Risk Factors for Muscle Loss in Hemodialysis Patients with High Comorbidity
by

Wesley J. Visser
1, 
Anneke M.E. de Mik-van Egmond
1,
Reinier Timman
2,3,
David Severs
4 and
Ewout J. Hoorn
4,* 1
Department of Internal Medicine, Division of Dietetics, Erasmus MC, University Medical Center, 3015 GD Rotterdam, The Netherlands
2
Department of Internal Medicine, Erasmus MC, University Medical Center, 3015 GD Rotterdam, The Netherlands
3
Department of Psychiatry, Erasmus MC, University Medical Center, 3015 GD Rotterdam, The Netherlands
4
Department of Internal Medicine, Division of Nephrology and Transplantation, Erasmus MC, University Medical Center, 3015 GD Rotterdam, The Netherlands
*
Author to whom correspondence should be addressed.
Nutrients 2020, 12(9), 2494; https://doi.org/10.3390/nu12092494
Submission received: 30 June 2020
/
Revised: 10 August 2020
/
Accepted: 14 August 2020
/
Published: 19 August 2020
(This article belongs to the Section Nutrition Methodology & Assessment)
Abstract
:With expanding kidney transplantation programs, remaining hemodialysis patients are more likely to have a high comorbidity burden and may therefore be more prone to lose muscle mass. Our aim was to analyze risk factors for muscle loss in hemodialysis patients with high comorbidity. Fifty-four chronic hemodialysis patients (Charlson Comorbidity Index 9.0 ± 3.4) were followed for 20 weeks using 4-weekly measurements of lean tissue mass, intracellular water, and body cell mass (proxies for muscle mass), handgrip strength (HGS), and biochemical parameters. Mixed models were used to analyze covariate effects on LTM. LTM (−6.4 kg, interquartile range [IQR] −8.1 to −4.8), HGS (−1.9 kg, IQR −3.1 to −0.7), intracellular water (−2.11 L, IQR −2.9 to −1.4) and body cell mass (−4.30 kg, IQR −5.9 to −2.9) decreased in all patients. Conversely, adipose tissue mass increased (4.5 kg, IQR 2.7 to 6.2), resulting in no significant change in body weight (−0.5 kg, IQR −1.0 to 0.1). Independent risk factors for LTM loss over time were male sex (−0.26 kg/week, 95% CI −0.33 to −0.19), C-reactive protein above median (−0.1 kg/week, 95% CI −0.2 to −0.001), and baseline lean tissue index ≥10th percentile (−1.6 kg/week, 95% CI −2.1 to −1.0). Age, dialysis vintage, serum albumin, comorbidity index, and diabetes did not significantly affect LTM loss over time. In this cohort with high comorbidity, we found universal and prominent muscle loss, which was further accelerated by male sex and inflammation. Stable body weight may mask muscle loss because of concurrent fat gain. Our data emphasize the need to assess body composition in all hemodialysis patients and call for studies to analyze whether intervention with nutrition or exercise may curtail muscle loss in the most vulnerable hemodialysis patients.
1. Introduction
In patients with chronic kidney disease (CKD) who undergo chronic hemodialysis, nutritional status, body composition, and especially muscle mass, are closely linked to morbidity, mortality, and quality of life [1,2,3]. There are multiple factors that lead to muscle mass loss in patients undergoing hemodialysis. First, with progression of CKD, there is a decline in protein intake [4], and anorexia is reported in approximately one-third of hemodialysis patients [5]. Second, fluid restriction may lead to a concurrent decrease in caloric intake [6]. Third, the hemodialysis procedure itself may contribute to the catabolic state due to decreased protein synthesis and increased proteolysis [7,8]. Finally, additional catabolic factors may be present that lead to muscle mass loss in hemodialysis patients including acidosis, comorbidity, inflammation, corticosteroid use, and sedentary lifestyle [9,10].
With expanding kidney transplantation programs, remaining hemodialysis patients are more likely to have a high comorbidity burden and may therefore be more prone to lose muscle mass. Therefore, we hypothesized that loss of muscle mass and muscle strength is especially prominent in hemodialysis patients with a high comorbidity burden. The Netherlands has a high kidney transplantation rate per million population [11]. Our university hospital harbors a large kidney transplantation program (approximately 200 transplantations per year). Accordingly, a relatively large proportion of our in-center hemodialysis population cannot be transplanted because of comorbidity. We considered that this specific hemodialysis population was suitable to address our hypothesis. Indeed, in this prospective longitudinal study, we find a dramatic and universal loss of both muscle mass and muscle strength in hemodialysis patients with high comorbidity. This particular group may be especially suited for interventions with nutrition or exercise.
2. Materials and Methods
2.1. Study Design and Subjects
The study protocol was reviewed and approved by our medical ethical review board (MEC-2017-445). We prospectively included adult patients undergoing chronic in-center hemodialysis from September to December 2017. All patients were included except if they had specific exclusion criteria, including life expectancy ≤6 months, active treatment for malignancy or infection, a (unipolar) pacemaker, and the use of intradialytic parenteral nutrition (IDPN). The first measurement of this study, regardless of dialysis vintage, was defined as the baseline measurement. Patients were followed for a minimum of 3 to a maximum of 6 measurements with 4-weekly study visits. Our standard of care includes a target spKt/V >1.4 and predialysis plasma bicarbonate >22 mmol/L. Dietary advice and support were provided to all subjects as standard policy. Dietary counseling includes an advice for protein requirement in the range of 1.0–1.2 g/kg and for patients with malnutrition or inflammation 1.2–1.5 g/kg and a calculation of the individual energy requirement by adding 30% to the estimated resting energy expenditure [12]. For all patients who did not meet their nutritional requirements, sip feeding, tube feeding and/or intradialytic parenteral nutrition is a possible treatment. During dialysis, we offer all patients energy and protein-rich food.
