
Satisfaction with and Continuous Usage Intention towards Mobile Health Services: Translating Users’ Feedback into Measurement

Abstract
1. Introduction
2. Literature Review
2.1. M-Health Management Apps and User Satisfaction
2.2. Kano Model-Based Approach to User Need Exploration
2.3. Kano Model and DEMATEL Method
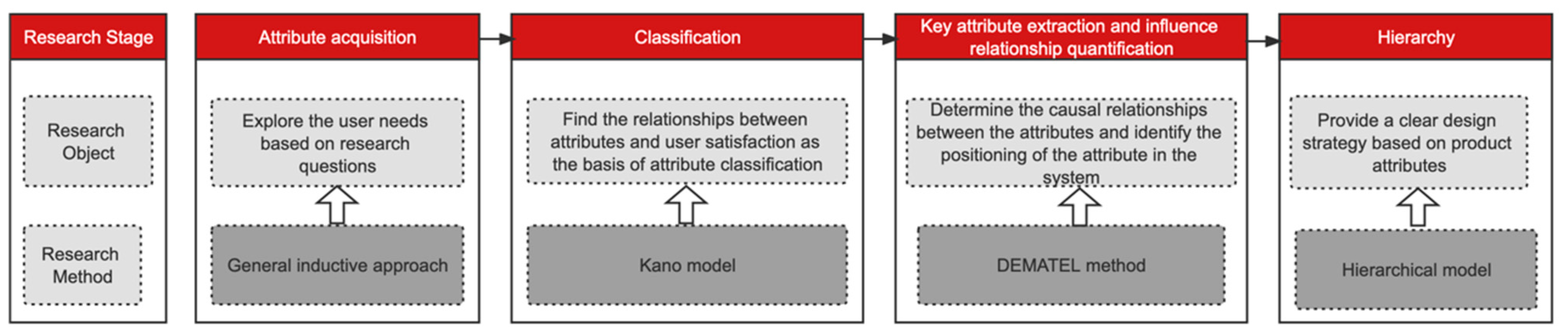
3. Methodology
3.1. Participants
3.2. Instruments
3.2.1. Acquisition of Attributes Based on the General Inductive Approach
3.2.2. Application of the Kano Model to Determine the Core Attributes and Their Relationships with User Satisfaction
3.2.3. Application of the DEMATEL Model to Clarify the Influence Relationships among the Attributes
3.2.4. Attribute Hierarchical Model for M-Health Management Apps
4. Results
4.1. Attributes for M-Health Management Apps
4.2. Core Attributes and Their Relationships with User Satisfaction
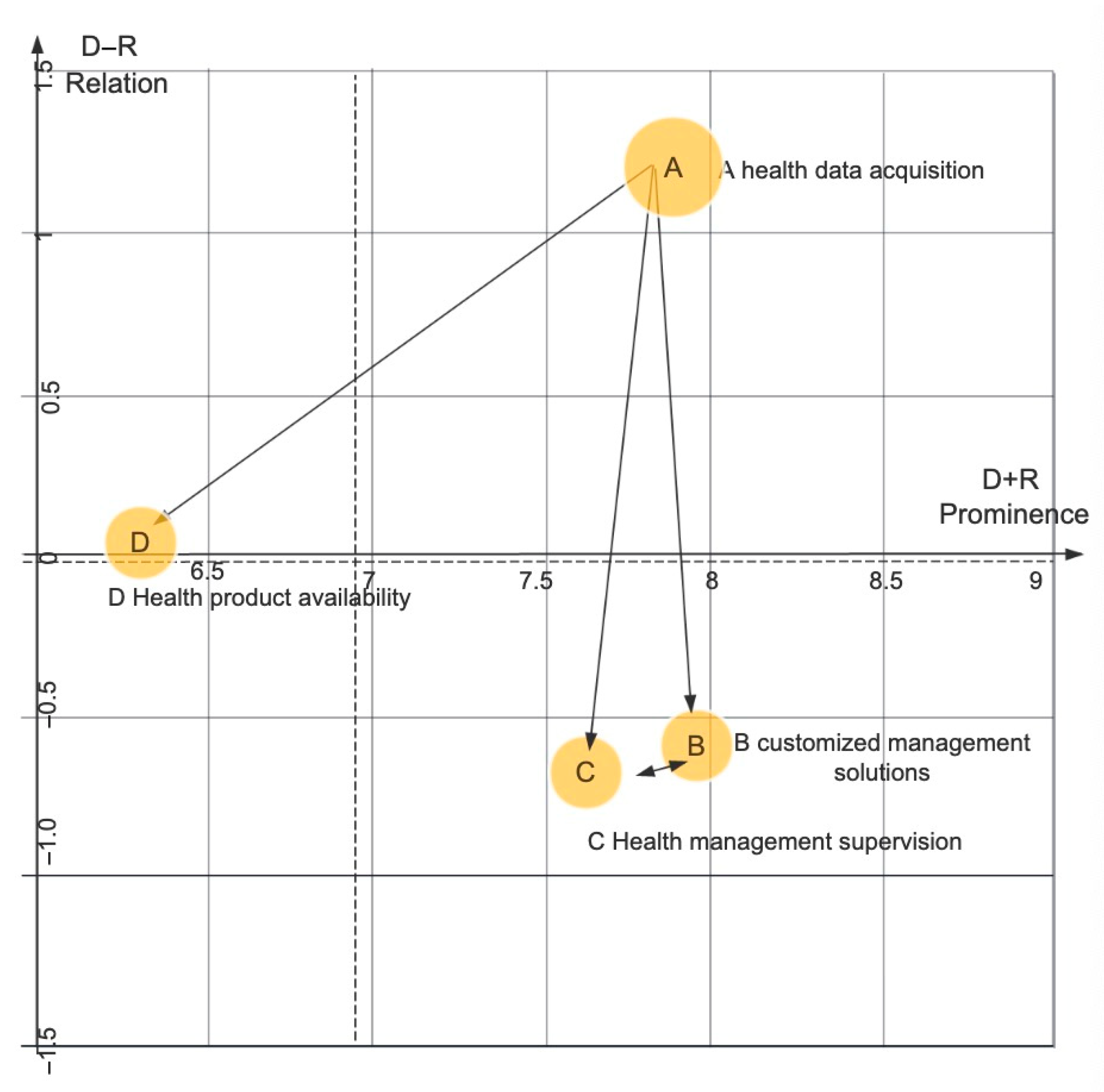
4.3. Extraction of Core Attributes and Quantification of Influence Relationships
4.4. M-Health Management App Attribute Hierarchical Model
5. Discussion
6. Conclusions
7. Limitations and Future Research Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Correction Statement
References
- Pires, I.M.; Marques, G.; Garcia, N.M.; Flórez-Revuelta, F.; Oniani, S. A Research on the Classification and Applicability of the Mobile Health Applications. J. Pers. Med. 2020, 10, 11. [Google Scholar] [CrossRef] [PubMed]
- Kongjit, C.; Nimmolrat, A.; Khamaksorn, A. Mobile health application for Thai women: Investigation and model. BMC Med. Inform. Decis. Mak. 2022, 22, 202. [Google Scholar] [CrossRef] [PubMed]
- Yin, M.; Tayyab, S.; Xu, X.Y.; Jia, S.W.; Wu, C.L. The Investigation of Mobile Health Stickiness: The Role of Social Support in a Sustainable Health Approach. Sustainability 2021, 13, 1693. [Google Scholar] [CrossRef]
- Hajesmaeel-Gohari, S.; Khordastan, F.; Fatehi, F.; Samzadeh, H.; Bahaadinbeigy, K. The most used questionnaires for evaluating satisfaction, usability, acceptance, and quality outcomes of mobile health. BMC Med. Inform. Decis. Mak. 2022, 22, 22. [Google Scholar] [CrossRef] [PubMed]
- Chiu, W.; Cho, H. The role of technology readiness in individuals’ intention to use health and fitness applications: A comparison between users and non-users. Asia Pac. J. Mark. Logist. 2020, 33, 807–825. [Google Scholar] [CrossRef]
- Miao, H.; Wang, Y.; Huang, L.; Wu, F.; Li, X. Research on User Functional Requirements Mining Based on Structured Topic Model. J. Intelli. 2020, 39, 134–141. [Google Scholar]
- Nisha, N.; Iqbal, M.; Rifat, A. The Changing Paradigm of Health and Mobile Phones: An Innovation in the Health Care System. J. Glob. Inf. Manag. 2019, 27, 19–46. [Google Scholar] [CrossRef]
