
Networking Digital Platforms and Healthcare Project Finance Bankability


Abstract
1. Introduction
2. Literature Review
- healthcare PPP/PF investments;
- network theory, digital platforms, and applications to healthcare (to make infrastructural investments “smart”).
3. Methodology
- Higher margins improve bankability, with a cascade benefit on all the involved stakeholders.
- The value-adding “pie” sharing among the stakeholders may be conveniently mastered by the networking digital platforms, igniting a value co-creation process.
- Digitalization-driven cost savings positively impact financial and economic marginality (proxied by the Earnings Before Interests, Taxes, Depreciation and Amortization—EBITDA and other parameters) of the PPP/PF initiative, improving the networking interaction of the stakeholders.
- Better financial marginality improves the bankability of the project, making its acceptance likelier.
- The additional value “pie” created by digitalization is subdivided among the main stakeholders (public; private; patients, etc.).
- The interaction among the stakeholders is eased by the digital platform bridging properties, fostering the incentive to co-create and then share the additional value.
- (a)
- An economic–financial sensitivity analysis, where digital savings impact on key PF parameters, including bankability;
- (b)
- A mathematical interpretation, based on network theory, where the stakeholders of two ecosystems—respectively, without and with a digital platform—are compared.
3.1. From Standard to Smart Healthcare PF: A Sensitivity Simulation
- a scenario with +20% revenues/−20% costs;
- a scenario with +15% revenues/−15% costs;
- a scenario with +10% revenues/−10% costs;
- a scenario with +5% revenues/−5% costs;
- a scenario with +2% revenues/−2% costs.
- (a)
- Financial and economic performance analysis.
- (b)
- Network theory.
3.2. Financial and Economic Performance Analysis
- (a)
- the Net Present Value (NPV) of the project substantially increases, and so does the Internal Rate of Return (IRR) of the project (both parameters incorporate financial debt service, being based on operating cash flows), showing respectively a greater amount of wealth creation, and a higher hurdle rate compared to a break-even WACC;
- (b)
- even the residual remuneration of shareholders (NPVequity and IRRequity) consistently improves, indicating that after financial debt compensation is positive and substantial;
- (c)
- the payback period shortens, witnessing a lower financial break-even;
- (d)
- the average debt service coverage ratio substantially grows, showing an excess of operating cash flows created each year to properly serve the expiring financial debt (the threshold rate is 1); this is possibly the most important parameter for bankability, as it shows if and to which extent the SPV can generate enough liquidity to properly serve expiring financial debt;
- (e)
- the financial leverage also decreases, showing a lower ratio of financial debt to equity;
- (f)
- the WACC is the only parameter that (slightly) worsens, but this is just due to a weighting adjustment (improved economic/financial margins accelerate debt repayment, therefore diminishing the leverage and increasing the equity weights; since the cost of equity is higher than the cost of debt, the WACC increases).
- Even if the financial debtholders (mainly represented by the banks that preside over the bankability concerns) cannot increase the face value of their credit, they improve the likelihood of straightforward debt service that reduces delinquency risk.
- Sub-contractors follow a similar pattern, with no extra gains but a higher certainty of being fully paid in due time.
- Digital platforms are a pass-through virtual B2B2C stakeholder that may receive a fixed remuneration.
- Patients may hope for better care at more competitive prices.
