
Effectiveness of Breastfeeding Support Packages in Low- and Middle-Income Countries for Infants under Six Months: A Systematic Review




Abstract

1. Introduction
- (1)
- identify and describe details of currently available breastfeeding support packages from LMICs for infants < 6 m,
- (2)
- assess the impact of breastfeeding support packages on breastfeeding practices, and
- (3)
- assess the impact of existing breastfeeding support packages on the knowledge/skills/practices of healthcare staff and caregivers.
2. Methods
2.1. Search Strategy
2.2. Eligibility Criteria
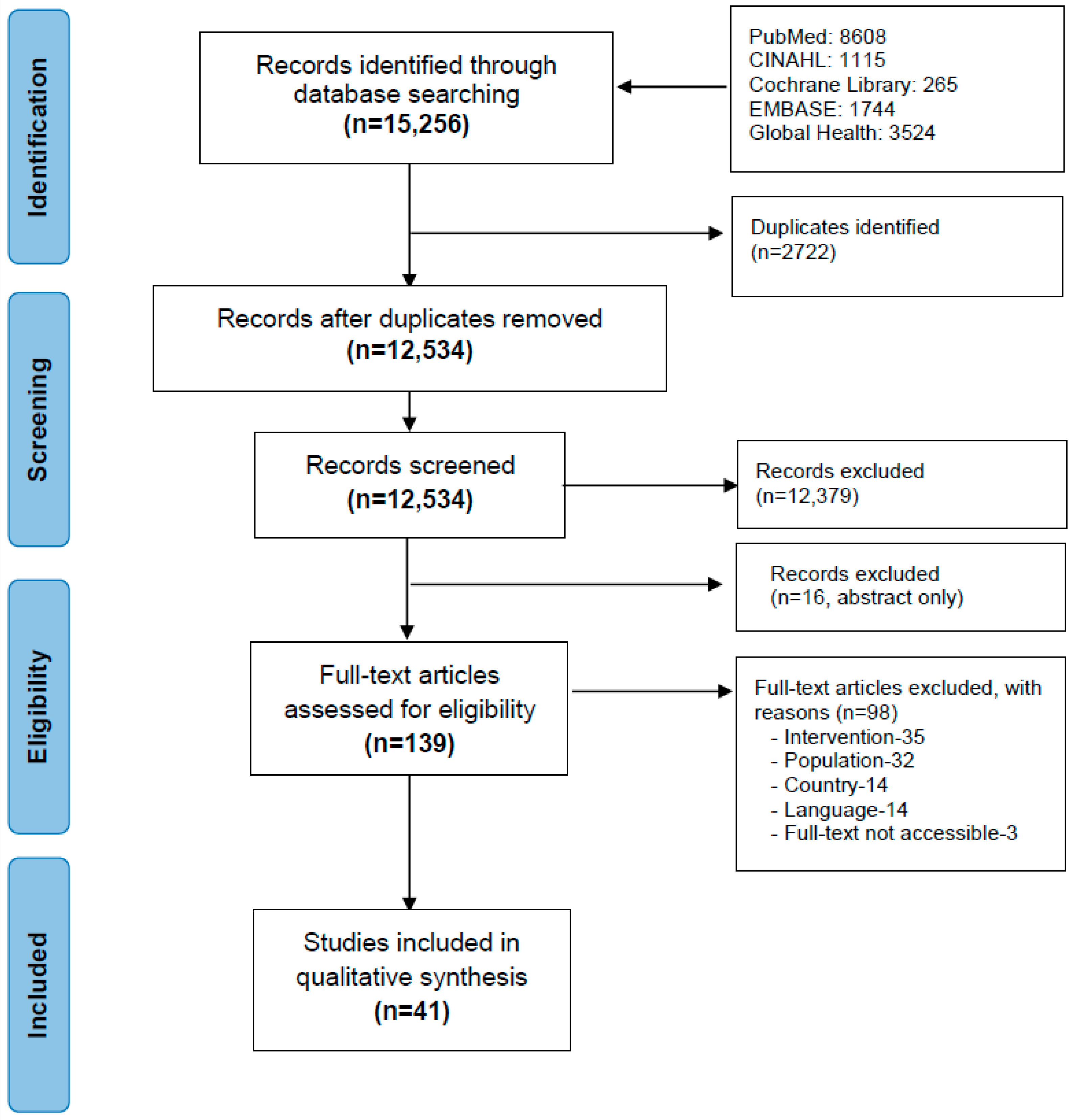
2.3. Study Selection
2.4. Quality Assessment
2.5. Data Extraction
2.6. Analysis and Reporting
2.7. Ethics Approval
3. Results
3.1. General Characteristics of the Included Studies
3.2. Breastfeeding Interventions and Their Effect on Various Outcomes
3.2.1. Breastfeeding Practices
3.2.2. Caregivers’ Knowledge/Skills/Practices
3.2.3. Healthcare Staff Knowledge/Skills/Practices
3.2.4. Morbidity
3.2.5. Anthropometry
4. Discussion
4.1. Summary of Key Findings
4.2. This Review’s Findings in Context
4.3. Limitations and Strengths
4.4. Implications for Practice and Research
- (1)
- Which factors are associated with morbidity (diarrhea, respiratory illness, and hospitalisation) and growth failure among infants < 6 m who are exclusively breastfed.
- (2)
- Which breastfeeding interventions are effective in improving breastfeeding practices and associated morbidity/mortality outcomes for particularly at-risk infants (premature babies, preterm, LWB, twin babies, or babies with anthropometric deficits/growth failure).
- (3)
- Which breastfeeding training interventions are most effective in improving the healthcare staffs’ knowledge/skills/practices, (and what are essential features/characteristics of those interventions).
