 2020, 15, 2. [Google Scholar] [CrossRef] [PubMed]
- Keller, H.; Laur, C.; Valaitis, R.; Bell, J.; McNicholl, T.; Ray, S.; Murphy, J.; Barnes, S. More-2-Eat: Evaluation protocol of a multi-site implementation of the Integrated Nutrition Pathway for Acute Care. BMC Nutr. 2017, 3, 13. [Google Scholar] [CrossRef]
- Laur, C.; Keller, H. Implementing best practice in hospital multidisciplinary nutritional care: An example of using the knowledge-to-action process for a research program. J. Multidiscip. Health 2015, 8, 463–472. [Google Scholar] [CrossRef]
- ten Cate, D.; Ettema, R.G.A.; Huisamn-de Waal, G.; Bell, J.J.; Verbrugge, R.; Schoonhoven, L.; Schuurmans, M.J.; Zwakhalen, S.; Vermeulen, H.; Ginkel, J.M.; et al. Interventions to prevent and treat malnutrition in older adults to be carried out by nurses: A systematic review. J. Clin. Nurs. 2019, 29, 1883–1902. [Google Scholar] [CrossRef]
- McMillan, S.S.; King, M.; Tully, M.P. How to use the nominal group and Delphi techniques. Int. J. Clin. Pharm. 2016, 38, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Zammit, K. Applying Thematic Analysis to Education: A Hybrid Approach to Interpreting Data in Practitioner Research. Int. J. Qual. Methods 2020, 19, 160940692091881. [Google Scholar] [CrossRef]
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef]
- Allied Health Professions’ Office of Queensland. Allied Health Expanded Scope Strategy 2016–2021; Department of Health, Clinical Excellence Division, Ed.; Queensland Health: Queensland, Australia, 2016. [Google Scholar]
- Allied Health Professions’ Office of Queensland. Allied Health Assistant Framework; Queensland Health: Queensland, Australia, 2015. [Google Scholar]
- Andersen, D.; Baird, S.; Bates, T.; Chapel, D.L.; Cline, A.D.; Ganesh, S.N.; Garner, M.; Grant, B.L.; Hamilton, K.K.; Jablonski, K.; et al. Academy of Nutrition and Dietetics: Revised 2017 Scope of Practice for the Nutrition and Dietetics Technician, Registered. J. Acad. Nutr. Diet. 2018, 118, 327–342. [Google Scholar] [CrossRef] [PubMed]
- Dietitians Association of Australia. Scope of Practice-Support Staff in Nutrition and Dietetic Services; Dietitians Association of Australia: Canberra, Australia, 2016. [Google Scholar]
- State of Queensland, Workplace Instruction (WPI3). Guidelines for Skill Sharing between Allied Health Professionals; Queensland Health, Queensland Government: Brisbane, Australia, 2013.
- The British Dietetic Association. Dietetic Support Worker & Assistant Practitioner Roles; The British Dietetic Association: Birmingham, UK, 2010. [Google Scholar]
- Queensland Health. Clinical Task Instructions. Available online: https://www.health.qld.gov.au/ahwac/html/clintaskinstructions (accessed on 2 April 2021).
