
Medication-Related Osteonecrosis of the Jaw (MRONJ): Are Antiresorptive Drugs the Main Culprits or Only Accomplices? The Triggering Role of Vitamin D Deficiency




Abstract
:
1. Introduction
2. Epidemiology
3. Clinical and Genetic Risk Factors for ONJ
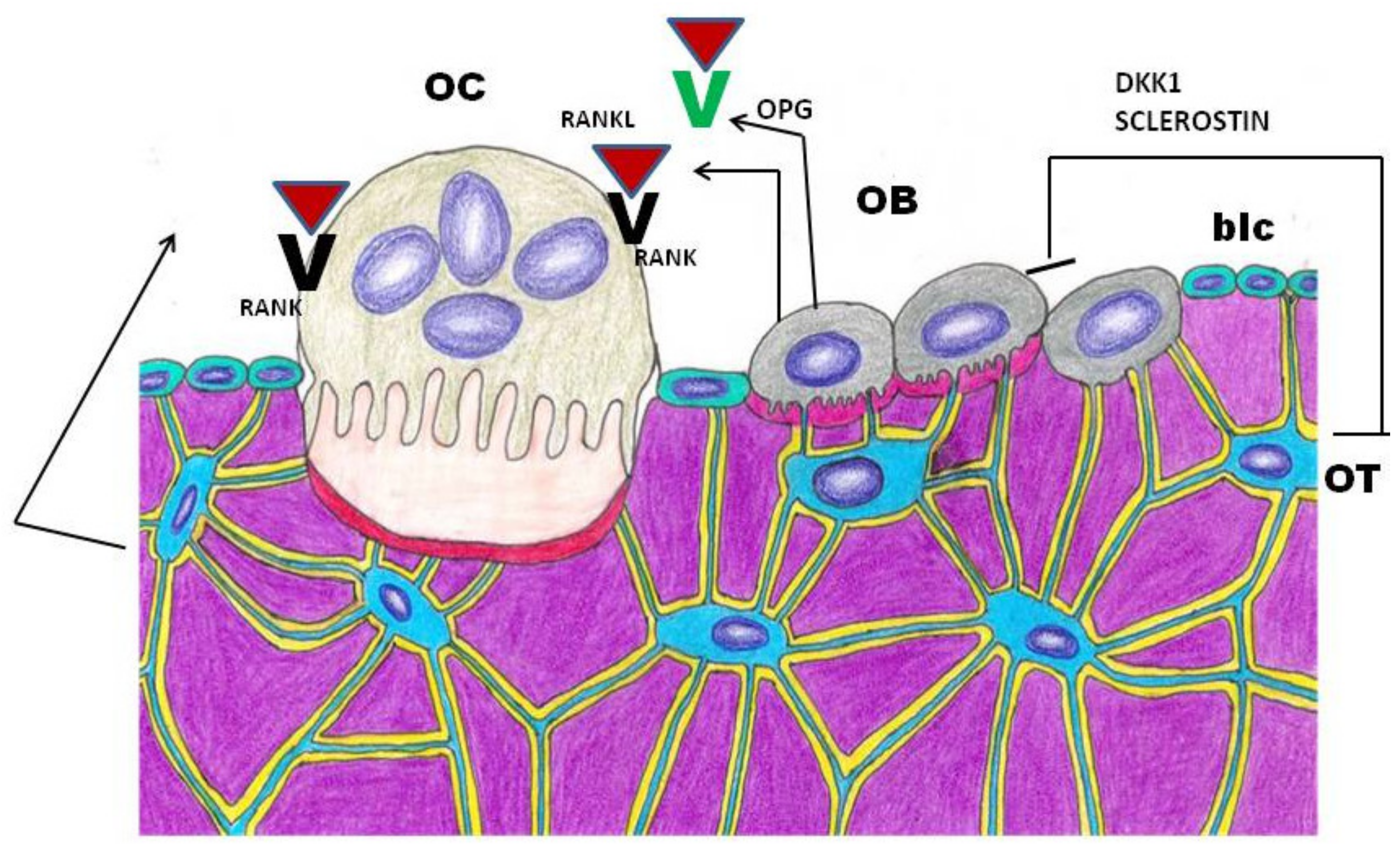
4. Bone Remodeling Impairment
5. How Do Different Antiresorptive Drugs Interfere with Bone Turnover
6. Animal Models Contribution to ONJ Studies
7. Osteomalacia and Vitamin D
8. Vitamin D and Oral Pathology
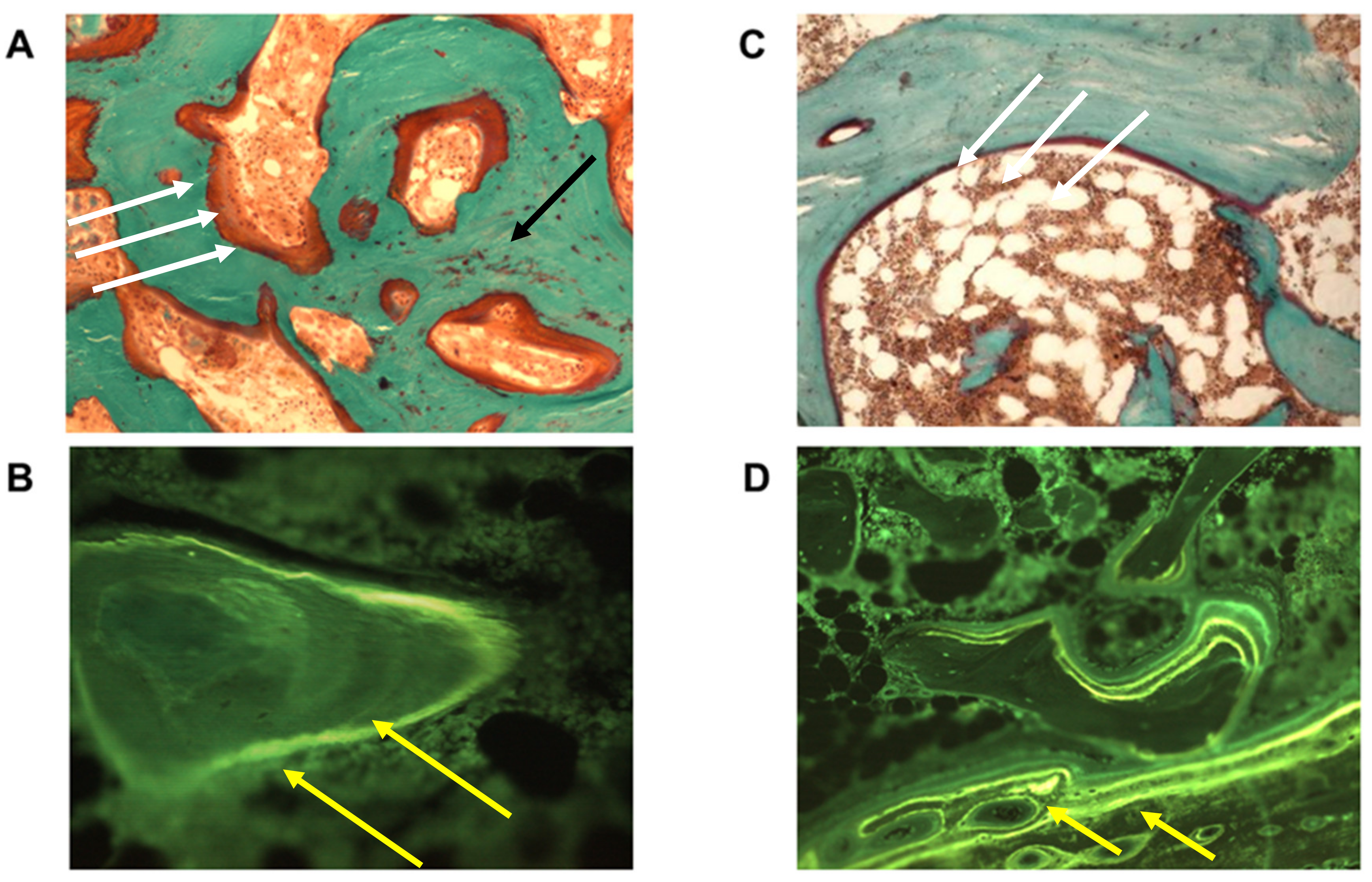
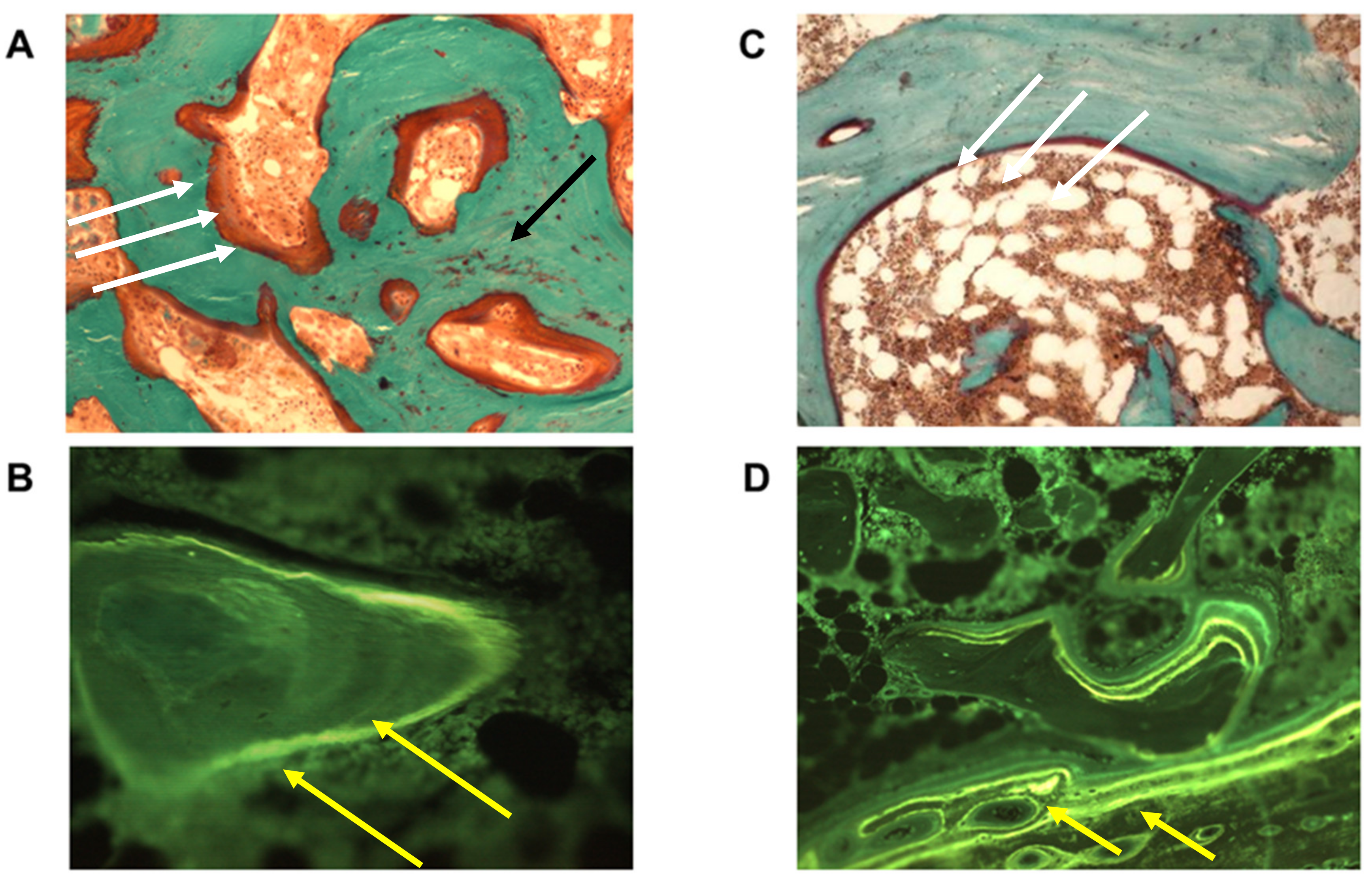
9. Histomorphometric Study
10. Discussion and Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ruggiero, S.L.; Dodson, T.B.; Fantasia, J.; Goodday, R.; Aghaloo, T.; Mehrotra, B.; O’Ryan, F. American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw—2014 update. J. Oral Maxillofac. Surg. 2014, 72, 1938–1956. [Google Scholar]
- Colella, G.; Fusco, V.; Campisi, G. American Association of Oral and Maxillofacial Surgeons position paper: Bisphosphonate-Related Osteonecrosis of the Jaws-2009 update: The need to refine the BRONJ definition. J. Oral Maxillofac. Surg. 2009, 67, 2698–2699. [Google Scholar]
- Otto, S.; Marx, R.E.; Tröltzsch, M.; Ristow, O.; Ziebart, T.; Al-Nawas, B.; Groetz, K.A.; Ehrenfeld, M.; Mercadante, V.; Porter, S.; et al. Comments on “diagnosis and management of osteonecrosis of the jaw: A systematic review and international consensus”. J. Bone Miner. Res. 2015, 30, 1113–1115. [Google Scholar]
- Schiodt, M.; Otto, S.; Fedele, S.; Bedogni, A.; Nicolatou-Galitis, O.; Guggenberger, R.; Herlofson, B.B.; Ristow, O.; Kofod, T. Workshop of European task force on medication-related osteonecrosis of the jaw—Current challenges. Oral Dis. 2019, 10, 1815–1821. [Google Scholar]
- Yarom, N.; Peterson, D.E.; Bohlke, K.; Saunders, D.P. Reply to Fusco et al. JCO Oncol. Pract. 2020, 16, 145–146. [Google Scholar]
- Nicolatou-Galitis, O.; Kouri, M.; Papadopoulou, E.; Vardas, E.; Galiti, D.; Epstein, J.B.; Elad, S.; Campisi, G.; Tsoukalas, N.; Bektas-Kayhan, K.; et al. Osteonecrosis of the jaw related to non-antiresorptive medications: A systematic review. Support. Care Cancer 2019, 27, 383–394. [Google Scholar]
- Khan, A.A.; Morrison, A.; Hanley, A.D.; Felsenberg, D.; McCauley, L.K.; O’Ryan, F.; Reid, I.R.; Ruggiero, S.L.; Taguchi, A.; Tetradis, S.; et al. Diagnosis and management of osteonecrosis of the jaw: A systematic review and international consensus. J. Bone Miner. Res. 2015, 30, 3–23. [Google Scholar]
- Mavrokokki, T.; Cheng, A.; Stein, B.; Goss, A. Nature and frequency of bisphosphonate-associated osteonecrosis of the jaws in Australia. J. Oral Maxillofac. Surg. 2007, 65, 415–423. [Google Scholar]
- Ulmner, M.; Jarnbring, F.; Törring, O. Osteonecrosis of the jaw in Sweden associated with the oral use of bisphosphonate. J. Oral Maxillofac. Surg. 2014, 72, 76–82. [Google Scholar]
- Kizub, D.A.; Miao, J.; Schubert, M.M.; Paterson, A.H.G.; Clemons, M.; Dees, E.C.; Ingle, J.N.; Falkson, C.I.; Barlow, W.E.; Hortobagyi, G.N.; et al. Risk factors for bisphosphonate-associated osteonecrosis of the jaw in the prospective randomized trial of adjuvant bisphosphonates for early-stage breast cancer (SWOG 0307). Support Care Cancer 2020. [Google Scholar] [CrossRef]
