
Compulsive Study Behaviors Are Associated with Eating Disorders and Have Independent Negative Effects on Well-Being: A Structural Equation Model Study among Young Musicians


Abstract
:1. Introduction
Hypotheses
2. Materials and Methods
2.1. Sample
2.2. Instruments
2.3. Procedure
2.4. Statistical Analyses
2.5. Ethics Statement
3. Results
3.1. Descriptive Statistics and Correlation Analysis
3.2. Prevalence
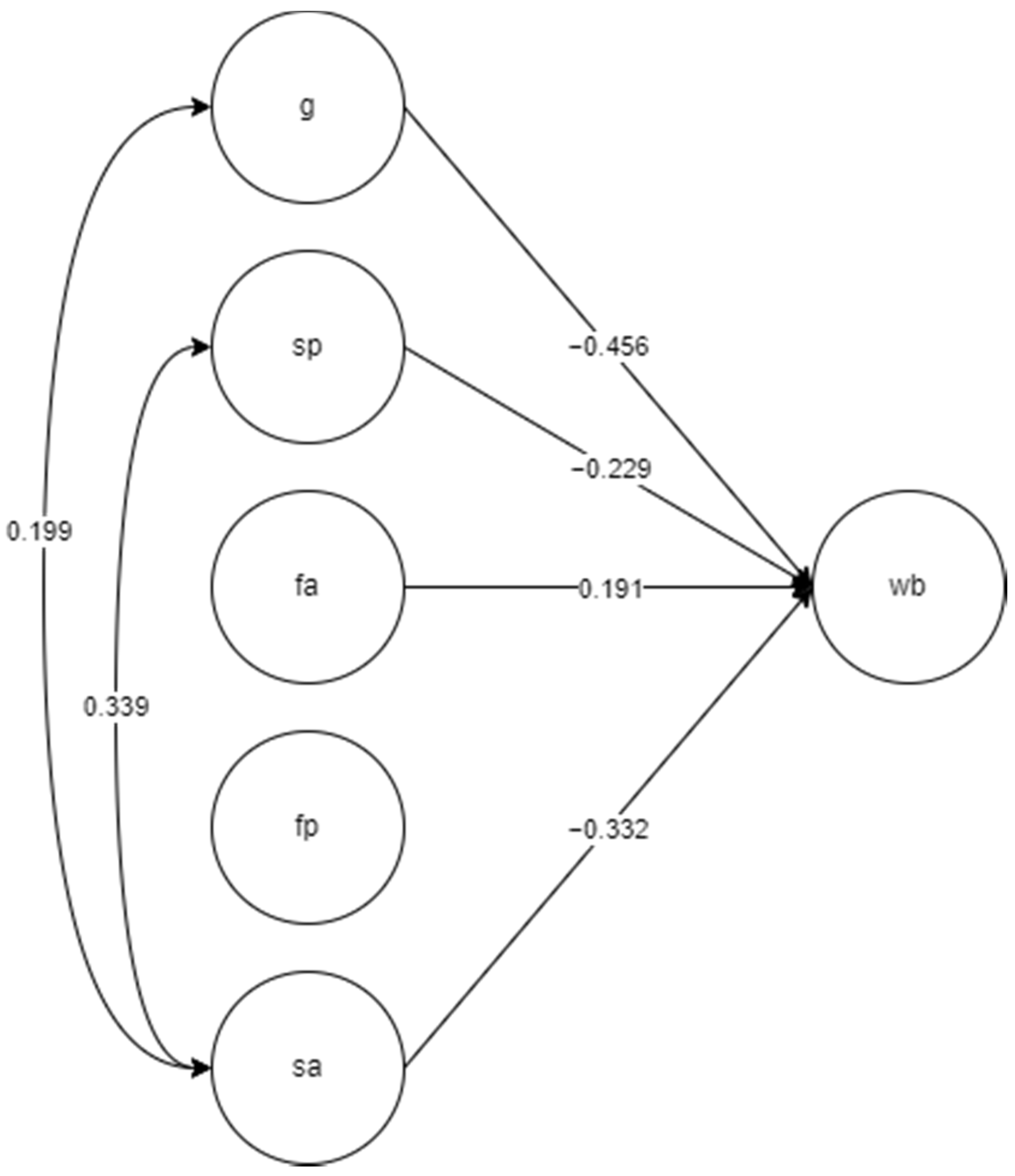
3.3. The SEM Model
4. Discussion
4.1. Strengths and Limitations
4.2. Conclusions and Future Research Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Klinger, D.A.; Freeman, J.G.; Bilz, L.; Liiv, K.; Ramelow, D.; Sebok, S.S. Cross-National Trends in Perceived School Pressure by Gender and Age from 1994 to 2010. Eur. J. Public Health 2015, 25, 51–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Loon, A.W.G.; Cremers, H.E.; Beumer, W.Y.; Okorn, A.; Vogelaar, S.; Saab, N.; Miers, A.C.; Westenberg, P.M.; Asscher, J.J. Can Schools Reduce Adolescent Psychological Stress? A Multilevel Meta-Analysis of the Effectiveness of School-Based Intervention Programs. J. Youth Adolesc. 2020, 49, 1127–1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosales-Ricardo, Y.; Rizzo-Chunga, F.; Mocha-Bonilla, J.; Ferreira, J.P. Prevalence of burnout syndrome in university students: A systematic review. Salud Ment. 2021, 44, 91–102. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Leiter, M.P.; Maslach, C. Burnout: 35 Years of Research and Practice. Career Dev. Int. 2009, 14, 204–220. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Burn-Out an “Occupational Phenomenon”. In International Classification of Diseases; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Imo, U.O. Burnout and Psychiatric Morbidity among Doctors in the UK: A Systematic Literature Review of Prevalence and Associated Factors. BJPsych Bull. 2017, 41, 197–204. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Mental Health in the Workplace; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Walburg, V. Burnout among High School Students: A Literature Review. Child. Youth Serv. Rev. 2014, 42, 28–33. [Google Scholar] [CrossRef]
- Atroszko, P.A. Non-Drug Addiction: Addiction to Work. In Handbook of Substance Misuse and Addictions; Patel, V.B., Preedy, V.R., Eds.; Springer: Cham, Switzerland, 2022. [Google Scholar]
- Atroszko, P.A.; Demetrovics, Z.; Griffiths, M.D. Work Addiction, Obsessive-Compulsive Personality Disorder, Burn-Out, and Global Burden of Disease: Implications from the ICD-11. Int. J. Environ. Res. Public Health 2020, 17, 660. [Google Scholar] [CrossRef] [Green Version]
- Samnaliev, M.; Noh, H.L.; Sonneville, K.R.; Austin, S.B. The Economic Burden of Eating Disorders and Related Mental Health Comorbidities: An Exploratory Analysis Using the US Medical Expenditures Panel Survey. Prev. Med. Rep. 2015, 2, 32–34. [Google Scholar] [CrossRef] [Green Version]
- Hudson, J.I.; Hiripi, E.; Pope, H.G.; Kessler, R.C. The Prevalence and Correlates of Eating Disorders in the National Comorbidity Survey Replication. Biol. Psychiatry 2007, 61, 348–358. [Google Scholar] [CrossRef] [Green Version]
