
Contrasting the COVID-19 Effects on Tourism Safety Perceptions and Coping Behavior among Young People during Two Pandemic Waves: Evidence from Egypt



Abstract
:1. Introduction
2. Theoretical Background
2.1. Perceived Risks
2.2. Tourism Safety Perceptions
2.3. Acceptance of Restrictions
2.4. Intentions to Change Behaviour
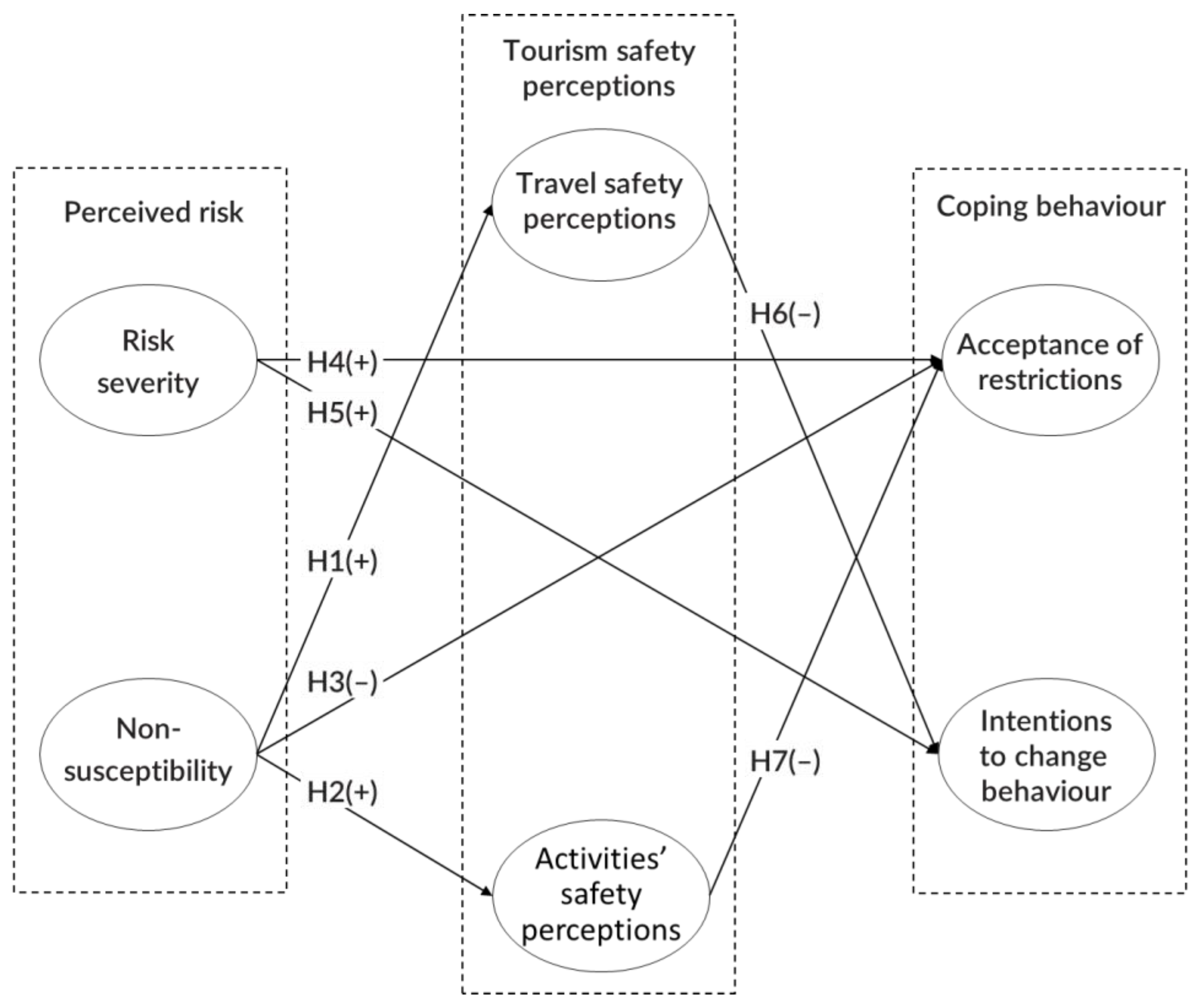
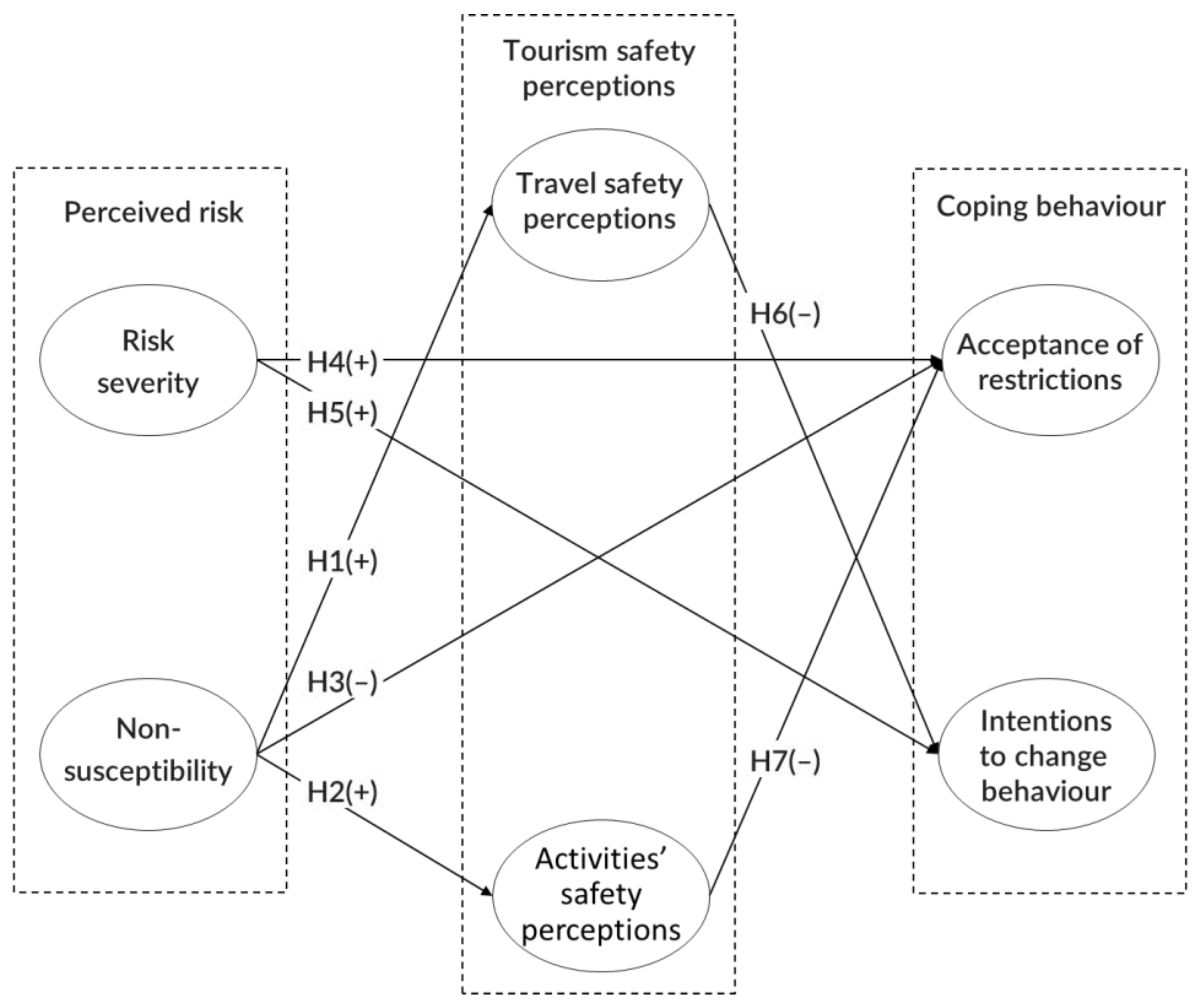
3. Conceptual Framework and Hypothesis Development
4. Study Context
5. Methods
6. Results and Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Holmes, E.C.; Goldstein, S.A.; Rasmussen, A.L.; Robertson, D.L.; Crits-Christoph, A.; Wertheim, J.O.; Anthony, S.J.; Barclay, W.S.; Boni, M.F.; Doherty, P.C.; et al. The origins of SARS-CoV-2: A critical review. Cell 2021, 184, 4848–4856. [Google Scholar] [CrossRef] [PubMed]
- Lau, H.; Khosrawipour, V.; Kocbach, P.; Mikolajczyk, A.; Schubert, J.; Bania, J.; Khosrawipour, T. The positive impact of lockdown in Wuhan on containing the COVID-19 outbreak in China. J. Travel Med. 2020, 27, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Worldometer. COVID-19 Coronavirus Pandemic. 2022. Available online: https://www.worldometers.info/coronavirus/ (accessed on 2 February 2020).
- Ahlfeldt, G.M.; Franke, B.; Maennig, W. Terrorism and international tourism: The case of Germany. Jahrbücher Für Natl. Und Stat. 2015, 235, 3–21. [Google Scholar] [CrossRef]
- Bonham, C.; Edmonds, C.; Mak, J. The impact of 9/11 and other terrible global events on tourism in the United States and Hawaii. J. Travel Res. 2006, 45, 99–110. [Google Scholar] [CrossRef]
- Bunghez, C.L. The importance of tourism to a destination’s economy. J. East. Eur. Res. Bus. Econ. 2016, 2016, 1–9. [Google Scholar] [CrossRef]
- Morrison, A.; Lynch, P.; Johns, N. International tourism networks. Int. J. Contemp. Hosp. Manag. 2004, 16, 197–202. [Google Scholar] [CrossRef]
- Du, D.; Lew, A.A.; Ng, P.T. Tourism and economic growth. J. Travel Res. 2016, 55, 454–464. [Google Scholar] [CrossRef]
- Kim, H.; Marcouiller, D.W. Considering disaster vulnerability and resiliency: The case of hurricane effects on tourism-based economies. Ann. Reg. Sci. 2015, 54, 945–971. [Google Scholar] [CrossRef]
- Saleh, A.S.; Assaf, A.G.; Ihalanayake, R.; Lung, S. A panel cointegration analysis of the impact of tourism on economic growth: Evidence from the Middle East region. Int. J. Tour. Res. 2015, 17, 209–220. [Google Scholar] [CrossRef]
- Karabag, S.F. An unprecedented global crisis! The global, regional, national, political, economic and commercial impact of the coronavirus pandemic. J. Appl. Econ. Bus. Res. 2020, 10, 1–6. [Google Scholar]
- Ranasinghe, R. After corona (COVID-19) impacts on global poverty and recovery of tourism based service economies: An appraisal. Int. J. Tour. Hosp. 2021, 1, 52–64. [Google Scholar] [CrossRef]
- Neuburger, L.; Egger, R. Travel risk perception and travel behaviour during the COVID-19 pandemic 2020: A case study of the DACH region. Curr. Issues Tour. 2021, 24, 1003–1016. [Google Scholar] [CrossRef]