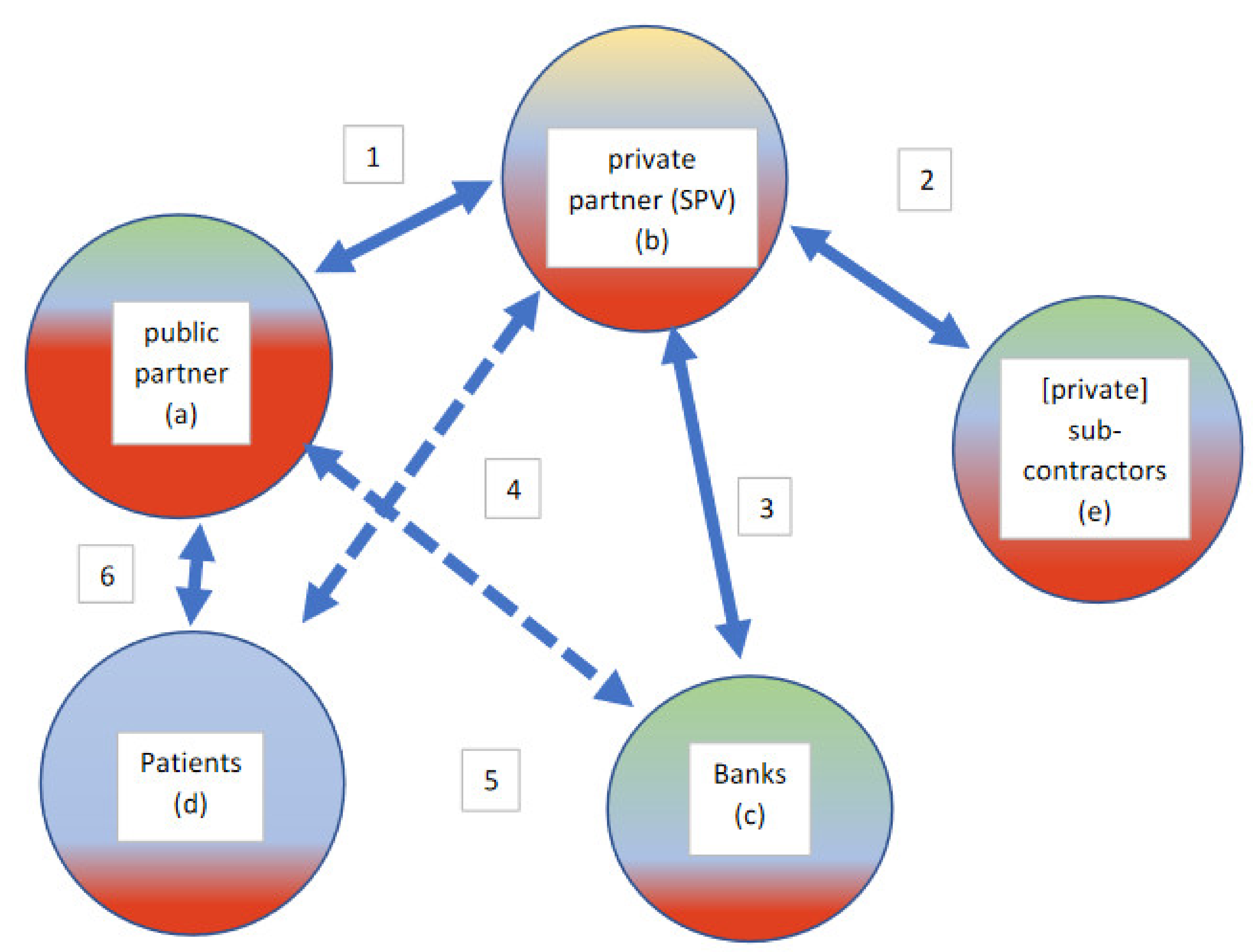
3.3. Network Theory Interpretation

| Legenda |
| 1. Private to Public invoicing: private income (cash-inflow) and specular public costs (cash-outflows) |
| 2. Sub-contractors to Private invoicing: private costs (cash-outflows) and sub-contractors income (cash-inflow) |
| 3. Private to Bank negative interests (costs and cash-outflows) and specular bank to private positive income |
| (revenues and cash-inflows); bank to private financing and payback |
| 4. Private supply to patients of non-core healthcare services |
| 5. Treasury intermediation (public to private payments are mediated by the banking agent) |
| 6. Public to the patient supply of services and patient to public payment of tickets |

| Legenda |
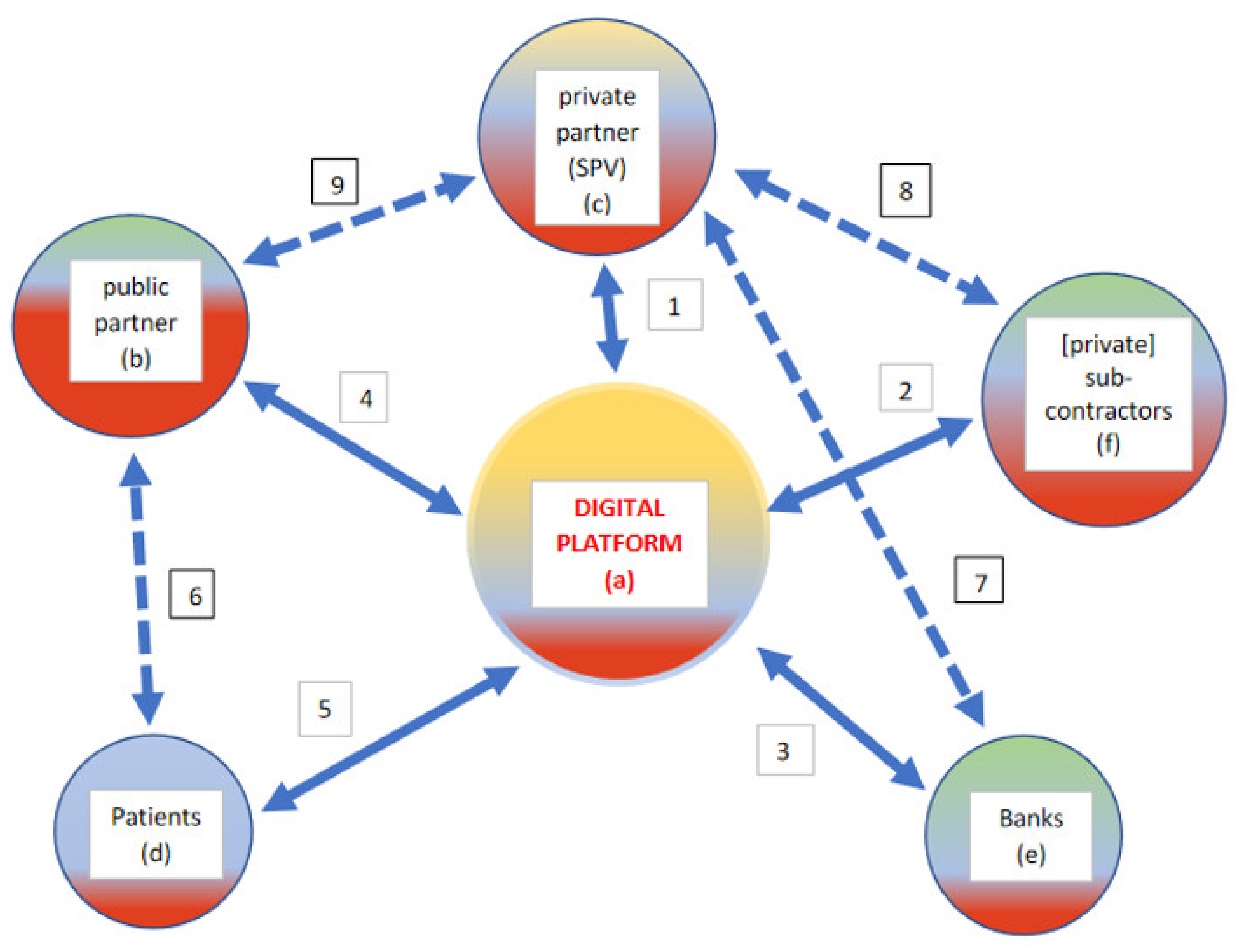
| 1 + 4. Private to Public invoicing Through the Digital Platform: private income (cash-inflow) and specular public costs (cash-outflows) |
| 2 + 1. Sub-contractors to Private invoicing through the Digital Platform: private costs (cash-outflows) and sub-contractors income (cash-inflow); digital B2B auctions are conducted through the platform, with time and cost savings along the digitized supply chain |
| 3 + 1. Private to Bank negative interests (costs and cash-outflows) and specular bank to private positive income (revenues and cash-inflows) |
| through the Digital Platform; bank to private financing and payback |
| 1+5. Private supply to patients (and visitors) of non-core healthcare services |
| 4 + 5. Public to the patient supply of services and patient to public payment of tickets through the Digital Platform |
| 5. Digital benefits for patients may be detected with Cost-Benefit Analysis and Cost-Effectiveness Analysis [51]. 6. Direct contact between patients and hospital (for healthcare treatment, etc.). 7. Indirect relationship between the private actor and the sponsoring banks (not intermediated through the digital platform/mobile banking). 8. Supply of physical goods and services to the private SPV. 9. Contractual public-to-private agreements. Supply of physical goods and services. |
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Action/Strategy/Device | Features and Impact |
|---|---|
| 1. Inclusion of digital platforms in the healthcare supply chain | Digital platforms enable and improve communication, knowledge generation, and information diffusion. Digital platforms accessed by a cluster of firms improve cooperation, coordination, and collaboration [60]. Platforms add up in the network a bridging node whose centrality improves traffic (volume of transactions, data, etc.). |
| 2. Digital scalability | Innovative business models can achieve exponentially increasing returns to scale as a response to digital disruption, fostering the growth multiplier. Economies of scale and experience lower the break-even point and foster long-term sustainability and resilience of the healthcare supply chain, even thanks to m-health applications [61]. |
| 3. Electronic health records (remote access and use to fuel big data and decision-making) | More and more health data are pulled from electronic health records to inform clinician decision-making. Paperless records are cheaper to store and use ubiquitously [62]. |
| 4. Inclusion of MedTech, digital health, and other innovative suppliers | Digital health’s primary value is to improve the triple aim: better outcomes, greater access, and affordable care (lower costs). Digital health has the power to decrease costs by 50% or more [63]. MedTech is a double-edged sword, with great potential but risky outcomes. MedTech can be effective in cutting healthcare costs, reduce repetitive tasks, and foster treatment optimization plans. |