- Wu, P.Z.; Zhang, R.; Zhu, X.; Liu, M. Factors Influencing Continued Usage Behavior on Mobile Health Applications. Healthcare 2022, 10, 208. [Google Scholar] [CrossRef]
- Yang, X.; Ma, L.; Zhao, X.; Kankanhalli, A. Factors influencing user’s adherence to physical activity applications: A scoping literature review and future directions. Int. J. Med. Inform. 2020, 134, 104–139. [Google Scholar] [CrossRef]
- Luo, Y.; Wang, G.; Li, Y.; Ye, Q. Examining Protection Motivation and Network Externality Perspective Regarding the Continued Intention to Use M-Health Apps. Multidiscip. Digit. Publ. Inst. 2021, 18, 5684. [Google Scholar] [CrossRef]
- Yan, M.; Filieri, R.; Raguseo, E.; Gorton, M. Mobile apps for healthy living: Factors influencing continuance intention for health apps. Technol. Forecast. Soc. Chang. 2021, 166, 120644. [Google Scholar] [CrossRef]
- Lee, C.; Lee, K.; Lee, D. Mobile Healthcare Applications and Gamification for Sustained Health Maintenance. Sustainability 2017, 9, 772. [Google Scholar] [CrossRef]
- Mzaa, B.; Mrh, C.; Wang, H.D.; Zb, E. Factors influencing the adoption of mHealth services in a developing country: A patient-centric study. Int. J. Inf. Manag. 2020, 50, 128–143. [Google Scholar]
- Hsu, J.; Liu, D.; Yu, Y.M.; Zhao, H.T.; Chen, Z.R.; Li, J.; Chen, W. The Top Chinese Mobile Health Apps: A Systematic Investigation. J. Med. Internet Res. 2016, 18, e222. [Google Scholar] [CrossRef]
- Degavre, F.; Kieffer, S.; Bol, D.; Dekimpe, R.; Desterbecq, C.; Pirson, T.; Sandu, G.; Tubeuf, S. Searching for Sustainability in Health Systems: Toward a Multidisciplinary Evaluation of Mobile Health Innovations. Sustainability 2022, 14, 5286. [Google Scholar] [CrossRef]
- Grabara, J. Sustainable Development—Never Fulfilled Dream. Access Success 2019, 20, 565–570. [Google Scholar]
- Iyengar, S. Chapter 12—Mobile health (mHealth). In Fundamentals of Telemedicine and Telehealth; Gogia, S., Ed.; Academic Press: Cambridge, MA, USA, 2020; pp. 277–294. [Google Scholar]
- Istepanian, R.S.H. Mobile Health (m-Health) in Retrospect: The Known Unknowns. Int. J. Environ. Res. Public Health 2022, 19, 3747. [Google Scholar] [CrossRef]
- Edwards, P.; Patel, V.; Haines, A. The effectiveness of mobile-health technologies to improve health care service delivery processes: A systematic review and meta-analysis. PLoS Med. 2013, 10, e1001363. [Google Scholar] [CrossRef]
- WHO. Use of Appropriate Digital Technologies for Public Health, Provisional Agenda Item 12.4 (A71/20). In Proceedings of the In Seventy-First World Health Assembly, Geneva, Switzerland, 26 May 2018. [Google Scholar]
- WHO. WHO Guideline: Recommendations on Digital Interventions for Health System Strengthening; WHO: Geneva, Switzerland, 2019; pp. 1–124. [Google Scholar]
