
Does Internet Use Aggravate Public Distrust of Doctors? Evidence from China


Abstract
:1. Introduction
2. Literature Review
2.1. Research on Patient Trust
2.2. Internet Use and Patient Trust
3. Materials and Methods
3.1. Source of Data
3.2. Variable Measurement
3.3. Analytic Strategy
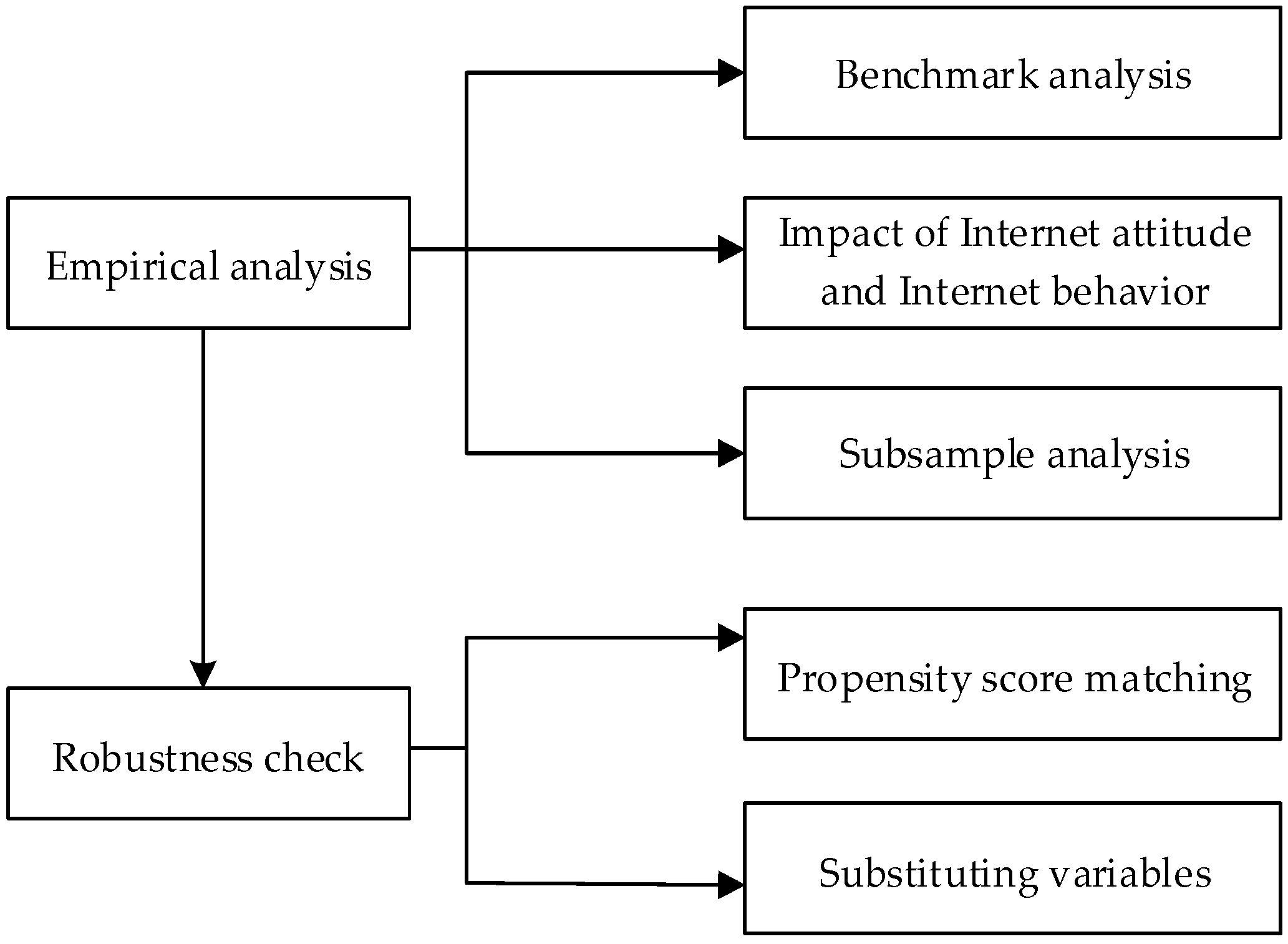