| 5. Price-based competition with B auctions | Online reverse auctions (with one buyer and many competing sellers) are reshaping healthcare. E-auctions reduce transaction costs, ease coordination among stakeholders. Quality assessment may represent an obstacle to comparative auctions, and therefore standardization, whenever possible, is needed. |
| 6. Healthcare analytics | Acquisition and interpretation of (big) data improve the patient experience, decrease readmission rates, and provide a better quality of care, bringing to quality improvements, health cost reduction, and increased patient satisfaction. |
| 7. M-apps for access and feedbacks | Providers adopt m-health using mobile apps to ease clinical communication with patients to improve the management of hospital workflows. Mobile apps allow effective optimization of communication between providers, patients, and their caregivers, with a 24/7 personalized management of a patient’s condition. Bottom-up patient feedback (possibly, in real-time) refocus top-down strategies, fueling big data creation. |
| 8. Disease management/surveillance | Epidemic is a complex problem that can be traced using network theory [64]. Disease surveillance increasingly requires m-health devices and strategies. Prompt identification of patient zero represents, whenever possible, a mighty target. |
| 9. Transformation of (non-acute) in-patients to out-patients and home-patients | Chronic patients (suffering from diabetes, cardiovascular diseases, etc.) may avoid, whenever possible, unnecessary hospitalization, improving m-health and remote monitoring [53]. Savings and other socio-economic benefits are potentially enormous. |
| 10. Transmission of secured information through Blockchains/patient-driven interoperability | Patient-centered interoperability requires new challenges concerning privacy and security, incentives, technology, and governance that represented a prerequisite for scalability. Blockchain technology might facilitate the exchange of secured data through digital access rules, data aggregation, patient identity, and data immutability [65]. |
| 11. Personalized/precision medicine | Precision/personalized medicine differentiates people into different groups. Practices, interventions, medical decisions, and/or products are tailored to the individual patient according to their predicted response or risk of disease. Personalized medicine can tailor the fittest therapy with the highest safety margin for better patient care. |
| 12. Feedbacks from patients (customer experience/patient portals) Evaluation of treatment effectiveness-assessment of patient’s acuity level | Patients’ feedbacks may derive from data collected through M-apps (see point 7), fostering data mining applications [66]. Feedbacks enhance value co-creation, reducing information asymmetries and feeding big data. Electronic documentation can be used to predict patient acuity [67]. |
| 13. Digital medical devices | Digital medicine started around 2007 with the introduction of smartphones. Mobile devices connected with the Internet were incorporated in technology platforms following telemedicine patterns. Wearable sensors, endowing hand-held devices with the ability to acquire images and perform lab assays, complement the framework. This has resulted in a new path for generating in real-time, and in a real-world environment, medical data by the individual [68]. |