- Seabra, C.; Reis, P.; Abrantes, J.L. The influence of terrorism in tourism arrivals: A longitudinal approach in a Mediterranean country. Ann. Tour. Res. 2020, 80, 102811. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Liu-Lastres, B.; Ritchie, B.W.; Mills, D.J. Travellers’ self-protections against health risks: An application of the full Protection Motivation Theory. Ann. Tour. Res. 2019, 78, 102743. [Google Scholar] [CrossRef]
- Zheng, D.; Luo, Q.; Ritchie, B.W. Afraid to travel after COVID-19? Self-protection, coping and resilience against pandemic ‘travel fear’. Tour. Manag. 2021, 83, 104261. [Google Scholar] [CrossRef]
- Gössling, S.; Scott, D.; Hall, C.M. Pandemics, tourism and global change: A rapid assessment of COVID-19. J. Sustain. Tour. 2020, 29, 1–20. [Google Scholar] [CrossRef]
- Chua, B.-L.; Al-Ansi, A.; Lee, M.J.; Han, H. Impact of health risk perception on avoidance of international travel in the wake of a pandemic. Curr. Issues Tour. 2020, 24, 985–1002. [Google Scholar] [CrossRef]
- Kaushal, V.; Srivastava, S. Hospitality and tourism industry amid COVID-19 pandemic: Perspectives on challenges and learnings from India. Int. J. Hosp. Manag. 2021, 92, 102707. [Google Scholar] [CrossRef]
- Novelli, M.; Gussing Burgess, L.; Jones, A.; Ritchie, B.W. ‘No Ebola… still doomed’—The Ebola-induced tourism crisis. Ann. Tour. Res. 2018, 70, 76–87. [Google Scholar] [CrossRef]
- Seabra, C.; AlAshry, M.; Çınar, K.; Raja, I.; Reis, M.; Sadiq, N. Acceptance of restrictions and risk perception by young generations in a COVID-19 context. Int. J. Tour. Cities 2021, 7, 463–491. [Google Scholar] [CrossRef]
- Bae, S.Y.; Chang, P.J. The effect of coronavirus disease-19 (COVID-19) risk perception on behavioural intention towards ‘untact’ tourism in South Korea during the first wave of the pandemic. Curr. Issues Tour. 2020, 24, 1017–1035. [Google Scholar] [CrossRef]
- Caber, M.; Albayrak, T.; Crawford, D. Perceived value and its impact on travel outcomes in youth tourism. J. Outdoor Recreat. Tour. 2020, 31, 100327. [Google Scholar] [CrossRef]
- Vukic, M.; Kuzmanovic, M.; Kostic Stankovic, M. Understanding the heterogeneity of Generation Y’s preferences for travelling: A conjoint analysis approach. Int. J. Tour. Res. 2015, 17, 482–491. [Google Scholar] [CrossRef]
- Richards, G. An Economic Contribution that Matters. In The Power of Youth Travel; Fitzgerald, D., Jordan, P., Egido, L., Eds.; World Tourism Organization: Madrid, Spain, 2011; Volume 2, pp. 7–8. Available online: https://genctraveller.files.wordpress.com/2013/11/thepowerofyouthtravel.pdf (accessed on 21 January 2022).
- Francis, T.; Hoefel, F. True Gen: Generation Z and Its Implications for Companies; McKinsey & Company: São Paulo, Brasil, 2018; Available online: www.mckinsey.com/industries/consumer-packaged-goods/ourinsights/true-gen-generation-z-and-its-implications-for-companies# (accessed on 21 December 2021).
- UNWTO. WYSE Travel Confederation. The Power of Youth Travel (Volume 2). UNWTO. 2011. Available online: https://www.wysetc.org/wp-content/uploads/2014/12/wysetc-unwto-report-english_the-power-of-youth.pdf (accessed on 21 January 2022).