- (4)
- Which breastfeeding support packages are most valued by mothers/carers and why (e.g., maternal perceptions of value might also focus on time needed to attend; confidence gained during engagement; perception of being well supported by a particular intervention).
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations and Acronyms
| AG | Adolescent girls |
| BASNEF | Beliefs, Attitudes, Subjective Norms and Enabling Factors |
| BF | Breastfeeding |
| BHFI | Baby Friendly Hospital Initiative |
| CG | Control group |
| CHW | Community Health Worker |
| CI | Confidence interval |
| CM | Community mobilisation |
| CMAM | Community based Management of Acute Malnutrition |
| CV | Community volunteer |
| EBF | Exclusive breastfeeding |
| EIBF | Early initiation of breastfeeding |
| FBSIC | Facility based semi-intensive counselling |
| HAZ | Height-for-Age z-score |
| HBIC | Home based intensive counselling |
| HICs | High Income Countries |
| IG | Intervention group |
| IMNCI | Integrated Management of Childhood Illness |
| IPC | Interpersonal counselling |
| IYCF | Infant and Young Child Feeding |
| K/S/P | Knowledge/skills/practices |
| LBW | Low Birth Weight |
| LMICs | Low- and Middle-Income Countries |
| MAMI | Management of At-risk Mothers and Infants |
| MIYCN | Maternal Infant and Young Child Nutrition |
| MM | Mass media |
| NICE | National Institute for Health and Care Excellence |
| PA | Policy advocacy |
| PRECEDE | Predisposing, reinforcing, enabling constructs in educational diagnosis and evaluation |
| PRISMA | Preferred Reporting Items for Systematic reviews and Meta-Analyses |
| SAM | Severe Acute Malnutrition |
| TBA | Traditional Birth Attendant |
| UNICEF | United Nations Children’s Fund |
| WAZ | Weight-for-Age z-score |
| WHO | World Health Organization |
| WLZ | Weight-for-Length z-score |
References
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Bernardo, H.L.; Victora, C.G. Long-Term Effects of Breastfeeding: A Systematic Review. 2013. Available online: https://apps.who.int/iris/bitstream/handle/10665/79198/9789241505307_eng.pdf?sequence=1 (accessed on 21 August 2019).
- UNICEF; WHO; WB. Levels and Trends in Child Malnutrition: Key Findings of the 2018 Edition of the Joint Child Malnutrition Estimates; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- McDonald, C.M.; Olofin, I.; Flaxman, S.; Fawzi, W.W.; Spiegelman, D.; Caulfield, L.E. The effect of multiple anthropometric deficits on child mortality: Meta-analysis of individual data in 10 prospective studies from developing countries. Am. J. Clin. Nutr. 2013, 97, 896–901. [Google Scholar] [CrossRef] [PubMed]
- Bhutta, Z.A.; Berkley, J.A.; Bandsma, R.H.J.; Kerac, M.; Trehan, I.; Briend, A. Severe childhood malnutrition. Nat. Rev. Dis. Primers. 2017, 3, 17067. [Google Scholar] [CrossRef]
- United Nations Inter-Agency Group for Child Mortality Estimation. Levels & Trends in Child Mortality: Report 2017; United Nations Children’s Fund: New York, NY, USA, 2017. [Google Scholar]
- Kerac, M.; Mwangome, M.; McGrath, M.; Haider, R.; Berkley, J.A. Management of acute malnutrition in infants aged under 6 months (MAMI): Current issues and future directions in policy and research. Food Nutr. Bull. 2015, 36 (Suppl. S1), S30–S44. [Google Scholar] [CrossRef]
- Kerac, M.; Blencowe, H.; Grijalva-Eternod, C.; McGrath, M.; Shoham, J.; Cole, T.J. Prevalence of wasting among under 6-month-old infants in developing countries and implications of new case definitions using WHO growth standards: A secondary data analysis. Arch. Dis. Child. 2011, 96, 1008–1013. [Google Scholar] [CrossRef] [PubMed]
- Kerac, M.; Frison, S.; Connell, N.; Page, B.; McGrath, M. Informing the management of acute malnutrition in infants aged under 6 months (MAMI): Risk factor analysis using nationally-representative demographic & health survey secondary data. Peer J. 2019, 6, e5848. [Google Scholar] [PubMed]
- Kerac, M.; McGrath, M. 14 Management of acute malnutrition in infants under 6 months of age. In The Biology of the First 1,000 Days; CRC Press: Boca Raton, FL, USA, 2018; pp. 207–220. [Google Scholar]
- Kerac, M.; McGrath, M.; Grijalva-Eternod, C.; Bizouerne, C.; Saxton, J.; Bailey, H. Management of acute malnutrition in infants (MAMI) Project Technical review: Current evidence, policies, practices & programme outcomes IASC, ACF, UCL, Emergency Nutrition Network [Internet]. 2010. Available online: https://reliefweb.int/sites/reliefweb.int/files/resources/8A7E77D26B35660F492576F70010D7DF-mami-report-complete.pdf (accessed on 16 August 2018).