- Atroszko, P.A.; Mytlewska, W.M.; Atroszko, B. The Majority of Professionally Active Women Diagnosed with Eating Disorders May Be at Risk of Work Addiction: An Overlooked Comorbidity. Health Psychol. Rep. 2021, 9, 308–337. [Google Scholar] [CrossRef]
- Atroszko, P.A. The Structure of Study Addiction: Selected Risk Factors and the Relationship with Stress, Stress Coping and Psychosocial Functioning. Ph.D. Thesis, University of Gdansk, Gdansk, Poland, 2015. [Google Scholar]
- Atroszko, P.A.; Andreassen, C.S.; Griffiths, M.D.; Pallesen, S. Study Addiction—A New Area of Psychological Study: Conceptualization, Assessment, and Preliminary Empirical Findings. J. Behav. Addict. 2015, 4, 75–84. [Google Scholar] [CrossRef] [Green Version]
- Atroszko, P.A.; Andreassen, C.S.; Griffiths, M.D.; Pallesen, S. The Relationship between Study Addiction and Work Addiction: A Cross-Cultural Longitudinal Study. J. Behav. Addict. 2016, 5, 708–714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013; ISBN 978-0-89042-555-8. [Google Scholar]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems, 11th Revision; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Atroszko, P.A. Research on Behavioural Addictions: Work Addiction. In Modern Research Trends of Young Scientists: Current Status, Problems and Prospects; Baranowska-Szczepańska, M., Gołaszewski, M., Eds.; Wydawnictwo Naukowe Wyższej Szkoły Handlu i Usług: Poznań, Poland, 2012; pp. 11–24. [Google Scholar]
- Andreassen, C.S. Workaholism: An Overview and Current Status of the Research. J. Behav. Addict. 2014, 3, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oates, W.E. On being a “Workaholic”. Pastor. Psychol. 1968, 19, 16–20. [Google Scholar] [CrossRef]
- Sussman, S. Workaholism: A Review. J. Addict. Res. Ther. 2012, 6, 4120. [Google Scholar] [CrossRef]
- Atroszko, P.A.; Demetrovics, Z.; Griffiths, M.D. Beyond the Myths about Work Addiction: Toward a Consensus on Definition and Trajectories for Future Studies on Problematic Overworking. J. Behav. Addict. 2019, 8, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Lawendowski, R.; Bereznowski, P.; Wróbel, W.K.; Kierzkowski, M.; Atroszko, P.A. Study Addiction among Musicians: Measurement, and Relationship with Personality, Social Anxiety, Performance, and Psychosocial Functioning. Musicae Sci. 2020, 24, 449–474. [Google Scholar] [CrossRef]
- Atroszko, P.A.; Atroszko, B.; Charzyńska, E. Subpopulations of Addictive Behaviors in Different Sample Types and Their Relationships with Gender, Personality, and Well-Being: Latent Profile vs. Latent Class Analysis. Int. J. Environ. Res. Public Health 2021, 18, 8590. [Google Scholar] [CrossRef]
- Charzyńska, E.; Sussman, S.; Atroszko, P.A. Profiles of Potential Behavioral Addictions’ Severity and Their Associations with Gender, Personality, and Well-Being: A Person-Centered Approach. Addict. Behav. 2021, 119, 106941. [Google Scholar] [CrossRef]
- Wróbel, W. Study Addiction among High School Students: Measurement and Relationship with Psychopathology, Personality, Quality of Life, and School Variables. Master’s Thesis, University of Gdańsk, Gdańsk, Poland, 2020. [Google Scholar]