| 14. Telemedicine, e-health, m-health | Telemedicine applications are increasingly important in healthcare. Indispensable tools for remote patient monitoring, home healthcare, and disease management are made available. Applications are fully consistent with networking digital platforms (see Figure 2 and Figure 3). E-health and m-health may improve health outcomes (diagnosis, treatment, reduced hospitalization, longer life expectancy…) |
| 15. Artificial intelligence applications-(Early) prediction of pathologies-digital epidemiology | Prediction of pathologies can be carried forward with artificial intelligence patterns. Healthcare data and big data analytics are increasingly available, making the successful applications of AI in healthcare possible. Powerful AI techniques, driven by relevant clinical questions, can unlock clinically relevant information hidden in the massive amount of data, assisting clinical decision-making [69]. (Early) prediction of pathologies is enhanced by a combination of MedTech, precision medicine, patient-centered feedbacks, m-health, etc. |
| 16. Result-Based Financing (RBF) (Pay-for-Performance) | RBF for health consists of a non-monetary transfer or cash payment made to a manager, provider, or consumer as an incentive to use or deliver priority healthcare services. Payment is subordinated to measurable actions and benchmark savings. Technological applications in a PPP context can produce public savings that may be partially used to remunerate private players for their non-routine efforts [11]. |
References
- Yang, Y.; Zheng, R.; Zhao, L. Population aging, health investment and economic growth: Based on a cross-country panel data analysis. Int. J. Environ. Res. Public Health 2021, 18, 1801. [Google Scholar] [CrossRef] [PubMed]
- Baxter, D.; Casady, C.B. Proactive and strategic healthcare public-private partnerships (PPPs) in the coronavirus (Covid-19) epoch. Sustainability 2020, 12, 5097. [Google Scholar] [CrossRef]
- Hueskes, M.; Verhoest, K.; Block, T. Governing public–private partnerships for sustainability: An analysis of procurement and governance practices of PPP infrastructure projects. Int. J. Proj. Manag. 2017, 35, 1184–1195. [Google Scholar] [CrossRef]
- Barlow, J.; Roehrich, J.; Wright, S. Europe sees mixed results from public-private partnerships for building and managing health care facilities and services. Health Aff. 2013, 32, 146–154. [Google Scholar] [CrossRef] [PubMed]
- Boyer, E.J.; Van Slyke, D.M.; Rogers, J.D. An empirical examination of public involvement in public-private partnerships: Qualifying the benefits of public involvement in PPPs. J. Pub. Adm. Res. Theor. 2016, 26, 45–61. [Google Scholar] [CrossRef]
- Hellowell, M. The price of certainty: Benefits and costs of public–private partnerships for healthcare infrastructure and related services. Health Serv. Manag. Res. 2016, 29. [Google Scholar] [CrossRef]
- Kosycarz, E.A.; Nowakowska, B.A.; Mikołajczyk, M.M. Evaluating opportunities for successful public–private partnership in the healthcare sector in Poland. J. Pub. Health 2019, 27, 1–9. [Google Scholar] [CrossRef]
- Pereira, M.A.; Ferreira, D.C.; Marques, R.C. A critical look at the Portuguese public–private partnerships in healthcare. Int. J. Health Plan. Manag. 2020, 36, 302–315. [Google Scholar] [CrossRef]