- WHO. Guideline: Updates on the Management of Severe Acute Malnutrition in Infants and Children; World Health Organisation: Geneva, Switzerland, 2013. [Google Scholar]
- WHO; UNICEF. Global Strategy for Infant and Young Child Feeding; World Health Organisation: Geneva, Switzerland, 2003. [Google Scholar]
- Victora, C.G.; Bahl, R.; Barros, A.J.; França, G.V.; Horton, S.; Krasevec, J. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef]
- Burgio, M.A.; Laganà, A.S.; Sicilia, A.; Porta, R.P.; Porpora, M.G.; Ban Frangez, H. Breastfeeding education: Where are we going? a systematic review article. Iran J. Public Health 2016, 45, 970. [Google Scholar] [PubMed]
- Sinha, B.; Chowdhury, R.; Sankar, M.J.; Martines, J.; Taneja, S.; Mazumder, S. Interventions to improve breastfeeding outcomes: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 114–134. [Google Scholar] [CrossRef]
- Sunguya, B.F.; Poudel, K.C.; Mlunde, L.B.; Shakya, P.; Urassa, D.P.; Jimba, M. Effectiveness of nutrition training of health workers toward improving caregivers’ feeding practices for children aged six months to two years: A systematic review. Nutr. J. 2013, 12, 66. [Google Scholar] [CrossRef] [PubMed]
- Jesus, P.C.d.; Oliveira, M.I.C.d.; Fonseca, S.C. Impact of health professional training in breastfeeding on their knowledge, skills, and hospital practices: A systematic review. J Pediatr. 2016, 92, 436–450. [Google Scholar] [CrossRef]
- Kerac, M.; McGrath, M.; Connell, N.; Kompala, C.; Moore, W.H.; Bailey, J. ‘Severe malnutrition’: Thinking deeply, communicating simply. BMJ Global Health 2020, 5, e003023. [Google Scholar] [CrossRef] [PubMed]
- McGrath, M. Management of At Risk Mothers and Infants (MAMI): Emergency Nutrition Network (ENN). 2016. Available online: https://www.ennonline.net/ourwork/research/mami (accessed on 15 December 2020).
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Fantom, N.; Serajuddin, U. The World Bank’s Classification of Countries by Income, Policy Research Working Paper 7528; World Bank: Washington, DC, USA, 2016. [Google Scholar]
- National Institute for Health and Care Excellence. Methods for the development of NICE public health guidance 2012. Available online: https://www.nice.org.uk/process/pmg4/chapter/introduction (accessed on 20 July 2018).
- Campbell, M.; McKenzie, J.E.; Sowden, A.; Katikireddi, S.V.; Brennan, S.E.; Ellis, S. Synthesis without meta-analysis (SWiM) in systematic reviews: Reporting guideline. BMJ 2020, 368, l6890. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, J.E.; Brennan, S.E. Synthesizing and presenting findings using other methods. In Cochrane Handbook for Systematic Reviews of Interventions; Wiley: Hoboken, NJ, USA, 2019; pp. 321–347. [Google Scholar]
- Ahmadi, S.; Kazemi, F.; Masoumi Seyedeh, Z.; Parsa, P.; Roshanaei, G. Intervention based on BASNEF model increases exclusive breastfeeding in preterm infants in Iran: A randomised controlled trial. Int. Breastfeed. J. 2016, 11, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Aidam, B.A.; Perez-Escamilla, R.; Lartey, A. Lactation counseling increases exclusive breast-feeding rates in Ghana. J. Nutr. 2005, 135, 1691–1695. [Google Scholar] [CrossRef] [PubMed]
- Albernaz, E.; Victora, C.G.; Haisma, H.; Wright, A.; Coward, W.A. Lactation counseling increases breast-feeding duration but not breast milk intake as measured by isotopic methods. J. Nutr. 2003, 133, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, L.D.; Giugliani, E.R.J.; Santo, L.C.d.E.; Nunes, L.M. Counselling sessions increased duration of exclusive breastfeeding: A randomised clinical trial with adolescent mothers and grandmothers. Nutr. J. 2014, 13, 73. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Engebretsen, I.M.S.; Jackson, D.; Fadnes Lars, T.; Nankabirwa, V.; Diallo Abdoulaye, H.; Doherty, T. Growth effects of exclusive breastfeeding promotion by peer counsellors in sub-Saharan Africa: The cluster-randomised PROMISE EBF trial. BMC Public Health 2014, 14, 633. [Google Scholar] [CrossRef] [PubMed]
- Tylleskar, T.; Jackson, D.; Meda, N.; Engebretsen, I.M.; Chopra, M.; Diallo, A.H. Exclusive breastfeeding promotion by peer counsellors in sub-Saharan Africa (PROMISE-EBF): A cluster-randomised trial. Lancet 2011, 378, 420–427. [Google Scholar] [CrossRef]
- Kimani-Murage, E.W.; Griffiths, P.L.; Wekesah, F.M.; Wanjohi, M.; Muhia, N.; Muriuki, P.; Egondi, T.; Kyobutungi, C.; Ezeh, A.C.; McGarvey, S.T.; et al. Effectiveness of home-based nutritional counselling and support on exclusive breastfeeding in urban poor settings in Nairobi: A cluster randomised controlled trial. Global Health 2017, 13, 90. [Google Scholar] [CrossRef] [PubMed]
- Kimani-Murage, E.W.; Norris, S.A.; Mutua, M.K.; Wekesah, F.; Wanjohi, M.; Muhia, N.; Muriuki, P.; Egondi, T.; Kyobutungi, C.; Ezeh, A.C.; et al. Potential effectiveness of Community Health Strategy to promote exclusive breastfeeding in urban poor settings in Nairobi, Kenya: A quasi-experimental study. J. Dev. Orig. Health Dis. 2016, 7, 172–184. [Google Scholar] [CrossRef]
- Leite, A.J.; Puccini, R.F.; Atalah, A.N.; Alves Da Cunha, A.L.; Machado, M.T. Effectiveness of home-based peer counselling to promote breastfeeding in the northeast of Brazil: A randomised clinical trial. Acta Paediatr. 2005, 94, 741–746. [Google Scholar] [CrossRef] [PubMed]