- Felsenstein, S.; Hedrich, C.M. COVID-19 in children and young people. Lancet Rheumatol. 2020, 2, e514–e516. [Google Scholar] [CrossRef]
- Xie, C.; Zhang, J.; Morrison, A.M. Developing a Scale to Measure Tourist Perceived Safety. J. Travel Res. 2020, 60, 1232–1251. [Google Scholar] [CrossRef]
- Liu-Lastres, B.; Mirehie, M.; Cecil, A. Are female business travelers willing to travel during COVID-19? An exploratory study. J. Vacat. Mark. 2021, 27, 252–266. [Google Scholar] [CrossRef]
- Becker, M.H. The Health Belief Model and personal health behavior. Health Educ. Monogr. 1974, 2, 324–508. [Google Scholar] [CrossRef]
- Janz, N.K.; Becker, M.H. The health belief model: A decade later. Health Educ. Behav. 1984, 11, 1–47. [Google Scholar] [CrossRef] [Green Version]
- Ajzen, I. The theory of planned behaviour. Organ. Behav. Hum. Decis. Processes 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Bauer, R.A. Consumer behavior as risk taking. In Dynamic Marketing for a Changing World; Hancock, R.S., Ed.; American Marketing Association: Chicago, IL, USA, 1960; pp. 389–398. [Google Scholar]
- Dowling, G.R.; Staelin, R. A model of perceived risk and intended risk-handling activity. J. Consum. Res. 1994, 21, 119–134. [Google Scholar] [CrossRef]
- Pavlou, P.A. Consumer acceptance of electronic commerce: Integrating trust and risk with the technology acceptance model. Int. J. Electron. Commer. 2003, 7, 101–134. [Google Scholar]
- Conchar, M.P.; Zinkhan, G.M.; Peters, C.; Olavarrieta, S. An integrated framework for the conceptualization of consumers’ perceived-risk processing. J. Acad. Mark. Sci. 2004, 32, 418–436. [Google Scholar] [CrossRef]
- Huang, X.; Dai, S.; Xu, H. Predicting tourists’ health risk preventative behaviour and travelling satisfaction in Tibet: Combining the theory of planned behaviour and health belief model. Tour. Manag. Perspect. 2020, 33, 100589. [Google Scholar] [CrossRef]
- Liu-Lastres, B.; Schroeder, A.; Pennington-Gray, L. Cruise line customers’ responses to risk and crisis communication messages: An application of the risk perception attitude framework. J. Travel Res. 2019, 58, 849–865. [Google Scholar] [CrossRef]
- Seabra, C.; Dolnicar, S.; Abrantes, J.L.; Kastenholz, E. Heterogeneity in risk and safety perceptions of international tourists. Tour. Manag. 2013, 36, 502–510. [Google Scholar] [CrossRef]
- Quintal, V.A.; Lee, J.A.; Soutar, G.N. Risk, uncertainty and the theory of planned behavior: A tourism example. Tour. Manag. 2010, 31, 797–805. [Google Scholar] [CrossRef]
- Sönmez, S.F.; Graefe, A.R. Influence of terrorism risk on foreign tourism decisions. Ann. Tour. Res. 1998, 25, 112–144. [Google Scholar] [CrossRef] [Green Version]
- Borko, S.; Geerts, W.; Wang, H. The Travel Industry Turned Upside down: Insights, Analysis and Actions for Travel Executives. 2020. Available online: https://www.mckinsey.com/industries/travel-logistics-and-infrastructure/our-insights/the-travel-industry-turned-upside-down-insights-analysis-and-actions-for-travel-executives (accessed on 28 December 2021).