- Moro Visconti, R. Multidimensional principal–agent value for money in healthcare project financing. Public Money Manag. 2014, 34, 259–264. [Google Scholar] [CrossRef]
- Moro Visconti, R.; Martiniello, L. Smart Hospitals and Patient-Centered Governance. Corp. Ownersh. Control. 2019, 16, 83–96. [Google Scholar] [CrossRef]
- Moro Visconti, R.; Martiniello, L.; Morea, D.; Gebennini, E. Can public-private partnerships foster investment sustainability in smart hospitals? Sustainability 2019, 11, 1704. [Google Scholar] [CrossRef]
- Moro Visconti, R. Corporate governance, digital platforms, and network theory: Information and risk-return sharing of connected stakeholders. Manag. Control. 2020, 2, 179–204. [Google Scholar] [CrossRef]
- Moro Visconti, R. Combining Network theory with corporate governance: Converging models for connected stakeholders. Corp. Ownersh. Control. 2019, 17, 125–139. [Google Scholar] [CrossRef]
- Hodge, G.; Greve, C.; Biygautane, M. Do PPP’s work? What and how have we been learning so far? Public Manag. Rev. 2018, 20, 1105–1121. [Google Scholar] [CrossRef]
- Narbaev, T.; De Marco, A.; Orazalin, N. A multi-disciplinary meta-review of the public–private partnerships research. Constr. Manag. Econ. 2020, 38, 109–125. [Google Scholar] [CrossRef]
- Wang, H.; Xiong, W.; Wu, G.; Zhu, D. Public–private partnership in Public Administration discipline: A literature review. Public Manag. Rev. 2018, 20, 293–316. [Google Scholar] [CrossRef]
- Rosell, J.; Saz-Carranza, A. Determinants of public–private partnership policies. Public Manag. Rev. 2020, 22, 1171–1190. [Google Scholar] [CrossRef]
- Aizawa, M.A. Scoping Study of PPP Guidelines. DESA Working Paper No. 154. January. Available online: https://www.un.org/esa/desa/papers/2018/wp154_2018.pdf (accessed on 26 April 2021).
- Akintoye, A.; Beck, M.; Kumaraswamy, M. Public Private Partnerships; A Global Review; Routledge: London, UK, 2016. [Google Scholar]
- Moro Visconti, R.; Dos, A.; Pelin Gurgun, A. Public-private partnerships for sustainable healthcare in emerging economies. In Handbook on Public-Private Partnerships in Developing & Emerging Economies; Leitão, J., Ed.; Emerald Group Publishing: London, UK, 2017; pp. 409–442. [Google Scholar]
- Fanelli, S.; Salvatore, F.P.; De Pascale, G.; Faccilongo, N. Insights for the future of health system partnerships in low- and middle-income countries: A systematic literature review. BMC Health Serv. Res. 2020, 20. [Google Scholar] [CrossRef]
- Roehrich, J.K.; Lewis, M.A.; George, G. Are public–private partnerships a healthy option? A systematic literature reviews. Soc. Sci. Med. 2014, 113, 110–119. [Google Scholar] [CrossRef]
- Torchia, M.; Calabrò, A.; Morner, M. Public–Private Partnerships in the Health Care Sector: A systematic review of the literature. Public Manag. Rev. 2015, 17, 236–261. [Google Scholar] [CrossRef]
- Venkat Raman, A.; Björkman, J.W. Public-private partnerships in healthcare. In The Palgrave International Handbook of Healthcare Policy and Governance; Palgrave Macmillan: London, UK, 2016; pp. 376–392. [Google Scholar]
- Barabási, A. Network Science; Cambridge University Press: Cambridge, UK, 2016. [Google Scholar]
- Asadullah, A.; Faik, I.; Kankanhalli, A. Digital Platforms: A Review and Future Directions; Twenty-Second Pacific Asia Conference on Information Systems, Japan. 2018. Available online: https://www.academia.edu/37873177/Digital_Platforms_A_Review_and_Future_Directions (accessed on 26 April 2021).