- Christo, G.; Jones, S.L.; Haylett, S.; Stephenson, G.M.; Lefever, R.M.; Lefever, R. The Shorter PROMIS Questionnaire: Further Validation of a Tool for Simultaneous Assessment of Multiple Addictive Behaviours. Addict. Behav. 2003, 28, 225–248. [Google Scholar] [CrossRef]
- Haylett, S.A.; Stephenson, G.M.; Lefever, R.M. Covariation in addictive behaviours: A study of addictive orientations using the Shorter PRO-MIS Questionnaire. Addict. Behav. 2004, 29, 61–71. [Google Scholar] [CrossRef]
- MacLaren, V.V.; Best, L.A. Multiple addictive behaviors in young adults: Student norms for the Shorter PROMIS Questionnaire. Addict. Behav. 2010, 35, 252–255. [Google Scholar] [CrossRef] [PubMed]
- Polivy, J.; Herman, C.P. Causes of Eating Disorders. Annu. Rev. Psychol. 2002, 53, 187–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blinder, B.J.; Cumella, E.J.; Sanathara, V.A. Psychiatric Comorbidities of Female Inpatients with Eating Disorders. Psychosom. Med. 2006, 68, 454–462. [Google Scholar] [CrossRef]
- Lilenfeld, L.R.; Wonderlich, S.; Riso, L.P.; Crosby, R.; Mitchell, J. Eating Disorders and Personality: A Methodological and Empirical Review. Clin. Psychol. Rev. 2006, 26, 299–320. [Google Scholar] [CrossRef]
- Lutz, A.P.; Dierolf, A.; Van Dyck, Z.; Georgii, C.; Schnepper, R.; Blechert, J.; Vögele, C. Mood-Induced Changes in the Cortical Processing of Food Images in Bulimia Nervosa. Addict. Behav. 2021, 113, 106712. [Google Scholar] [CrossRef]
- Touchette, E.; Henegar, A.; Godart, N.T.; Pryor, L.; Falissard, B.; Tremblay, R.E.; Côté, S.M. Subclinical Eating Disorders and Their Comorbidity with Mood and Anxiety Disorders in Adolescent Girls. Psychiatry Res. 2011, 185, 185–192. [Google Scholar] [CrossRef]
- Monteleone, A.M.; Cascino, G.; Marciello, F.; Abbate-Daga, G.; Baiano, M.; Balestrieri, M.; Barone, E.; Bertelli, S.; Carpiniello, B.; Castellini, G.; et al. Risk and Resilience Factors for Specific and General Psychopathology Worsening in People with Eating Disorders during COVID-19 Pandemic: A Retrospective Italian Multicentre Study. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2021, 26, 2443–2452. [Google Scholar] [CrossRef]
- Kapsetaki, M.E.; Easmon, C. Eating Disorders in Non-Dance Performing Artists: A Systematic Literature Review. Med. Probl. Perform. Artist. 2017, 32, 227–234. [Google Scholar] [CrossRef]
- Kapsetaki, M.E.; Easmon, C. Eating Disorders in Musicians: A Survey Investigating Self-Reported Eating Disorders of Musicians. Eat. Weight. Disord.-Stud. Anorex. Bulim. Obes. 2019, 24, 541–549. [Google Scholar] [CrossRef] [Green Version]
- Ringham, R.; Klump, K.; Kaye, W.; Stone, D.; Libman, S.; Stowe, S.; Marcus, M. Eating Disorder Symptomatology among Ballet Dancers. Int. J. Eat. Disord. 2006, 39, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Kreutz, G.; Ginsborg, J.; Williamon, A. Music Students’ Health Problems and Health-Promoting Behaviours. Med. Probl. Perform. Artist. 2008, 23, 3–11. [Google Scholar] [CrossRef]