- Hsu, C.-L.L.; Chuan, J. Effect of perceived value and social influences on mobile app stickiness and in-app purchase intention. Technol. Forecast. Soc. Chang. 2016, 108, 42–53. [Google Scholar] [CrossRef]
- Chiu, W. Consumers’ continuance intention to use fitness and health app: An integration of the expectation–confirmation model and investment model. Inf. Technol. People 2020, 34, 978–998. [Google Scholar] [CrossRef]
- Palas, J.U.; Sorwar, G.; Hoque, M.R.; Sivabalan, A. Factors influencing the elderly’s adoption of mHealth: An empirical study using extended UTAUT2 model. BMC Med. Inf. Decis. Mak. 2022, 22, 191. [Google Scholar] [CrossRef] [PubMed]
- Akter, S.; D’Ambra, J.; Ray, P.; Hani, U. Modelling the impact of mHealth service quality on satisfaction, continuance and quality of life. Behav. Inf. Technol. 2012, 32, 1225–1241. [Google Scholar] [CrossRef]
- Alperzer, M.T.A.; Argan, M. The effect of mobile service quality dimensions on customer satisfaction. Soc. Behav. Sci. 2013, 99, 428–438. [Google Scholar]
- Mensah, I.K. Understanding the Drivers of Ghanaian Citizens’ Adoption Intentions of Mobile Health Services. Front. Public Health 2022, 10, 906106. [Google Scholar] [CrossRef] [PubMed]
- Lien, C.-H.; Cao, Y.; Zhou, X. Service quality, satisfaction, stickiness, and usage intentions: An exploratory evaluation in the context of WeChat services. Comput. Hum. Behav. 2017, 68, 403–410. [Google Scholar] [CrossRef]
- Ahmad, N. Quality Attribute and Customer Satisfaction: Using Kano’s Model to Prioritize What Matters Most to Customers. J. Mark. Consum. Behav. Emerg. Mark. 2016, 1, 15–28. [Google Scholar] [CrossRef]
- Yu, H.; Si, C.; Wang, H. Research on Product Iteration and Service Innovation Based on Fuzzy KANO Model. Sci. Technol. Manag. Res. 2018, 38, 24–31. [Google Scholar]
- Yaseen, M.; Ibrahim, N.; Mustapha, A. Requirements prioritization and using iteration model for successful implementation of requirements. Int. J. Adv. Comput. Sci. Appl. 2019, 10, 121–127. [Google Scholar] [CrossRef]
- Hu, S.; Liu, J.; Wang, Y.; Guo, W.; Wang, N. Research on product iterative innovation design method based on user dynamic demand. Mod. Manuf. Eng. 2020, 000, 41–48. [Google Scholar]
- Lo, C.-H. Application of Refined Kano’s Model to Shoe Production and Consumer Satisfaction Assessment. Sustainability 2021, 13, 2484. [Google Scholar] [CrossRef]
- Li, M.; Zhang, J. Integrating Kano Model, AHP, and QFD Methods for New Product Development Based on Text Mining. Math. Probl. Eng. 2021, 2021, 2349716. [Google Scholar]
- Neira-Rodado, D.; Ortíz-Barrios, M.; De la Hoz-Escorcia, S. Smart product design process through the implementation of a fuzzy Kano-AHP-DEMATEL-QFD approach. Appl. Sci. 2020, 10, 1792. [Google Scholar] [CrossRef]