- Passfield, J.; Nielsen, I.; Brebner, N.; Johnstone, C. Skill sharing and delegation practice in two Queensland regional allied health cancer care services: A comparison of tasks. Aust. Health Rev. 2018, 42, 656–660. [Google Scholar] [CrossRef] [PubMed]
- Bell, J.J.; Bauer, J.D.; Capra, S.; Pulle, R.C. Multidisciplinary, multi-modal nutritional care in acute hip fracture inpatients—Results of a pragmatic intervention. Clin. Nutr. 2014, 33, 1101–1107. [Google Scholar] [CrossRef]
- Newman, C.S.; Cornwell, P.L.; Young, A.M.; Ward, E.C.; McErlain, A.L. Accuracy and confidence of allied health assistants administering the subjective global assessment on inpatients in a rural setting: A preliminary feasibility study. Nutr. Diet. 2018, 75, 129–136. [Google Scholar] [CrossRef]
- Rushton, A.; Edwards, A.; Bauer, J.; Bell, J.J. Dietitian assistant opportunities within the nutrition care process for patients with or at risk of malnutrition: A systematic review. Nutr. Diet. 2021, 78, 69–85. [Google Scholar] [CrossRef]
- Keller, H.; Koechl, J.M.; Laur, C.; Chen, H.; Curtis, L.; Dubin, J.A.; Gramlich, L.; Ray, S.; Valaitis, R.; Yang, Y.; et al. More-2-Eat implementation demonstrates that screening, assessment and treatment of malnourished patients can be spread and sustained in acute care; a multi-site, pretest post-test time series study. Clin. Nutr. 2021, 40, 2100–2108. [Google Scholar] [CrossRef]
- Keller, H.H.; Valaitis, R.; Laur, C.V.; McNicholl, T.; Xu, Y.; Dubin, J.A.; Curtis, L.; Obiorah, S.; Ray, S.; Bernier, P.; et al. Multi-site implementation of nutrition screening and diagnosis in medical care units: Success of the More-2-Eat project. Clin. Nutr. 2019, 38, 897–905. [Google Scholar] [CrossRef]
- State-Wide Professional Group for Dietetics Queensland. Clinical Task Instruction: D-DN04 Administer the Subjective Global Assessment (SGA); Queensland, Allied Health Professions Office of Queensland, Ed.; Queensland Health: Queensland, Australia, 2018. [Google Scholar]
- Bell, J.J.; Bauer, J.; Capra, S.; Pulle, R.C. Quick and Easy Is Not without Cost: Implications of Poorly Performing Nutrition Screening Tools in Hip Fracture. J. Am. Geriatr. Soc. 2014, 62, 237–243. [Google Scholar] [CrossRef]
- Chima, C.S.; Dietz-Seher, C.; Kushner-Benson, S. Nutrition Risk Screening in Acute Care: A Survey of Practice. Nutr. Clin. Pract. 2008, 23, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Field, L.B.; Hand, R.K. Differentiating Malnutrition Screening and Assessment: A Nutrition Care Process Perspective. J. Acad. Nutr. Diet. 2015, 115, 824–828. [Google Scholar] [CrossRef]
- Gibson, S.; Sequeira, J.; Cant, R.; Ku, C. Identifying malnutrition risk in acute medical patients: Validity and utility of Malnutrition Universal Screening Tool and Modified Malnutrition Screening Tool. Nutr. Diet. 2012, 69, 309–314. [Google Scholar] [CrossRef]
- Laporte, M.; Keller, H.H.; Payette, H.; Allard, J.P.; Duerksen, D.R.; Bernier, P.; Jeejeebhoy, K.; Gramlich, L.; Davidson, B.; Vesnaver, E.; et al. Validity and reliability of the new Canadian Nutrition Screening Tool in the ‘real-world’ hospital setting. Eur. J. Clin. Nutr. 2014, 69, 558–564. [Google Scholar] [CrossRef] [PubMed]