2.2. Measurements
Body composition was assessed with the Body Composition Monitor (Fresenius Medical Care, Bad Homburg, Germany), which is based on bio-impedance spectroscopy (BIS) at 50 different frequencies ranging between 5 and 1000 kHz. The Body Composition Monitor has been validated against gold-standard reference methods [13] and has the ability to differentiate between excess fluid and normally hydrated lean tissue mass [14]. The following parameters were generated during each measurement: total body water (TBW), extracellular water (ECW), intracellular water (ICW), lean tissue mass (LTM), body cell mass (BCM), adipose tissue mass (ATM), phase angle, and estimated predialysis overhydration. Lean tissue index (LTI) and fat tissue index (FTI) were calculated respectively as LTM and ATM divided by height2 (kg/m2) and compared with reference values (10th percentile) for age and gender [15]. Phase angle is an measure related to body cell mass and the ratio between extracellular and intracellular fluid, and is calculated as the arc tangent of reactance over resistance. BIS measurements were performed using a standardized protocol and experienced operators before the start of the dialysis session. Dry weight was recorded from the dialysis prescription most recent from each study visit. Physical function was assessed by handgrip strength measured with a hand dynamometer (hydraulic, JAMAR; Patterson Medical, Warrenville, IL, USA). The test was performed in a sitting position, with the patient instructed to perform three consecutive contractions with both hands (except for AV fistula side). The highest value was compared with reference values [16]. Protein intake was estimated by the normalized protein catabolic rate (nPCR) [17]. The nPCR is based on interdialytic (ID) changes in blood urea nitrogen (BUN) concentrations and urinary protein and urea excretion, where nPCR in g/kg per day = 0.22 + (0.036 × ID rise in BUN × 24)/ID interval (hours). In patients with urine output ≥200 mL/day, we added the following calculation to the equation: urinary urea nitrogen (g) × 150/ID interval (hours) × weight (kg) [17]. Serum albumin (bromocresol green method), and serum C-reactive protein (CRP) were measured using the Cobas 8000 modular analyzer series (Roche Diagnostics, Almere, The Netherlands). Blood samples were taken every four weeks before dialysis. For assessing comorbidity, we used the Charlson Comorbidity Index [18].
2.3. Statistical Analysis
The primary endpoint was LTM, which was measured 3 to 6 times during this study. For the longitudinal analyses, mixed models were applied. The results from the mixed models analyses are reported in the tables, while recorded data are shown in Figure 1. Two levels were included in the mixed models, of which the upper level represented the patients and the lower level their repeated measures. Time was postulated as a continuous linear fixed effect. The covariance structure was determined with the deviance statistic [19] using restricted maximum likelihood [20]. The statistical analyses for the secondary study parameters were the same as for the primary endpoint. For the exploration of potential influences of the covariates, the multilevel analyses were extended with these effects and their interactions with time as covariates. These covariates were gender, age < or ≥65 years, LTI < or ≥10th percentile, dialysis vintage < or ≥12 months, CCI < or ≥mean, serum CRP and albumin levels below or above median (all as dichotomous variables). Dropout analyses were performed with independent group t-tests by comparing baseline LTM measures between the retained and dropped-out patients at 20 weeks. p-values < 0.05 were considered statistically significant. Statistical analyses were performed with IBM-SPSS version 24.
3. Results
3.1. Baseline Characteristics
Sixty-four hemodialysis patients were screened for inclusion, of whom 54 were included. Reasons for exclusion were a unipolar pacemaker (n = 1), active treatment for malignancy (n = 2) or infection (n = 2), and the use of intradialytic parenteral nutrition (n = 5). Baseline characteristics are shown in Table 1. Our cohort was relatively old, consisted predominantly of males, and had a high prevalence of diabetes and cardiovascular disease. This resulted in a high Charlson Comorbidity Index (9.0 ± 3.4). All 54 included patients were followed up for at least 8 weeks (3 study visits), while 37 patients completed the 20 week visit (6 study visits). There was no significant difference in baseline LTM between patients with three and patients with six measurements (39.8 vs. 37.1 kg; p = 0.5). Loss to follow up was uniformly caused by transfer to other dialysis centers.
3.2. Lean Tissue Mass Is Replaced by Adipose Tissue Mass
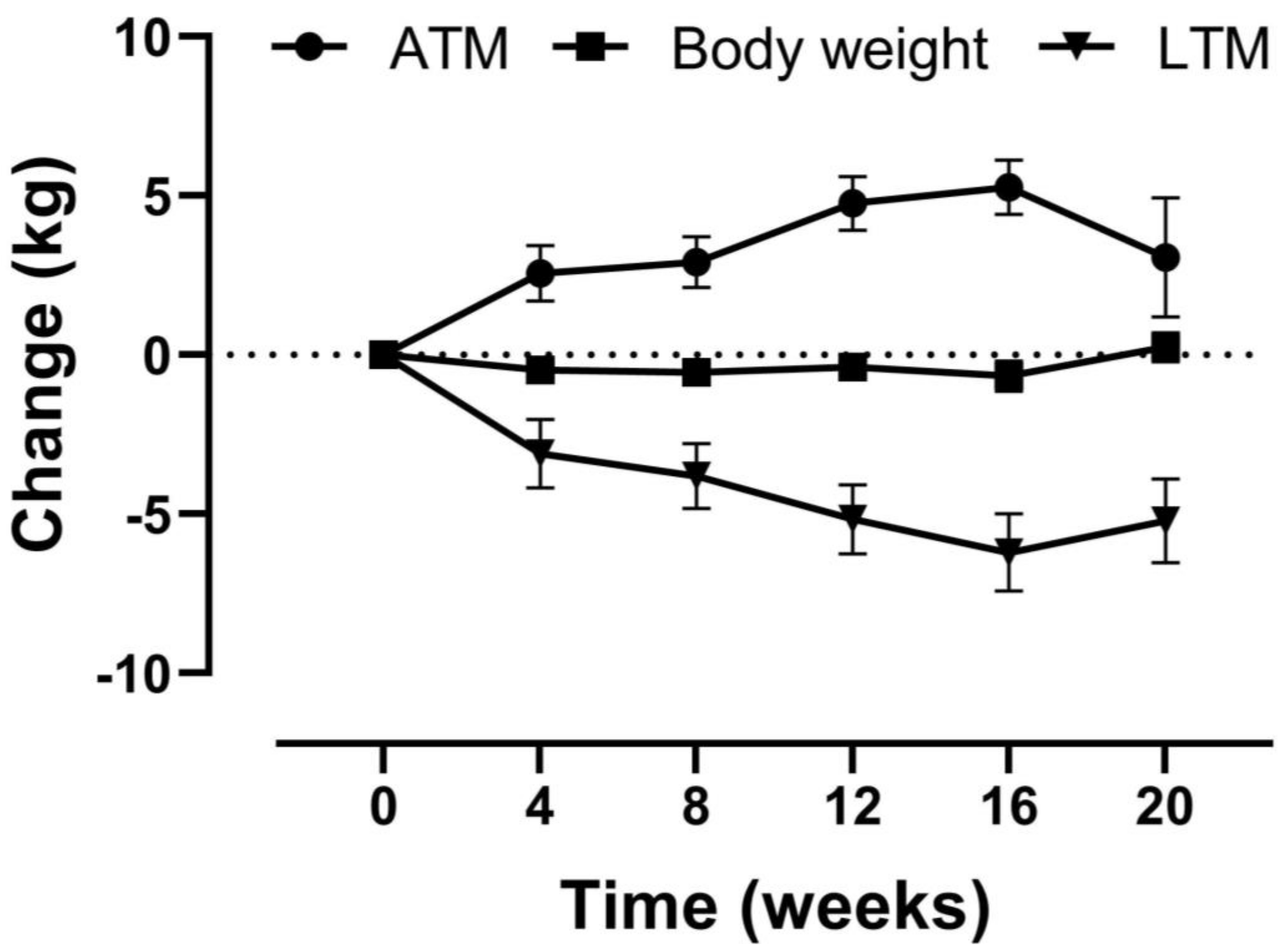
Body weight did not decrease significantly in 20 weeks (−0.5 kg, 95% confidence interval [CI] −1.0 to 0.1), which was caused by a decrease in LTM (−6.4 kg, 95% CI −8.1 to −4.8) and an increase in ATM (4.5 kg, 95% CI 2.7 to 6.2, Table 2 and Figure 1). In addition to LTM, ICW (−2.11 L, 95% CI −2.9 to −1.4) and BCM (−4.30 kg, 95% CI −5.9 to −2.9) also decreased significantly (Table 2). Handgrip strength decreased by −1.9 kg (95% CI −3.1 to −0.7). There were no significant changes over time in phase angle, predialysis overhydration, nPCR, serum albumin, and serum CRP (Table 2). In addition, no significant changes were observed in target dry weight and body mass index (data not shown). A sensitivity analysis was performed including only those participants with complete follow up, which showed similar results (Table S1).