- Garner, D.M.; Olmsted, M.P.; Bohr, Y.; Garfinkel, P.E. The Eating Attitudes Test: Psychometric Features and Clinical Correlates. Psychol. Med. 1982, 12, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Laporta-Herrero, I.; Jáuregui-Lobera, I.; Serrano-Troncoso, E.; Garcia-Argibay, M.; Cortijo-Alcarria, M.C.; Santed-Germán, M.-A. Attachment, Body Appreciation, and Body Image Quality of Life in Adolescents with Eating Disorders. Eat. Disord. 2022, 30, 168–181. [Google Scholar] [CrossRef]
- Meule, A.; Richard, A.; Schnepper, R.; Reichenberger, J.; Georgii, C.; Naab, S.; Voderholzer, U.; Blechert, J. Emotion Regulation and Emotional Eating in Anorexia Nervosa and Bulimia Nervosa. Eat. Disord. 2021, 29, 175–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogoza, R.; Brytek-Matera, A.; Garner, D. Analysis of the EAT-26 in a Non-Clinical Sample. Arch. Psychiatry Psychother. 2016, 18, 54–58. [Google Scholar] [CrossRef]
- Uriegas, N.A.; Emerson, D.M.; Smith, A.B.; Kelly, M.R.; Torres-McGehee, T.M. Examination of Eating Disorder Risk among University Marching Band Artists. J. Eat. Disord. 2021, 9, 35. [Google Scholar] [CrossRef] [PubMed]
- Newman, C.; George, R.P.; Beitz, T.; Bergson, Z.; Zemon, V. Mental Health Issues among International Touring Professionals in the Music Industry. J. Psychiatr. Res. 2022, 145, 243–249. [Google Scholar] [CrossRef]
- Vaag, J.; Bjerkeset, O.; Sivertsen, B. Anxiety and Depression Symptom Level and Psychotherapy Use Among Music and Art Students Compared to the General Student Population. Front. Psychol. 2021, 12, 607927. [Google Scholar] [CrossRef]
- Atroszko, P.; Sawicki, A.; Kamble, S. Cross-Cultural Pilot Study on the Relationship between Study Addiction and Narcissism among Undergraduate Students in Poland and India. Health Psychol. Rep. 2019, 7, 325–333. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Czerwiński, S.K.; Mackiewicz, J.J.; Mytlewska, W.M.; Atroszko, P.A. Factorial Validity, Measurement Invariance and Concurrent Validity of Hospital Anxiety and Depression Scale in a Sample of Polish Undergraduate Students. Psychiatr. Psychol. Klin. 2020, 20, 13–18. [Google Scholar] [CrossRef]
- Mihalca, A.M.; Pilecka, W. The Factorial Structure and Validity of the Hospital Anxiety and Depression Scale (HADS) in Polish Adolescents. Psychiatr. Pol. 2015, 49, 1071–1088. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A Global Measure of Perceived Stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Czerwiński, S.K.; Atroszko, P.A. Scores of Short and Free Scale for Big Five Explain Perceived Stress at Different Stages of Life: Validity, Reliability and Measurement Invariance of the Polish Adaptation of Mini-IPIP. Curr. Issues Personal. Psychol. 2020, 8, 73–82. [Google Scholar] [CrossRef]
- Skevington, S.M.; Lotfy, M.; O’Connell, K.A. The World Health Organization’s WHOQOL-BREF Quality of Life Assessment: Psychometric Properties and Results of the International Field Trial. A Report from the WHOQOL Group. Qual. Life Res. 2004, 13, 299–310. [Google Scholar] [CrossRef]
