
Global Trends (1961–2017) in Human Dietary Potassium Supplies



Abstract
1. Introduction
2. Materials and Methods
2.1. Demographic Data
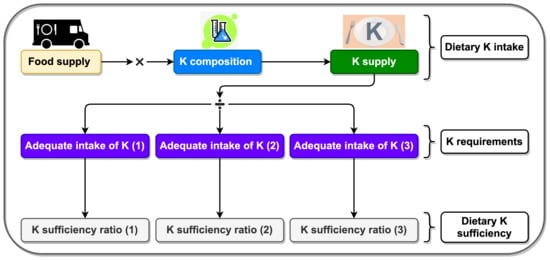
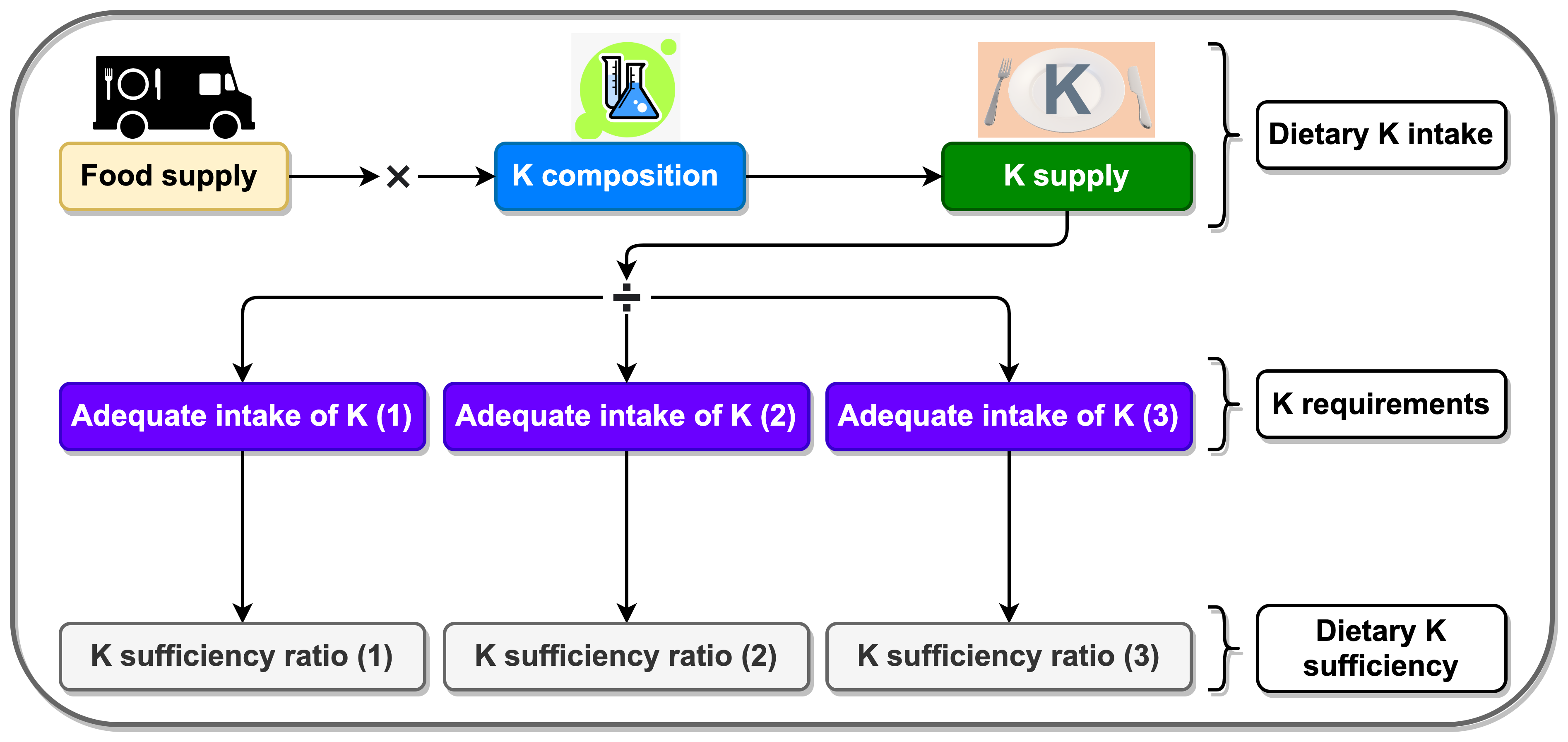
2.2. Dietary Supplies of Potassium (DSK)
2.3. Potassium Requirement
2.4. Potassium (K) Sufficiency Ratio
2.5. Data Analyses and Visualisation
3. Results
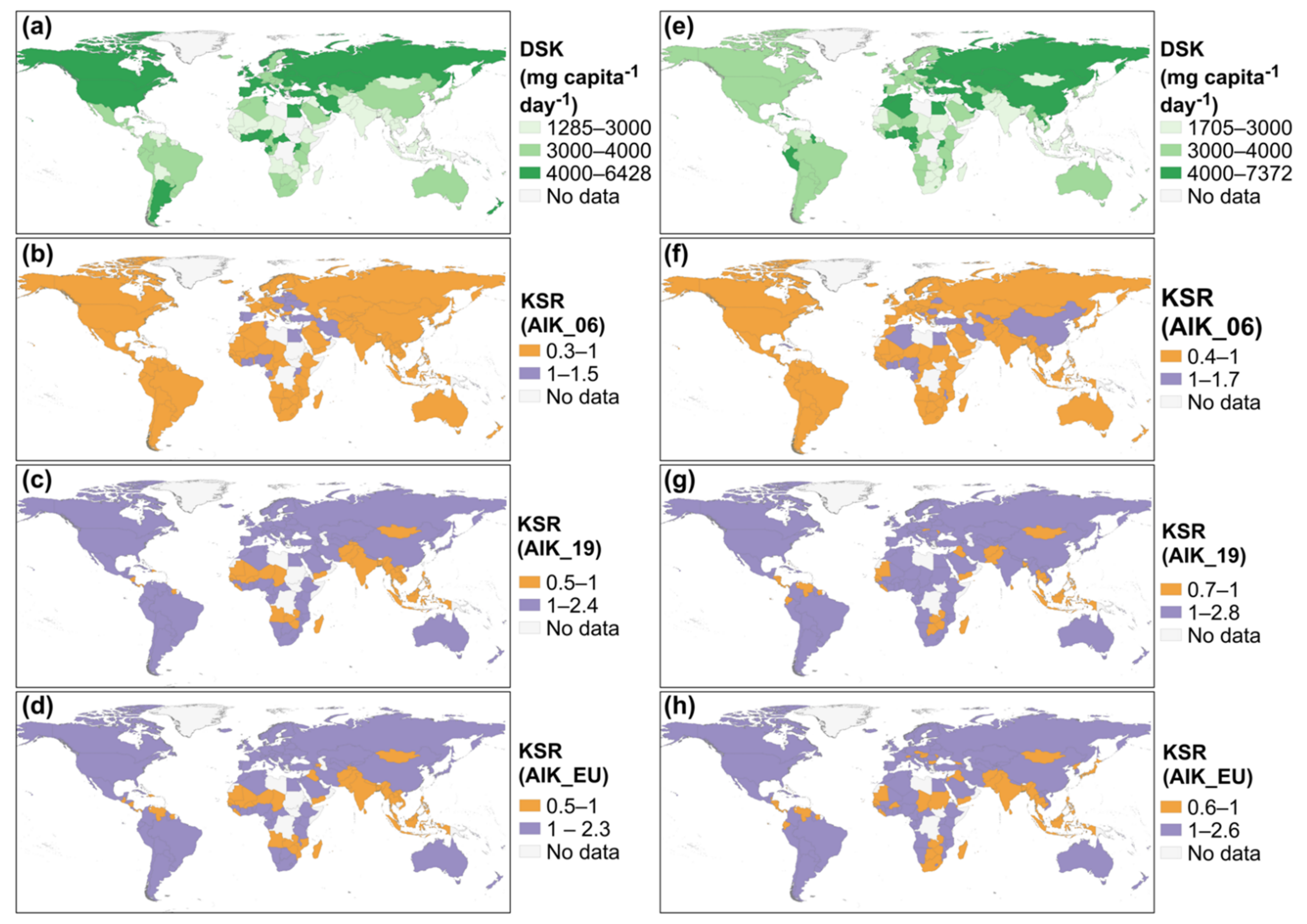
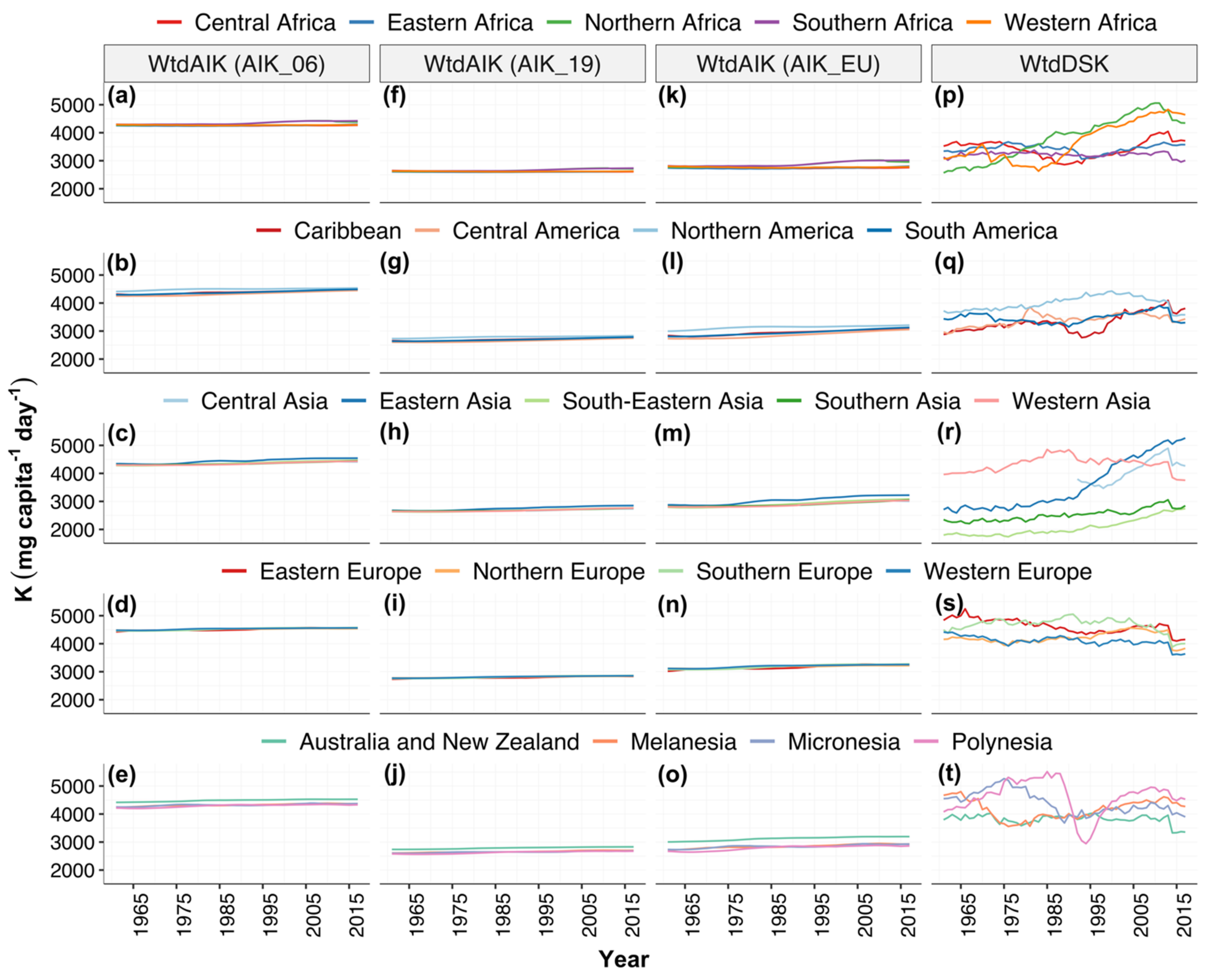
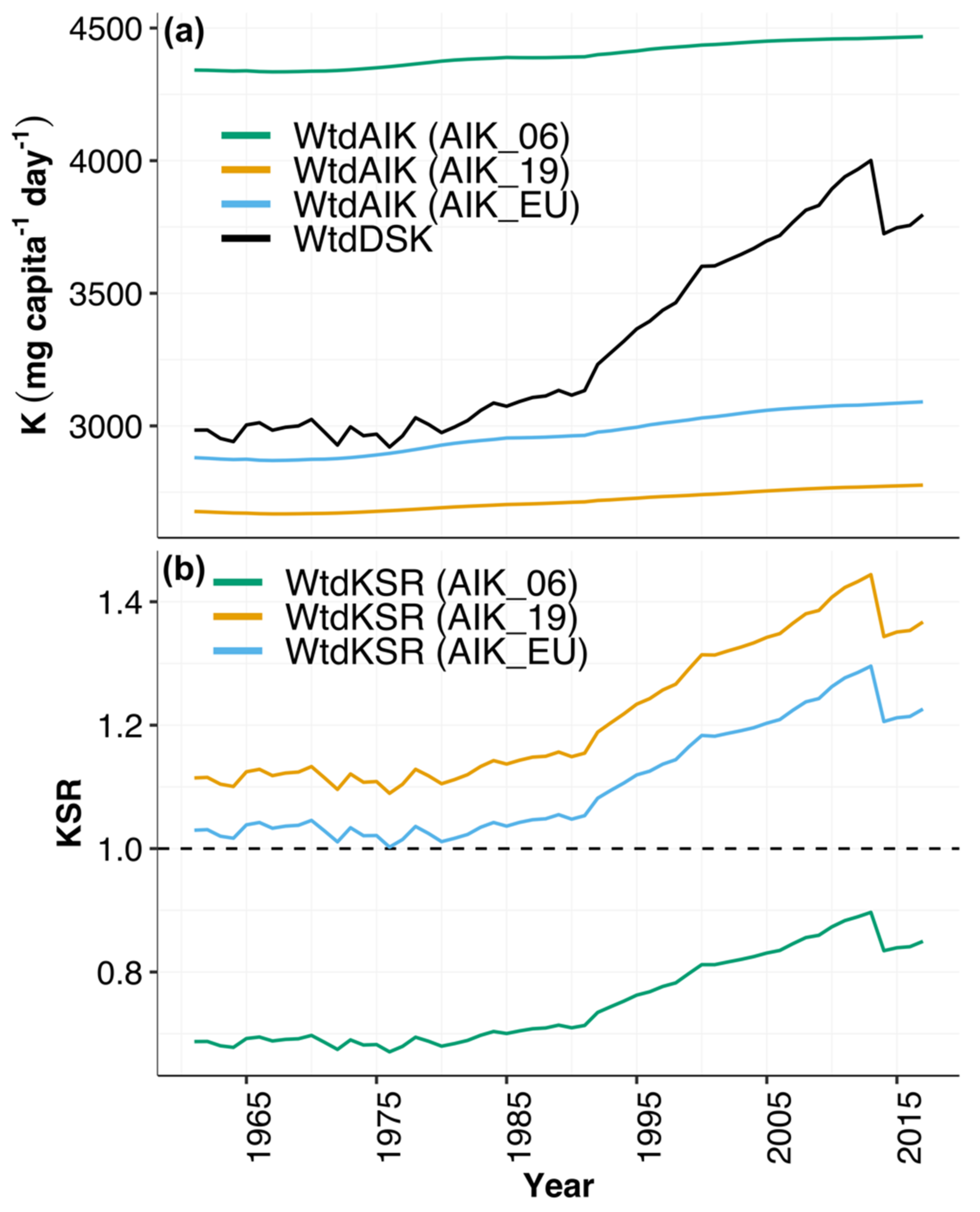
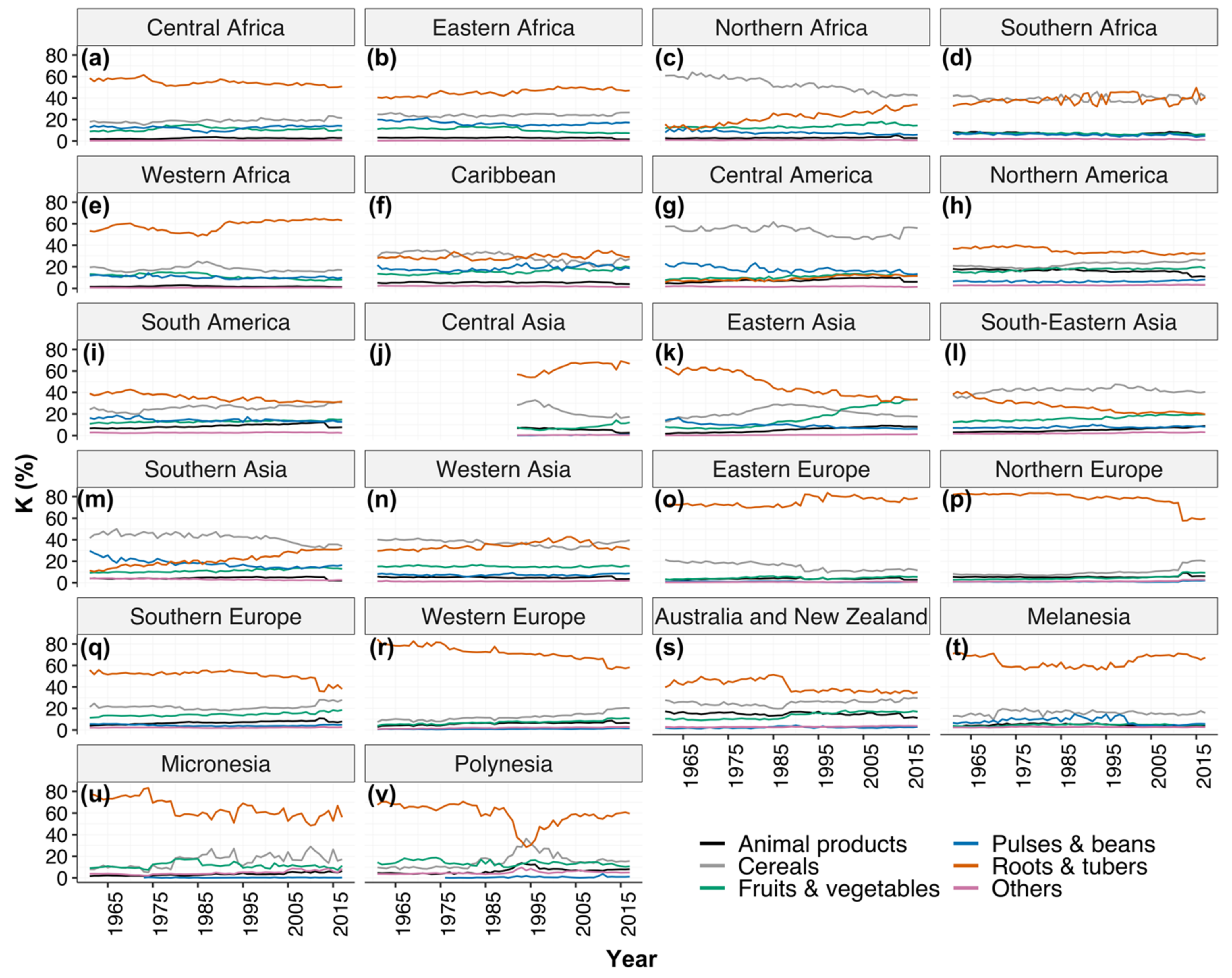
3.1. Dietary Potassium (K) Supplies and Requirements
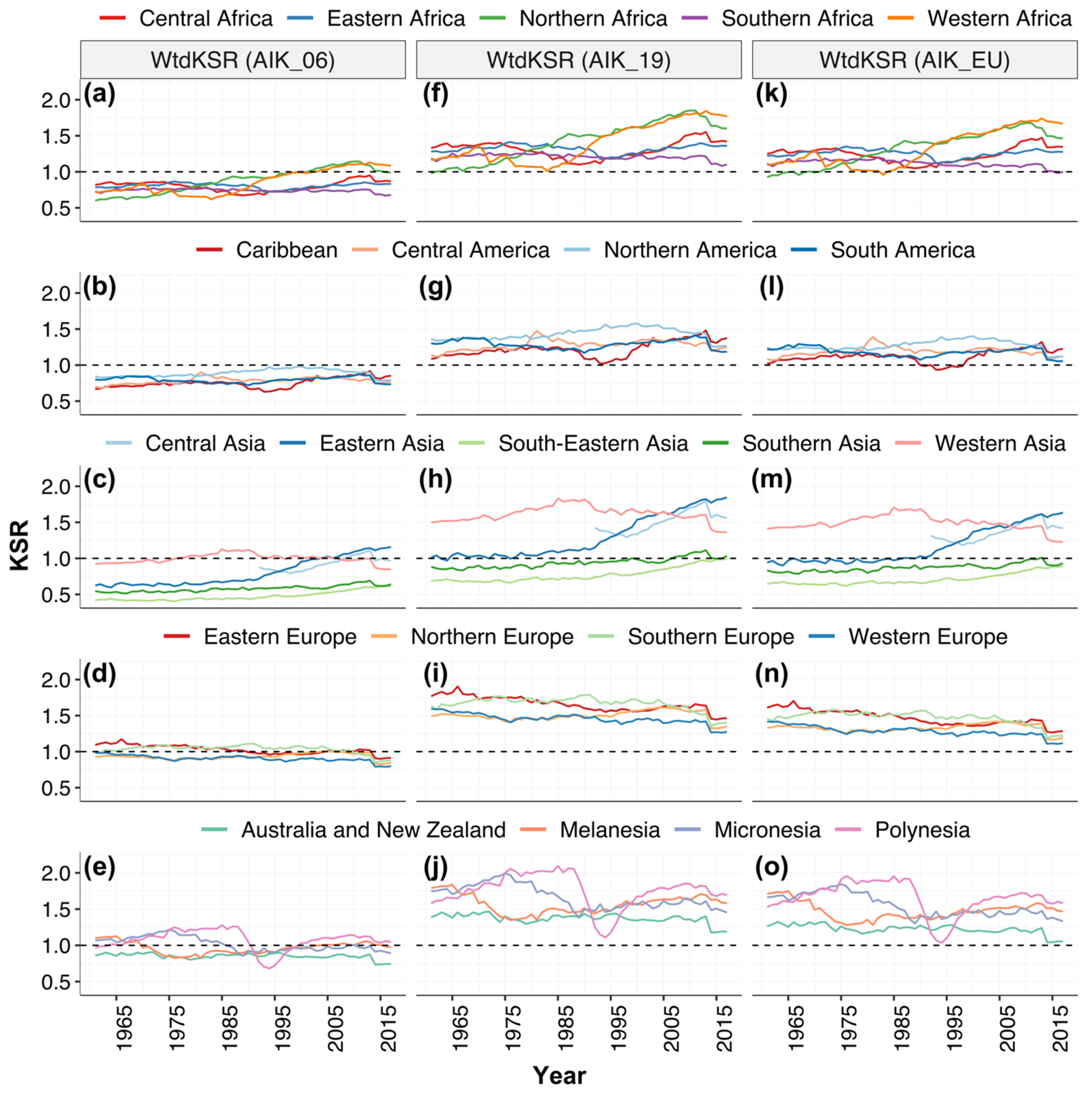
3.2. Potassium Sufficiency Ratio (KSR)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Palmer, B.F. Regulation of potassium homeostasis. Clin. J. Am. Soc. Nephrol. 2015, 10, 1050–1060. [Google Scholar] [CrossRef] [PubMed]