3.3. Male Sex and Inflammation Accelerate Loss of Lean Tissue Mass
All patients demonstrated a significant loss of LTM over time, regardless of stratifying the covariates age, sex, LTI, baseline serum CRP, serum albumin, dialysis vintage, diabetes, or comorbidity index (Table 3). However, LTM loss over time was greater in males and patients with higher baseline CRP and LTI. These covariates remained independent predictors of greater LTM loss in the multivariate analysis (Table 4). The presence of diabetes, lower serum albumin, longer dialysis vintage, and higher comorbidity index were not associated with greater LTM loss over time.
4. Discussion
The aim of this prospective and longitudinal study was to identify risk factors for muscle loss in chronic hemodialysis patients with high comorbidity. To do so, we performed serial measurements of lean tissue mass (LTM) as a proxy for muscle mass. The results show that all patients experienced muscle loss and that on average this loss was very pronounced (−6.4 kg in 20 weeks or ~1.3 kg/month). Muscle loss was further accelerated by male sex and by inflammation. Because we focused specifically on hemodialysis patients with high comorbidity, the magnitude of the changes in body composition was considerably greater in this study than in most previous studies (summarized in Table 5). We also show that muscle loss was not reflected by a change in body weight or body mass index, because of a concurrent gain in fat mass. This is the first study to analyze muscle loss in hemodialysis patients with high comorbidity and our results suggest that this specific patient category may benefit from nutritional or exercise interventions. Our study also reinforces the need to more routinely perform body composition monitoring to estimate muscle mass. Additional strengths of this study are the inclusion of patients regardless of dialysis vintage and the inclusion of handgrip strength, a measure of muscle function that correlates well with physical function and all-cause mortality [21,22].
The link between inflammation and muscle loss that we identified in this study has been reported previously [32]. Inflammation may decrease protein anabolism, increase protein catabolism, or both [33]. A state of low-grade inflammation, as indicated by elevated CRP or other acute-phase reactants, is highly common in patients undergoing dialysis treatment [34]. Remarkably, this effect on LTM loss has not previously been demonstrated in longitudinal studies in hemodialysis patients, although Johansen et al. did report an association between higher interleukin 1β concentrations [29]. Patients in our study had a higher CRP than in most previous reports (Table 5) [24,28,29]. In addition to CRP, serum albumin correlates with LTM in chronic kidney disease patients [35]. Moreover, serum albumin usually inversely correlates with inflammatory parameters [36]. Our failure to detect this effect, as well as the relatively high serum albumin concentrations in our population, may partly be explained by the measurement method we employed. The bromocresol green assay used in this study significantly overestimates serum albumin concentrations when compared with reference immunoassays [37]. Importantly, interference by acute-phase reactants is partially responsible for this error [38], which could have led to an underestimation of the effect of serum albumin concentration on LTM loss in our study.
The observation that males on hemodialysis have a greater loss of muscle mass than females was also reported by Marcelli et al. [24] and may be related to the response to inflammation [39]. For example, male but not female dialysis patients with inflammation have worse outcomes [40]. There are clear sex differences in skeletal muscle kinetics and fiber-type composition [41]. In addition, there are several theoretical explanations for sex differences in muscle wasting, including the anabolic effects of testosterone, and the anti-inflammatory effects of estrogen [42,43]. Testosterone deficiency is especially common in male dialysis patients with low muscle mass [44] and this may have contributed to the greater LTM loss over time. Conversely, estrogen may have exerted an anti-inflammatory effect in the premenopausal women included in this study.
Three other observations in this study merit discussion. First, we found that patients with LTI > P10 at baseline were also more prone for LTM loss over time. This seems logical, because these patients “have more to lose”. Yet, this finding is clinically relevant, because patients with higher LTM at baseline will likely not be selected for close monitoring of nutritional status. The need for monitoring of nutritional status was also illustrated by the fact that the baseline BMI was 25.6 kg/m2, whereas 76% of the patients had some degree of malnutrition according to SGA and 48% had an LTI < P10. Second, the rate of LTM loss over time was not significantly influenced by the presence of diabetes mellitus, which differs from the study by Pupim et al. [28]. Interestingly, in that study, patients with diabetes had a significantly higher baseline LTM than patients without diabetes, while we observed the opposite in our cohort. This may be explained by differences in study population, measurement methods (DEXA vs. BIS), or dialysis vintage. Third, in our study the magnitude of LTM loss was not significantly affected by dialysis vintage. The observation that “stable” hemodialysis patients may still lose significant muscle mass corresponds with findings by Molina et al., who reported a mean 12-month decrease in LTM of 6.8 kg in a population with a median dialysis vintage of 40 months [23]. In contrast, Chertow et al. found only a small negative effect of vintage on body cell mass in a large patient sample [45]. Importantly, cross-sectional analyses such as theirs probably underestimate changes in body composition. We argue that factors that precipitate loss of muscle mass likely exist irrespective of dialysis vintage.