- Atroszko, P.; Bagińska, P.; Mokosińska, M.; Sawicki, A.; Atroszko, B. Validity and Reliability of Single-Item Self-Report Measures of General Quality of Life, General Health and Sleep Quality. In Proceedings of the 4th Biannual CER Comparative European Research Conference: International Scientific Conference for Ph.D. Students of EU Countries, London, UK, 26–30 October 2015. [Google Scholar]
- Atroszko, P.; Krzyżaniak, P.; Sendal, L.; Atroszko, B. Validity and Reliability of Single-Item Self-Report Measures of Meaning in Life and Satisfaction with Life. In Proceedings of the 4th Biannual CER Comparative European Research Conference: International Scientific Conference for Ph.D. Students of EU Countries, London, UK, 26–30 October 2015. [Google Scholar]
- Atroszko, P.A.; Pianka, L.; Raczyńska, A.; Sęktas, M.; Atroszko, B. Validity and Reliability of Single-Item Self-Report Measures of Social Support. In Proceedings of the 4th Biannual CER Comparative European Research Conference: International Scientific Conference for Ph.D. Students of EU Countries, London, UK, 26–30 October 2015. [Google Scholar]
- Atroszko, P.A.; Sawicki, A.; Sendal, L.; Atroszko, B. Validity and Reliability of Single-Item Self-Report Measure of Global Self-Esteem. In Proceedings of the 7th Biannual CER Comparative European Research Conference: International Scientific Conference for Ph.D. Students of EU Countries, London, UK, 29–31 March 2017. [Google Scholar]
- Garner, D.M.; Garfinkel, P.E. The Eating Attitudes Test: An Index of the Symptoms of Anorexia Nervosa. Psychol. Med. 1979, 9, 273–279. [Google Scholar] [CrossRef]
- Vacca, M.; Ballesio, A.; Lombardo, C. The Relationship between Perfectionism and Eating-related Symptoms in Adolescents: A Systematic Review. Eur. Eat. Disord. Rev. 2021, 29, 32–51. [Google Scholar] [CrossRef]
- Giles, S.; Hughes, E.K.; Fuller-Tyszkiewicz, M.; Treasure, J.; Fernandez-Aranda, F.; Karwautz, A.F.K.; Wagner, G.; Anderluh, M.; Collier, D.A.; Krug, I. Bridging of Childhood Obsessive-compulsive Personality Disorder Traits and Adult Eating Disorder Symptoms: A Network Analysis Approach. Eur. Eat. Disord. Rev. 2022, 30, 110–123. [Google Scholar] [CrossRef]
- Drakes, D.H.; Fawcett, E.J.; Rose, J.P.; Carter-Major, J.C.; Fawcett, J.M. Comorbid Obsessive-Compulsive Disorder in Individuals with Eating Disorders: An Epidemiological Meta-Analysis. J. Psychiatr. Res. 2021, 141, 176–191. [Google Scholar] [CrossRef]
- Robinson, B.E. Chained to the Desk: A Guidebook for Workaholics, Their Partners and Children, and the Clinicians Who Treat Them; NYU Press: New York, NY, USA, 2014. [Google Scholar]
- Atroszko, P.A.; Atroszko, B. Type-A Personality Competitiveness Component Linked to Increased Cardiovascular Risk Is Positively Related to Study Addiction but Not to Study Engagement. Curr. Sci. 2019, 117, 1184. [Google Scholar] [CrossRef]
- Rorty, M.; Yager, J. Histories of childhood trauma and complex post-traumatic sequelae in women with eating disorders. Psychiatr. Clin. N. Am. 1996, 19, 773–791. [Google Scholar] [CrossRef]
- Atroszko, B. The Costs of Work-Addicted Managers in Organizations: Towards Integrating Clinical and Organizational Frameworks. Amfiteatru Econ. 2020, 22, 1265. [Google Scholar] [CrossRef]