- Turck, D.; Bresson, J.L.; Burlingame, B.; Dean, T.; Fairweather-Tait, S.; Heinonen, M.; Hirsch-Ernst, K.I.; Mangelsdorf, I.; McArdle, H.; Neuhäuser-Berthold, M. Dietary reference values for potassium. EFSA J. 2016, 14. [Google Scholar] [CrossRef]
- Weaver, C.M. Potassium and health. Adv. Nutr. 2013, 4, 368S–377S. [Google Scholar] [CrossRef] [PubMed]
- Viera, A.J.; Wouk, N. Potassium Disorders: Hypokalemia and Hyperkalemia. Am. Fam. Physician 2015, 92, 487–495. [Google Scholar]
- Haddy, F.J.; Vanhoutte, P.M.; Feletou, M. Role of potassium in regulating blood flow and blood pressure. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2006, 290, R546–R552. [Google Scholar] [CrossRef] [PubMed]
- Salomonsson, M.; Brasen, J.C.; Sorensen, C.M. Role of renal vascular potassium channels in physiology and pathophysiology. Acta Physiol. 2017, 221, 14–31. [Google Scholar] [CrossRef]
- Kong, S.H.; Kim, J.H.; Hong, A.R.; Lee, J.H.; Kim, S.W.; Shin, C.S. Dietary potassium intake is beneficial to bone health in a low calcium intake population: The Korean National Health and Nutrition Examination Survey (KNHANES) (2008–2011). Osteoporos. Int. 2017, 28, 1577–1585. [Google Scholar] [CrossRef]