This study has a number of limitations. First, this is a single-center observational study with relatively short follow up, and therefore the results may not be generalizable to other settings. However, our specific aim was to address muscle loss in hemodialysis patients with high comorbidity. Therefore, our specific hypothesis was addressable in this specific patient population whose Charlson Comorbidity Index was clearly higher than in previous studies [46,47,48]. A second limitation may be that not all patients completed all visits and that the sample size was moderate. However, we applied specific statistical methodology to account for missing data (mixed models) and the sample size was comparable to previous prospective studies (Table 5). A third limitation may be that we measured body composition before dialysis. This was done to allow assessment of predialysis overhydration, ultrafiltration rate, and target dry weight. In addition to LTM, we recorded ICW and BCM as proxies of muscle mass, as recommended by Carrero et al. when assessing body composition before dialysis [49]. These data support the LTM results and confirm that the observed changes indeed reflect loss of muscle mass. Finally, protein intake in our cohort was slightly below recommendations, but similar to previous studies [50]. In addition, we achieved this protein intake by following current guidelines for nutrition, suggesting that other approaches such as IDPN may be necessary to meet the recommendations [51].
In summary, in this prospective longitudinal study in chronic hemodialysis patients, we found a major loss in LTM. A simultaneous increase in ATM obscured changes in body weight. This observation was most pronounced in males and in patients with evidence of inflammation and was present regardless of dialysis vintage. Muscle strength at baseline was low and decreased significantly during this study. The findings of this study demonstrate the relevance of monitoring body composition in all hemodialysis patients. Coupled with the growing amount of data supporting a link between muscle mass and clinical outcomes in dialysis patients [1,2,3], our data call for studies to analyze whether exercise or nutritional interventions, such as oral nutritional supplements or IDPN, are able to maintain or increase LTM and muscle strength.
Supplementary Materials
The following are available online at https://www.mdpi.com/2072-6643/12/9/2494/s1, Table S1: Change in primary and secondary study parameters for the patients who completed the 20 week visit (n = 37).
Author Contributions
Conceptualization, W.J.V., A.M.E.d.M.-v.E. and E.J.H.; formal analysis, W.J.V., A.M.E.d.M.-v.E., R.T., D.S. and E.J.H.; investigation, W.J.V. and A.M.E.d.M.-v.E.; methodology, W.J.V., A.M.E.d.M.-v.E. and E.J.H.; supervision, D.S. and E.J.H.; writing—original draft, W.J.V., R.T., D.S. and E.J.H.; writing—review and editing, W.J.V., A.M.E.d.M.v.E., R.T., D.S. and E.J.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
We thank all patients who participated in this trial, Timmerman and the hemodialysis nurses for their help with data collection.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Martinson, M.; Ikizler, T.A.; Morrell, G.; Wei, G.; Almeida, N.; Marcus, R.L.; Filipowicz, R.; Greene, T.H.; Beddhu, S. Associations of body size and body composition with functional ability and quality of life in hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2014, 9, 1082–1090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rambod, M.; Bross, R.; Zitterkoph, J.; Benner, D.; Pithia, J.; Colman, S.; Kovesdy, C.P.; Kopple, J.D.; Kalantar-Zadeh, K. Association of Malnutrition-Inflammation Score with quality of life and mortality in hemodialysis patients: A 5-year prospective cohort study. Am. J. Kidney Dis. 2009, 53, 298–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stenvinkel, P.; Carrero, J.J.; Von Walden, F.; Ikizler, T.A.; Nader, G.A. Muscle wasting in end-stage renal disease promulgates premature death: Established, emerging and potential novel treatment strategies. Nephrol. Dial. Transplant. 2015, 31, 1070–1077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duenhas, M.R.; Draibe, S.A.; Avesani, C.M.; Sesso, R.; Cuppari, L. Influence of renal function on spontaneous dietary intake and on nutritional status of chronic renal insufficiency patients. Eur. J. Clin. Nutr. 2003, 57, 1473–1478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bossola, M.; Tazza, L.; Giungi, S.; Luciani, G. Anorexia in hemodialysis patients: An update. Kidney Int. 2006, 70, 417–422. [Google Scholar] [CrossRef] [Green Version]
- Sherman, R.A.; Cody, R.P.; Rogers, M.E.; Solanchick, J.C. Interdialytic weight gain and nutritional parameters in chronic hemodialysis patients. Am. J. kidney Dis. 1995, 25, 579–583. [Google Scholar] [CrossRef]
- Ikizler, T.A. Effects of hemodialysis on protein metabolism. J. Ren. Nutr. 2005, 15, 39–43. [Google Scholar] [CrossRef]
- Ikizler, T.A.; Pupim, L.B.; Brouillette, J.R.; Levenhagen, D.K.; Farmer, K.; Hakim, R.M.; Flakoll, P.J. Hemodialysis stimulates muscle and whole body protein loss and alters substrate oxidation. Am. J. Physiol. Endocrinol. Metab. 2002, 282, E107–E116. [Google Scholar] [CrossRef] [Green Version]
- Fouque, D.; Kalantar-Zadeh, K.; Kopple, J.; Cano, N.; Chauveau, P.; Cuppari, L.; Franch, H.; Guarnieri, G.; Ikizler, T.A.; Kaysen, G.; et al. A proposed nomenclature and diagnostic criteria for protein–energy wasting in acute and chronic kidney disease. Kidney Int. 2008, 73, 391–398. [Google Scholar] [CrossRef] [Green Version]