- Marcus, J. ‘Immunity Pods’ of Family and Friends Start to Venture out on Private ‘Vaxications’. Boston Sunday Globe, 4 April 2021; p. 13. Available online: https://assets.simpleviewinc.com/simpleview/image/upload/v1/clients/rhodeisland/Boston_Globe_4_4_21_b237746e-c8bc-4d2e-b503-7af21a9046ae.pdf(accessed on 15 December 2021).
- Quintal, V.; Sung, B.; Lee, S. Is the coast clear? Trust, risk-reducing behaviours and anxiety toward cruise travel in the wake of COVID-19. Curr. Issues Tour. 2022, 25, 206–218. [Google Scholar] [CrossRef]
- Fong, L.H.N.; Law, R.; Ye, B.H. Outlook of tourism recovery amid an epidemic: Importance of outbreak control by the government. Ann. Tour. Res. 2020, 86, 102951. [Google Scholar] [CrossRef]
- Sharieh, A.; Khurmah, R.A.; Masadeh, R.; Alzaqebah, A.; Alsharman, N.; Sharieh, F. Effect of Threat Control Management Strategies on Number Infected by COVID-19. In The Effect of Coronavirus Disease (COVID-19) on Business Intelligence; Alshurideh, M.T., Hassanien, A.E., Masa’deh, R., Eds.; Springer: Cham, Switzerland, 2021; pp. 15–41. [Google Scholar]
- Pasion, R.; Paiva, T.O.; Fernandes, C.; Barbosa, F. The AGE effect on protective behaviors during the COVID-19 outbreak: Sociodemographic, perceptions and psychological accounts. Front. Psychol. 2020, 11, 2785. [Google Scholar] [CrossRef]
- Chien, P.M.; Sharifpour, M.; Ritchie, B.W.; Watson, B. Travelers’ health risk perceptions and protective behavior: A psychological approach. J. Travel Res. 2017, 56, 744–759. [Google Scholar] [CrossRef]
- Albarracin, D.; Johnson, B.T.; Fishbein, M.; Muellerleile, P.A. Theories of reasoned action and planned behavior as models of condom use: A meta-analysis. Psychol. Bull. 2001, 127, 142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watts, F.N. Habituation model of systematic desensitization. Psychol. Bull. 1979, 86, 627–637. [Google Scholar] [CrossRef] [PubMed]
- Barros, M.N.; Aguiar, M.M.; Carvalho, F.; Macedo, A.; Pereira, A.T. COVID-19 Fear Scale-Validation and adaptation for the perinatal period. J. Hum. Growth Dev. 2021, 31, 9–17. [Google Scholar]
- Rimal, R.N.; Real, K. Perceived risk and efficacy beliefs as motivators of change: Use of the risk perception attitude (RPA) framework to understand health behaviors. Hum. Commun. Res. 2003, 29, 370–399. [Google Scholar] [CrossRef]
- Matiza, T.; Kruger, M. Ceding to their fears: A taxonomic analysis of the heterogeneity in COVID-19 associated perceived risk and intended travel behaviour. Tour. Recreat. Res. 2021, 46, 158–174. [Google Scholar] [CrossRef]
- Zhang, Y.-C.; Li, Z.; Zhou, G.-B.; Xu, N.-R.; Liu, J.-B. The Evolution Model of Public Risk Perception Based on Pandemic Spreading Theory under Perspective of COVID-19. Complexity 2021, 2021, 1015049. [Google Scholar] [CrossRef]
- Zenker, S.; Braun, E.; Gyimóthy, S. Too afraid to Travel? Development of a Pandemic (COVID-19) Anxiety Travel Scale (PATS). Tour. Manag. 2021, 84, 104286. [Google Scholar] [CrossRef]
- Sánchez-Cañizares, S.M.; Cabeza-Ramírez, L.J.; Muñoz-Fernández, G.; Fuentes-García, F.J. Impact of the perceived risk from COVID-19 on intention to travel. Curr. Issues Tour. 2021, 24, 970–984. [Google Scholar] [CrossRef]
- Tang, C.F.; Ozturk, I. Is tourism a catalyst of growth in Egypt? Evidence from Granger non-causality and the generalised variance decomposition analysis. Anatolia 2017, 28, 173–181. [Google Scholar] [CrossRef]
- World Travel and Tourism Council Travel & Tourism Economic Impact 2018 Egypt. 2018. Available online: https://studylib.net/doc/25207687/world-travel-and-tourism-council---travel-and-tourism---econo (accessed on 20 December 2021).
- Central Agency for Public Mobilization and Statistics. Statistics about Population. 2021. Available online: https://www.capmas.gov.eg/ (accessed on 11 December 2021).
- Din, S. Current status and prospects for development of international tourism in the Arab Republic of Egypt. In Proceedings of the International Scientific Conference “Far East Con” (ISCFEC 2020), Vladivostok, Russia, 6–9 October 2020; Atlantis Press: Amsterdam, The Netherlands, 2020; pp. 2401–2406. [Google Scholar]
- Samir, A.; Elabd, A.M.; Mohamed, W.; Baess, A.I.; Sweed, R.A.; Abdelgawad, M.S. COVID-19 in Egypt after a year: The first and second pandemic waves from the radiological point of view. Egypt. J. Radiol. Nucl. Med. 2021, 52, 168. [Google Scholar] [CrossRef]
- Salem, I.E.; Elkhwesky, Z.; Ramkissoon, H. A content analysis for government’s and hotels’ response to COVID-19 pandemic in Egypt. Tour. Hosp. Res. 2022, 22, 42–59. [Google Scholar] [CrossRef]
- Diab, A. 14 Governmental Measures to Confront the Second Wave of Coronavirus. Elwatannews. Available online: https://www.elwatannews.com/news/details/5052956 (accessed on 19 November 2020).