- Dennison, E.; Cooper, C.; Kanis, J.; Bruyère, O.; Silverman, S.; McCloskey, E.; Abrahamsen, B.; Prieto-Alhambra, D.; Ferrari, S.; On behalf of the IOF Epidemiology/Quality of Life Working Group. Fracture risk following intermission of osteoporosis therapy. Osteoporos. Int. 2019, 30, 1733–1743. [Google Scholar]
- Cummings, S.R.; Ferrari, S.; Eastell, R.; Gilchrist, N.; Jensen, J.-E.B.; McClung, M.; Roux, C.; Törring, O.; Valter, I.; Wang, A.T.; et al. Vertebral fractures after discontinuation of denosumab: A post hoc analysis of the randomized placebo-controlled FREEDOM trial and its extension. J. Bone Miner. Res. 2018, 33, 190–198. [Google Scholar]
- Ferrari, S.L.; Lewiecki, E.M.; Butler, P.W.; Kendler, D.L.; Napoli, N.; Huang, S.; Crittenden, D.B.; Pannacciulli, N.; Siris, E.; Binkley, N. Favorable skeletal benefit/risk of long-term denosumab therapy: A virtual-twin analysis of fractures prevented relative to skeletal safety events observed. Bone 2020, 134, 115287. [Google Scholar]
- Ottesen, C.; Schiodt, M.; Gotfredsen, K. Efficacy of a high-dose antiresorptive drug holiday to reduce the risk of medication-related osteonecrosis of the jaw (MRONJ): A systematic review. Heliyon 2020, 6, e03795. [Google Scholar]
- Fujieda, Y.; Doi, M.; Asaka, T.; Ota, M.; Hisada, R.; Ohnishi, N.; Kono, M.; Kameda, H.; Nakazawa, D.; Kato, M.; et al. Incidence and risk of antiresorptive agent-related osteonecrosis of the jaw (ARONJ) after tooth extraction in patients with autoimmune disease. J. Bone Miner. Metab. 2020, 38, 1–8. [Google Scholar]
- Maciel, A.P.; Quispe, R.A.; Martins, L.J.O.; Caldas, R.J.; Santos, P.S.D.S. Clinical profile of individuals with bisphosphonate-related osteonecrosis of the jaw: An integrative review. Sao Paulo Med. J. 2020, 138, 326–335. [Google Scholar]
- Marini, F.; Tonelli, P.; Cavalli, L.; Cavalli, T.; Masi, L.; Falchetti, A.; Brandi, M.L. Pharmacogenetics of bisphosphonate-associated osteonecrosis of the jaw. Front. Biosci. (Elite Ed.) 2011, 3, 364–370. [Google Scholar]
- Sarasquete, M.E.; García-Sanz, R.; Marín, L.; Alcoceba, M.; Chillón, M.D.C.; Balanzategui, A.; Santamaria, C.; Rosiñol, L.; De La Rubia, J.; Hernandez, M.T.; et al. Bisphosphonate-related osteonecrosis of the jaw is associated with polymorphisms of the cytochrome P450 CYP2C8 in multiple myeloma: A genome-wide single nucleotide polymorphism analysis. Blood 2008, 112, 2709–2712. [Google Scholar]
- Yang, G.; Hamadeh, I.S.; Katz, J.; Riva, A.; Lakatos, P.; Balla, B.; Kosa, J.; Vaszilko, M.; Pelliccioni, G.A.; Davis, N.; et al. SIRT1/HERC4 locus associated with bisphosphonate-induced osteonecrosis of the jaw: An exome-wide association analysis. J. Bone Miner. Res. 2018, 33, 91–98. [Google Scholar]
- Yang, G.; Collins, J.M.; Rafiee, R.; Singh, S.; Langaee, T.; McDonough, C.W.; Holliday, L.S.; Wang, D.; Lamba, J.K.; Kim, Y.S.; et al. SIRT1 Gene SNP rs932658 Is Associated With Medication-Related Osteonecrosis of the Jaw. J. Bone Miner. Res. 2020. [Google Scholar] [CrossRef]