4. Results and Discussion
4.1. Descriptive Results
4.2. Benchmark Equation Results
4.3. Estimating the Impact of Internet Use on Patient Trust and Its Average Treatment Effect (ATT)
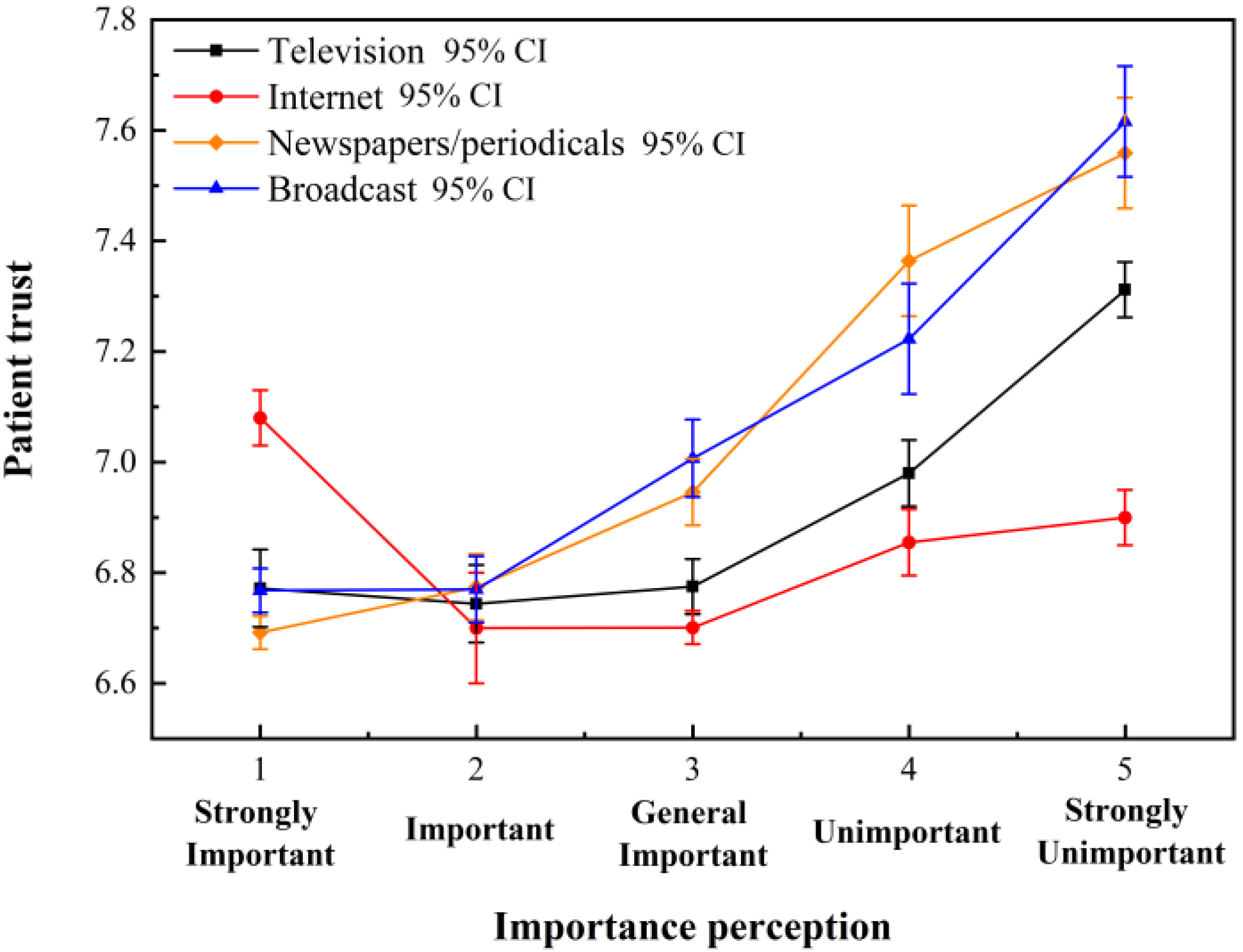
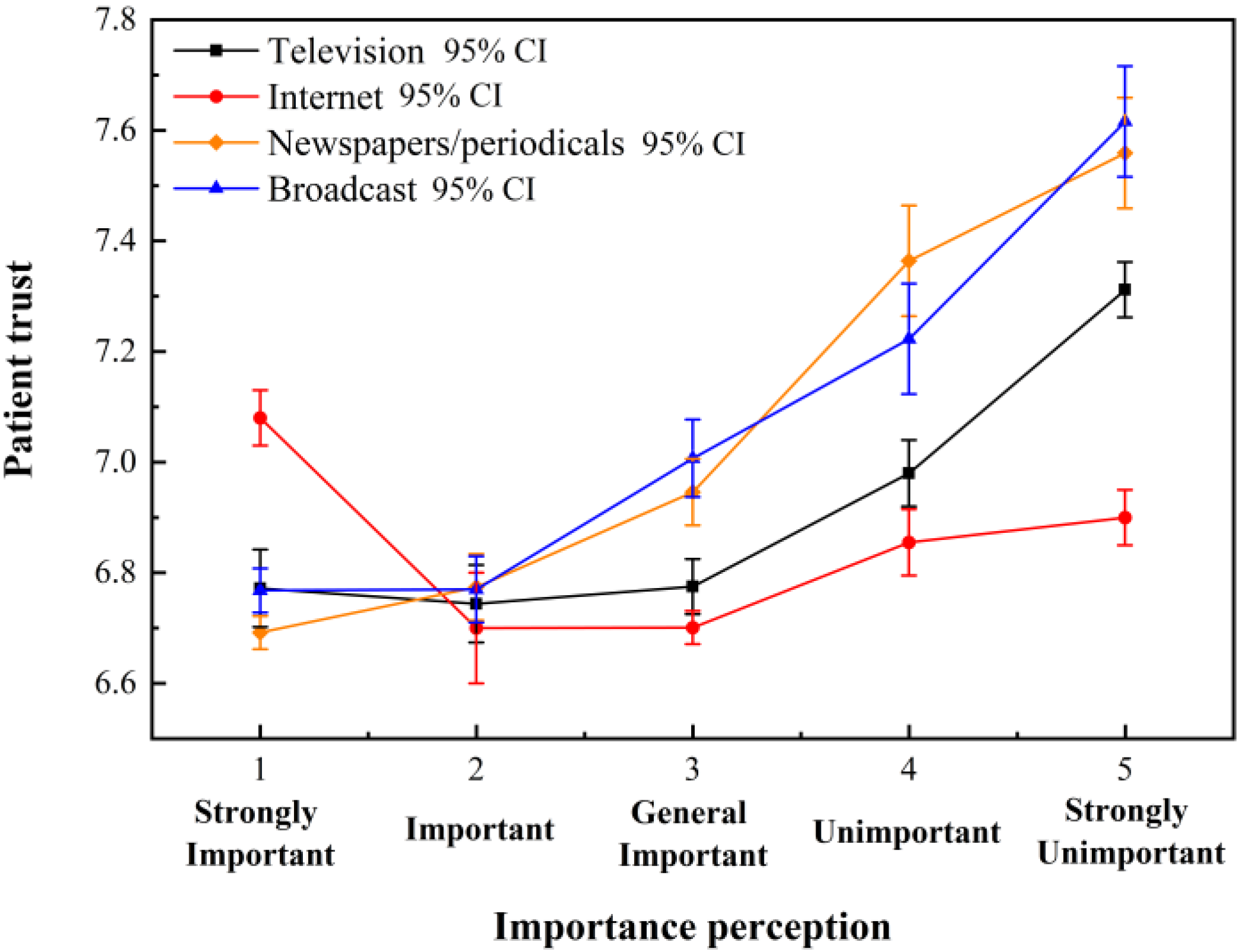
4.4. Relationship between Information Channel Importance Attitude, Internet Behavior and Patient Trust