- Morrow, A.L.; Guerrero, M.L.; Shults, J.; Calva, J.J.; Lutter, C.; Bravo, J. Efficacy of home-based peer counselling to promote exclusive breastfeeding: A randomised controlled trial. Lancet 1999, 353, 1226–1231. [Google Scholar] [CrossRef]
- Tahir, N.M.; Al-Sadat, N. Does telephone lactation counselling improve breastfeeding practices? A randomised controlled trial. Int. J. Nurs. Stud. 2013, 50, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.H. Breastfeeding preterm infants: An educational program to support mothers of preterm infants in Cairo, Egypt. Pediatr. Nurs. 2008, 34, 125–140. [Google Scholar] [PubMed]
- Aksu, H.; Kucuk, M.; Duzgun, G. The effect of postnatal breastfeeding education/support offered at home 3 days after delivery on breastfeeding duration and knowledge: A randomised trial. J. Matern. Fetal. Neonatal. Med. 2011, 24, 354–361. [Google Scholar] [CrossRef] [PubMed]
- Froozani, M.D.; Permehzadeh, K.; Motlagh, A.R.; Golestan, B. Effect of breastfeeding education on the feeding pattern and health of infants in their first 4 months in the Islamic Republic of Iran. Bull. World Health Organ. 1999, 77, 381–385. [Google Scholar]
- Jakobsen, M.S.; Sodemann, M.; Biai, S.; Nielsen, J.; Aaby, P. Promotion of exclusive breastfeeding is not likely to be cost effective in West Africa: A randomised intervention study from Guinea-Bissau. Acta Paediatr. 2008, 97, 68–75. [Google Scholar] [CrossRef]
- Khresheh, R.; Suhaimat, A.; Jalamdeh, F.; Barclay, L. The effect of a postnatal education and support program on breastfeeding among primiparous women: A randomised controlled trial. Int. J. Nurs. Stud. 2011, 48, 1058–1065. [Google Scholar] [CrossRef] [PubMed]
- Neyzi, O.; Gulecyuz, M.; Dincer, Z.; Olgun, P.; Kutluay, T.; Uzel, N. An educational intervention on promotion of breast feeding complemented by continuing support. Paediatr Perinat Epidemiol. 1991, 5, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Ozluses, E.; Celebioglu, A. Educating fathers to improve breastfeeding rates and paternal-infant attachment. Indian Pediatr. 2014, 51, 654–657. [Google Scholar] [CrossRef] [PubMed]
- Su, M.; Ouyang, Y.Q. Father’s role in breastfeeding promotion: Lessons from a quasi-experimental trial in China. Breastfeed Med. 2016, 11, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Susin, L.R.; Giugliani, E.R. Inclusion of fathers in an intervention to promote breastfeeding: Impact on breastfeeding rates. J. Hum. Lact. 2008, 24, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Akram, D.S.; Agboatwalla, M.; Shamshad, S. Effect of intervention on promotion of exclusive breast feeding. J. Pak. Med. Assoc. 1997, 47, 46–48. [Google Scholar]
- Cangol, E.; Sahin, N.H. The effect of a breastfeeding motivation program maintained during pregnancy on supporting breastfeeding: A randomised controlled trial. Breastfeed Med. 2017, 12, 218–226. [Google Scholar] [CrossRef]
- Gu, Y.; Zhu, Y.; Zhang, Z.; Wan, H. Effectiveness of a theory-based breastfeeding promotion intervention on exclusive breastfeeding in China: A randomised controlled trial. Midwifery 2016, 42, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Moudi, A.; Tafazoli, M.; Boskabadi, H.; Ebrahimzadeh, S.; Salehiniya, H. Comparing the effect of breastfeeding promotion interventions on exclusive breastfeeding: An experimental study. Biomed. Res. Ther. 2016, 3, 910–927. [Google Scholar] [CrossRef]
- Reinsma, K.; Bolima, N.; Fonteh, F.; Okwen, P.; Siapco, G.; Yota, D. Bobbi Be Best: The development and evaluation of an audio program and discussion guide to promote exclusive breastfeeding in Cameroon, Central Africa. Glob. Health Promot. 2016, 23, 14–26. [Google Scholar] [CrossRef]
- Saljughi, F.; Esfahani, M.S.; Kohan, S.; Ehsanpour, S. Promoting breastfeeding self-efficacy through role-playing in pregnant women. Int. J. Pediatr. 2016, 4, 2061–2068. [Google Scholar] [CrossRef]
- Bich, T.H.; Hoa, D.T.; Ha, N.T.; Vui le, T.; Nghia, D.T.; Malqvist, M. Father’s involvement and its effect on early breastfeeding practices in Viet Nam. Matern Child Nutr. 2016, 12, 768–777. [Google Scholar] [CrossRef] [PubMed]
- Bich, T.H.; Hoa, D.T.; Malqvist, M. Fathers as supporters for improved exclusive breastfeeding in Viet Nam. Matern. Child Health J. 2014, 18, 1444–1453. [Google Scholar] [CrossRef] [PubMed]
- Bich, T.H.; Cuong, N.M. Changes in knowledge, attitude and involvement of fathers in supporting exclusive breastfeeding: A community-based intervention study in a rural area of Vietnam. Int. J. Public Health 2017, 62 (Suppl. S1), 17–26. [Google Scholar] [CrossRef] [PubMed]
- Dearden, K.; Altaye, M.; De Maza, I.; De Oliva, M.; Stone-Jimenez, M.; Burkhalter, B.R. The impact of mother-to-mother support on optimal breast-feeding: A controlled community intervention trial in peri-urban Guatemala City, Guatemala. Rev. Panam. Salud. Publica. 2002, 12, 193–201. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Agrasada, G.V.; Gustafsson, J.; Kylberg, E.; Ewald, U. Postnatal peer counselling on exclusive breastfeeding of low-birthweight infants: A randomised, controlled trial. Acta Paediatr. 2005, 94, 1109–1115. [Google Scholar] [CrossRef] [PubMed]
- Balaluka, G.B.; Nabugobe, P.S.; Mitangala, P.N.; Cobohwa, N.B.; Schirvel, C.; Dramaix, M.W. Community volunteers can improve breastfeeding among children under six months of age in the Democratic Republic of Congo crisis. Int. Breastfeed. J. 2012, 7. [Google Scholar] [CrossRef]