- Allen, R.M.; Burr, D.B. The pathogenesis of bisphosphonate-related osteonecrosis of the jaw: So many hypotheses, so few data. J. Oral Maxillofac. Surg. 2009, 67, 61–70. [Google Scholar]
- Heim, N.; Götz, W.; Kramer, F.-J.; Faron, A. Antiresorptive drug-related changes of the mandibular bone densitiy in medication-related osteonecrosis of the jaw patients. Dentomaxillofac. Radiol. 2019, 48, 20190132. [Google Scholar]
- Anesi, A.; Generali, L.; Sandoni, L.; Pozzi, S.; Grande, A. From osteoclast differentiation to osteonecrosis of the jaw: Molecular and clinical insights. Int. J. Mol. Sci. 2019, 20, 4925. [Google Scholar]
- Kim, H.J.; Kim, H.J.; Choi, Y.; Bae, M.-K.; Hwang, D.S.; Shin, S.-H.; Lee, J.-Y. Zoledronate enhances osteocyte-mediated osteoclast differentiation by IL-6/RANKL axis. Int. J. Mol. Sci. 2019, 20, 1467. [Google Scholar]
- Kim, J.; Lee, D.-H.; Dziak, R.; Ciancio, S. Bisphosphonate-related osteonecrosis of the jaw: Current clinical significance and treatment strategy review. Am. J. Dent. 2020, 33, 115–128. [Google Scholar]
- Carbonare, L.D.; Zanatta, M.; Gasparetto, A.; Valenti, M.T. Safety and tolerability of zoledronic acid and other bisphosphonates in osteoporosis management. Drug Healthc. Patient Saf. 2010, 2, 121. [Google Scholar]
- Carbonare, L.D.; Mottes, M.; Malerba, G.; Mori, A.; Zaninotto, M.; Plebani, M.; Dellantonio, A.; Valenti, M.T. Enhanced osteogenic differentiation in zoledronate-treated osteoporotic patients. Int. J. Mol. Sci. 2017, 18, 1261. [Google Scholar]
- Reid, I.R. Osteonecrosis of the jaw—Who gets it, and why? Bone 2009, 44, 4–10. [Google Scholar]
- Drake, M.T.; Clarke, B.L.; Khosla, S. Bisphosphonates: Mechanism of action and role in clinical practice. Mayo Clin. Proc. 2008, 83, 1032–1045. [Google Scholar]
- Benlidayi, C.I.; Guzel, R. Oral bisphosphonate related osteonecrosis of the jaw: A challenging adverse effect. ISRN Rheumatol. 2013, 2013, 1–6. [Google Scholar]
- Paulo, S.; Abrantes, A.M.; Laranjo, M.; Carvalho, F.L.; Serra, A.C.; Botelho, M.F.; Ferreira, M.M. Bisphosphonate-related osteonecrosis of the jaw: Specificities. Oncol. Rev. 2014, 8, 254. [Google Scholar]
- Lewiecki, E.M. Denosumab update. Curr. Opin. Rheumatol. 2009, 21, 369–373. [Google Scholar]
- Lewiecki, E.M. Denosumab in postmenopausal osteoporosis: What the clinician needs to know. Ther. Adv. Musculoskelet. Dis. 2009, 1, 13–26. [Google Scholar]
- Fizazi, K.; Lipton, A.; Mariette, X.; Body, J.-J.; Rahim, Y.; Gralow, J.R.; Gao, G.M.; Wu, L.; Sohn, W.; Jun, S. Randomized phase II trial of denosumab in patients with bone metastases from prostate cancer, breast cancer, or other neoplasms after intravenous bisphosphonates. J. Clin. Oncol. 2009, 27, 1564–1571. [Google Scholar]
- Aghaloo, L.T.; Felsenfeld, A.L.; Tetradis, S. Osteonecrosis of the jaw in a patient on Denosumab. J. Oral Maxillofac. Surg. 2010, 68, 959–963. [Google Scholar]
- Lima, M.V.D.S.; Rizzato, J.; Marques, D.V.G.; Kitakawa, D.; Carvalho, L.F.D.C.E.S.D.; Scherma, A.P.; Carvalho, L.F.C.S. Denosumab related osteonecrosis of jaw: A case report. J. Oral Maxillofac. Res. 2018, 9, e1. [Google Scholar]
- Allen, M. Animal models of osteonecrosis of the jaw. J. Musculoskelet. Neuronal Interact. 2007, 7, 358. [Google Scholar]