- Alashry, M.S.; Alkhudari, M. The Impact of COVID-19 Pandemic on Egypt’s Tourism. New Challenges for Media Houses to Make Awareness for Safety to Travel. J. Environ. Manag. Tour. 2021, 12, 2251–2262. [Google Scholar]
- Mahmoud, A.B.; Hack-Polay, D.; Reisel, W.D.; Fuxman, L.; Grigoriou, N.; Mohr, I.; Aizouk, R. Who’s more vulnerable? A generational investigation of COVID-19 perceptions’ effect on Organisational citizenship Behaviours in the MENA region: Job insecurity, burnout and job satisfaction as mediators. BMC Public Health 2021, 21, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, A.B.; Reisel, W.D.; Fuxman, L.; Hack-Polay, D. Locus of control as a moderator of the effects of COVID-19 perceptions on job insecurity, psychosocial, organisational, and job outcomes for MENA region hospitality employees. Eur. Manag. Rev. 2021. [Google Scholar] [CrossRef]
- Lojo, A. Young Chinese in Europe: Travel behavior and new trends based on evidence from Spain. Tourism 2020, 68, 7–20. [Google Scholar] [CrossRef] [Green Version]
- Packer, J.; Ballantyne, J. The impact of music festival attendance on young people’s psychological and social well-being. Psychol. Music. 2011, 39, 164–181. [Google Scholar] [CrossRef] [Green Version]
- Ranta, M.; Silinskas, G.; Wilska, T.A. Young adults’ personal concerns during the COVID-19 pandemic in Finland: An issue for social concern. Int. J. Sociol. Soc. Policy 2020, 40, 1201–1219. [Google Scholar] [CrossRef]
- Zhou, S.J.; Wang, L.L.; Yang, R.; Yang, X.J.; Zhang, L.G.; Guo, Z.C.; Chen, J.C.; Wang, J.Q.; Chen, J.X. Sleep problems among Chinese adolescents and young adults during the coronavirus-2019 pandemic. Sleep Med. 2020, 74, 39–47. [Google Scholar] [CrossRef]
- Huddy, L.; Feldman, S.; Capelos, T.; Provost, C. The consequences of terrorism: Disentangling the effects of personal and national threat. Political Psychol. 2002, 23, 485–509. [Google Scholar] [CrossRef]
- Seabra, C.; Kastenholz, E.; Abrantes, J.L.; Reis, M. Peacefulness at home: Impacts on international travel. Int. J. Tour. Cities 2018, 4, 413–428. [Google Scholar] [CrossRef]
- Huddy, L.; Khatib, N.; Capelos, T. Trends: Reactions to the terrorist attacks of September 11, 2001. Public Opin. Q. 2002, 66, 418–450. [Google Scholar] [CrossRef]
- Hair, J.; Hult, G.; Ringle, C.M.; Sarstedt, M. A Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM); SAGE Publications: Thousand Oaks, CA, USA, 2022. [Google Scholar]
- Ryan, C. Refereeing articles including SEM—What should referees look for? Tour. Crit. Pract. Theory 2020, 1, 47–61. [Google Scholar] [CrossRef]
- Chang, L.; Liu, Y.Y.; Lu, H.J.; Lansford, J.E.; Bornstein, M.H.; Steinberg, L.; Deater-Deckard, K.; Rothenberg, W.A.; Skinner, A.T.; Dodge, K.A. Slow life history strategies and increases in externalizing and internalizing problems during the COVID-19 pandemic. J. Res. Adolesc. 2021, 31, 595–607. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Ren, Y. Moral obligation, public leadership, and collective action for epidemic prevention and control: Evidence from the corona virus disease 2019 (COVID-19) emergency. Int. J. Environ. Res. Public Health 2020, 17, 2731. [Google Scholar] [CrossRef] [Green Version]