- Stenvinkel, P. Inflammation in end-stage renal disease—A fire that burns within. In Cardiovascular Disorders in Hemodialysis; Karger Publishers: Basel, Switzerland, 2005; Volume 149, pp. 185–199. [Google Scholar]
- Kramer, A.; Pippias, M.; Noordzij, M.; Stel, V.S.; Andrusev, A.M.; Aparicio-Madre, M.I.; Arribas Monzón, F.E.; Åsberg, A.; Barbullushi, M.; Beltrán, P.; et al. The European Renal Association—European Dialysis and Transplant Association (ERA-EDTA) Registry Annual Report 2016: A summary. Clin. Kidney J. 2019, 12, 702–720. [Google Scholar] [CrossRef] [Green Version]
- Fouque, D. European Best Practice Guidelines (EBPG) Guideline on Nutrition. Nephrol. Dial. Transplant. 2007, 22, 2162–2166. [Google Scholar]
- Wabel, P.; Chamney, P.; Moissl, U.; Jirka, T. Importance of whole-body bioimpedance spectroscopy for the management of fluid balance. Blood Purif. 2009, 27, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Mulasi, U.; Kuchnia, A.J.; Cole, A.J.; Earthman, C.P. Bioimpedance at the bedside: Current applications, limitations, and opportunities. Nutr. Clin. Pract. 2015, 30, 180–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moissl, U.; Wieskotten, S.; Chamney, P.; Wabel, P. Reference ranges for human body composition and fluid overload. J. Am. Soc. Nephrol. 2009, 20, 469A. [Google Scholar]
- Dodds, R.M.; Syddall, H.E.; Cooper, R.; Benzeval, M.; Deary, I.J.; Dennison, E.M.; Der, G.; Gale, C.R.; Inskip, H.M.; Jagger, C.; et al. Grip strength across the life course: Normative data from twelve British studies. PLoS ONE 2014, 9, e113637. [Google Scholar] [CrossRef] [Green Version]
- Urea kinetic modelling in chronic hemodialysis: Benefits, problems, and practical solutions. In Seminars in Dialysis; Jindal, K.K.; Goldstein, M.B. (Eds.) Wiley Online Library; Blackwell Publishing Ltd.: Oxford, UK, 1988. [Google Scholar]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Singer, J.D.; Willett, J.B.; Willett, J.B. Applied Longitudinal Data Analysis: Modeling Change and Event Occurrence; Oxford University Press: Oxford, UK, 2003. [Google Scholar]
- Verbeke, G. Linear mixed models for longitudinal data. In Linear Mixed Models in Practice; Springer: Berlin/Heidelberg, Germany, 1997; pp. 63–153. [Google Scholar]
- Leal, V.O.; Mafra, D.; Fouque, D.; Anjos, L.A. Use of handgrip strength in the assessment of the muscle function of chronic kidney disease patients on dialysis: A systematic review. Nephrol. Dial. Transplant. 2010, 26, 1354–1360. [Google Scholar] [CrossRef] [Green Version]
- Vogt, B.P.; Borges, M.C.C.; de Goés, C.R.; Caramori, J.C.T. Handgrip strength is an independent predictor of all-cause mortality in maintenance dialysis patients. Clin. Nutr. 2016, 35, 1429–1433. [Google Scholar] [CrossRef] [Green Version]
- Molina, P.; Vizcaíno, B.; Molina, M.D.; Beltrán, S.; González-Moya, M.; Mora, A.; Castro-Alonso, C.; Kanter, J.; Ávila, A.I.; Górriz, J.L.; et al. The effect of high-volume online haemodiafiltration on nutritional status and body composition: The ProtEin Stores prEservaTion (PESET) study. Nephrol. Dial. Transplant. 2018, 33, 1223–1235. [Google Scholar] [CrossRef]
- Marcelli, D.; Brand, K.; Ponce, P.; Milkowski, A.; Marelli, C.; Ok, E.; Godino, J.I.; Gurevich, K.; Jirka, T.; Rosenberger, J.; et al. Longitudinal Changes in Body Composition in Patients After Initiation of Hemodialysis Therapy: Results From an International Cohort. J. Ren. Nutr. 2016, 26, 72–80. [Google Scholar] [CrossRef] [Green Version]
- Keane, D.; Gardiner, C.; Lindley, E.; Lines, S.; Woodrow, G.; Wright, M. Changes in body composition in the two years after initiation of haemodialysis: A retrospective cohort study. Nutrients 2016, 8, 702. [Google Scholar] [CrossRef] [Green Version]
- Mathew, S.; Abraham, G.; Vijayan, M.; Thandavan, T.; Mathew, M.; Veerappan, I.; Revathy, L.; Alex, M.E. Body composition monitoring and nutrition in maintenance hemodialysis and CAPD patients—A multicenter longitudinal study. Ren. Fail. 2015, 37, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Di Gioia, M.C.; Di-Gioia, M.; Gallar, P.; Rodriguez, I.; Rodríguez, I.; Laso, N.; Callejas, R.; Ortega, O.; Herrero, J.C.; Herrero, J.C.; et al. Changes in body composition parameters in patients on haemodialysis and peritoneal dialysis. Nefrología 2012, 32, 108–113. [Google Scholar] [PubMed]
- Pupim, L.B.; Heimburger, O.; Qureshi, A.R.; Ikizler, T.; Stenvinkel, P. Accelerated lean body mass loss in incident chronic dialysis patients with diabetes mellitus. Kidney Int. 2005, 68, 2368–2374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johansen, K.L.; Kaysen, G.A.; Young, B.S.; Hung, A.M.; da Silva, M.; Chertow, G.M. Longitudinal study of nutritional status, body composition, and physical function in hemodialysis patients. Am. J. Clin. Nutr. 2003, 77, 842–846. [Google Scholar] [CrossRef]
- Vendrely, B.; Chauveau, P.; Barthe, N.; El Haggan, W.; Castaing, F.; De Précigout, V.; Combe, C.; Aparicio, M. Nutrition in hemodialysis patients previously on a supplemented very low protein diet. Kidney Int. 2003, 63, 1491–1498. [Google Scholar] [CrossRef] [Green Version]
- Ishimura, E.; Okuno, S.; Kim, M.; Yamamoto, T.; Izumotani, T.; Otoshi, T.; Shoji, T.; Inaba, M.; Nishizawa, Y. Increasing body fat mass in the first year of hemodialysis. J. Am. Soc. Nephrol. 2001, 12, 1921–1926. [Google Scholar]