- Ruggiero, S.L.; Dodson, T.B.; Assael, L.A.; Landesberg, R.; Marx, R.E.; Mehrotra, B. American Association of Oral and Maxillofacial Surgeons position paper on bisphosphonate-related osteonecrosis of the jaw—2009 update. Aust. Endod. J. 2009, 35, 119–130. [Google Scholar]
- Khosla, S.; Burr, D.; Cauley, J.; Dempster, D.W.; Ebeling, P.R.; Felsenberg, D.; Gagel, R.F.; Gilsanz, V.; Guise, T.; Koka, S.; et al. Bisphosphonate-associated osteonecrosis of the jaw: Report of a task force of the American Society for Bone and Mineral Research. J. Bone Miner. Res. 2007, 22, 1479–1491. [Google Scholar]
- Garetto, L.P.; Tricker, N.D. Remodeling of bone surrounding the implant interface. In Bridging the Gap between Dental and Orthopaedic Implants, Proceedings of the 3rd Annual Indiana Conference, Indianapolis, IN, USA, 13–16 May 1998; Garetto, L.P., Turner, C.H., Duncan, R.L., Burr, D.B., Eds.; Indiana University School of Dentistry: Indianapolis, IN, USA, 2002. [Google Scholar]
- Huja, S.S.; Fernandez, S.A.; Hill, K.J.; Li, Y. Remodeling dynamics in the alveolar process in skeletally mature dogs. Anat. Rec. A Discov. Mol. Cell. Evol. Biol. 2006, 288, 1243–1249. [Google Scholar]
- Van Poznak, C.; Estilo, C. Osteonecrosis of the jaw in cancer patients receiving IV bisphosphonates. Oncology 2006, 20, 1053–1062. [Google Scholar]
- Ruggiero, S.L.; Fantasia, J.; Carlson, E. Bisphosphonate-related osteonecrosis of the jaw: Background and guidelines for diagnosis, staging and management. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 102, 433–441. [Google Scholar]
- Li, C.Y.; Schaffler, M.B.; Wolde-Semait, H.T.; Hernandez, C.J.; Jepsen, K.J. Genetic background influences cortical bone response to ovariectomy. J. Bone Miner. Res. 2005, 20, 2150–2158. [Google Scholar]
- Holtmann, H.; Lommen, J.; Kübler, N.R.; Sproll, C.; Rana, M.; Karschuck, P.; Depprich, R. Pathogenesis of medication-related osteonecrosis of the jaw: A comparative study of in vivo and in vitro trials. J. Int. Med. Res. 2018, 46, 4277–4296. [Google Scholar]
- Vasconcelos, A.C.U.; Berti-Couto, S.A.; Azambuja, A.A.; Salum, F.G.; Figueiredo, M.A.; Da Silva, V.D.; Cherubini, K. Comparison of effects of clodronate and zoledronic acid on the repair of maxilla surgical wounds–histomorphometric, receptor activator of nuclear factor-kB ligand, osteoprotegerin, von Willebrand factor, and caspase-3 evaluation. J. Oral Pathol. Med. 2012, 41, 702–712. [Google Scholar]
- Janovszky, Á.; Szabó, A.; Varga, R.; Garab, D.; Borós, M.; Mester, C.; Beretka, N.; Zombori, T.; Wiesmann, H.-P.; Bernhardt, R.; et al. Periosteal microcirculatory reactions in a zoledronate-induced osteonecrosis model of the jaw in rats. Clin. Oral Investig. 2015, 19, 1279–1288. [Google Scholar]
- Abtahi, J.; Agholme, F.; Sandberg, O.; Aspenberg, P. Effect of local vs. systemic bisphosphonate delivery on dental implant fixation in a model of osteonecrosis of the jaw. J. Dent. Res. 2013, 92, 279–283. [Google Scholar]