- Liu, Y.; Yang, Y.; Liu, Y.; Tzeng, G.H. Improving Sustainable Mobile Health Care Promotion: A Novel Hybrid MCDM Method. Sustainability 2019, 11, 752. [Google Scholar] [CrossRef]
- Mikulić, J.; Prebežac, D. A critical review of techniques for classifying quality attributes in the Kano model. Manag. Serv. Qual. Int. J. 2011, 21, 46–66. [Google Scholar] [CrossRef]
- Dey, U.; Kumar, A.; Ray, A.; Pradhan, B.B. Supplier Selection: Integrated Theory using DEMATEL and Quality Function Deployment Methodology. Procedia. Eng. 2012, 38, 3560–3565. [Google Scholar] [CrossRef]
- Berger, C.; Blauth, R.; Boger, D. Kano’s methods for understanding customer-defined quality. Cent. Qual. Manag. J. 1993, 2, 3–36. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Research Method | Advantages | Disadvantages |
|---|---|---|
| Kano Model | Rational allocation of resources through prioritized classification to increase user satisfaction or minimize dissatisfaction, when solving the market positioning problem of product attributes, satisfaction evaluation is used as a typical qualitative analysis model in the early stage of auxiliary research. | Product development efficiency suffers when certain design features or inter-influence relationships between requirements cannot be identified when implemented alone. |
| DEMATEL Method | Enables effective analysis of the interactions between different factors (direct and indirect), it helps to understand the complex causal relationship in decision problems. Visualizes the interrelationship of influencing factors, which are used to determine the hierarchy of functional requirements, identify key evaluation criteria, and measure the weight of the evaluation criteria. | Prioritization of requirements based only on interdependencies, with other criteria (e.g., user satisfaction) not included as a basis for decision-making. The relative weights of experts are not considered when aggregating their individual judgements into the group assessment. |
| Demographic Characteristics | Number of Respondents | Frequency | Percentage (%) |
|---|---|---|---|
| Gender | Male | 225 | 44.1 |
| Female | 285 | 55.9 | |
| Age | 18–24 Years | 128 | 25.1 |
| 25–34 Years | 173 | 33.9 | |
| 35–44 Years | 105 | 20.6 | |
| 45–54 Years | 79 | 15.5 | |
| 55 and above | 25 | 4.9 | |
| Education | High school and below | 45 | 8.8 |
| Pre-University/Certificate/Diploma | 91 | 17.8 | |
| Undergraduate (Bachelor’s Degree) | 239 | 46.9 | |
| Postgraduate (Doctorate/Master’s Degree) | 135 | 26.5 |
| Demand | Question | Dislike | Tolerable | Does Not Matter | Behoove | Like |
|---|---|---|---|---|---|---|
| Functional Attribute | Meets requirements | 1 | 2 | 3 | 4 | 5 |