- Bhandari, N.; Bahl, R.; Mazumdar, S.; Martines, J.; Black, R.E.; Bhan, M.K. Effect of community-based promotion of exclusive breastfeeding on diarrhoeal illness and growth: A cluster randomised controlled trial. Lancet 2003, 361, 1418–1423. [Google Scholar] [CrossRef]
- Khayyati, F.; Mansouri, M. The effect of training movies on exclusive breastfeeding. Pak. J. Med. Sci. 2009, 25, 434–438. [Google Scholar]
- Ma, Y.Y.; Wallace, L.L.; Qiu, L.Q.; Kosmala-Anderson, J.; Bartle, N. A randomised controlled trial of the effectiveness of a breastfeeding training DVD on improving breastfeeding knowledge and confidence among healthcare professionals in China. BMC Pregnancy Childbirth 2018, 18, 80. [Google Scholar] [CrossRef]
- Mukantwali, C.; Maunder, E.M.W.; Paterson, M.; Gibson, C. Impact of the special training of community health workers on breastfeeding counselling and support in KwaZulu-Natal. South Afr. J. Clin. Nutr. 2006, 19, 29–36. [Google Scholar] [CrossRef]
- Mukhopadhyay, D.K.; Sarkar, A.P.; Aniket, C.; Eashin, G.; Sarkar, G.N. Can frontline workers be change agents for infant feeding and growth?—A community trial. Al Ameen J. Med. Sci. 2017, 10, 71–77. [Google Scholar]
- Shamim, T.; Dina, F.; Vitta, B.; Greiner, T. In a rural area of Bangladesh, traditional birth attendant training improved early infant feeding practices: A pragmatic cluster randomised trial. Matern. Child. Nutr. 2017, 13, e12237. [Google Scholar] [CrossRef]
- Menon, P.; Nguyen Phuong, H.; Saha Kuntal, K.; Khaled, A.; Kennedy, A.; Tran Lan, M. Impacts on breastfeeding practices of at-scale strategies that combine intensive interpersonal counseling, mass media, and community mobilisation: Results of cluster-randomised program evaluations in Bangladesh and Viet Nam. PLoS Med. 2016, 13, 1–28. [Google Scholar] [CrossRef]
- Yotebieng, M.; Labbok, M.; Soeters, H.M.; Chalachala, J.L.; Lapika, B.; Vitta, B.S.; Behets, F. Ten steps to successful breastfeeding programme to promote early initiation and exclusive breastfeeding in DR Congo: A cluster-randomised controlled trial. Lancet Glob. Health 2015, 3, e546–e555. [Google Scholar] [CrossRef]
- Ochola, S.A.; Labadarios, D.; Nduati, R.W. Impact of counselling on exclusive breast-feeding practices in a poor urban setting in Kenya: A randomised controlled trial. Public Health Nutr. 2013, 16, 1732–1740. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Matsiko, E.; Hulshof, P.J.; van Der Velde, L.; Kenkhuis, M.-F.; Tuyisenge, L.; Melse-Boonstra, A. Comparing saliva and urine samples for measuring breast milk intake with the 2 H oxide dose-to-mother technique among children 2–4 months old. Br. J. Nutr. 2020, 123, 232–240. [Google Scholar] [CrossRef]
- Haroon, S.; Das, J.K.; Salam, R.A.; Imdad, A.; Bhutta, Z.A. Breastfeeding promotion interventions and breastfeeding practices: A systematic review. BMC Public Health 2013, 13, S20. [Google Scholar] [CrossRef]
- Imdad, A.; Yakoob, M.Y.; Bhutta, Z.A. Effect of breastfeeding promotion interventions on breastfeeding rates, with special focus on developing countries. BMC Public Health 2011, 11, S24. [Google Scholar] [CrossRef] [PubMed]
- Shakya, P.; Kunieda, M.K.; Koyama, M.; Rai, S.S.; Miyaguchi, M.; Dhakal, S.; Sandy, S.; Sunuya, B.F.; Jimba, M. Effectiveness of community-based peer support for mothers to improve their breastfeeding practices: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0177434. [Google Scholar] [CrossRef]
- Sudfeld, C.R.; Fawzi, W.W.; Lahariya, C. Peer support and exclusive breastfeeding duration in low and middle-income countries: A systematic review and meta-analysis. PLoS ONE 2012, 7, e45143. [Google Scholar] [CrossRef] [PubMed]
- Gavine, A.; MacGillivray, S.; Renfrew, M.J.; Siebelt, L.; Haggi, H.; McFadden, A. Education and training of healthcare staff in the knowledge, attitudes and skills needed to work effectively with breastfeeding women: A systematic review. Int. Breastfeed J. 2016, 12, 6. [Google Scholar] [CrossRef] [PubMed]
- Davies-Adetugbo, A.A.; Fabiyi, A.K.; Ojoofeitimi, E.O.; Adetugbo, K. Breastfeeding training improves health worker performance in rural Nigeria. East Afr. Med. J. 1997, 74, 510–513. [Google Scholar] [PubMed]
- Mahdiah; Siagian, A.; Aritonang, E.Y.; Lubis, N.L. Effect of nutrition peer counseling and breastfeeding the improvement in exclusive breastfeeding and infant nutrition status in Sub Lubuk Pakam and Tanjung Morawa, Deli Serdang. Indian J. Public Health Res. Dev. 2018, 9, 194–199. [Google Scholar] [CrossRef]
- Shashikala, N.; Kulkarni, P.; Renuka, M.; Sunil, D. Strategising the educational interventional methods on infant feeding practices: An exploratory study among primary care workers in rural Mysore. Indian J. Public Health Res. Dev. 2016, 7, 171–176. [Google Scholar] [CrossRef]
- Balogun, O.O.; Dagvadorj, A.; Anigo, K.M.; Ota, E.; Sasaki, S. Factors influencing breastfeeding exclusivity during the first 6 months of life in developing countries: A quantitative and qualitative systematic review. Matern. Child. Nutr. 2015, 11, 433–451. [Google Scholar] [CrossRef] [PubMed]
- Read, S.; McGrath, M. Community management of uncomplicated malnourished infants under six months old: Barriers to national policy change. Field Exch. 2018, 57, 27. Available online: https://www.ennonline.net/fex/57/malnourishedinfantschange (accessed on 16 December 2020).