- Newberry, S.J.; Chung, M.; Anderson, C.A.M.; Chen, C.; Fu, Z.; Tang, A.; Zhao, N.; Booth, M.; Marks, J.; Hollands, S.; et al. AHRQ comparative effectiveness reviews. In Sodium and Potassium Intake: Effects on Chronic Disease Outcomes and Risks; AHRQ Comparative Effectiveness Reviews; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2018. [Google Scholar]
- IOM. Dietary Reference Intakes: The Essential Guide to Nutrient Requirements; Otten, J.J., Hellwig, J.P., Meyers, L.D., Eds.; National Academies Press: Washington, DC, USA, 2006. [Google Scholar]
- World Health Organization. Guideline: Potassium Intake for Adults and Children; World Health Organization: Geneva, Switzerland, 2012. [Google Scholar]
- Broadley, M.R.; White, P.J. Eats roots and leaves. Can edible horticultural crops address dietary calcium, magnesium and potassium deficiencies? Proc. Nutr. Soc. 2010, 69, 601–612. [Google Scholar] [CrossRef]
- Rosanoff, A.; Kumssa, D.B. Impact of rising body weight and cereal grain food processing on human magnesium nutrition. Plant Soil 2020, 5–23. [Google Scholar] [CrossRef]
- Du, S.; Wang, H.; Zhang, B.; Popkin, B.M. Dietary potassium intake remains low and sodium Iitake remains high, and most sodium is derived from home food preparation for Chinese adults, 1991–2015 trends. J. Nutr. 2020, 150, 1230–1239. [Google Scholar] [CrossRef]
- Rauber, F.; Da Costa Louzada, M.L.; Steele, E.M.; Millett, C.; Monteiro, C.A.; Levy, R.B. Ultra-processed food consumption and chronic non-communicable diseases-related dietary nutrient profile in the UK (2008–2014). Nutrients 2018, 10, 587. [Google Scholar] [CrossRef]
- Brown, I.J.; Tzoulaki, I.; Candeias, V.; Elliott, P. Salt intakes around the world: Implications for public health. Int. J. Epidemiol. 2009, 38, 791–813. [Google Scholar] [CrossRef]