| Does not meet requirements | 1 | 2 | 3 | 4 | 5 |
| Coordinate Information | Definition |
|---|---|
| Degree of influence D | Is the sum of the values of the rows of matrix T and represents the combined influence of the corresponding element of each row on all other elements |
| Degree of being influenced R | Is the sum of the values of the columns of matrix T, indicating the combined influence of the corresponding element in each column by all the other elements |
| Horizontal vector centrality (D+R) | Indicates the position of the element in the system of impact factor indicators and the magnitude of the role that it plays, i.e., the degree of importance between each element in the overall system; the influence of the factor on the system as a whole and the influence of other system elements on that factor |
| Vertical vector causality (D−R) | Indicates the degree of influence of the element on the system; a positive value of (D−R) indicates a causal factor, indicating that the factor has a strong influence on other factors; a negative value of (D−R) indicates an outcome factor, indicating that the factor is strongly influenced by other factors |
| Number | Attributes | Hi |
|---|---|---|
| 1 | Physical sign data collection | 4.56 |
| 2 | Psychological evaluation | 4.00 |
| 3 | Health risk assessment | 4.00 |
| 4 | Health tracking | 3.89 |
| 5 | Health record creation | 4.67 |
| 6 | Health management plan | 4.11 |
| 7 | Comparative feedback on health management effectiveness | 4.22 |
| 8 | Continuous usage | 4.44 |
| 9 | Matching recommendations (articles, videos, live experts, etc.) | 3.22 |
| 10 | Reminder settings | 2.89 |
| 11 | Eco-friendly lifestyle ideas | 3.44 |
| 12 | Expert consultation | 2.56 |
| 13 | Community discussions | 3.22 |
| 14 | Social sharing of health management experiences | 4.67 |
| 15 | Goal completion incentives | 4.00 |
| 16 | Simple and intuitive interface | 4.56 |
| 17 | Ease of use | 4.56 |
| 18 | Privacy and security | 4.33 |
| 19 | Reasonable functional layout | 4.44 |
| 20 | Icons or menus are easy to understand | 4.33 |
| Category | Number | Attributes |
|---|---|---|
| A. Health data acquisition | A1 | Physical sign data collection |
| A2 | Psychological evaluation | |
| A3 | Privacy and security | |
| A4 | Health risk assessment | |
| A5 | Health record creation | |
| A6 | Health tracking | |
| A7 | Health data association | |
| B. Health management scheme customization | B8 | Helps the user’s diet |
| B9 | Exercise scheme | |
| B10 | Health management plan | |
| B11 | Periodic assessment | |
| B12 | Eco-friendly lifestyle | |
| B13 | Matching recommendations (articles, videos, live experts, etc.) | |