- Wester, P.; Angus, R.; Easlea, D.; Lin, M.; Chen, B.; Bisset, L. Use of the malnutrition screening tool by non-dietitians to identify at-risk patients in a rehabilitation setting: A validation study. Nutr. Diet. 2018, 75, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Graham, I.D.; Logan, J.; Harrison, M.B.; Straus, S.E.; Tetroe, J.; Caswell, W.; Robinson, N. Lost in knowledge translation: Time for a map? J. Contin. Educ. Health Prof. 2006, 26, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Cane, J.; O’Connor, D.; Michie, S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement. Sci. 2012, 7, 37. [Google Scholar] [CrossRef]
- French, S.D.; E Green, S.; O’Connor, D.A.; E McKenzie, J.; Francis, J.J.; Michie, S.; Buchbinder, R.; Schattner, P.; Spike, N.; Grimshaw, J.M. Developing theory-informed behaviour change interventions to implement evidence into practice: A systematic approach using the Theoretical Domains Framework. Implement. Sci. 2012, 7, 38. [Google Scholar] [CrossRef]
- Michie, S.; Van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef]
- Laur, C.; Bell, J.; Valaitis, R.; Ray, S.; Keller, H. The Sustain and Spread Framework: Strategies for sustaining and spreading nutrition care improvements in acute care based on thematic analysis from the More-2-Eat study. BMC Health Serv. Res. 2018, 18, 930. [Google Scholar] [CrossRef] [PubMed]
- Nilsen, P.; Roback, K.; Broström, A.; Ellström, P.-E. Creatures of habit: Accounting for the role of habit in implementation research on clinical behavior change. Implement. Sci. 2012, 7, 53. [Google Scholar] [CrossRef]
- Potthoff, S.; Presseau, J.; Sniehotta, F.F.; Johnston, M.; Elovainio, M.; Avery, L. Planning to be routine: Habit as a mediator of the planning-behaviour relationship in healthcare professionals. Implement. Sci. 2017, 12, 24. [Google Scholar] [CrossRef] [PubMed]
- Ray, J.M.; Ratwani, R.M.; A Sinsky, C.; Frankel, R.M.; Friedberg, M.; Powsner, S.M.; I Rosenthal, D.; Wachter, R.M.; Melnick, E.R. Six habits of highly successful health information technology: Powerful strategies for design and implementation. J. Am. Med. Inform. Assoc. 2019, 26, 1109–1114. [Google Scholar] [CrossRef] [PubMed]
- Laur, C.; Valaitis, R.; Bell, J.; Keller, H. Changing nutrition care practices in hospital: A thematic analysis of hospital staff perspectives. BMC Health Serv. Res. 2017, 17, 498. [Google Scholar] [CrossRef]
- Delbecq, A.L.; Van de Ven, A.H.; Gustafson, D.H.; Group Techniques for Program. Planning: A Guide to Nominal Group and Delphi Processes. J. Appl. Behav. Sci. 1976, 12, 581. [Google Scholar]
- U.S. Department of Health and Human Services. Gaining Consensus among Stakeholders through the Nominal Group Technique; Centers for Disease Control and Prevention, Ed.; U.S. Department of Health and Human Services: Washington, DC, USA, 2018.


{kind=link}
| Demographic/Variable | n (%) |
|---|---|
| Position/role | |
| Dietitian | 44 (70) |
| Assistant | 12 (19) |
| Director | 4 (6) |
| Student dietitians | 3 (5) |
| Gender * | |
| Male | 7 (14) |
| Female | 42 (86) |
| Age group ** | |
| <30 | 11 (26) |
| 30–39 | 13 (31) |
| 40–49 | 11 (26) |
| 50–59 | 5 (12) |
| 60+ | 2 (5) |
| Employment contract ** | |
| Full time | 34 (81) |
| Part time | 8 (19) |
| Casual | 0 (0) |
| Number of years practicing *** | |
| <2 yrs | 3 (6) |
| 2–5 yrs | 16 (33) |
| 6–10 yrs | 13 (27) |
| 11–20 yrs | 9 (19) |
| 21–30 yrs | 6 (13) |
| 31+ yrs | 1 (2) |
| NCP Step (Theme) | n (%) |
|---|---|
| Screening | 5 (5) |
| Assessment | 31 (31) |
| Diagnosis | 2 (2) |
| Care planning and intervention | 45 (44) |
| Monitoring and evaluation | 18 (18) |
| NCP Step Theme and Categories | Votes n (%) |
|---|---|
| Screening | 19 |
| Low value dietetics malnutrition screening | 19 (100) |
| Assessment | 54 |