- Sutherland, W.; Jarrahi, M.H. The sharing economy and digital platforms: A review and research agenda. Int. J. Infor. Manag. 2018, 43, 328–341. [Google Scholar] [CrossRef]
- Iyawa, G.E.; Herselman, M.; Botha, A. A Scoping Review of Digital Health Innovation Ecosystems in Developed and Developing Countries; Conference: IST Africa, At Windhoek, Namibia, 2017. Available online: https://www.researchgate.net/publication/318013312_A_Scoping_Review_of_Digital_Health_Innovation_Ecosystems_in_Developed_and_Developing_Countries (accessed on 26 April 2021).
- Ranerup, A.; Zinner Henriksen, H.; Hedman, J. An analysis of business models in public service platforms. Gov. Inform. Q. 2016, 33, 6–14. [Google Scholar] [CrossRef]
- Menvielle, L.; Audrain-Pontevia, A.; Menvielle, W. The Digitization of Healthcare. New Challenges and Opportunities; Palgrave Macmillan: Cham, Switzerland, 2017. [Google Scholar]
- Velez-Lapão, L. The Challenge of Digital transformation in Public Health in Europe? Eur. J. Public Health. 2019, 29. [Google Scholar] [CrossRef]
- Moro Visconti, R.; Morea, D. Healthcare digitalization and pay-for-performance incentives in smart hospital project financing. Int. J. Environ. Res. Pub. Health 2020, 17, 2318. [Google Scholar] [CrossRef]
- Kagermann, H. Change through digitization -value creation in the age of Industry 4.0. In Management of Permanent Change; Albach, H., Meffert, H., Pinkwart, A., Reichwald, R., Eds.; Springer Fachmedien: Wiesbaden, German, 2015. [Google Scholar]
- EXPH (Expert Panel on Effective Ways of Investing in Health). Assessing the Impact of Digital Transformation of Health Services. 2019. Available online: https://ec.europa.eu/health/sites/health/files/expert_panel/docs/022_digitaltransformation_en.pdf (accessed on 26 April 2021).
- Nghiem, S.H.; Connelly, L.C. Convergence and determinants of health expenditures in OECD countries. Health Econ. Rev. 2017, 7, 1–11. [Google Scholar] [CrossRef]
- Fenwick, M.; McCahery, J.A.; Vermeulen, E.P.M. The End of ‘Corporate’ Governance: Hello ‘Platform’ Governance. Eur. Bus. Organ. Law Rev. 2019, 20, 171–199. [Google Scholar] [CrossRef]
- Blaschke, M.; Uwe, R.; Kazem, H.; Aier, S. Design principles for digital value co-creation networks: A service-dominant logic perspective. Electron. Mark. 2019, 29, 443–447. [Google Scholar] [CrossRef]
- Beirão, G.; Patrício, L.; Fisk, R.P. Value Co-creation in service ecosystems. J. Serv. Manag. 2017, 28, 227–249. [Google Scholar] [CrossRef]
- Galvagno, M.; Dalli, D. Theory of value co-creation: A systematic literature review. Manag Serv Qual. 2014, 24, 643–683. [Google Scholar] [CrossRef]
- Net Engineering. New Acute-Care Hospital Complex of Monselice-Este. 2015. Available online: https://www.net-italia.com/wp-content/uploads/2015/05/Monselice-Este-Hospital.pdf (accessed on 26 April 2021).
- Steam. Borgo Roma Hospital—Verona. 2020. Available online: https://www.steam.it/project/borgo-roma-hospital-verona/ (accessed on 26 April 2021).
- Addarii, F.; Lipparini, F.; Medda, F. Impact Investing Innovation: Bringing Together Public, Private and Third Sectors to Create Greater Value: The Case of the Public Private Partnership Initiative for the New Public Hospital of Treviso. In Social Impact Investing Beyond the SIB Evidence from the Market; La Torre, M., Calderini, M., Eds.; Palgrave Macmillan: Cham, Stwitzerland, 2018; pp. 115–140. [Google Scholar]
- Steam. New Cittadella Sanitaria of Ca’ Foncello Hospital—Treviso. 2020. Available online: https://www.steam.it/project/new-cittadella-sanitaria-of-ca-foncello-hospital-treviso/ (accessed on 26 April 2021).