- Carrero, J.J.; Chmielewski, M.; Axelsson, J.; Snaedal, S.; Heimburger, O.; Barany, P.; Suliman, M.E.; Lindholm, B.; Stenvinkel, P.; Qureshi, A.R. Muscle atrophy, inflammation and clinical outcome in incident and prevalent dialysis patients. Clin. Nutr. 2008, 27, 557–564. [Google Scholar] [CrossRef]
- Avesani, C.M.; Carrero, J.J.; Axelsson, J.; Qureshi, A.R.; Lindholm, B.; Stenvinkel, P. Inflammation and wasting in chronic kidney disease: Partners in crime. Kidney Int. 2006, 70, S8–S13. [Google Scholar] [CrossRef] [Green Version]
- Stenvinkel, P.; Gillespie, I.A.; Tunks, J.; Addison, J.; Kronenberg, F.; Drueke, T.B.; Marcelli, D.; Schernthaner, G.; Eckardt, K.U.; Floege, J.; et al. Inflammation Modifies the Paradoxical Association between Body Mass Index and Mortality in Hemodialysis Patients. J. Am. Soc. Nephrol. 2016, 27, 1479–1486. [Google Scholar] [CrossRef]
- Wang, Y.W.; Lin, T.Y.; Peng, C.H.; Huang, J.L.; Hung, S.C. Factors Associated with Decreased Lean Tissue Index in Patients with Chronic Kidney Disease. Nutrients 2017, 9, 434. [Google Scholar] [CrossRef]
- Kaysen, G.A.; Greene, T.; Daugirdas, J.T.; Kimmel, P.L.; Schulman, G.W.; Toto, R.D.; Levin, N.W.; Yan, G.; HEMO Study Group. Longitudinal and cross-sectional effects of C-reactive protein, equilibrated normalized protein catabolic rate, and serum bicarbonate on creatinine and albumin levels in dialysis patients. Am. J. Kidney Dis. 2003, 42, 1200–1211. [Google Scholar] [CrossRef] [PubMed]
- van de Logt, A.E.; Rijpma, S.R.; Vink, C.H.; Prudon-Rosmulder, E.; Wetzels, J.F.; van Berkel, M. Albumin assays and clinical decision-making in nephrotic syndrome patients reply. Kidney Int. 2019, 96, 249. [Google Scholar] [CrossRef] [PubMed]
- Ueno, T.; Hirayama, S.; Ito, M.; Nishioka, E.; Fukushima, Y.; Satoh, T.; Idei, M.; Horiuchi, Y.; Shoji, H.; Ohmura, H.; et al. Albumin concentration determined by the modified bromocresol purple method is superior to that by the bromocresol green method for assessing nutritional status in malnourished patients with inflammation. Ann. Clin. Biochem. 2013, 50, 576–584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrero, J.J. Gender differences in chronic kidney disease: Underpinnings and therapeutic implications. Kidney Blood Press. Res. 2010, 33, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Stenvinkel, P.; Barany, P.; Chung, S.H.; Lindholm, B.; Heimburger, O. A comparative analysis of nutritional parameters as predictors of outcome in male and female ESRD patients. Nephrol. Dial. Transplant. 2002, 17, 1266–1274. [Google Scholar] [CrossRef]
- Haizlip, K.M.; Harrison, B.C.; Leinwand, L.A. Sex-based differences in skeletal muscle kinetics and fiber-type composition. Physiology 2015, 30, 30–39. [Google Scholar] [CrossRef]
- Anderson, L.J.; Liu, H.; Garcia, J.M. Sex Differences in Muscle Wasting. Adv. Exp. Med. Biol. 2017, 1043, 153–197. [Google Scholar]
- Rosa-Caldwell, M.E.; Greene, N.P. Muscle metabolism and atrophy: Let’s talk about sex. Biol. Sex Differ. 2019, 10, 43. [Google Scholar] [CrossRef]
- Rymarz, A.; Matyjek, A.; Gomolka, M.; Niemczyk, S. Lean Tissue Index and Body Cell Mass Can Be Predictors of Low Free Testosterone Levels in Men on Hemodialysis. J. Ren. Nutr. 2019, 29, 529–535. [Google Scholar] [CrossRef] [Green Version]
- Chertow, G.M.; Johansen, K.L.; Lew, N.; Lazarus, J.M.; Lowrie, E.G. Vintage, nutritional status, and survival in hemodialysis patients. Kidney Int. 2000, 57, 1176–1181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beddhu, S.; Bruns, F.J.; Saul, M.; Seddon, P.; Zeidel, M.L. A simple comorbidity scale predicts clinical outcomes and costs in dialysis patients. Am. J. Med. 2000, 108, 609–613. [Google Scholar] [CrossRef]
- Chae, J.W.; Song, C.S.; Kim, H.; Lee, K.B.; Seo, B.S.; Kim, D.I. Prediction of mortality in patients undergoing maintenance hemodialysis by Charlson Comorbidity Index using ICD-10 database. Nephron Clin. Pract. 2011, 117, c379–c384. [Google Scholar] [CrossRef] [PubMed]
- Gomez, A.T.; Kiberd, B.A.; Royston, J.P.; Alfaadhel, T.; Soroka, S.D.; Hemmelgarn, B.R.; Tennankore, K.K. Comorbidity burden at dialysis initiation and mortality: A cohort study. Can. J. Kidney Health Dis. 2015, 2, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrero, J.J.; Johansen, K.L.; Lindholm, B.; Stenvinkel, P.; Cuppari, L.; Avesani, C.M. Screening for muscle wasting and dysfunction in patients with chronic kidney disease. Kidney Int. 2016, 90, 53–66. [Google Scholar] [CrossRef]
- Molfino, A.; Amabile, M.I.; Ammann, T.; Lai, S.; Grosso, A.; Lionetto, L.; Spagnoli, A.; Simmaco, M.; Monti, M.; Laviano, A.; et al. Longitudinal physical activity change during hemodialysis and its association with body composition and plasma BAIBA levels. Front. Physiol. 2019, 10, 805. [Google Scholar] [CrossRef] [Green Version]
- Pupim, L.B.; Flakoll, P.J.; Brouillette, J.R.; Levenhagen, D.K.; Hakim, R.M.; Ikizler, T.A. Intradialytic parenteral nutrition improves protein and energy homeostasis in chronic hemodialysis patients. J. Clin. Investig. 2002, 110, 483–492. [Google Scholar] [CrossRef]
Figure 1.
Change in body weight, lean tissue mass (LTM), and adipose tissue mass (ATM) over time. Data are shown as the mean ± SEM. Measurements available for all 54 patients (t = 0, 4 and 8 weeks), 46 patients (t = 12 weeks), 42 patients (t = 16 weeks), and 37 patients (t = 20 weeks).
Figure 1.
Change in body weight, lean tissue mass (LTM), and adipose tissue mass (ATM) over time. Data are shown as the mean ± SEM. Measurements available for all 54 patients (t = 0, 4 and 8 weeks), 46 patients (t = 12 weeks), 42 patients (t = 16 weeks), and 37 patients (t = 20 weeks).

{kind=link}
Table 1.