- Sonis, S.T.; Watkins, B.A.; Lyng, G.D.; Lerman, M.A.; Anderson, K.C. Bony changes in the jaws of rats treated with zoledronic acid and dexamethasone before dental extractions mimic bisphosphonate-related osteonecrosis in cancer patients. Oral Oncol. 2009, 45, 164–172. [Google Scholar]
- Song, M.; AlShaikh, A.; Kim, T.; Kim, S.; Dang, M.; Mehrazarin, S.; Shin, K.-H.; Kang, M.; Park, N.-H.; Kim, R.H. Preexisting periapical inflammatory condition exacerbates tooth extraction–induced bisphosphonate-related osteonecrosis of the jaw lesions in mice. J. Endod. 2016, 42, 1641–1646. [Google Scholar]
- Kuroshima, S.; Yamashita, J. Chemotherapeutic and antiresorptive combination therapy suppressed lymphangiogenesis and induced osteonecrosis of the jaw-like lesions in mice. Bone 2013, 56, 101–109. [Google Scholar]
- Aghaloo, T.L.; Cheong, S.; Bezouglaia, O.; Kostenuik, P.; Atti, E.; Dry, S.M.; Pirih, F.Q.; Tetradis, S. RANKL inhibitors induce osteonecrosis of the jaw in mice with periapical disease. J. Bone Miner. Res. 2014, 29, 843–854. [Google Scholar]
- Pautke, C.; Kreutzer, K.; Weitz, J.; Knödler, M.; Münzel, D.; Wexel, G.; Otto, S.; Hapfelmeier, A.; Sturzenbaum, S.; Tischer, T. Bisphosphonate related osteonecrosis of the jaw: A minipig large animal model. Bone 2012, 51, 592–599. [Google Scholar]
- Li, Y.; Xu, J.; Mao, L.; Liu, Y.; Gao, R.; Zheng, Z.; Chen, W.; Le, A.; Shi, S.; Wang, S. Allogeneic mesenchymal stem cell therapy for bisphosphonate-related jaw osteonecrosis in swine. Stem Cells Dev. 2013, 22, 2047–2056. [Google Scholar]
- Voss, P.J.; Stoddart, M.J.; Bernstein, A.; Schmelzeisen, R.; Nelson, K.; Stadelmann, V.A.; Ziebart, T.; Poxleitner, P. Zoledronate induces bisphosphonate-related osteonecrosis of the jaw in osteopenic sheep. Clin. Oral Investig. 2016, 20, 31–38. [Google Scholar]
- Moreira, C.A.; Costa, T.M.R.L.; Marques, J.V.O.; Sylvestre, L.; Almeida, A.C.R.; Maluf, E.M.C.P.; Borba, V.Z.C. Prevalence and clinical characteristics of X-linked hypophosphatemia in Paraná, southern Brazil. Arch. Endocrinol. Metab. 2020, 64, 796–802. [Google Scholar]
- Bhadada, S.K.; Bhansali, A.; Upreti, V.; Dutta, P.; Santosh, R.; Das, S.; Nahar, U. Hypophosphataemic rickets/osteomalacia: A descriptive analysis. Indian J. Med Res. 2010, 131, 399. [Google Scholar]
- Laurent, M.R.; Bravenboer, N.; van Schoor, N.M.; Bouillon, R.; Pettifor, J.M.; Lips, P. Rickets and osteomalacia. In Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism; John Wiley & Sons: Newark, NJ, USA, 2018; pp. 684–694. [Google Scholar]
- Feng, J.Q.; Clinkenbeard, E.L.; Yuan, B.; White, K.E.; Drezner, M.K. Osteocyte regulation of phosphate homeostasis and bone mineralization underlies the pathophysiology of the heritable disorders of rickets and osteomalacia. Bone 2013, 54, 213–221. [Google Scholar]
- Homan, E.P.; Rauch, F.; Grafe, I.; Lietman, C.; Doll, J.A.; Dawson, B.; Bertin, T.; Napierala, D.; Morello, R.; Gibbs, R.; et al. Mutations in SERPINF1 cause osteogenesis imperfecta type VI. J. Bone Miner. Res. 2011, 26, 2798–2803. [Google Scholar]
- Frame, B.; Frost, H.M.; Pak, C.Y.; Reynolds, W.; Argen, R.J. Fibrogenesis imperfecta ossium: A collagen defect causing osteomalacia. N. Engl. J. Med. 1971, 285, 769–772. [Google Scholar]