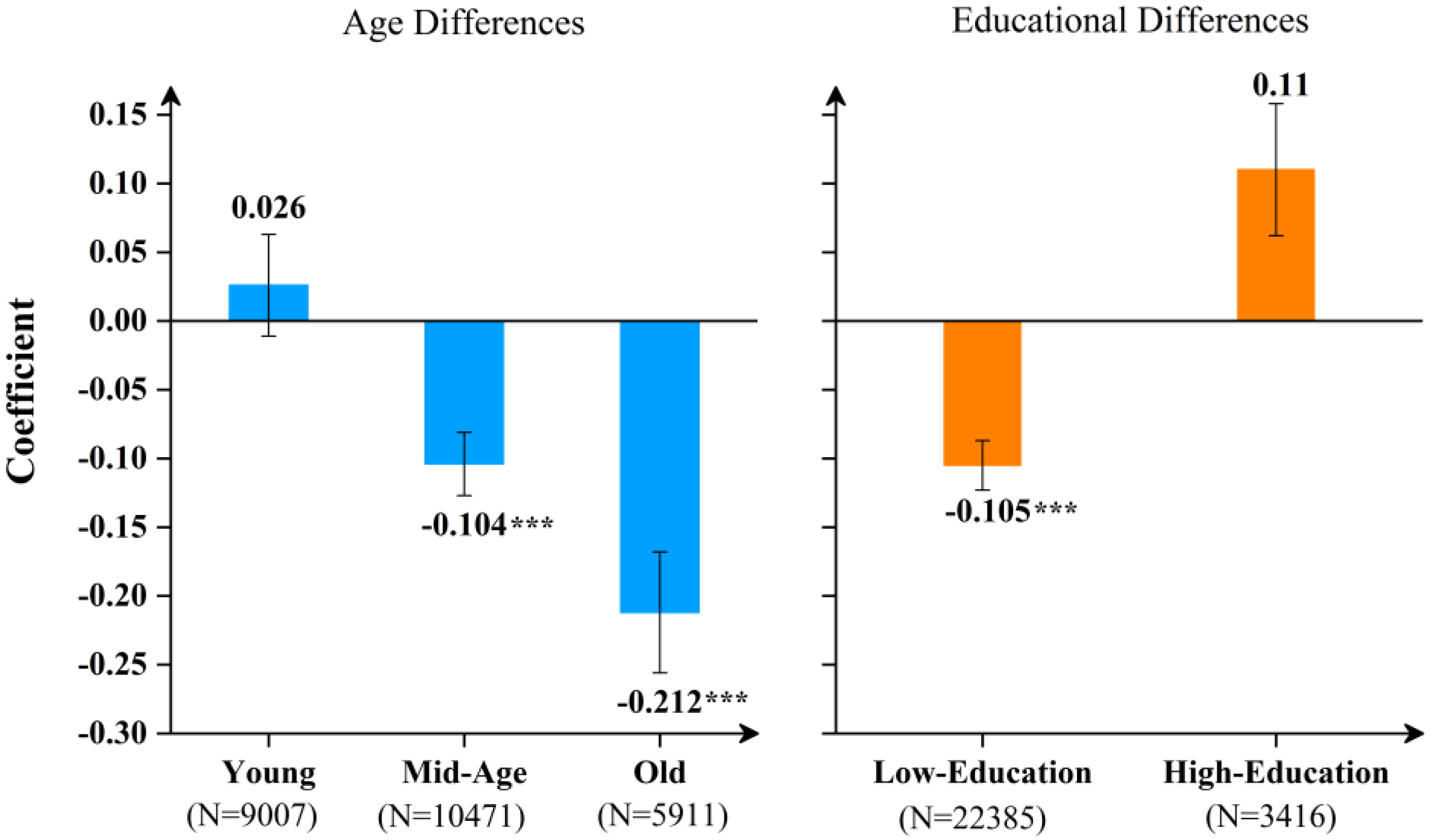
4.5. Subsample Results
4.6. Robustness Check
5. Conclusions and Policy Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Related Report Link. Available online: https://www.dxy.cn/bbs/newweb/pc/post/43581181 (accessed on 12 October 2021).