| C. Health management supervision | C14 | Reminder settings |
| C15 | Health monitoring and management | |
| C16 | Community discussions | |
| C17 | Online consultation | |
| C18 | Social sharing of health management experiences | |
| C19 | Comparative feedback on health management effectiveness | |
| C20 | Goal completion incentives | |
| C21 | Emergency rescue instruction | |
| D. M-health management app usability | D22 | Simple and intuitive interface |
| D23 | Reasonable functional layout | |
| D24 | Continuance usage | |
| D25 | Ease of use | |
| D26 | Icons or menus are easy to understand |
| Attribute Number | Number of Answers in the Category | Bei | Woi | Assessment of the Attribute | |||||
|---|---|---|---|---|---|---|---|---|---|
| A 1 | O 2 | M 3 | I 4 | R 5 | Q 6 | ||||
| A1 | 64 | 42 | 48 | 116 | 4 | 12 | 39.26% | −33.33% | M |
| A2 | 74 | 34 | 32 | 132 | 4 | 10 | 39.71% | −24.26% | I |
| A3 | 26 | 152 | 80 | 24 | 0 | 4 | 63.12% | −82.27% | O |
| A4 | 138 | 46 | 18 | 78 | 2 | 4 | 65.71% | −22.86% | A |
| A5 | 110 | 24 | 12 | 130 | 8 | 2 | 48.55% | −13.04% | I |
| A6 | 144 | 40 | 6 | 92 | 4 | 0 | 65.25% | −16.31% | A |
| A7 | 68 | 32 | 34 | 142 | 8 | 2 | 36.23% | −23.91% | I |
| B8 | 98 | 34 | 20 | 128 | 6 | 0 | 47.14% | −19.29% | I |
| B9 | 122 | 34 | 16 | 110 | 4 | 0 | 55.32% | −17.73% | I |
| B10 | 112 | 86 | 20 | 68 | 0 | 0 | 69.23% | −37.06% | O |
| B11 | 146 | 64 | 14 | 62 | 0 | 0 | 73.43% | −27.27% | A |
| B12 | 114 | 44 | 20 | 108 | 0 | 0 | 55.24% | −22.38% | I |
| B13 | 90 | 30 | 20 | 140 | 4 | 2 | 42.86% | −17.86% | I |
| C14 | 90 | 22 | 20 | 146 | 6 | 2 | 40.29% | −15.11% | I |
| C15 | 122 | 42 | 10 | 110 | 0 | 0 | 57.75% | −18.31% | A |
| C16 | 108 | 52 | 12 | 100 | 10 | 4 | 58.82% | −23.53% | A |
| C17 | 86 | 24 | 12 | 156 | 4 | 4 | 39.57% | −12.95% | I |
| C18 | 122 | 60 | 18 | 82 | 0 | 4 | 64.54% | −27.66% | A |
| C19 | 122 | 40 | 4 | 112 | 4 | 4 | 58.27% | −15.83% | A |
| C20 | 96 | 26 | 18 | 128 | 16 | 2 | 45.52% | −16.42% | I |
| C21 | 108 | 30 | 6 | 136 | 4 | 2 | 49.29% | −12.86% | I |
| D22 | 94 | 114 | 26 | 52 | 0 | 0 | 72.73% | −48.95% | O |
| D23 | 82 | 122 | 42 | 40 | 0 | 0 | 71.33% | −57.34% | O |
| D24 | 94 | 86 | 32 | 74 | 0 | 0 | 62.94% | −41.26% | O |
| D25 | 72 | 76 | 20 | 118 | 0 | 0 | 51.75% | −33.57% | M |
| D26 | 106 | 94 | 26 | 60 | 0 | 0 | 69.93% | −41.96% | O |
| Category | D | R | D+R | D−R |
|---|---|---|---|---|
| A. health data acquisition | 4.515 | 3.31 | 7.825 | 1.206 |
| B. customized management solutions | 3.689 | 4.272 | 7.961 | −0.583 |
| C. health management supervision | 3.488 | 4.166 | 7.654 | −0.678 |
| D. health product availability | 3.179 | 3.124 | 6.304 | 0.055 |
| Attribute | D | R | D+R | D−R |
|---|---|---|---|---|
| (A1). Physical sign data collection | 4.39 | 3.57 | 7.97 | 0.82 |