Baseline characteristics of study cohort (n = 54).
| General Characteristics | Age (Years) | 66 (52, 74) |
| Males, n (%) | 38 (71) | |
| Comorbidities | Charlson Comorbidity Index | 9.0 ± 3.4 |
| Diabetes, n (%) | 20 (37) | |
| Cardiovascular disease, n (%) | 38 (71) | |
| Dialysis characteristics | Dialysis vintage (months) | 19 (7, 40) |
| spKt/V | 1.49 ± 0.24 | |
| Laboratory values | Albumin, g/L | 38 (36.6, 39.2) |
| C-reactive protein, mg/L | 11 (7.6, 14.3) | |
| Body composition | Body weight, kg | 76.7 (71.9, 81.6) |
| Body mass index for dry weight, kg/m2 | 25.6 (22.3, 28.5) | |
| Predialysis overhydration (mL) | 1278 (835, 1712) | |
| Total body water (L) | 34.5 (29.1, 40.5) | |
| Extracellular water | 16.6 (14.5, 19.3) | |
| Intracellular water | 17.5 (14.1, 21.3) | |
| Body cell mass (kg) | 18.3 (12.6, 23.7) | |
| Lean tissue mass, kg | 37.7 (34.7, 40.6) | |
| Lean tissue index < P10, n (%) | 26 (48) | |
| Adipose tissue mass, kg | 37.6 (32.6, 42.5) | |
| Fat tissue index > P90, n (%) | 14 (26) | |
| Phase angle,° | 4.35 ± 1.1 | |
| Muscle strength | Handgrip strength, kg | 23 (19.8, 25.2) |
| Handgrip strength < P10, n (%) | 33 (61) | |
| Protein intake | Normalized protein catabolic rate, g/kg | 0.9 ± 0.2 |
| Subjective Global Assessment | Severely malnourished (1–2), n (%) | 1 (2) |
| Moderately malnourished (3–5), n (%) | 40 (74) | |
| Well nourished (6–7), n (%) | 13 (24) |
Footnote: The data are shown as the mean ± SD or median [IQRs].
Table 2.
Change in primary and secondary study parameters from mixed models analysis *.
| Baseline | 20 Weeks | Difference in Time | |||
|---|---|---|---|---|---|
| % | p−Value | ||||
| Lean tissue mass, kg | 37.7 (34.7, 40.6) | 31.3 (28.2, 34.3) | −6.4 (−8.1, −4.8) | −17.1 | <0.001 |
| Body weight, kg | 76.7 (71.9, 81.6) | 76.2 (71.4, 81.1) | −0.5 (−1.0, 0.1) | −0.6 | 0.09 |
| Adipose tissue mass, kg | 37.6 (32.6, 42.5) | 42.1 (37.1, 47.07) | 4.5 (2.7, 6.2) | 11.9 | <0.001 |
| Handgrip strength, kg | 22.5 (19.8, 25.2) | 20.6 (17.8, 23.3) | −1.9 (−3.1, −0.7) | −8.6 | 0.002 |
| Pre−dialysis OH, mL | 1278 (835, 1712) | 1509 (1031, 1973) | 236 (−205, 678) | 18.5 | 0.292 |
| Total body water, L | 34.5 (29.1, 40.5) | 31.7 (28.9, 33.9) | −2.79 (−3.5, −2.0) | −8.1 | <0.001 |
| Extracellular water, L | 16.6 (14.5, 19.3) | 15.9 (14.7, 17.0) | −0.69 (−1.4, −0.5) | −4.3 | <0.001 |
| Intracellular water, L | 17.5 (14.1, 21.3) | 15.4 (13.8, 16.8) | −2.11 (−2.9, −1.4) | −12 | <0.001 |
| Body cell mass, kg | 18.3 (12.6, 23.7) | 14.0 (12.4, 17.4) | −4.30 (−5.9, −2.9) | −23.5 | <0.001 |
| Phase angle, ° | 4.35 (4.04, 4.66) | 4.21 (3.89, 4.53) | −0.14 (−0.28, −0.01) | −3.2 | 0.07 |
| Serum albumin, g/L | 38.0 (36.6, 39.2) | 37.2 (35.7, 38.4) | −0.8 (−2.0, 0.3) | −2.2 | 0.1 |
| Serum CRP, mg/L | 11 (7.6, 14.3) | 9.7 (6.0, 13.21) | −1.3 (−5.5, 2.8) | −12.3 | 0.5 |
| nPCR, g/kg | 0.9 (0.77, 1.03) | 1.0 (0.82, 1.09) | +0.1 (−0.05, 0.16) | 11.1 | 0.4 |
Footnote: * The data are shown as the median [IQRs]. Abbreviations: OH, overhydration; CRP, C-reactive protein; nPCR, normalized protein catabolic rate.
Table 3.
Lean tissue mass at baseline and after 20 weeks and the effect of covariates.
| Baseline | 20 Weeks | Difference | |||||
|---|---|---|---|---|---|---|---|
| kg | p-Value | kg | kg | % | p-Value | ||
| Age | <65 years | 41.9 | 36.1 | −5.8 | −13.7 | <0.001 | |
| ≥65 years | 33.7 | 26.8 | −6.9 | −20.5 | <0.001 | ||
| difference | 8.2 | 0.004 | 9.3 | 1.1 | 6.8 | 0.5 | |
| Sex | male | 42.3 | 34.9 | −7.4 | −17.5 | <0.001 | |
| female | 26.8 | 22.6 | −4.2 | −15.7 | <0.001 | ||
| difference | 15.5 | <0.001 | 12.3 | 3.2 | −1.8 | 0.07 | |
| LTI (percentile) | <P10 | 37.0 | 31.2 | −5.8 | −15.6 | <0.001 | |
| ≥P10 | 39.3 | 32.1 | −7.2 | −18.4 | <0.001 | ||
| difference | −2.3 | <0.001 | −0.9 | −1.4 | −2.8 | <0.001 | |
| C-reactive protein | <median | 37.1 | 31.6 | −5.5 | −14.7 | <0.001 | |
| ≥median | 40.0 | 29.7 | −10.3 | −25.6 | <0.001 | ||
| difference | 2.9 | 0.03 | −1.9 | −4.8 | −10.9 | 0.005 | |
| Serum albumin | <median | 38.9 | 31.5 | −7.4 | −18.9 | <0.001 | |
| ≥median | 37.1 | 30.9 | −6.2 | −16.8 | < 0.001 | ||
| difference | 1.8 | 0.1 | 0.6 | −1.2 | −2.1 | 0.5 | |
| Dialysis vintage | <12 months | 41.1 | 32.8 | −8.3 | −20.2 | <0.001 | |
| ≥12 months | 35.6 | 30.0 | −5.6 | −15.8 | <0.001 | ||
| difference | 5.5 | 0.07 | 2.8 | −2.7 | −4.4 | 0.1 | |
| Diabetes mellitus | no diabetes | 39.7 | 34.1 | −5.6 | −14.1 | <0.001 | |
| diabetes | 34.2 | 26.3 | −7.9 | −23.3 | <0.001 | ||
| difference | 5.5 | 0.07 | 7.8 | −2.3 | −9.2 | 0.2 | |
| Charlson Comorbidity Index | <mean | 42.6 | 36.2 | −6.4 | −15.1 | <0.001 | |
| ≥mean | 32.8 | 26.3 | −6.5 | −19.6 | <0.001 | ||
| difference | 9.8 | <0.001 | 9.9 | 0.1 | 4.5 | 0.9 | |
Table 4.