- Sun, H.; Weaver, C.M. Rise in potassium deficiency in the US population links to agriculture practices and dietary potassium deficits. J. Agric. Food Chem. 2020, 68, 11121–11127. [Google Scholar] [CrossRef]
- He, F.J.; MacGregor, G.A. Beneficial effects of potassium on human health. Physiol. Plant 2008, 133, 725–735. [Google Scholar] [CrossRef]
- Sebastian, A.; Frassetto, L.A.; Sellmeyer, D.E.; Morris, R.C. The evolution-informed optimal dietary potassium intake of human beings greatly exceeds current and recommended intakes. Semin. Nephrol. 2006, 26, 447–453. [Google Scholar] [CrossRef] [PubMed]
- Millen, B.E.; Abrams, S.; Adams-Campbell, L.; Anderson, C.A.; Brenna, J.T.; Campbell, W.W.; Clinton, S.; Hu, F.; Nelson, M.; Neuhouser, M.L.; et al. The 2015 dietary guidelines advisory committee scientific report: Development and major conclusions. Adv. Nutr. 2016, 7, 438–444. [Google Scholar] [CrossRef] [PubMed]
- National Academies of Sciences, Engineering, and Medicine. Dietary Reference Intakes for Sodium and Potassium; National Academies Press: Washington, DC, USA, 2019. [Google Scholar]
- IOM. Dietary Reference Intakes: Applications in Dietary Assessment; The National Academies Press: Washington, DC, USA, 2000. [Google Scholar]
- Kumssa, D.B.; Joy, E.J.; Ander, E.L.; Watts, M.J.; Young, S.D.; Walker, S.; Broadley, M.R. Dietary calcium and zinc deficiency risks are decreasing but remain prevalent. Sci. Rep. 2015, 5, 10974. [Google Scholar] [CrossRef] [PubMed]
- Kumssa, D.B.; Joy, E.J.M.; Ander, E.L.; Watts, M.J.; Young, S.D.; Rosanoff, A.; White, P.J.; Walker, S.; Broadley, M.R. Global magnesium supply in the food chain. Crop. Pasture Sci. 2015, 66, 1278–1289. [Google Scholar] [CrossRef]
- UN. World Population Prospects 2019. Available online: https://population.un.org/wpp/Download/Standard/Population/ (accessed on 6 October 2020).