- Hilliard, H.M.; Cem, C.; Ignaszewski, M.J.; Sobowale, K.; Chokroverty, L. Social media for emergency messaging with youth and families during the coronavirus 2019 (COVID-19) pandemic: Getting it right. J. Emerg. Manag. 2021, 19, 109–116. [Google Scholar] [CrossRef]
- Levine, I.S. Travel Pods: The New Pandemic Vacation Trend. Forbes. Available online: https://www.forbes.com/sites/irenelevine/2020/08/28/travel-pods-the-new-pandemic-vacation-trend/?sh=39e16a853996 (accessed on 28 August 2020).
- Sanborn, F.W.; Harris, R.J. A Cognitive Psychology of Mass Communication; Routledge: London, UK, 2019. [Google Scholar]
- Wen, J.; Kozak, M.; Yang, S.; Liu, F. COVID-19: Potential effects on Chinese citizens’ lifestyle and travel. Tour. Rev. 2021, 76, 74–87. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristics | COVID-19 1st Wave n = 206 | COVID-19 2nd Wave n = 180 | ||
|---|---|---|---|---|
| n | % | n | % | |
| Gender | ||||
| Female | 157 | 76.2 | 130 | 72.2 |
| Male | 47 | 22.8 | 50 | 27.8 |
| Other/prefer not to say | 2 | 1.0 | 0 | 0 |
| Age (mean) | 21.6 years | 20.7 years | ||
| Education | ||||
| Middle school | 4 | 2.0 | 8 | 4.5 |
| High school | 2 | 1.0 | 4 | 2.2 |
| University or postgraduate degree | 200 | 97.1 | 168 | 93.3 |
| Occupation | ||||
| Student | 192 | 93.2 | 173 | 96.1 |
| Other | 14 | 7 | 7 | 4 |
| Unemployed | 0.0 | 0.0 | 0.0 | 0.0 |
| Number of trips abroad in the last 3 years | ||||
| Less than 5 trips | 154 | 74.8 | 123 | 68.3 |
| 6 to 10 trips | 29 | 14.1 | 34 | 18.9 |
| More than 10 trips | 21 | 10.2 | 23 | 12.8 |
| Missing | 2 | 1.0 | 0 | 0.0 |
| Construct/Associated Items | COVID-19 1st Wave | COVID-19 2nd Wave | ||||
|---|---|---|---|---|---|---|
| M | SD | α | M | SD | α | |
| Risk severity (TS) | 3.98 | 1.33 | 0.808 | 3.90 | 1.32 | 0.826 |
| 1. I am concerned that I or someone from my family could be a victim of coronavirus | 4.16 | 1.44 | 4.08 | 1.38 | ||
| 2. I have been bothered and feel nervous by coronavirus fear | 3.81 | 1.46 | 3.72 | 1.47 | ||
| Non-susceptibility (NS) | 1.46 | 1.03 | 0.868 | 1.61 | 1.16 | 0.944 |
| 1. Normal citizens are not likely to be victims of coronavirus | 1.52 | 1.14 | 1.61 | 1.21 | ||
| 2. Tourists are not likely to be victims of coronavirus | 1.39 | 1.06 | 1.60 | 1.18 | ||
| Travel safety perceptions (TSP) | 1.64 | 0.90 | 0.871 | 2.08 | 1.10 | 0.909 |
| 1. Travelling abroad with my family is very safe | 1.76 | 1.33 | 2.17 | 1.35 | ||
| 2. Travelling abroad to visit friends or relatives is perfectly safe | 1.60 | 1.25 | 2.04 | 1.41 | ||
| 3. Vacation travel abroad is perfectly safe | 1.50 | 1.19 | 1.88 | 1.33 | ||
| 4. Travelling abroad for business or work is perfectly safe | 1.54 | 1.12 | 2.06 | 1.33 | ||
| 5. I feel very comfortable travelling abroad right now | 1.46 | 1.16 | 1.95 | 1.43 | ||
| 6. Travelling in my country to visit friends or relatives is perfectly safe | 1.87 | 1.19 | 2.28 | 1.42 | ||
| 7. Travelling in my country for business or work is perfectly safe | 1.76 | 1.12 | 2.19 | 1.32 | ||
| Activities’ safety perceptions (ASP) | 1.40 | 0.72 | 0.940 | 1.88 | 0.93 | 0.941 |
| 1. Doing sports in closed spaces | 1.47 | 1.00 | 1.92 | 1.23 | ||
| 2. Shopping in shopping malls, streets, markets | 1.60 | 1.01 | 1.96 | 1.15 | ||
| 3. Sightseeing and going on organized visits | 1.55 | 1.04 | 2.20 | 1.29 | ||
| 4. Visiting art galleries, museums, monuments | 1.43 | 0.93 | 2.07 | 1.22 | ||