- Leong Bin Abdullah, M.F.I.; Mansor, N.S.; Mohamad, M.A.; Teoh, S.H. Quality of Life and Associated Factors among University Students during the COVID-19 Pandemic: A Cross-Sectional Study. BMJ Open 2021, 11, e048446. [Google Scholar] [CrossRef] [PubMed]
- Woon, L.S.-C.; Sidi, H.B.; Ravindran, A.; Gosse, P.J.; Mainland, R.L.; Kaunismaa, E.S.; Hatta, N.H.; Arnawati, P.; Zulkifli, A.Y.; Mustafa, N.; et al. Depression, Anxiety, and Associated Factors in Patients with Diabetes: Evidence from the Anxiety, Depression, and Personality Traits in Diabetes Mellitus (ADAPT-DM) Study. BMC Psychiatry 2020, 20, 227. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Estimate | S.E. | Est./S.E. | Two-Tailed p-Value | AVE | CR | Omega/ Omega Subscale | Omega Hierarchical/Omega Hierarchical Subscale | ECV | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| SA | 0.49 | 0.87 | 0.87 | - | - | ||||||
| BSTAS 1 | Salience | 0.48 | 0.05 | 9.68 | <0.001 | ||||||
| BSTAS 2 | Tolerance | 0.55 | 0.05 | 11.45 | <0.001 | ||||||
| BSTAS 3 | Mood modification | 0.65 | 0.04 | 15.09 | <0.001 | ||||||
| BSTAS 4 | Relapse | 0.81 | 0.03 | 24.51 | <0.001 | ||||||
| BSTAS 5 | Withdrawal | 0.78 | 0.03 | 25.83 | <0.001 | ||||||
| BSTAS 6 | Conflict | 0.74 | 0.03 | 21.66 | <0.001 | ||||||
| BSTAS 7 | Problems | 0.82 | 0.03 | 26.99 | <0.001 | ||||||
| G | 0.21 | 0.67 | 0.90 | 0.46 | 0.35 | ||||||
| EATS 3 | Food preoccupation | 0.48 | 0.08 | 5.75 | <0.001 | ||||||
| EATS 4 | Binge-eating | 0.41 | 0.09 | 4.75 | <0.001 | ||||||
| EATS 6 | Calorie awareness | 0.55 | 0.07 | 8.33 | <0.001 | ||||||
| EATS 7 | Carbohydrates avoidance | 0.51 | 0.08 | 6.47 | <0.001 | ||||||
| EATS 8 | Social pressure to eat more | −0.05 | 0.08 | −0.98 | 0.325 | ||||||
| EATS 13 | Others’ concerns | −0.25 | 0.08 | −3.37 | 0.001 | ||||||
| EATS 16 | Sugar avoidance | 0.32 | 0.08 | 4.03 | <0.001 | ||||||
| EATS 17 | Dieting food | 0.41 | 0.08 | 5.24 | <0.001 | ||||||
| EATS 18 | Lack of control | 0.72 | 0.07 | 9.67 | <0.001 | ||||||
| EATS 20 | External pressure to eat | 0.24 | 0.08 | 3.05 | 0.002 | ||||||
| EATS 21 | Food preoccupation | 0.81 | 0.08 | 11.27 | <0.001 | ||||||
| SP | 0.67 | 0.86 | 0.88 | 0.87 | - | ||||||
| EATS 8 | Social pressure to eat more | 0.92 | 0.04 | 22.26 | <0.001 | ||||||
| EATS 13 | Others’ concerns | 0.75 | 0.05 | 15.46 | <0.001 | ||||||
| EATS 20 | External pressure to eat | 0.78 | 0.05 | 15.16 | <0.001 | ||||||
| FA | 0.36 | 0.77 | 0.83 | 0.53 | - | ||||||
| EATS 6 | Calorie awareness | 0.44 | 0.07 | 6.50 | <0.001 | ||||||
| EATS 7 | Carbohydrates avoidance | 0.62 | 0.07 | 8.76 | <0.001 | ||||||
| EATS 16 | Sugar avoidance | 0.75 | 0.06 | 12.77 | <0.001 | ||||||
| EATS 17 | Dieting foods | 0.53 | 0.07 | 8.06 | <0.001 | ||||||
| FP | 0.31 | 0.51 | 0.90 | 0.41 | - | ||||||
| EATS 3 | Food preoccupation | 0.73 | 0.09 | 8.49 | <0.001 | ||||||
| EATS 4 | Binge-eating | 0.50 | 0.09 | 5.62 | <0.001 | ||||||
| EATS 18 | Lack of control | 0.48 | 0.10 | 4.77 | <0.001 | ||||||