- Herm, F.; Killguss, H.; Stewart, A. Osteomalacia in Hazara District, Pakistan. Trop. Dr. 2005, 35, 8–10. [Google Scholar]
- Campbell, A.G.; Hosking, D.J.; Kemm, J.R.; Boyd, R.V. How common is osteomalacia in the elderly? Lancet 1984, 324, 386–388. [Google Scholar]
- Lips, P. Vitamin D deficiency and secondary hyperparathyroidism in the elderly: Consequences for bone loss and fractures and therapeutic implications. Endocr. Rev. 2001, 22, 477–501. [Google Scholar]
- Priemel, M.; Von Domarus, C.; Klatte, T.O.; Kessler, S.; Schlie, J.; Meier, S.; Proksch, N.; Pastor, F.; Netter, C.; Streichert, T.; et al. Bone mineralization defects and vitamin D deficiency: Histomorphometric analysis of iliac crest bone biopsies and circulating 25-hydroxyvitamin D in 675 patients. J. Bone Miner. Res. 2010, 25, 305–312. [Google Scholar]
- Rabelink, N.M.; Westgeest, H.M.; Bravenboer, N.; Jacobs, M.A.J.M.; Lips, P. Bone pain and extremely low bone mineral density due to severe vitamin D deficiency in celiac disease. Arch. Osteoporos. 2011, 6, 209–213. [Google Scholar]
- Parfitt, A.; Pødenphant, J.; Villanueva, A.; Frame, B. Metabolic bone disease with and without osteomalacia after intestinal bypass surgery: A bone histomorphometric study. Bone 1985, 6, 211–220. [Google Scholar]
- Bisballe, S.; Eriksen, E.F.; Melsen, F.; Mosekilde, L.; Sorensen, O.H.; Hessov, I. Osteopenia and osteomalacia after gastrectomy: Interrelations between biochemical markers of bone remodelling, vitamin D metabolites, and bone histomorphometry. Gut 1991, 32, 1303–1307. [Google Scholar]
- Gupta, D.; Vashi, P.G.; Trukova, K.; Lis, C.G.; Lammersfeld, C.A. Prevalence of serum vitamin D deficiency and insufficiency in cancer: Review of the epidemiological literature. Exp. Ther. Med. 2011, 2, 181–193. [Google Scholar]
- Nogués, X.; Servitja, S.; Peña, M.J.; Prieto-Alhambra, D.; Nadal, R.; Mellibovsky, L.; Albanell, J.; Diez-Perez, A.; Tusquets, I. Vitamin D deficiency and bone mineral density in postmenopausal women receiving aromatase inhibitors for early breast cancer. Maturitas 2010, 66, 291–297. [Google Scholar]
- Neuhouser, M.L.; Bernstein, L.; Hollis, B.W.; Xiao, L.; Ambs, A.; Baumgartner, K.; Baumgartner, R.; McTiernan, A.; Ballard-Barbash, R. Serum vitamin D and breast density in breast cancer survivors. Cancer Epidemiol. Prev. Biomark. 2010, 19, 412–417. [Google Scholar]
- Crew, K.D.; Shane, E.; Cremers, S.; McMahon, D.J.; Irani, D.; Hershman, D.L. High prevalence of vitamin D deficiency despite supplementation in premenopausal women with breast cancer undergoing adjuvant chemotherapy. J. Clin. Oncol. 2009, 27, 2151. [Google Scholar]
- Rainville, C.; Khan, Y.; Tisman, G. Triple negative breast cancer patients presenting with low serum vitamin D levels: A case series. Cases J. 2009, 2, 1–5. [Google Scholar]
- Neuhouser, M.L.; Sorensen, B.; Hollis, B.W.; Ambs, A.; Ulrich, C.M.; McTiernan, A.; Bernstein, L.; Wayne, S.; Gilliland, F.; Baumgartner, K.; et al. Vitamin D insufficiency in a multiethnic cohort of breast cancer survivors. Am. J. Clin. Nutr. 2008, 88, 133–139. [Google Scholar]