- Finlombarda. Finlombarda survey of Project Finance in Healthcare Sector; Maggioli Editore: Rimini, Italy, 2012. [Google Scholar]
- Moro Visconti, R.; Morea, D. Big Data for the Sustainability of Healthcare Project Financing. Sustainability 2019, 11, 3748. [Google Scholar] [CrossRef]
- Dubey, R.; Gunasekaran, A.; Childe, S.J.; Wamba, S.F.; Papadopoulos, T. The impact of big data on world-class sustainable manufacturing. Int. J. Adv. Manufact. Techn. 2016, 84, 631–645. [Google Scholar] [CrossRef]
- McKinsey&Company. Big Data: The Next Frontier for Innovation, Competition, and Productivity. 2011. Available online: https://www.mckinsey.com/~/media/McKinsey/Business%20Functions/McKinsey%20Digital/Our%20Insights/Big%20data%20The%20next%20frontier%20for%20innovation/MGI_big_data_full_report.ashx (accessed on 26 April 2021).
- Papadopoulos, T.; Gunasekaran, A.; Dubey, R.; Altay, N.; Childe, S.J.; Fosso-Wamba, S. The role of Big Data in explaining disaster resilience in supply chains for sustainability. J. Clean Prod. 2017, 142, 1108–1118. [Google Scholar] [CrossRef]
- Witjas-Paalberends, E.R.; van Laarhoven, L.P.M.; van de Burgwal, L.H.M.; Feilzer, J.; de Swart, J.; Claassen, E.; Jansen, W.T.M. Challenges and best practices for big data-driven healthcare innovations conducted by profit–non-profit partnerships—A quantitative prioritization. Int. J. Health Manag. 2018, 11, 171–181. [Google Scholar] [CrossRef]
- Burke, R.; Demirag, I. Risk management by SPV partners in toll road public private partnerships. Pub. Manag. Rev. 2019, 21, 711–731. [Google Scholar] [CrossRef]
- Bergmo, T.S. How to measure costs and benefits of ehealth interventions: An overview of methods and frameworks. J. Med. Internet Res. 2015, 17, e254. [Google Scholar] [CrossRef]
- Bianconi, G. Multilayer Networks; Oxford University Press: Oxford, UK, 2018. [Google Scholar]
- Moro Visconti, R.; Larocca, A.; Marconi, M. Accessibility to First-Mile health services: A time-cost model for rural Uganda. Soc. Sci. Med. 2020, 265, 1–12. [Google Scholar] [CrossRef]
- Cappellaro, G.; Ricci, A. PPPs in health and social services: A performance measurement perspective. Public Money Manag. 2017, 37, 417–424. [Google Scholar] [CrossRef]
- Catuogno, S.; Arena, C.; Saggese, S.; Sarto, F. Performance implications of public–private partnerships in research hospitals: Lessons from the involvement of a charity. Health Serv. Manag. Res. 2016, 29, 91–98. [Google Scholar] [CrossRef]
- De Marco, A.; Mangano, G. Risk and value in privately financed health care projects. J. Constr. Eng. Manag. 2013, 139, 918–926. [Google Scholar] [CrossRef]
- Cui, C.; Liu, Y.; Hope, A.; Wang, J. Review of studies on the public–private partnerships (PPP) for infrastructure projects. Int. J. Proj. Manag. 2018, 36, 773–794. [Google Scholar] [CrossRef]
- Benítez-Ávila, C.; Hartmann, A.; Dewulf, G.; Henseler, J. Interplay of relational and contractual governance in public-private partnerships: The mediating role of relational norms, trust and partners’ contribution. Int. J. Proj. Manag. 2018, 36, 429–444. [Google Scholar] [CrossRef]
- Biygautane, M.; Neesham, C.; Al-Yahya, K. Institutional entrepreneurship, and infrastructure public-private partnership (PPP): Unpacking the role of social actors in implementing PPP projects. Int. J. Proj. Manag. 2019, 37, 192–219. [Google Scholar] [CrossRef]
- Cremona, L.; Lin, T.; Ravarini, A. The Role of Digital Platforms in Inter-Firm Collaboration. In Proceedings of the 8th Mediterranean Conference on Information Systems, Verona, Italy, 3–5 September 2014. [Google Scholar]