Multivariate model for relation of covariates and lean tissue mass.
| Effect 1 | Time × Effect 2 | |||
|---|---|---|---|---|
| Estimate (95% CI) | p-Value | Estimate (95% CI) | p-Value | |
| Intercept | 46.7 (43.4, 49.9) | <0.001 | −5.2 (−9.1, −1.4) | 0.007 |
| Age ≥ 65 years | −8.4 (−11.8, −4.9) | <0.001 | 0.595 (−3.2, 4.3) | 0.8 |
| Male gender | 12.4 (11.6, 13.3) | <0.001 | −5.2 (−6.6, −3.8) | 0.02 |
| LTI ≥ P10 | 2.6 (2.1, 3.1) | <0.001 | −1.6 (−2.1. −1.0) | <0.001 |
| Serum CRP ≥ median | 0.08 (0.004, 0.1) | 0.04 | −0.1 (−0.2, 0.001) | 0.03 |
| Serum albumin < median | −0.08 (−2.3, 2.1) | 0.9 | 0.1 (−3.3, 3.6) | 0.9 |
| Dialysis vintage ≥ 12 M | −2.6 (−5.8, 0.07) | 0.1 | 1.5 (−2.3, 5.2) | 0.5 |
| Diabetes mellitus | −1.9 (−5.1, 1.3) | 0.3 | −1.5 (−4.9, 1.9) | 0.4 |
| CCI ≥ mean | −0.141 (−3.7, 3.4) | 0.9 | −3.5 (−7.6, 0.6) | 0.09 |
Footnotes: 1 Effect is the effect at baseline, 2 Time × effect is for the effect on change in time. Abbreviations: CCI, Charlson Comorbidity Index; CRP, C-reactive protein; LTI, lean tissue index; M, months.
Table 5.
Overview of studies on change in body composition over time in dialysis patients *.
| 1st Auth. | Visser | Molina | Marcelli | Keane | Mathew | Di Goia | Pupim | Johansen | Vendrely | Ishimura |
|---|---|---|---|---|---|---|---|---|---|---|
| Year | 2020 | 2018 | 2016 | 2016 | 2014 | 2012 | 2005 | 2003 | 2003 | 2001 |
| Ref. | - | [23] | [24] | [25] | [26] | [27] | [28] | [29] | [30] | [31] |
| Number | 54 | 32 | 8227 | 299 | 99 | 84 | 142 | 54 | 30 | 72 |
| Design | P | P | R | R | P | P | P | P | P | R |
| Mod. | HD | HD | HD | HD | HD + PD | HD + PD | HD | HD | HD | HD |
| Vintage | Any | Any | Start | Start | Start | Any | Start | Any | Start | Start |
| Age | 66 | 60 | 61 | 63 | 55 | 57 | 53 | 51 | 58 | 62 |
| %Male | 71 | 58 | 64 | 62 | 78 | 34 | 63 | 67 | 66 | 59 |
| %DM | 37 | 18 | 32 | 42 | 39 | - | 31 | - | 10 | 50 |
| %CVD | 70 | 21 | 52 | - | - | - | 33 | - | - | - |
| F-U | 20 w | 1 y | 2 y | 2 y | 2 y | 6 m | 1 y | 1 y | 1 y | 1 y |
| Method | BIS | BIS | BIS | BIS | BIS | BIS | DEXA | DEXA | DEXA | DEXA |
| LTM ** | −6.4 | −0.5 vs. −6.8 | −1.2 | −0.9 | −1.8 | −0.2 | −3.4 vs. −1.1 | +1.1 | 0 | −0.7 |
| ATM | +4.5 | −0.1 + 9.8 | +2.6 | +0.7 | +0.6 | +0.3 | +1.6 | −0.4 | +2.4 | +1.3 |
| CRP | 11 | 3.3 | 6 | - | - | 5.2 | <10 | 20 | - | - |
| Albumin | 38 | 39 | 38 | - | 36 | 37.6 | 32.5 | 39 | 38.5 | 39 |
Footnotes: * Age in years, LTM and ATM in kg, CRP in mg/L, albumin in g/L; ** The studies by Molina et al. and Pupim et al. compared the change in LTM in patients receiving hemodiafiltration vs. hemodialysis and in hemodialysis patients with and without diabetes, respectively. Abbreviations: ATM, adipose tissue mass; BIS, bio-impedance spectroscopy; CRP, C-reactive protein; CVD, cardiovascular disease; DEXA, dual energy X-ray absorptiometry; DM, diabetes mellitus; F-U, follow up; HD, hemodialysis; LTM, lean tissue mass; Mod., modality; nPCR, normalized protein catabolic rate; P, prospective; PD, peritoneal dialysis; R, retrospective; Ref., reference.
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Visser, W.J.; de Mik-van Egmond, A.M.E.; Timman, R.; Severs, D.; Hoorn, E.J. Risk Factors for Muscle Loss in Hemodialysis Patients with High Comorbidity. Nutrients 2020, 12, 2494. https://doi.org/10.3390/nu12092494
AMA Style
Visser WJ, de Mik-van Egmond AME, Timman R, Severs D, Hoorn EJ. Risk Factors for Muscle Loss in Hemodialysis Patients with High Comorbidity. Nutrients. 2020; 12(9):2494. https://doi.org/10.3390/nu12092494
Chicago/Turabian StyleVisser, Wesley J., Anneke M.E. de Mik-van Egmond, Reinier Timman, David Severs, and Ewout J. Hoorn. 2020. "Risk Factors for Muscle Loss in Hemodialysis Patients with High Comorbidity" Nutrients 12, no. 9: 2494. https://doi.org/10.3390/nu12092494
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.