- Bo, S.; Chen, J.; Song, Y.; Zhou, S. Media attention and choice of major: Evidence from anti-doctor violence in China. J. Econ. Behav. Org. 2020, 170, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Nie, J.B.; Tucker, J.D.; Zhu, W.; Cheng, Y.; Wong, B.; Kleinman, A.M. Rebuilding patient-physician trust in China, developing a trust-oriented bioethics. Dev. World Bioethics 2017, 18, 4–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Platonova, E.A.; Kennedy, K.N.; Shewchuk, R.M. Understanding patient satisfaction, trust, and loyalty to primary care physicians. Med. Care Res. Rev. 2008, 65, 696–712. [Google Scholar] [CrossRef]
- Lu, T.; Xu, Y.; Wallace, S. Internet usage and patient’s trust in physician during diagnoses: A knowledge power perspective. J. Assoc. Inf. Sci. Technol. 2018, 69, 110–120. [Google Scholar] [CrossRef]
- Calabro, K.; Mackey, T.A.; Williams, S. Evaluation of training designed to prevent and manage patient violence. Issues Ment. Health Nurs. 2002, 23, 3–15. [Google Scholar] [CrossRef]
- Enosh, G.; Freund, A.; Goldblatt, H.; Drach-Zahavy, A.; Guindy, M.; Ofer-Bialer, G. Whose fault is it? Attribution of causes of patient violence among exposed and unexposed community-based family physicians. Health Soc. Care Community 2021, 29, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Blendon, R.J.; Benson, J.M.; Hero, J.O. Public trust in physicians—US medicine in international perspective. N. Engl. J. Med. 2014, 371, 1570–1572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, P.L.; Jiang, S. Patient-centered communication mediates the relationship between health information acquisition and patient trust in physicians: A five-year comparison in China. Health Commun. 2021, 36, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Hillen, M.A.; De Haes, H.C.J.M.; Smets, E.M. Cancer patients’ trust in their physician—A review. Psych. Oncol. 2011, 20, 227–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, H.; Tong, P.; Zhu, R. Does Internet use affect netizens’ trust in government? Empirical evidence from China. Soc. Indic. Res. 2020, 149, 167–185. [Google Scholar] [CrossRef]
- Yang, Q.; Tai-Seale, M.; Liu, S.; Shen, Y.; Zhang, X.; Xiao, X.; Zhang, K. Measuring public reaction to violence against doctors in China: Interrupted time series analysis of media reports. J. Med. Internet Res. 2021, 23, e19651. [Google Scholar] [CrossRef] [PubMed]
- Daraz, L.; Morrow, A.S.; Ponce, O.J.; Beuschel, B.; Farah, M.H.; Katabi, A.; Alsawas, M.; Majzoub, A.M.; Benkhadra, R.; Seisa, M.O.; et al. Can patients trust online health information? A meta-narrative systematic review addressing the quality of health information on the internet. J. Gen. Intern. Med. 2019, 34, 1884–1891. [Google Scholar] [CrossRef] [PubMed]
- Wallsten, S. Regulation and internet use in developing countries. Econ. Dev. Cult. Chang. 2005, 53, 501–523. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Cheng, M.; Wei, X.; Yu, N.N. The Internet-driven sexual revolution in China. Technol. Forecast. Soc. Chang. 2020, 153, 119911. [Google Scholar] [CrossRef]
- Zhu, X.; Hu, R.; Zhang, C.; Shi, G. Does Internet use improve technical efficiency? Evidence from apple production in China. Technol. Forecast. Soc. Chang. 2021, 166, 120662. [Google Scholar] [CrossRef]
- Liu, P.; Han, C.; Teng, M. The influence of Internet use on pro-environmental behaviors: An integrated theoretical framework. Resour. Conserv. Recyc. 2021, 164, 105162. [Google Scholar] [CrossRef]
- Im, T.; Cho, W.; Porumbescu, G.; Park, J. Internet, trust in government, and citizen compliance. J. Public Adm. Res. Theory 2014, 24, 741–763. [Google Scholar] [CrossRef]
- Valkenburg, P.M.; Peter, J. Internet communication and its relation to well-being: Identifying some underlying mechanisms. Media Psych. 2007, 9, 43–58. [Google Scholar] [CrossRef]
- Gollan, J.K.; Connolly, M.; Buchanan, A.; Hoxha, D.; Rosebrock, L.; Cacioppo, J.; Csernansky, J.; Wang, X. Neural substrates of negativity bias in women with and without major depression. Biol. Psychol. 2015, 109, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Zhao, D.; Zhang, Z. Changes in public trust in physicians: Empirical evidence from China. Front. Med. 2019, 13, 504–510. [Google Scholar] [CrossRef]