- FAO. FAOSTAT Data: Food Balance. Available online: http://www.fao.org/faostat/en/#data (accessed on 6 October 2020).
- USDA. USDA National Nutrient Database for Standard Reference, Release 26. Available online: http://www.ars.usda.gov/ba/bhnrc/ndl (accessed on 20 November 2020).
- IBM Corp. IBM SPSS Statistics for Macintosh; Version 27.0.; IBM Corp: Armonk, NY, USA, 2020. [Google Scholar]
- QGIS Development Team. QGIS, Version 3.16-Hannover; Open-Source Geospatial Foundation Project. Available online: https://qgis.org/en/site/ (accessed on 20 November 2020).
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis, 2nd ed.; Springer International Publishing: Houston, TX, USA, 2016. [Google Scholar]
- R Core Team. A Language and Environment of Statistical Computing; R Core Team: Vienna, Austria, 2020. [Google Scholar]
- Wessells, K.R.; Brown, K.H. Estimating the global prevalence of zinc deficiency: Results based on zinc availability in national food supplies and the prevalence of stunting. PLoS ONE 2012, 7, e50568. [Google Scholar] [CrossRef]
- Joy, E.J.M.; Young, S.D.; Black, C.R.; Ander, E.L.; Watts, M.J.; Broadley, M.R. Risk of dietary magnesium deficiency is low in most African countries based on food supply data. Plant Soil 2012, 368, 129–137. [Google Scholar] [CrossRef]
- Paice, B.J.; Paterson, K.R.; Onyanga-Omara, F.; Donnelly, T.; Gray, J.M.; Lawson, D.H. Record linkage study of hypokalaemia in hospitalized patients. Postgrad. Med. J. 1986, 62, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Favaloro, E.J.; Montagnana, M.; Guidi, G.C. Prevalence of hypokalaemia: The experience of a large academic hospital. Intern. Med. J. 2010, 40, 315–316. [Google Scholar] [CrossRef] [PubMed]
- Filippini, T.; Violi, F.; D’Amico, R.; Vinceti, M. The effect of potassium supplementation on blood pressure in hypertensive subjects: A systematic review and meta-analysis. Int. J. Cardiol. 2017, 230, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, H.O.; Nicolson, D.J.; Campbell, F.; Beyer, F.R.; Mason, J. Potassium supplementation for the management of primary hypertension in adults. Cochrane Database Syst. Rev. 2006, CD004641. [Google Scholar] [CrossRef]
- Filippini, T.; Naska, A.; Kasdagli, M.I.; Torres, D.; Lopes, C.; Carvalho, C.; Moreira, P.; Malavolti, M.; Orsini, N.; Whelton, P.K.; et al. Potassium intake and blood pressure: A dose-response meta-analysis of randomized controlled trials. J. Am. Heart Assoc. 2020, 9, e015719. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guideline: Sodium Intake for Adults and Children; World Health Organization: Geneva, Swizerland, 2012. [Google Scholar]
- Jung, S.; Kim, M.K.; Shin, J.; Choi, B.Y.; Lee, Y.H.; Shin, D.H.; Shin, M.H. High sodium intake and sodium to potassium ratio may be linked to subsequent increase in vascular damage in adults aged 40 years and older: The Korean multi-rural communities cohort (MRCohort). Eur. J. Nutr. 2019, 58, 1659–1671. [Google Scholar] [CrossRef]
- Binia, A.; Jaeger, J.; Hu, Y.; Singh, A.; Zimmermann, D. Daily potassium intake and sodium-to-potassium ratio in the reduction of blood pressure: A meta-analysis of randomized controlled trials. J. Hypertens. 2015, 33, 1509–1520. [Google Scholar] [CrossRef]
- Thout, S.R.; Santos, J.A.; McKenzie, B.; Trieu, K.; Johnson, C.; McLean, R.; Arcand, J.; Campbell, N.R.C.; Webster, J. The Science of Salt: Updating the evidence on global estimates of salt intake. J. Clin. Hypertens. 2019, 21, 710–721. [Google Scholar] [CrossRef]
- NHANES. Nutrient Intakes from Food and Beverages: Mean Amounts Consumed per Indvidual by Gender and Age, in the United States, 2017–2018. Available online: https://www.ars.usda.gov/ARSUserFiles/80400530/pdf/1718/tables_1-56_2017-2018.pdf (accessed on 3 March 2021).