| Patients with malnutrition screen score 2 by dietitian | 22 (41) |
| Comprehensive, individualised nutrition assessments where unlikely to add value | 15 (27) |
| Dietitian assessment prior to delegation | 4 (7) |
| Diagnosis | 5 |
| Dietitian malnutrition diagnosis | 5 (100) |
| Care planning and intervention | 58 |
| Intervention—Food and nutrient delivery | |
| Supplements As Medicine (SAM) by dietitian | 5 (7) |
| Intervention—education | |
| Education by dietitian to patients | 28 (41) |
| Intervention—coordinated care | |
| Low value dietitian intervention—coordination of care | 5 (7) |
| Dietitian discharge handover low risk patient | 4 (6) |
| Intervention—multicomponent | |
| Low value dietitian intervention [broad] | 8 (12) |
| Monitoring and evaluation | |
| Low value reviews | 32 (70) |
| Preference checks | 11 (16) |
| Intake reviews by dietitian | 10 (21) |
| NCP Step (Theme) | n (%) |
|---|---|
| Screening | 8 (7) |
| Assessment | 11 (10) |
| Diagnosis | 4 (4) |
| Care planning and intervention | 75 (66) |
| Monitoring and evaluation | 15 (13) |
| NCP Step Theme and Categories | Votes n (%) |
|---|---|
| Screening | 17 |
| Triaging processes | 9 (53) |
| Delegated/skill shared nutrition care process for at risk patients who do not require specialized care | 4 (24) |
| Assessment | 22 |
| Assistant assessment data | 10 (45) |
| Clinical governance—triaging | 7 (32) |
| Clinical governance—assessment | 4 (18) |
| Diagnosis | 8 |
| Delegated/skill shared diagnosis | 8 (100) |
| Care planning and intervention | 157 |
| Intervention—Food and nutrient delivery | |
| Delegated/skill shared supportive food/fluids | 14 (9) |
| Food service system | 5 (3) |
| Intervention—education | |
| Delegated/skill shared education | 24 (15) |
| Patient engagement | 5 (3) |
| Intervention—coordinated care | |
| Mealtime assistance | 13 (8) |
| Systematised processes to support integrated care | 12 (8) |
| Intervention—multicomponent | |
| Delegated/skill shared nutrition care processes for at risk patients who do not require specialized care | 55 (35) |
| Abbreviated malnutrition care processes where clinically appropriate | 23 (15) |
| Monitoring and evaluation | |
| Clinical governance—monitoring and evaluation | 11 (44) |
| Delegated/skill shared monitoring | 10 (40) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rushton, A.; Elmas, K.; Bauer, J.; Bell, J.J. Identifying Low Value Malnutrition Care Activities for De-Implementation and Systematised, Interdisciplinary Alternatives—A Multi-Site, Nominal Group Technique Approach. Nutrients 2021, 13, 2063. https://doi.org/10.3390/nu13062063
Rushton A, Elmas K, Bauer J, Bell JJ. Identifying Low Value Malnutrition Care Activities for De-Implementation and Systematised, Interdisciplinary Alternatives—A Multi-Site, Nominal Group Technique Approach. Nutrients. 2021; 13(6):2063. https://doi.org/10.3390/nu13062063
Chicago/Turabian StyleRushton, Alita, Kai Elmas, Judith Bauer, and Jack J. Bell. 2021. "Identifying Low Value Malnutrition Care Activities for De-Implementation and Systematised, Interdisciplinary Alternatives—A Multi-Site, Nominal Group Technique Approach" Nutrients 13, no. 6: 2063. https://doi.org/10.3390/nu13062063
APA StyleRushton, A., Elmas, K., Bauer, J., & Bell, J. J. (2021). Identifying Low Value Malnutrition Care Activities for De-Implementation and Systematised, Interdisciplinary Alternatives—A Multi-Site, Nominal Group Technique Approach. Nutrients, 13(6), 2063. https://doi.org/10.3390/nu13062063