- Fakih, M.G.; Trump, D.L.; Johnson, C.S.; Tian, L.; Muindi, J.; Sunga, A.Y. Chemotherapy is linked to severe vitamin D deficiency in patients with colorectal cancer. Int. J. Colorectal Dis. 2009, 24, 219–224. [Google Scholar]
- Trump, D.L.; Chadha, M.K.; Sunga, A.Y.; Fakih, M.G.; Ashraf, U.; Silliman, C.G.; Hollis, B.W.; Nesline, M.K.; Tian, L.; Tan, W.; et al. Vitamin D deficiency and insufficiency among patients with prostate cancer. BJU Int. 2009, 104, 909. [Google Scholar]
- Maier, G.S.; Horas, K.; Kurth, A.A.; Lazovic, D.; Seeger, J.B.; Maus, U. Prevalence of vitamin D deficiency in patients with bone metastases and multiple myeloma. Anticancer Res. 2015, 35, 6281–6285. [Google Scholar]
- Jagelavičienė, E.; Vaitkevičienė, I.; Šilingaitė, D.; Šinkūnaitė, E.; Daugėlaitė, G. The relationship between vitamin D and periodontal pathology. Medicina 2018, 54, 45. [Google Scholar]
- Alshouibi, E.; Kaye, E.; Cabral, H.; Leone, C.; Garcia, R. Vitamin D and periodontal health in older men. J. Dent. Res. 2013, 92, 689–693. [Google Scholar]
- Zhou, F.; Zhou, Y.; Shi, J. The association between serum 25-hydroxyvitamin D levels and dental caries in US adults. Oral Dis. 2020, 26, 1537–1547. [Google Scholar]
- Kim, I.-J.; Lee, H.-S.; Ju, H.-J.; Na, J.-Y.; Oh, H.-W. A cross-sectional study on the association between vitamin D levels and caries in the permanent dentition of Korean children. BMC Oral Health 2018, 18, 1–6. [Google Scholar]
- Chhonkar, A.; Gupta, A.; Arya, V. Comparison of vitamin D level of children with severe early childhood caries and children with no caries. Int. J. Clin. Pediatric Dent. 2018, 11, 199. [Google Scholar]
- Deane, S.; Schroth, R.J.; Sharma, A.; Rodd, C. Combined deficiencies of 25-hydroxyvitamin D and anemia in preschool children with severe early childhood caries: A case–control study. Paediatr. Child Health 2018, 23, e40–e45. [Google Scholar]
- Danila, M.I.; Outman, R.C.; Rahn, E.J.; Mudano, A.S.; Redden, D.T.; Li, P.; Allison, J.J.; Anderson, F.A.; Wyman, A.; Greenspan, S.L.; et al. Evaluation of a multimodal, direct-to-patient educational intervention targeting barriers to osteoporosis care: A randomized clinical trial. J. Bone Miner. Res. 2018, 33, 763–772. [Google Scholar]
- Heim, N.; Warwas, F.B.; Wilms, C.T.; Reich, R.H.; Martini, M. Vitamin D (25-OHD) deficiency may increase the prevalence of medication-related osteonecrosis of the jaw. J. Cranio-Maxillofac. Surg. 2017, 45, 2068–2074. [Google Scholar]
- Demircan, S.; Isler, S. Changes in serological bone turnover markers in bisphosphonate induced osteonecrosis of the jaws: A case control study. Niger. J. Clin. Pract. 2020, 23, 154. [Google Scholar]
- Bedogni, A.; Saia, G.; Bettini, G.; Tronchet, A.; Totola, A.; Bedogni, G.; Tregnago, P.; Valenti, M.T.; Bertoldo, F.; Ferronato, G.; et al. Osteomalacia: The missing link in the pathogenesis of bisphosphonate-related osteonecrosis of the jaws? Oncologist 2012, 17, 1114. [Google Scholar]
- Boyce, B.F.; Adamson, B.B.; Gallacher, S.J.; Byars, J.; Ralston, S.H.; Boyle, I.T. Mineralisation defects after pamidronate for Paget’s disease. Lancet 1994, 343, 1231–1232. [Google Scholar]