- Jackson, D.N.; Peterson, E.B.; Blake, K.D.; Coa, K.; Chou, W.Y.S. Americans’ trust in health information sources: Trends and sociodemographic predictors. Am. J. Health Prom. 2019, 33, 1187–1193. [Google Scholar] [CrossRef] [PubMed]
- Thom, D.H.; Campbell, B. Patient-physician trust: An exploratory study. J. Fam. Pract. 1997, 44, 169–176. [Google Scholar]
- Gabay, G. Perceived control over health, communication and patient–physician trust. Patient Educ. Couns. 2015, 98, 1550–1557. [Google Scholar] [CrossRef]
- Lu, L.Y.; Sheikholeslami, N.; Alokozai, A.; Eppler, S.L.; Kamal, R.N. The role of patient research in patient trust in their physician. J. Hand Surg. 2019, 44, 617.e1–617.e9. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Yin, P.; Deng, Z.; Wang, R. Patient–Physician Interaction and Trust in Online Health Community: The role of perceived usefulness of health information and services. Int. J. Environ. Res. Public Health 2020, 17, 139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dibben, M.R.; Lean, M.E.J. Achieving compliance in chronic illness management: Illustrations of trust relationships between physicians and nutrition clinic patients. Health Risk Soc. 2003, 5, 241–258. [Google Scholar] [CrossRef]
- Du, L.; Xu, J.; Chen, X.; Zhu, X.; Zhang, Y.; Wu, R.; Ji, H.; Zhou, L. Rebuild doctor–patient trust in medical service delivery in China. Sci. Rep. 2020, 10, 21956. [Google Scholar] [CrossRef] [PubMed]
- Gajewski, J.F.; Li, L. Can Internet-based disclosure reduce information asymmetry? Adv. Acc. 2015, 31, 115–124. [Google Scholar] [CrossRef]
- Kwan, G.; Shaw, J.A.; Murnane, L. Internet usage within healthcare: How college students use the Internet to obtain health information. J. Consum. Health Internet 2019, 23, 366–377. [Google Scholar] [CrossRef]
- Li, G.; Han, C.; Liu, P. Does Internet Use Affect Medical Decisions among Older Adults in China? Evidence from CHARLS. Healthcare 2021, 10, 60. [Google Scholar] [CrossRef]
- Chang, S.J.; Yang, E.; Lee, K.E.; Ryu, H. Internet health information education for older adults: A pilot study. Geriatr. Nurs. 2021, 42, 533–539. [Google Scholar] [CrossRef] [PubMed]
- Baucas, M.J.; Spachos, P.; Gregori, S. Internet-of-Things devices and assistive technologies for health care: Applications, challenges, and opportunities. IEEE Signal Proc. Mag. 2021, 38, 65–77. [Google Scholar] [CrossRef]
- Stevenson, F.A.; Leydon-Hudson, G.; Murray, E.; Seguin, M.; Barnes, R. Patients’ use of the internet to negotiate about treatment. Soc. Sci. Med. 2021, 290, 114262. [Google Scholar] [CrossRef]
- Nguyen, D.; Arnold, M.; Chenhall, R. The internet as non-biomedical milieu: Production of alternative health techno-social spaces and the persistence of marginalised medical practices. Health Place 2021, 70, 102583. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Zhang, R.; Lu, X.; Zhu, X. Impact of personal trust tendency on patient compliance based on internet health information seeking. Telemed. e-Health 2020, 26, 294–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soroka, S.; McAdams, S. News, politics, and negativity. Political Comm. 2015, 32, 1. [Google Scholar] [CrossRef]
- Tan, L.; Yuan, S.; Cheng, P.; Ning, P.; Gao, Y.; Xiao, W.; Schwebel, D.C.; Hu, G. Media reports about violence against medical care providers in China. Int. J. Environ. Res. Public Health 2021, 18, 2922. [Google Scholar] [CrossRef]
- Serçekuş, P.; Değirmenciler, B.; Özkan, S. Internet use by pregnant women seeking childbirth information. J. Gynecol. Obstet. Hum. Reprod. 2021, 50, 102144. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Li, W.; Zhang, T. Internet and private insurance participation. Int. J. Financ. Econ. 2022, 27, 1495–1509. [Google Scholar] [CrossRef]
- Brown, R.J.; Skelly, N.; Chew-Graham, C.A. Online health research and health anxiety: A systematic review and conceptual integration. Clin. Psychol. Sci. Pract. 2020, 27, e12299. [Google Scholar] [CrossRef]
- Xie, Y.; Hu, J. An introduction to the China family panel studies (CFPS). Chin. Sociol. Rev. 2014, 47, 3–29. [Google Scholar]
- Kim, H.; Choi, Y. Political discussion, political news, and internet use: Factors of media trust in South Korea. Commun. Res. Rep. 2017, 34, 211–220. [Google Scholar] [CrossRef]