{kind=link}
{kind=link}
| Author (Year) | Country | Design | Quality (Internal, External Validity) | Population | Sample Size | Intervention Type | Outcomes | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Breast-Feeding Practices | Care-Giver K/S/P | Health-Care Staff K/S/P | Morbidity | Anthropo-metry | |||||||
| Counselling interventions | |||||||||||
| Ahmadi (2016) [26] | Iran | RCT | (+,++) | Mother–premature infants | 124 | Hospital-based | √ | √ | √ | ||
| Aidam (2005) [27] | Ghana | RCT | (+,+) | Pregnant women | 136 | Hospital-based | √ | ||||
| Albernaz (2003) [28] | Brazil | RCT | (+,+) | Infants | 188 | Hospital-based | √ | √ | |||
| Oliveira (2014) [29] | Brazil | RCT | (+,+) | AM–infants–grandmother | 323 | Hospital-based | √ | ||||
| Engebretsen (2014) [30] Tylleskar (2011) [31] † | Burkina Faso, Uganda, South Africa | C-RCT | (++,++) | Mother–infant pairs | 2579 | Community-based | √ | √ | √ | ||
| Kimani-Murage (2017, 2016) [32,33] † | Kenya | C-RCT | (++,++) | Mother–child pairs | 1110 | Community-based | √ | ||||
| Leite (2005) [34] | Brazil | RCT | (+,−) | Mothers–infants | 1001 | Community-based | √ | ||||
| Morrow (1999) [35] | Mexico | RCT | (−,−) | Pregnant women | 130 | Community-based | √ | √ | |||
| Tahir (2013) [36] | Malaysia | RCT | (−,+) | Mothers | 357 | Hospital-based | √ | ||||
| Education interventions | |||||||||||
| Ahmed (2008) [37] | Egypt | QE | (−,−) | Mother–preterm infants | 60 | Hospital-based | √ | ||||
| Aksu (2011) [38] | Turkey | RCT | (+,+) | Pregnant women | 66 | Community-based | √ | √ | |||
| Froozani (1999) [39] | Iran | QE | (−,+) | Mother–infant pairs | 120 | Hospital-based | √ | √ | √ | ||
| Jakobsen (2008) [40] | Guinea-Bissau | RCT | (+,+) | Mothers and infants | 1721 | Community-based | √ | √ | √ | ||
| Khresheh (2011) [41] | Jordan | RCT | (+,+) | Primiparous women | 140 | Hospital-based | √ | √ | √ | ||
| Neyzi (1991) [42] | Turkey | QE | (−,−) | Mother–infant pairs | 146 | Hospital-based | √ | ||||
| Ozluses (2014) [43] | Turkey | QE | (−,−) | Couples with their infants | 117 | Hospital-based | √ | ||||
| Su (2016) [44] | China | QE | (−,−) | Pregnant women–partners | 72 | Hospital-based | √ | √ | |||
| Susin (2008) [45] | Brazil | QE | (+,+) | Mother–father–infant triads | 586 | Hospital-based | √ | ||||
| Promotion interventions | |||||||||||
| Akram (1997) [46] | Pakistan | QE | (−,−) | Pregnant women | 120 | Community-based | √ | √ | |||
| Cangol (2017) [47] | Turkey | RCT | (−,+) | Pregnant women | 100 | Hospital-based | √ | √ | √ | ||
| Gu (2016) [48] | China | RCT | (−,+) | Pregnant women–husband/mother | 352 | Hospital-based | √ | ||||
| Moudi (2016) [49] | Iran | QE | (+,−) | Pregnant women | 108 | Hospital-based | √ | ||||
| Reinsma (2016) [50] | Cameroon | QE | (+,−) | Pregnant women–partners | 384 | Community-based | √ | ||||
| Saljughi (2016) [51] | Iran | QE | (−,−) | Pregnant women | 74 | Hospital-based | √ | ||||
| Peer support interventions | |||||||||||
| Bich (2017, 2017, 2014) [52,53,54] † | Vietnam | QE | (+,+) | Fathers–pregnant wives | 492 | Community-based | √ | √ | |||
| Dearden (2002) [55] | Guatemala | B-A | (+,+) | Mothers of infants < 6 m | 768 | Community-based | √ | ||||
| Training interventions | |||||||||||
| Agrasada (2005) [56] | Philippines | RCT | (+,−) | Mother–infant (term LBW) | 204 | Hospital-based | √ | ||||
| Balaluka (2012) [57] | Congo | PE | (+,+) | Infants | 386 | Community-based | √ | √ | |||
| Bhandari (2001) [58] | India | C-RCT | (++,++) | Infants | 1115 | Community-based | √ | √ | √ | ||
| Khayyati (2009) [59] | Iran | RCT | (−,−) | Pregnant women | 244 | Hospital-based | √ | √ | √ | ||
| Ma (2018) [60] | China | RCT | (+,+) | Healthcare staff | 210 | Hospital-based | √ | ||||
| Mukantwali (2006) [61] | South Africa | QE | (−,−) | Mother–infant pairs | 182 | Community-based | √ | ||||
| Mukhopadhyay (2017) [62] | India | C-RCT | (−,−) | Mother–infant pairs | 130 | Community-based | √ | √ | |||
| Shamim (2017) [63] | Bangladesh | C-RCT | (+,+) | Mothers of infants < 6 m | 1182 | Community-based | √ | √ | |||
| Other intervention | |||||||||||
| Menon (2016) [64] | Bangladesh, Viet Nam | C-RE | (++,++) | Infants | 2000 | Community-based | √ | ||||
| Yotebieng (2015) [65] | Congo | C-RCT | (++,++) | Mother–infant pairs | 975 | Hospital-based | √ | √ | |||
| Ochola (2013) [66] | Kenya | C-RCT | (+,+) | Pregnant women | 360 | Community-, Hospital-based | √ | ||||