- Sekula, W.; Becker, W.; Trichopoulou, A.; Zajkas, G. Comparison of dietary data from different sources: Some examples. WHO Reg. Publ. Eur. Ser. 1991, 34, 91–117. [Google Scholar]
- Archer, E.; Hand, G.A.; Blair, S.N. Validity of U.S. nutritional surveillance: National Health and Nutrition Examination Survey caloric energy intake data, 1971–2010. PLoS ONE 2013, 8, e76632. [Google Scholar] [CrossRef]
- Aleksandrowicz, L.; Tak, M.; Green, R.; Kinra, S.; Haines, A. Comparison of food consumption in Indian adults between national and sub-national dietary data sources. Br. J. Nutr. 2017, 117, 1013–1019. [Google Scholar] [CrossRef]
- Gashu, D.; Lark, R.M.; Milne, A.E.; Amede, T.; Bailey, E.H.; Chagumaira, C.; Dunham, S.J.; Gameda, S.; Kumssa, D.B.; Mossa, A.W.; et al. Spatial prediction of the concentration of selenium (Se) in grain across part of Amhara Region, Ethiopia. Sci. Total Environ. 2020, 733, 139231. [Google Scholar] [CrossRef]
- Ligowe, I.S.; Phiri, F.P.; Ander, E.L.; Bailey, E.H.; Chilimba, A.D.C.; Gashu, D.; Joy, E.J.M.; Lark, R.M.; Kabambe, V.; Kalimbira, A.A.; et al. Selenium deficiency risks in sub-Saharan African food systems and their geospatial linkages. Proc. Nutr. Soc. 2020, 1–11. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Life-Stage Group | Age | AIK (mg capita−1 day−1) | |||
|---|---|---|---|---|---|
| AIK_06 | AIK_19 | AIK_EU | WHO | ||
| Infants | 0–6 months | 400 | 400 | ||
| 7–12 months | 700 | 860 | 750 | ||
| Children | 1–3 years | 3000 | 2000 | 1100 | |
| 4–8 years | 3800 | 2300 | 1800 | ||
| Males | 9–13 years | 4500 | 2500 | 2700 | |
| 14–18 years | 4700 | 3000 | 3500 | 3510 | |
| 19–30 years | 4700 | 3400 | 3500 | 3510 | |
| 31–50 years | 4700 | 3400 | 3500 | 3510 | |
| 51–70 years | 4700 | 3400 | 3500 | 3510 | |
| >70 years | 4700 | 3400 | 3500 | 3510 | |
| Females | 9–13 years | 4500 | 2300 | 2700 | |
| 14–18 years | 4700 | 2300 | 3500 | 3510 | |
| 19–30 years | 4700 | 2600 | 3500 | 3510 | |
| 31–50 years | 4700 | 2600 | 3500 | 3510 | |
| 51–70 years | 4700 | 2600 | 3500 | 3510 | |
| >70 years | 4700 | 2600 | 3500 | 3510 | |
| Pregnancy | 14–18 years | 4700 | 2600 | 3500 | |
| 19–30 years | 4700 | 2900 | 3500 | ||
| 31–50 years | 4700 | 2900 | 3500 | ||
| Lactation | 14–18 years | 5100 | 2500 | 4000 | |
| 19–30 years | 5100 | 2800 | 4000 | ||
| 31–50 years | 5100 | 2800 | 4000 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kumssa, D.B.; Joy, E.J.M.; Broadley, M.R. Global Trends (1961–2017) in Human Dietary Potassium Supplies. Nutrients 2021, 13, 1369. https://doi.org/10.3390/nu13041369
Kumssa DB, Joy EJM, Broadley MR. Global Trends (1961–2017) in Human Dietary Potassium Supplies. Nutrients. 2021; 13(4):1369. https://doi.org/10.3390/nu13041369
Chicago/Turabian StyleKumssa, Diriba B., Edward J. M. Joy, and Martin R. Broadley. 2021. "Global Trends (1961–2017) in Human Dietary Potassium Supplies" Nutrients 13, no. 4: 1369. https://doi.org/10.3390/nu13041369
APA StyleKumssa, D. B., Joy, E. J. M., & Broadley, M. R. (2021). Global Trends (1961–2017) in Human Dietary Potassium Supplies. Nutrients, 13(4), 1369. https://doi.org/10.3390/nu13041369