| EATS 21 | Food preoccupation | 0.49 | 0.11 | 4.63 | <0.001 | ||||||
| WB | 0.55 | 0.58 | 0.58 | - | - | ||||||
| Anxiety | Anxiety | −0.93 | 0.04 | −24.49 | <0.001 | ||||||
| Depression | Depression | −0.67 | 0.04 | −15.33 | <0.001 | ||||||
| Quality of life | Quality of life | 0.67 | 0.05 | 13.76 | <0.001 | ||||||
| Stress | Stress | −0.66 | 0.05 | −13.21 | <0.001 |
| General | Social Pressure | Food Awareness | Food Preoccupation | Study Addiction | Well-Being | |
|---|---|---|---|---|---|---|
| SR AVE | 0.46 | 0.82 | 0.60 | 0.56 | 0.70 | 0.74 |
| Study Addiction | 0.20 | 0.19 | −0.10 | −0.02 | - | - |
| Well-being | −0.49 | 0.00 | 0.35 | −0.11 | −0.50 | - |
| Variables | Gender | N | M (SD)/% |
|---|---|---|---|
| Age | Women | 184 | 23.09 (3.37) |
| Men | 71 | 22.94 (3.71) | |
| Study addiction | Women | 184 | 19.64 (5.67) |
| Men | 71 | 18.07 (5.85) | |
| Anxiety | Women | 184 | 11.55 (3.77) |
| Men | 71 | 9.00 (3.67) | |
| Depression | Women | 184 | 5.96 (3.36) |
| Men | 71 | 6.14 (3.20) | |
| Quality of life | Women | 184 | 36.69 (9.92) |
| Men | 71 | 38.42 (10.34) | |
| Stress | Women | 184 | 12.40 (2.83) |
| Men | 71 | 11.11 (2.97) |
| Garner et al. (1982) [41] | Rogoza et al. (2016) [44] | Study Addiction | |
|---|---|---|---|
| Am terrified about being overweight. | Dieting | - | 0.13 * |
| Avoid eating when I am hungry. | Oral Control | - | 0.25 ** |
| Find myself preoccupied with food. | Bulimia and Food Preoccupation | Food preoccupation | 0.03 |
| Have gone on eating binges where I feel that I may not be able to stop. | Bulimia and Food Preoccupation | Food preoccupation | 0.11 |
| Cut my food into small pieces. | Oral Control | - | 0.08 |
| Aware of the calorie content of foods that I eat. | Dieting | Food awareness | 0.08 |
| Particularly avoid food with a high carbohydrate content (i.e., bread, rice, potatoes, etc.). | Dieting | Food awareness | 0.06 |
| Feel that others would prefer if I ate more. | Oral Control | Social pressure | 0.19 ** |
| Vomit after I have eaten. | Bulimia and Food Preoccupation | Purging behaviors | 0.10 |
| Feel extremely guilty after eating. | Dieting | - | 0.19 ** |
| Am preoccupied with a desire to be thinner. | Dieting | - | 0.16 * |
| Think about burning up calories when I exercise. | Dieting | - | 0.17 ** |
| Other people think that I am too thin. | Oral Control | Social pressure | 0.19 ** |
| Am preoccupied with the thought of having fat on my body. | Dieting | - | 0.14 * |
| Take longer than others to eat my meals. | Oral Control | - | 0.08 |
| Avoid foods with sugar in them. | Dieting | Food awareness | 0.01 |
| Eat diet foods. | Dieting | Food awareness | 0.12 |
| Feel that food controls my life. | Bulimia and Food Preoccupation | Food preoccupation | 0.07 |
| Display self-control around food. | Oral Control | - | 0.13 * |
| Feel that others pressure me to eat. | Oral Control | Social pressure | 0.21 ** |
| Give too much time and thought to food. | Bulimia and Food Preoccupation | Food preoccupation | 0.17 ** |
| Feel uncomfortable after eating sweets. | Dieting | - | 0.14 * |
| Engage in dieting behavior. | Dieting | - | 0.09 |