- Jakob, T.; Tesfamariam, Y.M.; Macherey, S.; Kuhr, K.; Adams, A.; Monsef, I.; Heidenreich, A.; Skoetz, N. Bisphosphonates or RANK-ligand-inhibitors for men with prostate cancer and bone metastases: A network meta-analysis. Cochrane Database Syst. Rev. 2020, 12, CD013020. [Google Scholar]
- Endo, Y.; Funayama, H.; Yamaguchi, K.; Monma, Y.; Yu, Z.; Deng, X.; Oizumi, T.; Shikama, Y.; Tanaka, Y.; Okada, S.; et al. Basic Studies on the Mechanism, Prevention, and Treatment of Osteonecrosis of the Jaw Induced by Bisphosphonates. Yakugaku zasshi: J. Pharm. Soc. Japan 2020, 140, 63–79. [Google Scholar]
- Suzuki, K.; Takeyama, S.; Murakami, S.; Nagaoka, M.; Chiba, M.; Igarashi, K.; Shinoda, H. Structure-Dependent Effects of Bisphosphonates on Inflammatory Responses in Cultured Neonatal Mouse Calvaria. Antioxidants 2020, 9, 503. [Google Scholar]
- D’Andrea, S.; Martorella, A.; Coccia, F.; Castellini, C.; Minaldi, E.; Totaro, M.; Parisi, A.; Francavilla, F.; Barbonetti, A. Relationship of Vitamin D status with testosterone levels: A systematic review and meta-analysis. Endocrine 2020. [Google Scholar] [CrossRef]
- Monier-Faugere, M.C.; Mawad, H.; Qi, Q.; Friedler, R.M.; Malluche, H.H. High prevalence of low bone turnover and occurrence of osteomalacia after kidney transplantation. J. Am. Soc. Nephrol. 2000, 11, 1093–1099. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1. | ONJ is a severe and multifactorial clinical condition |
| 2. | ONJ incidence is low in cancer, almost irrelevant in osteoporosis |
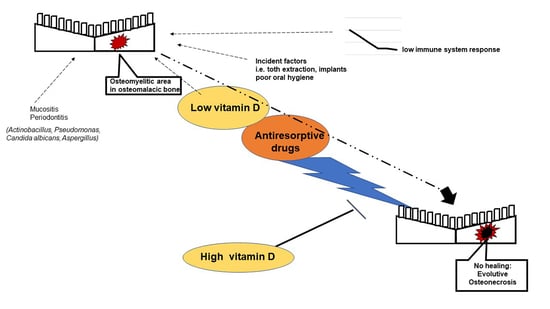
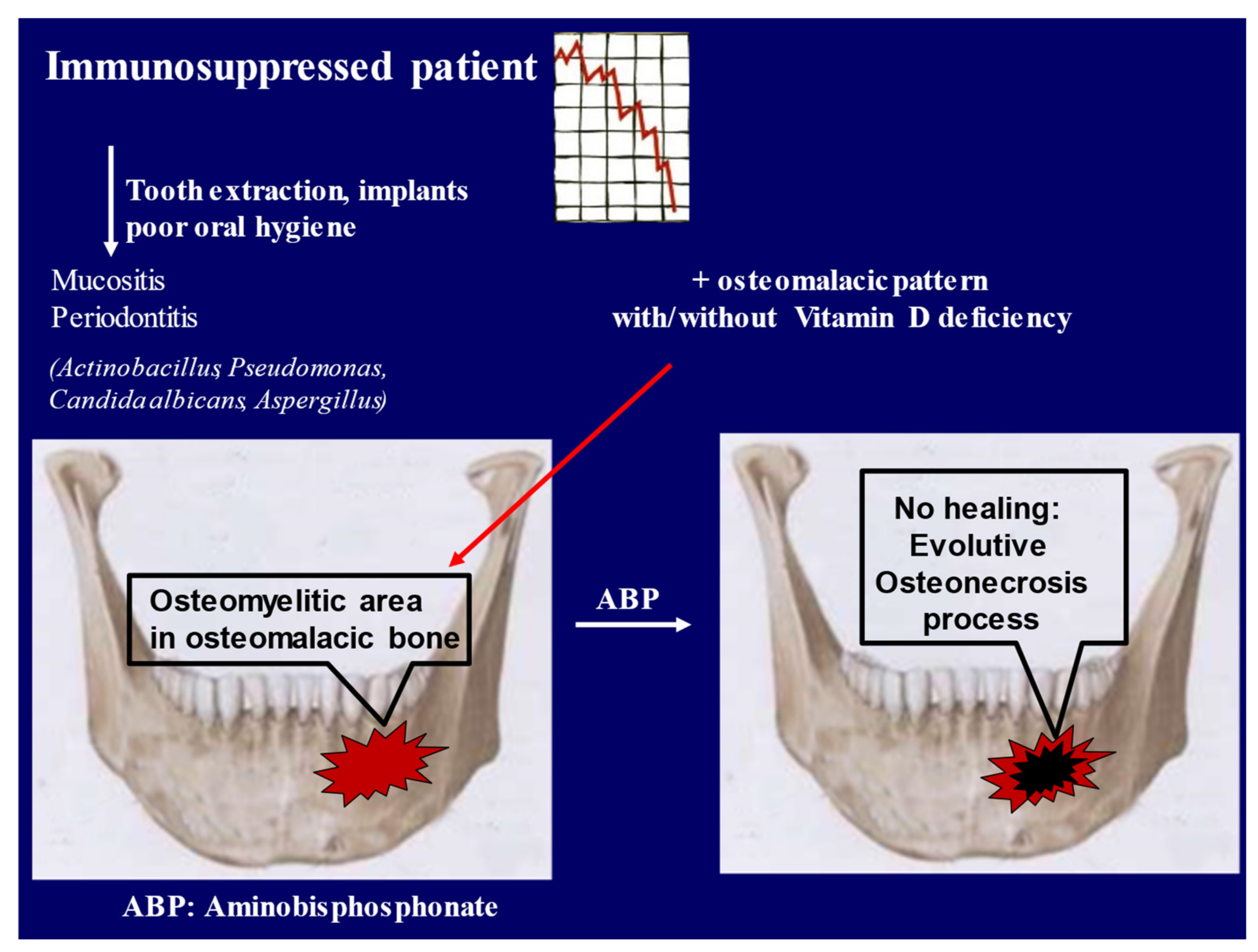
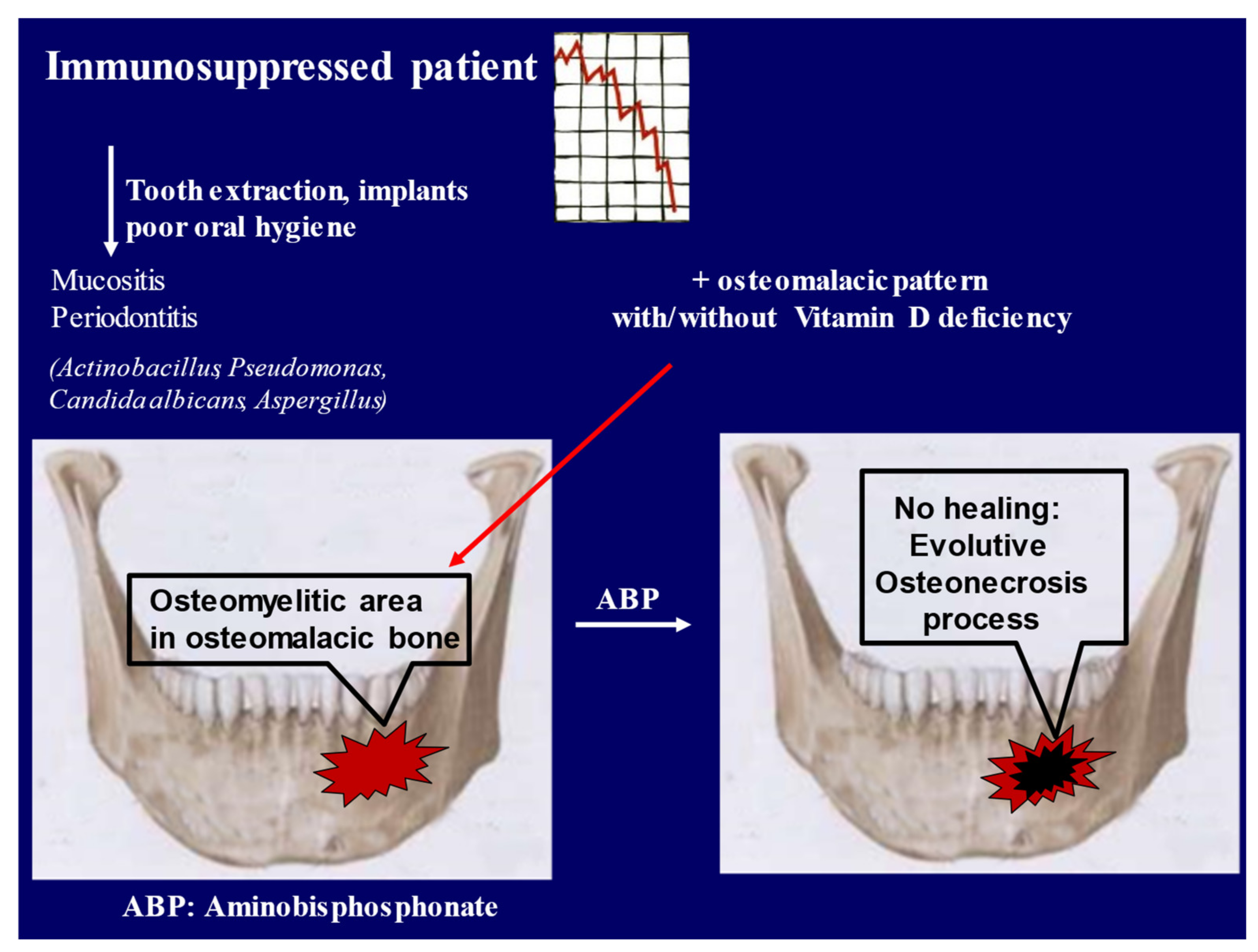
| 3. | The incident factors are: immunodeficiency, assumption of drugs such as glucocorticoids, dental interventions, oral and gingival infections |
| 4. | A general or local osteomalacia condition may be the main factor in the pathogenetic involvement of antiresorptive drugs |
| 5. | Vitamin D is important in the prevention of ONJ |
| 6. | The safety levels of 25-OH vitamin D in this pattern need to be specifically investigated |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dalle Carbonare, L.; Mottes, M.; Valenti, M.T. Medication-Related Osteonecrosis of the Jaw (MRONJ): Are Antiresorptive Drugs the Main Culprits or Only Accomplices? The Triggering Role of Vitamin D Deficiency. Nutrients 2021, 13, 561. https://doi.org/10.3390/nu13020561
Dalle Carbonare L, Mottes M, Valenti MT. Medication-Related Osteonecrosis of the Jaw (MRONJ): Are Antiresorptive Drugs the Main Culprits or Only Accomplices? The Triggering Role of Vitamin D Deficiency. Nutrients. 2021; 13(2):561. https://doi.org/10.3390/nu13020561
Chicago/Turabian StyleDalle Carbonare, Luca, Monica Mottes, and Maria Teresa Valenti. 2021. "Medication-Related Osteonecrosis of the Jaw (MRONJ): Are Antiresorptive Drugs the Main Culprits or Only Accomplices? The Triggering Role of Vitamin D Deficiency" Nutrients 13, no. 2: 561. https://doi.org/10.3390/nu13020561
APA StyleDalle Carbonare, L., Mottes, M., & Valenti, M. T. (2021). Medication-Related Osteonecrosis of the Jaw (MRONJ): Are Antiresorptive Drugs the Main Culprits or Only Accomplices? The Triggering Role of Vitamin D Deficiency. Nutrients, 13(2), 561. https://doi.org/10.3390/nu13020561