- Siaw, A.; Jiang, Y.; Twumasi, M.A.; Agbenyo, W. The Impact of Internet Use on Income: The Case of Rural Ghana. Sustainability 2020, 12, 3255. [Google Scholar] [CrossRef] [Green Version]
- Lu, X.; Zhang, R.; Wu, W.; Shang, X.; Liu, M. Relationship between internet health information and patient compliance based on trust: Empirical study. J. Med. Internet Res. 2018, 20, e253. [Google Scholar] [CrossRef] [PubMed]
- Mojo, D.; Fischer, C.; Degefa, T. The determinants and economic impacts of membership in coffee farmer cooperatives: Recent evidence from rural Ethiopia. J. Rural. Stud. 2017, 50, 84–94. [Google Scholar] [CrossRef]
- Lokshin, M.; Sajaia, Z. Maximum likelihood estimation of endogenous switching regression models. Stata J. 2004, 4, 282–289. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.; Chen, X.; Zheng, Q.; Zhang, Y.; Ming, Z.; Wang, D.; Wu, H.; Ye, H.; Zhou, X.; Xu, Y.; et al. Serious workplace violence against healthcare providers in China between 2004 and 2018. Front. Public Health 2021, 8, 963. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Kandilov, I.T. Does Mobile Internet Use Affect the Subjective Well-being of Older Chinese Adults? An Instrumental Variable Quantile Analysis. J. Happiness Stud. 2021, 22, 3137–3156. [Google Scholar] [CrossRef]
- Banerjee, A.; Sanyal, D. Dynamics of doctor–patient relationship: A cross-sectional study on concordance, trust, and patient enablement. J. Fam. Comm. Med. 2012, 19, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lange, L.; Peikert, M.L.; Bleich, C.; Schulz, H. The extent to which cancer patients trust in cancer-related online information: A systematic review. PeerJ 2019, 7, e7634. [Google Scholar] [CrossRef] [PubMed]
- Zheng, S.; Hui, S.F.; Yang, Z. Hospital trust or doctor trust? A fuzzy analysis of trust in the health care setting. J. Bus. Res. 2017, 78, 217–225. [Google Scholar] [CrossRef]
- Wurm, S.; Tomasik, M.J.; Tesch-Römer, C. Serious health events and their impact on changes in subjective health and life satisfaction: The role of age and a positive view on ageing. Eur. J. Ageing 2008, 5, 117–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouffard, S.; Giglio, D.; Zheng, Z. Social Media and Romantic Relationship: Excessive Social Media Use Leads to Relationship Conflicts, Negative Outcomes, and Addiction via Mediated Pathways. Soc. Sci. Comput. Rev. 2021, 6. [Google Scholar] [CrossRef]
- Thom, R.P.; Bickham, D.S.; Rich, M. Internet use, depression, and anxiety in a healthy adolescent population: Prospective cohort study. JMIR Ment. Health 2018, 5, e8471. [Google Scholar] [CrossRef] [PubMed]
- Seifert, A.; Schelling, H.R. Seniors online: Attitudes toward the internet and coping with everyday life. J. Appl. Geront. 2018, 37, 99–109. [Google Scholar] [CrossRef] [PubMed]
- Zendehdel, M.; Paim, L.H.; Osman, S.B. Students’ online purchasing behavior in Malaysia: Understanding online shopping attitude. Cogent Bus. Manag. 2015, 2, 1078428. [Google Scholar] [CrossRef]
- Zhang, H.; Zhou, S.; Shen, B. Public trust: A comprehensive investigation on perceived media credibility in China. Asian J. Comm. 2014, 24, 158–172. [Google Scholar] [CrossRef]
- Wang, H.; Cai, T.; Mou, Y.; Shi, F. Traditional resources, Internet resources, and youth online political participation: The resource theory revisited in the Chinese context. Chin. Sociol. Rev. 2018, 50, 115–136. [Google Scholar] [CrossRef]
- Su, Z.; Su, S.; Zhou, Q. Government Trust in a Time of Crisis. China Rev. 2021, 21, 87–116. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Description | Mean | Std. Dev. | 95%CI |
|---|---|---|---|---|
| Dependent Variable | ||||
| Patient Trust | Patient trust in physicians | 6.782 | 2.207 | [6.755, 6.809] |
| Explanatory Variables | ||||
| Internet Use | Internet use status (1 = internet users, 0 otherwise) | 0.535 | 0.499 | [0.529, 0.541] |
| Urban | Urban respondent (1 = yes, 0 otherwise) | 0.508 | 0.500 | [0.502, 0.514] |
| Gender | Sex of respondent (1 = male, 0 otherwise) | 0.490 | 0.500 | [0.483, 0.496] |
| Age | Age of respondent (years) | 46.859 | 15.127 | [46.67, 47.04] |
| Education | Education level of respondent (1 = uneducated, 2 = primary education, 3 = secondary education, 4 = tertiary education) | 2.496 | 0.979 | [2.482, 2.508] |