| Like my stomach to be empty. | Dieting | - | 0.18 ** |
| Have the impulse to vomit after meals. | Bulimia and Food Preoccupation | Purging behaviors | 0.24 ** |
| Enjoy trying new rich foods. | Dieting | - | 0.04 |
| Study Addiction (At Least 4 Symptoms) | Study Addiction (All 7 Symptoms) | Eating Disorders (Possible Disorder) | Depression (Possible, At Least Mild Disorder) | Depression Clinical (Clinically Significant Disorder) | Anxiety (Possible, At Least Mild Disorder) | Anxiety Clinical (Clinically Significant Disorder) | |
|---|---|---|---|---|---|---|---|
| Study addictionpolythetic | 63 (24.7%) | 9 (14.3%) | 10 (15.9%) | 29 (46.0%) | 13 (20.6%) | 61 (96.8%) | 55 (87.3%) |
| Study addiction monothetic | 9 (100%) | 9 (3.5%) | 3 (33.3%) | 7 (77.8%) | 5 (55.6%) | 9 (100%) | 8 (88.9%) |
| Eating disorders | 10 (37.0%) | 3 (11.1%) | 27 (10.6%) | 15 (55.6%) | 6 (22.2%) | 27 (100%) | 25 (92.6%) |
| Depression (>= 8) | 29 (36.7%) | 7 (8.9%) | 15 (19.0%) | 79 (31.0%) | 26 (33.0%) | 75 (95.0%) | 60 (76.0%) |
| Depression (>= 11) | 13 (50.0%) | 5 (19.2%) | 6 (23.1%) | 26 (100.0%) | 26 (10.2%) | 24 (92.3%) | 21 (80.8%) |
| Anxiety (>= 8) | 61 (29.8%) | 9 (4.4%) | 27 (13.2%) | 75 (36.6%) | 24 (11.7%) | 205 (80.4%) | 130 (63.4%) |
| Anxiety (>= 11) | 55 (42.3%) | 8 (6.2%) | 25 (19.2%) | 60 (23.1%) | 21 (16.2%) | 130 (100%) | 130 (51.0%) |
| Estimate | S.E. | Est./S.E. | Two-Tailed p-Value | |||
|---|---|---|---|---|---|---|
| SA | WITH | G | 0.12 | 0.10 | 2.07 | 0.038 |
| SA | WITH | SP FA FP | 0.34 −0.03 −0.05 | 0.07 0.10 0.11 | 4.76 −0.26 −0.45 | <0.001 0.798 0.650 |
| WB | ON | G SP FA FP SA | −0.46 −0.23 0.19 −0.05 −0.33 | 0.09 0.08 0.08 0.12 0.08 | −4.83 −3.02 2.50 −0.40 −4.06 | <0.001 0.003 0.012 0.692 <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Woropay-Hordziejewicz, N.A.; Buźniak, A.; Lawendowski, R.; Atroszko, P.A. Compulsive Study Behaviors Are Associated with Eating Disorders and Have Independent Negative Effects on Well-Being: A Structural Equation Model Study among Young Musicians. Sustainability 2022, 14, 8617. https://doi.org/10.3390/su14148617
Woropay-Hordziejewicz NA, Buźniak A, Lawendowski R, Atroszko PA. Compulsive Study Behaviors Are Associated with Eating Disorders and Have Independent Negative Effects on Well-Being: A Structural Equation Model Study among Young Musicians. Sustainability. 2022; 14(14):8617. https://doi.org/10.3390/su14148617
Chicago/Turabian StyleWoropay-Hordziejewicz, Natalia A., Aleksandra Buźniak, Rafał Lawendowski, and Paweł A. Atroszko. 2022. "Compulsive Study Behaviors Are Associated with Eating Disorders and Have Independent Negative Effects on Well-Being: A Structural Equation Model Study among Young Musicians" Sustainability 14, no. 14: 8617. https://doi.org/10.3390/su14148617
APA StyleWoropay-Hordziejewicz, N. A., Buźniak, A., Lawendowski, R., & Atroszko, P. A. (2022). Compulsive Study Behaviors Are Associated with Eating Disorders and Have Independent Negative Effects on Well-Being: A Structural Equation Model Study among Young Musicians. Sustainability, 14(14), 8617. https://doi.org/10.3390/su14148617