| 5. Going to casinos or gambling | 1.22 | 0.75 | 1.49 | 1.02 | ||
| 6. Going to concerts, festivals, shows | 1.25 | 0.80 | 1.55 | 1.11 | ||
| 7. Visiting historical and cultural sites, and city centres | 1.47 | 1.00 | 2.04 | 1.24 | ||
| 8. Going out at night, dancing, going to nightclubs or discos | 1.25 | 0.82 | 1.56 | 1.10 | ||
| 9. Dining in restaurants | 1.44 | 0.92 | 2.34 | 1.23 | ||
| 10. Attending sports events | 1.41 | 0.94 | 1.88 | 1.20 | ||
| 11. Going to amusement or theme parks | 1.31 | 0.83 | 1.71 | 1.09 | ||
| Acceptance of restrictions (RA) | 4.25 | 1.15 | 0.934 | 3.93 | 1.14 | 0.909 |
| 1. Total closure of borders | 4.05 | 1.41 | 3.36 | 1.57 | ||
| 2. Preventing citizens coming from areas affected by the disease, from entering my country | 4.26 | 1.31 | 4.12 | 1.34 | ||
| 3. More control on all countries’ borders | 4.41 | 1.23 | 4.12 | 1.30 | ||
| 4. Limitations in my country to receive migrants and foreigners | 4.20 | 1.36 | 3.90 | 1.37 | ||
| 5. Mandatory quarantine in case of disease diagnosis | 4.40 | 1.29 | 4.27 | 1.23 | ||
| 6. Limitations in all countries to receive migrants and foreigners | 4.18 | 1.31 | 3.81 | 1.44 | ||
| Intentions to change behaviour (ICB) | 3.75 | 1.32 | 0.726 | 3.74 | 1.30 | 0.826 |
| 1. I am thinking of changing travel or vacation plans due to the fear of coronavirus | 3.85 | 1.57 | 3.81 | 1.45 | ||
| 2. I am thinking about changing many aspects of my life and routines due to the fear of coronavirus | 3.66 | 1.41 | 3.67 | 1.36 | ||
| Construct/Associated Items | Loadings | CR | AVE | |||
|---|---|---|---|---|---|---|
| 1st Wave | 2nd Wave | 1st Wave | 2nd Wave | 1st Wave | 2nd Wave | |
| Risk severity (TS) | 0.912 | 0.921 | 0.838 | 0.853 | ||
| TS1 | 0.916 | 0.923 | ||||
| TS2 | 0.914 | 0.923 | ||||
| Non-susceptibility (NS) | 0.939 | 0.973 | 0.885 | 0.947 | ||
| NS1 | 0.941 | 0.975 | ||||
| NS2 | 0.940 | 0.972 | ||||
| Travel safety perceptions (TSP) | 0.901 | 0.928 | 0.566 | 0.648 | ||
| TSP1 | 0.674 | 0.817 | ||||
| TSP2 | 0.844 | 0.878 | ||||
| TSP3 | 0.779 | 0.868 | ||||
| TSP4 | 0.790 | 0.857 | ||||
| TSP5 | 0.691 | 0.729 | ||||
| TSP6 | 0.730 | 0.765 | ||||
| TSP7 | 0.745 | 0.702 | ||||
| Activities’ safety perceptions (ASP) | 0.949 | 0.950 | 0.631 | 0.635 | ||
| ASP1 | 0.763 | 0.814 | ||||
| ASP2 | 0.721 | 0.784 | ||||
| ASP3 | 0.740 | 0.717 | ||||
| ASP4 | 0.801 | 0.796 | ||||
| ASP5 | 0.822 | 0.854 | ||||
| ASP6 | 0.868 | 0.845 | ||||
| ASP7 | 0.790 | 0.766 | ||||
| ASP8 | 0.802 | 0.872 | ||||
| ASP9 | 0.749 | 0.693 | ||||
| ASP10 | 0.862 | 0.797 | ||||
| ASP11 | 0.807 | 0.811 | ||||
| Acceptance of restrictions (RA) | 0.948 | 0.932 | 0.752 | 0.695 | ||
| RA1 | 0.785 | 0.740 | ||||
| RA2 | 0.800 | 0.851 | ||||
| RA3 | 0.909 | 0.847 | ||||
| RA4 | 0.897 | 0.856 | ||||
| RA5 | 0.910 | 0.841 | ||||
| RA6 | 0.892 | 0.861 | ||||
| Intentions to change behaviour (ICB) | 0.880 | 0.920 | 0.785 | 0.852 | ||
| ICB1 | 0.879 | 0.931 | ||||
| ICB2 | 0.893 | 0.915 | ||||
| Constructs | Configural Invariance (Same Algorithms for Both Groups) | Compositional Invariance (Correlation = 1) | Partial Measurement Invariance Established | Equal Mean Assessment | Equal Variance Assessment | Full Measurement Invariance Established | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| C = 1 | Confidence Interval (CIs) | Differences | Confidence Interval (CIs) | Equal | Differences | Confidence Interval (CIs) | Equal | ||||