| Marital Status | Marital status of respondent (1 = married, 0 otherwise) | 0.837 | 0.370 | [0.832, 0.841] |
| Income | Natural logarithm of annual personal income | 11.042 | 0.987 | [11.03, 11.05] |
| Insurance | Medical insurance status (1 = yes, 0 otherwise) | 0.924 | 0.266 | [0.920, 0.926] |
| Trust Intention | Whether respondent prefers to trust others (1 = yes, 0 otherwise) | 0.556 | 0.497 | [0.550, 0.562] |
| Life Satisfaction | Satisfaction with current life (1–5) | 3.996 | 0.950 | [3.984, 4.007] |
| Health condition | Self-rated health (1 = excellent, 2 = very good, 3 = good, 4 = fair, 5 = poor) | 2.952 | 1.221 | [2.943, 3.002] |
| Mobile Ownership | Mobile ownership status (1 = mobile owner, 0 otherwise) | 0.936 | 0.245 | [0.933, 0.939] |
| Variables | Internet Users N = 13,962 | Non-Internet Users N = 12,151 | Mean Difference | ||
|---|---|---|---|---|---|
| Mean | Std. Dev. | Mean | Std. Dev. | ||
| Dependent Variable | |||||
| Patient Trust | 6.653 | 2.102 | 6.931 | 2.313 | 0.278 *** |
| Explanatory Variables | |||||
| Urban | 0.600 | 0.490 | 0.401 | 0.490 | −0.199 *** |
| Gender | 0.512 | 0.500 | 0.466 | 0.499 | −0.046 *** |
| Age | 38.368 | 12.359 | 56.615 | 11.764 | 18.247 *** |
| Education | 2.987 | 0.778 | 1.933 | 0.879 | −1.054 *** |
| Marital Status | 0.798 | 0.402 | 0.881 | 0.324 | 0.084 *** |
| Income | 11.334 | 0.840 | 10.707 | 1.035 | −0.627 *** |
| Insurance | 0.918 | 0.274 | 0.930 | 0.255 | 0.012 *** |
| Trust Intention | 0.595 | 0.491 | 0.512 | 0.500 | −0.083 *** |
| Life Satisfaction | 3.899 | 0.903 | 4.107 | 0.989 | 0.208 *** |
| Health Condition | 2.713 | 1.086 | 3.227 | 1.307 | 0.513 *** |
| Mobile Ownership | 0.998 | 0.039 | 0.864 | 0.342 | −0.134 *** |
| Variables | OLS | Ordered Probit | ||||||
|---|---|---|---|---|---|---|---|---|
| (1) | (2) | (3) | 95% CI | (4) | (5) | (6) | 95% CI | |
| Internet use | −0.278 *** | −0.245 *** | −0.219 *** | [−0.292, −0.145] | −0.149 *** | −0.121 *** | −0.109 *** | [−0.144, −0.074] |
| (0.028) | (0.037) | (0.036) | (0.013) | (0.018) | (−0.018) | |||
| Urban | −0.290 *** | −0.275 *** | [−0.333, −0.215] | −0.142 *** | −0.133 *** | [−0.161, −0.104] | ||
| (0.029) | (0.030) | (0.014) | (0.014) | |||||
| Gender | −0.231 *** | −0.239 *** | [−0.291, −0.185] | −0.109 *** | −0.114 *** | [−0.139, −0.088] | ||
| (0.027) | (0.027) | (0.013) | (0.013) | |||||
| Age | −0.005 *** | −0.003 *** | [−0.005, 0.001] | −0.002 *** | −0.001 ** | [−0.002, −0.001] | ||
| (0.001) | (0.001) | (0.001) | (0.001) | |||||
| Education | −0.007 | 0.002 | [−0.034, 0.038] | −0.013 | −0.009 | [−0.026, 0.008] | ||
| (0.018) | (0.018) | (0.009) | (0.009) | |||||
| Marital status | −0.206 *** | −0.216 *** | [−0.290, −0.142] | −0.096 *** | −0.102 *** | [−0.137, −0.066] | ||
| (0.038) | (0.038) | (0.018) | (0.018) | |||||
| Income | −0.029 * | −0.035 ** | [−0.067, −0.003] | −0.019 ** | −0.020 *** | [−0.036, −0.004] | ||
| (0.016) | (0.016) | (0.008) | (0.008) | |||||
| Insurance | 0.216 *** | 0.177 *** | [0.070, 0.282] | 0.094 *** | 0.077 *** | [0.025, 0.127] | ||
| (0.054) | (0.051) | (0.026) | (0.025) | |||||
| Trust intention | 0.535 *** | 0.521 *** | [0.467, 0.575] | 0.248 *** | 0.243 *** | [0.216, 0.268] | ||
| (0.028) | (0.027) | (0.013) | (0.013) | |||||
| Life satisfaction | 0.388 *** | 0.384 *** | [0.353, 0.415] | 0.191 *** | 0.190 *** | [0.174, 0.204] | ||
| (0.016) | (0.014) | (0.008) | (0.007) | |||||
| Health condition | −0.056 *** | −0.055 *** | [−0.057, −0.026] | −0.133 *** | −0.027 *** | [−0.113, −0.002] | ||
| (0.011) | (0.011) | (0.016) | (0.005) | |||||
| Province | YES | YES | ||||||
| Constant | 6.931 *** | 5.861 *** | 5.972 *** | |||||
| (0.021) | (0.189) | (0.248) | ||||||
| R2 | 0.004 | 0.067 | 0.104 | 0.003# | 0.066# | 0.118# | ||
| N | 26113 | 26113 | 26113 | 26113 | 26113 | 26113 | ||
| Variables | First Stage | Patient Trust | |
|---|---|---|---|
| Internet Usage | Users | Non Users | |
| Urban | 0.240 *** | −0.216 *** | −0.283 *** |
| (10.815) | (−5.400) | (−5.840) | |
| Gender | 0.040 * | −0.266 *** | −0.158 *** |
| (1.930) | (−7.566) | (−3.679) | |
| Age | −0.056 *** | −0.018 *** | −0.002 |
| (−63.973) | (−7.353) | (−0.390) | |
| Education | 0.450 *** | 0.095 *** | 0.017 |