| Author, Population | Intervention and Comparison | Effect on Outcomes | ||||
|---|---|---|---|---|---|---|
| Breastfeeding Practices | Caregiver K/S/P | Healthcare Staff K/S/P | Morbidity | Anthropo-Metry | ||
| Counselling interventions | ||||||
| Ahmadi (2016) [26] Mothers with premature (34–37w) infants | IG: breastfeeding consultation sessions based on BASNEF model vs. CG: conventional training by staff | ↑ | ↑ | ↑ | ||
| Albernaz (2003) [28] Infants | IG: lactation counselling support by trained nurse- hospital and home visits vs. CG: standard care | ↔ | ↔ | |||
| Tahir (2013) [36] Mothers | IG: telephone lactation counselling twice monthly by certified lactation counsellors + conventional care vs. CG: conventional care | ↔ | ||||
| Aidam (2005) [27] ‡ Pregnant women attending prenatal clinics | IG1: lactation counselling- pre-, peri-, and post-natally vs. CG: non-breastfed health education support | ↑ | ||||
| IG2: lactation counselling- peri-, and post-natally vs. CG: non-breastfed health education support | ↑ | |||||
| Oliveira (2014) [29] ‡ Adolescent mothers with newborn and their mothers | IG1: counselling sessions for adolescent girls vs. CG1: adolescent girls without intervention (not living with mother) | ↑ | ||||
| IG2: counselling sessions for adolescent girls vs. CG2: adolescent girls without intervention (living with mother) | ↑ | |||||
| Kimani-Murage (2017, 2016) [32,33] † Mother–child pairs | IG: home-based nutrition counselling by CHWs (trained to offer counselling on MIYCN) vs. CG: standard care | ↔ | ||||
| Engebretsen (2014) [30] Tylleskar (2011) [31] † Mother–infant pairs | IG: peer counselling (1 antenatal and 4 postnatal) vs. CG: usual care | ↑ | ↔ | ↔ | ||
| Morrow (1999) [35] ‡ Pregnant women | IG1: home based peer counselling—6 visits vs. CG: no intervention | ↔ | ↑ | |||
| IG2: home based peer counselling—3 visits vs. CG: no intervention | ↔ | ↑ | ||||
| Leite (2005) [34] Mothers–infants | IG: home based peer counselling with home visits 5,15,30,60,90, and 120 days vs. CG: standard care | ↑ | ||||
| Education interventions | ||||||
| Froozani (1999) [39] Mother–infant pairs | IG: education, face-to-face, after delivery and during follow-up vs. CG: usual care | ↑ | ↔ | ↑ | ||
| Neyzi (1991) [42] Mother–infant pairs | IG: 2 educational sessions after delivery vs. CG: usual care | ↑ | ||||
| Khresheh (2011) [41] Primiparous women | IG: one-to-one postnatal education sessions and follow-up phone calls at 2 and 4 months vs. CG: routine care | ↔ | ↕ | ↔ | ||
| Susin (2008) [45] ‡ Mother–father–infant triads | IG1: educational session by a trained pediatrician to mother + father vs. CG: no intervention | ↑ | ||||
| IG2: Educational session by a trained pediatrician to mother only vs. CG: no intervention | ↔ | |||||
| Ozluses (2014) [43] ‡ Couples with their infants | IG1: educating mothers + fathers—20 min/day vs. CG: no education | ↑ | ||||
| IG2: educating mothers—20 min/day vs. CG: no education | ↑ | |||||
| Su (2016) [44] Pregnant women | IG: education to mother + father vs. CG: education to mother only | ↑ | ↑ | |||
| Ahmed (2008) [37] Mothers and preterm infants (born <37w) | IG: 5 session (PRECEDE model) vs. CG: routine care | ↑ | ||||
| Aksu (2011) [38] Pregnant women | IG: BF education at home on day 3 postpartum (reinforcement) vs. CG: no education/support | ↑ | ↑ | |||
| Jakobsen (2008) [40] Mothers and infants | IG: education provided individually and orally in local language vs. CG: standard care | ↑ | ↔ | ↔ | ||
| Training interventions | ||||||
| Agrasada (2005) [56] ‡ Mother–infant (term LBW) pairs | IG1: BF counselling by trained counsellors vs. CG: any counselling | ↑ | ||||
| IG2: child feeding counselling by trained counsellors vs. CG: any counselling | ↑ | |||||
| Khayyati (2009) [59] Pregnant women | IG: training movies and common method of face-to-face training vs. CG: face-to-face training | ↔ | ↔ | ↔ | ||
| Ma (2018) [60] Healthcare professional–doctor, nurse, midwife | IG: BF essential support skills DVD vs. CG: vaginal delivery DVD | ↑ | ||||
| Bhandari (2001) [58] Infants | IG: promotion by CHWs trained in BF (3-day course) vs. CG: usual care | ↑ | ↕ | ↔ | ||
| Balaluka (2012) [57] Infants | IG: trained CVs promoting EBF via door-to-door visits and community meetings vs. CG: usual care only | ↑ | ↔ | |||
| Mukantwali (2006) [61] Mother–infant pairs | IG: visited by specially trained CHW vs. CG: visited by normally trained CHW | ↔ | ||||