| TS | Yes | 1.000 | [0.999; 1.000] | Yes | −0.061 | [−0.199; 0.198] | Yes | −0.013 | [−0.289; 0.274] | Yes | Yes |
| NS | Yes | 1.000 | [0.999; 1.000] | Yes | 0.137 | [−0.196; 0.199] | Yes | 0.240 | [−0.490; 0.461] | Yes | Yes |
| TSP | Yes | 0.991 | [0.990; 1.000] | Yes | 0.437 | [−0.20. 0.205] | No | 0.412 | [−0.376; 0.369] | No | No |
| ASP | Yes | 0.998 | [0.997; 1.000] | Yes | 0.534 | [−0.200; 0.198] | No | 0.523 | [−0.547; 0.517] | No | No |
| RA | Yes | 0.999 | [0.999; 1.000] | Yes | −0.260 | [−0.200; 0.204] | No | −0.019 | [−0.347; 0.353] | Yes | No |
| ICB | Yes | 0.999 | [0.998; 1.000] | Yes | −0.013 | [−0.203; 0.200] | Yes | −0.038 | [−0.246; 0.234] | Yes | Yes |
| Hypothesis | Path Coefficient | Confidence Interval (95%) Bias Corrected | Path Coefficient Difference | p-Value Difference | Supported | |||
|---|---|---|---|---|---|---|---|---|
| COVID-19 1st Wave | COVID-19 2nd Wave | COVID-19 1st Wave | COVID-19 2nd Wave | MGA | Permutation Test | |||
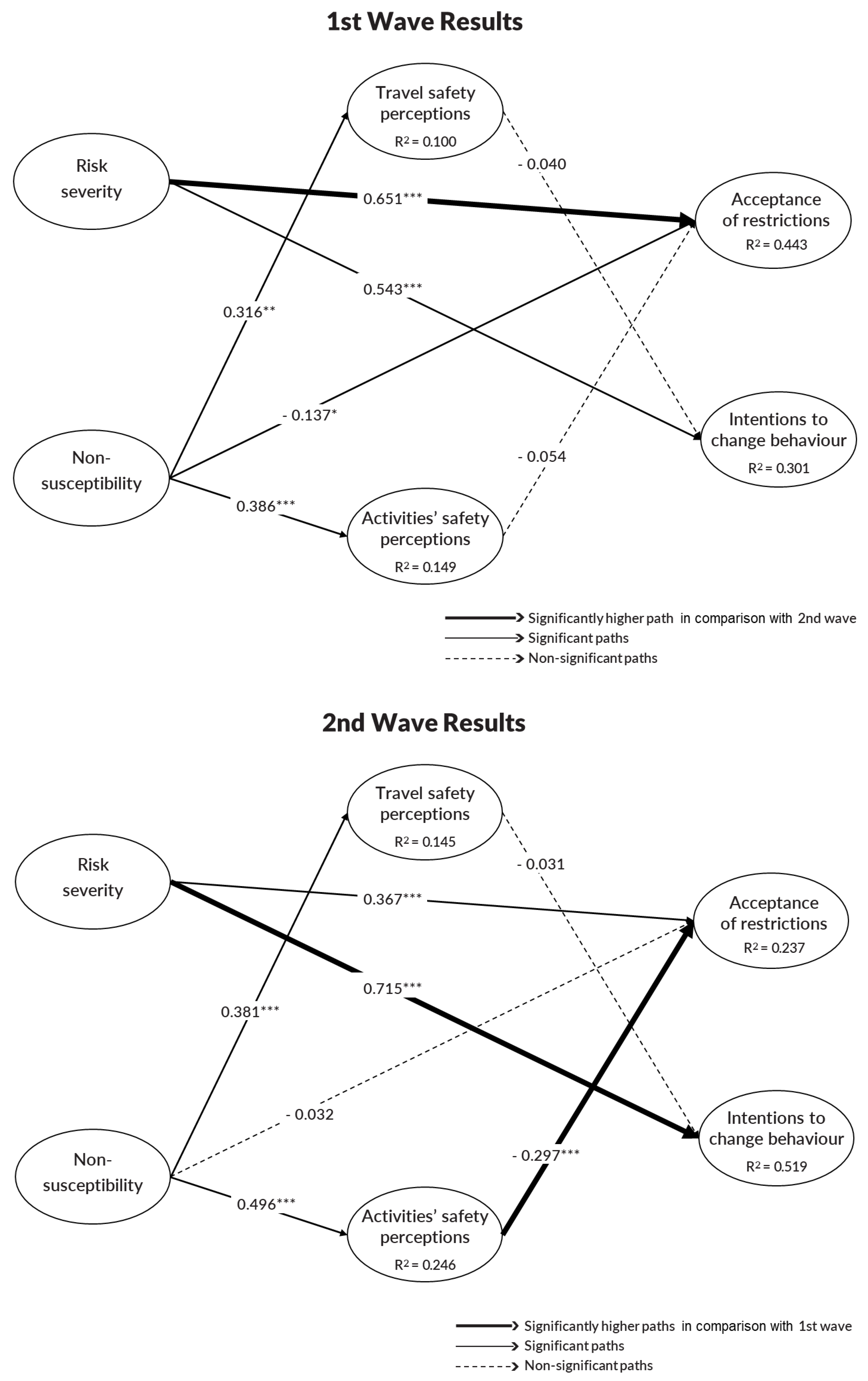
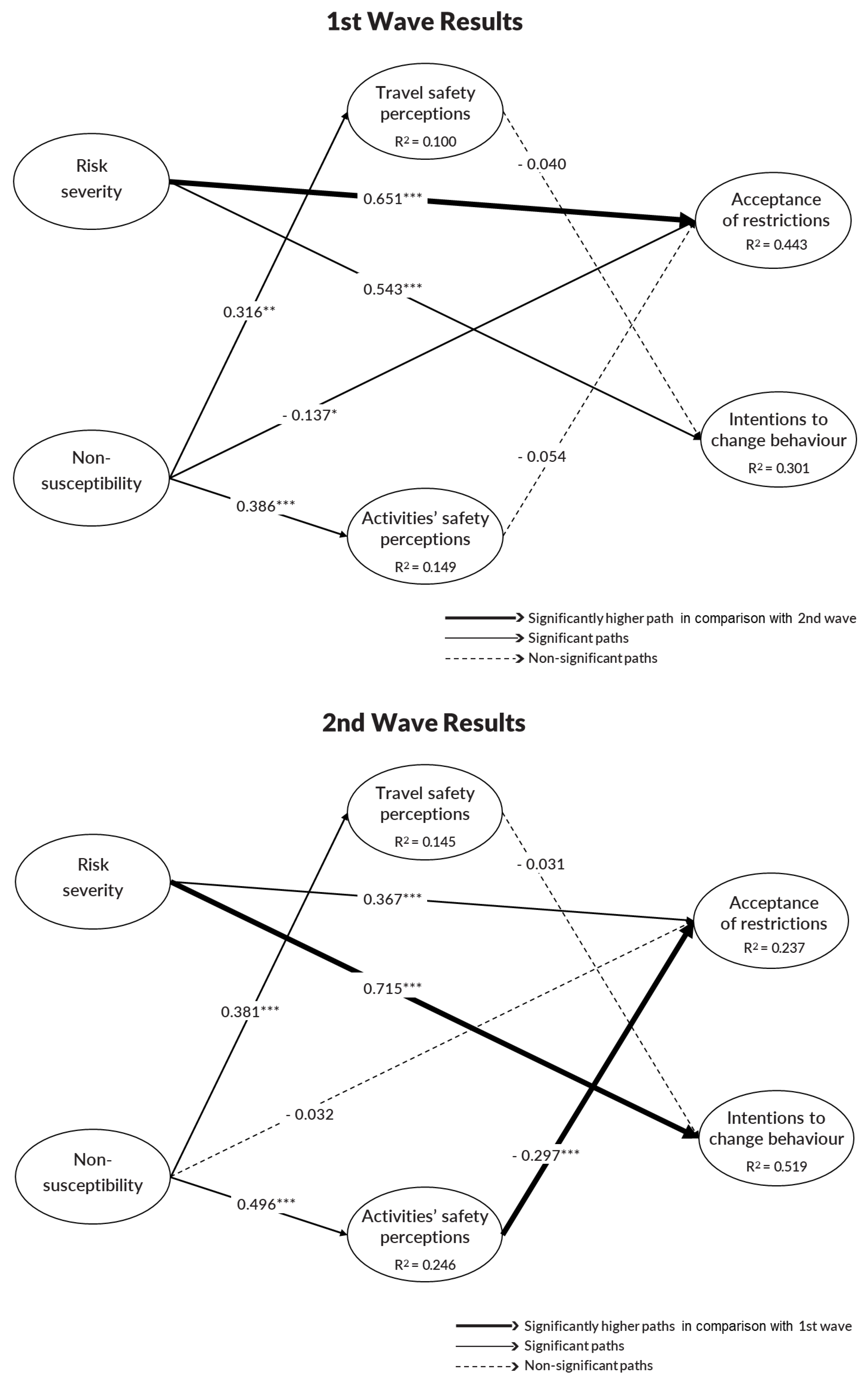
| H1. Non-susceptibility → Travel safety perceptions | 0.316 | 0.381 | [0.090; 0.493] | [0.217; 0.520] | –0.064 | 0.614 | 0.620 | No/No |
| H2. Non-susceptibility → Activities’ safety perceptions | 0.386 | 0.496 | [0.171; 0.582] | [0.315; 0.657] | –0.110 | 0.412 | 0.420 | No/No |
| H3. Non-susceptibility → Acceptance of restrictions | –0.137 | –0.032 | [–0.260; –0.050] | [–0.200; 0.120] | –0.105 | 0.271 | 0.288 | No/No |
| H4. Risk severity → Acceptance of restrictions | 0.651 | 0.367 | [0.521; 0.759] | [0.196; 0.514] | 0.284 | 0.005 | 0.004 | Yes/Yes |
| H5. Risk severity → Intentions to change behaviour | 0.543 | 0.715 | [0.397; 0.661] | [0.599; 0.808] | –0.172 | 0.044 | 0.049 | Yes/Yes |
| H6. Travel safety perceptions → Intentions to change behaviour | –0.040 | –0.031 | [–0.160; 0.093] | [–0.141; 0.084] | –0.009 | 0.916 | 0.920 | No/No |
| H7. Activities’ safety perceptions → Acceptance of restrictions | –0.054 | –0.297 | [–0.194; 0.053] | [–0.449; –0.117] | 0.243 | 0.029 | 0.028 | Yes/Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caldeira, A.M.; Seabra, C.; AlAshry, M.S. Contrasting the COVID-19 Effects on Tourism Safety Perceptions and Coping Behavior among Young People during Two Pandemic Waves: Evidence from Egypt. Sustainability 2022, 14, 7492. https://doi.org/10.3390/su14127492
Caldeira AM, Seabra C, AlAshry MS. Contrasting the COVID-19 Effects on Tourism Safety Perceptions and Coping Behavior among Young People during Two Pandemic Waves: Evidence from Egypt. Sustainability. 2022; 14(12):7492. https://doi.org/10.3390/su14127492
Chicago/Turabian StyleCaldeira, Ana Maria, Cláudia Seabra, and Miral Sabry AlAshry. 2022. "Contrasting the COVID-19 Effects on Tourism Safety Perceptions and Coping Behavior among Young People during Two Pandemic Waves: Evidence from Egypt" Sustainability 14, no. 12: 7492. https://doi.org/10.3390/su14127492
APA StyleCaldeira, A. M., Seabra, C., & AlAshry, M. S. (2022). Contrasting the COVID-19 Effects on Tourism Safety Perceptions and Coping Behavior among Young People during Two Pandemic Waves: Evidence from Egypt. Sustainability, 14(12), 7492. https://doi.org/10.3390/su14127492