| (A2). Psychological evaluation | 4.03 | 3.02 | 7.05 | 1.02 |
| (A3). Privacy and security | 4.67 | 3.59 | 8.26 | 1.08 |
| (A4). Health risk assessment | 3.85 | 3.28 | 7.13 | 0.58 |
| (A5). Health record creation | 4.11 | 3.59 | 7.70 | 0.52 |
| (A6). Health tracking | 3.93 | 3.45 | 7.38 | 0.48 |
| (A7). Health data association | 4.29 | 3.90 | 8.19 | 0.40 |
| (B8). Helps the user’s diet | 4.63 | 4.26 | 8.89 | 0.38 |
| (B9). Exercise scheme | 4.01 | 4.20 | 8.21 | −0.18 |
| (B10). Health management plan | 4.12 | 4.32 | 8.44 | −0.20 |
| (B11). Periodic assessment | 4.38 | 4.71 | 9.09 | −0.33 |
| (B12). Eco-friendly lifestyle | 3.80 | 4.16 | 7.95 | −0.36 |
| (B13). Matching recommendations (articles, videos, live experts, etc.) | 3.21 | 4.08 | 7.28 | −0.87 |
| (C14). Reminder settings | 3.09 | 3.24 | 6.33 | −0.16 |
| (C15). Health monitoring and management | 3.00 | 3.16 | 6.16 | −0.16 |
| (C16). Community discussions | 2.78 | 2.63 | 5.41 | 0.14 |
| (C17). Online consultation | 2.37 | 2.86 | 5.23 | −0.49 |
| (C18). Social sharing of health management experiences | 3.98 | 4.38 | 8.36 | −0.40 |
| (C19). Comparative feedback on health management effectiveness | 3.57 | 3.94 | 7.51 | −0.38 |
| (C20). Goal completion incentives | 2.06 | 3.24 | 5.29 | −1.18 |
| (C21). Emergency rescue instruction | 1.95 | 2.91 | 4.86 | −0.96 |
| (D22). Simple and intuitive interface | 3.51 | 3.44 | 6.95 | 0.08 |
| (D23). Reasonable functional layout | 3.45 | 3.09 | 6.54 | 0.36 |
| (D24). Continuous usage | 2.89 | 2.97 | 5.86 | −0.07 |
| (D25). Ease of use | 2.71 | 2.81 | 5.51 | −0.10 |
| (D26). Icons or menus are easy to understand | 2.48 | 2.48 | 4.96 | −0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fu, Y.; Wang, Y.; Ye, X.; Wu, W.; Wu, J. Satisfaction with and Continuous Usage Intention towards Mobile Health Services: Translating Users’ Feedback into Measurement. Sustainability 2023, 15, 1101. https://doi.org/10.3390/su15021101
Fu Y, Wang Y, Ye X, Wu W, Wu J. Satisfaction with and Continuous Usage Intention towards Mobile Health Services: Translating Users’ Feedback into Measurement. Sustainability. 2023; 15(2):1101. https://doi.org/10.3390/su15021101
Chicago/Turabian StyleFu, Yu, Yuanyuan Wang, Xinhui Ye, Weifang Wu, and Jianfeng Wu. 2023. "Satisfaction with and Continuous Usage Intention towards Mobile Health Services: Translating Users’ Feedback into Measurement" Sustainability 15, no. 2: 1101. https://doi.org/10.3390/su15021101
APA StyleFu, Y., Wang, Y., Ye, X., Wu, W., & Wu, J. (2023). Satisfaction with and Continuous Usage Intention towards Mobile Health Services: Translating Users’ Feedback into Measurement. Sustainability, 15(2), 1101. https://doi.org/10.3390/su15021101