| Mukhopadhyay (2017) [62] Mother–infant pairs | IG: trained CHWs vs. CG: standard care | ↑ | ↕ | |||
| Shamim (2017) [63] ‡ Mothers of infants < 6 m | IG1: trained TBAs/CVs vs. CG: TBAs/CVs without special training | ↕ | ↕ | |||
| IG2: trained + supervised TBAs/CVs vs. CG: TBAs/CVs without special training | ↕ | ↕ | ||||
| Promotion interventions | ||||||
| Cangol (2017) [47] Pregnant—applied to pregnancy preparation course | IG: BF motivation programme based on Pender’s Health Promotion Model—4 times-antenatal period, 1st postnatal day, 4th–6th postnatal week and 4th postnatal month vs. CG: standard care | ↑ | ↔ | ↔ | ||
| Gu (2016) [48] Primiparous women companied by husband/mother | IG: Theory of Planned Behaviour (TPB) based intervention programme—individual instruction, group education and telephone counselling vs. CG: routine nursing care | ↑ | ||||
| Moudi (2016) [49] ‡ Primiparous women referred to health centre | IG1: peer support group (4 times) vs. CG: routine care | ↑ | ||||
| IG2: health care provider’s education (4 training sessions) vs. CG: routine care | ↑ | |||||
| Saljughi (2016) [51] Pregnant women | IG: training on promoting BF self-efficacy at 36th week via role playing vs. CG: routine care | ↑ | ||||
| Akram (1997) [46] Pregnant women | IG: promotion of EBF via health messages vs. CG: no health messages | ↑ | ↑ | |||
| Reinsma (2016) [50] Pregnant women and their partners | IG: audio programme (Bobbi Be Best) and discussion guide to promote EBF- entertainment education (EBF) vs. CG: entertainment education (injection safety) | ↕ | ||||
| Peer support interventions | ||||||
| Bich (2017, 2017, 2014) [52,53,54] † Fathers and their pregnant wives from 7 to 30 w gestation | IG: fathers as supporters—BF education material, counselling services at community health centres, invitation to social events and household visits vs. CG: no intervention to fathers | ↑ | ↑ | |||
| Dearden (2002) [55] Mothers of infants < 6 m | IG: mother-to-mother support programme of La Leche League Guatemala-BF counselling by trained counsellor vs. CG: usual care | ↕ | ||||
| Other interventions | ||||||
| Yotebieng (2015) [65] Mother–infant pairs | IG1: BFHI steps 1–9, IG2: BFHI steps 1–10 vs. CG: standard care | ↔ | ↔ | |||
| Menon (2016) [64] Infants | IG: BF practices at scale-intensified IPC, MM, CM, and PA vs. CG: standard nutrition counselling and less intensive MM, CM, and PA | ↑ | ||||
| Ochola (2013) [66] ‡ Pregnant women (34–36 w) attending antenatal clinic | IG1: home based intensive counselling group (HBIC) vs. CG: standard care | ↑ | ||||
| IG2: facility based semi-intensive counselling group (FBSIC) vs. CG: standard care | ↔ | |||||
| Intervention Categories | Outcomes (Proportion of Effects †, 95% CI, p Value) | ||||
|---|---|---|---|---|---|
| Breast-Feeding Practices | Caregiver K/S/P | Healthcare Staff K/S/P | Morbidity | Anthropo-Metry | |
| Counselling | 0.58 (0.31–0.80, p = 0.77) | NA | - | 0.66 (0.20–0.93, p = 1.00) | 0.33 (0.06–0.79, p = 1.00) |
| Education | 0.80 (0.49–0.94, p = 0.10) | 0.75 (0.30–0.95, p = 0.62) | - | 0 | NA |
| Training | 0.55 (0.26–0.81, p = 1.00) | - | 0.33 (0.06–0.79, p = 1.00) | NA | 0 |
| Promotion | 1.00 (0.56–1.00, p = 0.06) | 0.50 (0.15–0.84, p = 1.00) | - | - | NA |
| Peer Support | NA | NA | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rana, R.; McGrath, M.; Sharma, E.; Gupta, P.; Kerac, M. Effectiveness of Breastfeeding Support Packages in Low- and Middle-Income Countries for Infants under Six Months: A Systematic Review. Nutrients 2021, 13, 681. https://doi.org/10.3390/nu13020681
Rana R, McGrath M, Sharma E, Gupta P, Kerac M. Effectiveness of Breastfeeding Support Packages in Low- and Middle-Income Countries for Infants under Six Months: A Systematic Review. Nutrients. 2021; 13(2):681. https://doi.org/10.3390/nu13020681
Chicago/Turabian StyleRana, Ritu, Marie McGrath, Ekta Sharma, Paridhi Gupta, and Marko Kerac. 2021. "Effectiveness of Breastfeeding Support Packages in Low- and Middle-Income Countries for Infants under Six Months: A Systematic Review" Nutrients 13, no. 2: 681. https://doi.org/10.3390/nu13020681
APA StyleRana, R., McGrath, M., Sharma, E., Gupta, P., & Kerac, M. (2021). Effectiveness of Breastfeeding Support Packages in Low- and Middle-Income Countries for Infants under Six Months: A Systematic Review. Nutrients, 13(2), 681. https://doi.org/10.3390/nu13020681