| (33.926) | (3.220) | (0.399) | |
| Marital status | −0.058 * | −0.116 ** | −0.191 *** |
| (−1.746) | (−2.383) | (−2.891) | |
| Income | 0.253 *** | −0.029 | 0.011 |
| (19.791) | (−1.163) | (0.432) | |
| Insurance | 0.177 *** | 0.248 *** | 0.147 * |
| (4.416) | (3.806) | (1.795) | |
| Trust intention | 0.052 ** | 0.573 *** | 0.455 *** |
| (2.547) | (15.902) | (10.886) | |
| Life satisfaction | −0.038 *** | 0.365 *** | 0.386 *** |
| (−3.541) | (18.582) | (18.227) | |
| Health condition | 0.093 ** | 0.671 *** | 0.556 *** |
| (2.547) | (15.902) | (10.886) | |
| Constant | −2.828 *** | 5.924 *** | 5.656 *** |
| (−9.393) | (14.392) | (7.915) | |
| Province | YES | YES | YES |
| Mobile Ownership | 1.733 *** | ||
| (14.661) | |||
| ρ1 | 0.128 *** | ||
| (0.035) | |||
| ρ2 | 0.134 | ||
| (0.682) | |||
| Patient Trust | ATT | T-Value | Change (%) | |
|---|---|---|---|---|
| Users | Non-Users | |||
| 6.655 | 7.154 | −0.499 | −74.947 ** | 6.98% |
| (0.545) | (0.561) | (0.355) | ||
| Variables | OLS | ||
|---|---|---|---|
| (1) | (2) | (3) | |
| Importance of the internet as information channel | −0.017 ** | ||
| (0.007) | |||
| Importance of television as information channel | 0.121 *** | ||
| (0.011) | |||
| Importance of newspapers/magazines as information channel | 0.028 ** | ||
| (0.013) | |||
| Importance of radio as information channel | 0.077 *** | ||
| (0.012) | |||
| Time spent on the internet during spare time | −0.077 *** | ||
| (0.012) | |||
| Entertainment time spent on the internet | 0.003 | ||
| (0.005) | |||
| Individual characteristics | YES | YES | YES |
| Province | YES | YES | YES |
| N | 25783 | 13702 | 13773 |
| Matching Method | Nearest Neighbor Matching | Radius Matching | Kernel Matching |
|---|---|---|---|
| Average Effect of Treatment Group | −0.199 ** | −0.14 ** | −0.15 ** |
| (0.085) | (0.065) | (0.064) | |
| T-Stat | −2.33 | −2.14 | −2.34 |
| Individual Characteristic | YES | YES | YES |
| Sample Number of Treatment Group | 13341 | 13341 | 13341 |
| Sample Number of Control Group | 10365 | 10365 | 10365 |
| Variables | First Stage | Medical Problem Perception | |
|---|---|---|---|
| Internet Use | Users | Non Users | |
| Urban | 0.238 *** | 0.102 ** | 0.003 |
| (10.729) | (2.319) | (0.063) | |
| Gender | 0.034 * | −0.011 | −0.052 |
| (1.664) | (−0.299) | (−1.107) | |
| Age | −0.056 *** | −0.002 | 0.002 |
| (−63.905) | (−0.780) | (0.436) | |
| Education | 0.452 *** | 0.247 *** | −0.062 |
| (34.090) | (7.378) | (−1.625) | |
| Marital Status | −0.056 * | 0.190 *** | −0.137 * |
| (−1.680) | (3.567) | (−1.906) | |
| Income | 0.253 *** | 0.054 ** | −0.029 |
| (19.869) | (1.977) | (−1.122) | |
| Insurance | 0.178 *** | 0.000 | −0.078 |
| (4.454) | (0.005) | (−0.869) | |
| Trust Intention | 0.051 ** | −0.164 *** | −0.169 *** |
| (2.508) | (−4.155) | (−3.676) | |
| Life Satisfaction | −0.038 *** | −0.067 *** | 0.037 |
| (−3.603) | (−3.113) | (1.578) | |
| Health Condition | 0.089 ** | −0.262 *** | −0.249 *** |
| (2.508) | (−4.155) | (−3.676) | |
| Constant | −2.802 *** | 5.848 *** | 5.705 *** |
| (−9.313) | (12.892) | (7.311) | |
| Province | YES | YES | YES |
| Mobile Ownership | 1.707 *** | ||
| (14.610) | |||
| ρ1 | −0.01 | ||
| 0.04 | |||
| ρ2 | −0.238 *** | ||
| 0.05 | |||
| Medical Problem Perception | ATT | T-Value | Change (%) | |
|---|---|---|---|---|
| Users | Non-Users | |||
| 7.287 | 5.879 | 1.418 | 285.736 | 23.95% |
| (0.003) | (0.003) | (0.358) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meng, L.; Yu, X.; Han, C.; Liu, P. Does Internet Use Aggravate Public Distrust of Doctors? Evidence from China. Sustainability 2022, 14, 3959. https://doi.org/10.3390/su14073959
Meng L, Yu X, Han C, Liu P. Does Internet Use Aggravate Public Distrust of Doctors? Evidence from China. Sustainability. 2022; 14(7):3959. https://doi.org/10.3390/su14073959
Chicago/Turabian StyleMeng, Lingpeng, Xiang Yu, Chuanfeng Han, and Pihui Liu. 2022. "Does Internet Use Aggravate Public Distrust of Doctors? Evidence from China" Sustainability 14, no. 7: 3959. https://doi.org/10.3390/su14073959
APA StyleMeng, L., Yu, X., Han, C., & Liu, P. (2022). Does Internet Use Aggravate Public Distrust of Doctors? Evidence from China. Sustainability, 14(7), 3959. https://doi.org/10.3390/su14073959