- Prasad, S. Designing for Scalability and Trustworthiness in mHealth Systems. In Proceedings of the 11th International Conference on Distributed Computing and Internet Technology, ICDCIT 2015, Bhubaneswar, India, 5–8 February 2015; Natarajan, R., Barua, G., Patra, M.R., Eds.; Springer: Cham, Switzerland, 2015. [Google Scholar]
- Kruse, C.S.; Stein, A.; Thomas, H.; Kaur, H. The use of electronic health records to support population health: A systematic review of the literature. J. Med. Syst. 2018, 42, 214. [Google Scholar] [CrossRef]
- Wasden, C.; Wasden, M. Tension: The Energy of Innovation. How Harnessing Tension Accelerates and Fuels Your Creative Genius; Scipio Press: Midway, UT, USA, 2015. [Google Scholar]
- Han, S.; Preciado, V.; Nowzari, C.; Pappas, G. Data-driven network resource allocation for controlling spreading processes. IEEE Tran. Net. Sci. 2015, 2, 1–11. [Google Scholar] [CrossRef]
- Gordon, W.J.; Catalini, C. Blockchain technology for healthcare: Facilitating the transition to patient-driven interoperability. Comput. Struct. Biotech. J. 2018, 16, 224–230. [Google Scholar] [CrossRef]
- Koh, H.C.; Tan, G. Data mining applications in healthcare. J. Health Inf. Manag. 2011, 19, 64–72. [Google Scholar]
- Kontio, E.; Airola, A.; Pahikkala, T.; Lundgren-Laine, H.; Junttila, K.; Korvenranta, H.; Salakoski, T.; Salanterä, S. Predicting patient acuity from electronic patient records. J. Biom. Inform. 2014, 51, 35–40. [Google Scholar] [CrossRef][Green Version]
- Topol, S. A decade of digital medicine innovation. Sci. Transl. Med. 2019, 11, eaaw7610. [Google Scholar] [CrossRef]
- Jiang, F.; Jiang, Y.; Zhi, H.; Dong, Y.; Li, H.; Ma, S.; Wang, Y.; Dong, Q.; Shen, H.; Wang, Y. Artificial intelligence in healthcare: Past, present, and future. Stroke Vasc. Neurol. 2017, 2, 230–243. [Google Scholar] [CrossRef]


 | ||||||
|---|---|---|---|---|---|---|
| Base Case | +/−20% | +/−15% | +/−10% | +/−5% | +/−2% | |
| Impact of Digitalization | Impact of Digitalization | Impact of Digitalization | Impact of Digitalization | Impact of Digitalization | ||
| Extension of the PF concession (years) | 28 | 28 | 28 | 28 | 28 | 28 |
| Yearly Availability Payment (*) (€) | 3,000,000 | 3,000,000 | 3,000,000 | 3,000,000 | 3,000,000 | 3,000,000 |
| Yearly Service Revenues (*) (€) | 18,675,000 | 18,675,000 | 18,675,000 | 18,675,000 | 18,675,000 | 18,675,000 |
| Yearly Commercial Revenues (€) (*) | 5,000,000 | 5,000,000 | 5,000,000 | 5,000,000 | 5,000,000 | 5,000,000 |
| Fixed Investment Sum (€) (#) | 100,000,000 | 100,000,000 | 100,000,000 | 100,000,000 | 100,000,000 | 100,000,000 |
| Public Grants (€) (#) | 50,000,000 | 50,000,000 | 50,000,000 | 50,000,000 | 50,000,000 | 50,000,000 |
| Equity (Share Capital) (€) | 5,000,000 | 5,000,000 | 5,000,000 | 5,000,000 | 5,000,000 | 5,000,000 |
| Subordinated Financial debt (€) | 10,000,000 | 10,000,000 | 10,000,000 | 10,000,000 | 10,000,000 | 10,000,000 |
| Senior Financial debt (€) | 46,978,861 | 47,541,094 | 47,388,242 | 47,243,758 | 47,107,383 | 47,029,344 |
| Average Inflation Rate (%) | 3 | 3 | 3 | 3 | 3 | 3 |
| Senior Financial debt Rate (%) | 5.81 | 5.81 | 5.81 | 5.81 | 5.81 | 5.81 |
| Subordinated Financial debt Rate (%) | 6.06 | 6.06 | 6.06 | 6.06 | 6.06 | 6.06 |
| Total Financial Charges (€) | 40,334,867 | 40,657,903 | 40,570,070 | 40,487,052 | 40,408,700 | 40,363,868 |
| Net Present Value (NPV)equity (€) | 17,229,881 | 1,210,460,994 | 492,869,901 | 196,306,265 | 71,562,595 | 33,909,517 |
| Net Present Value (NPV)project (€) | 30,034,485 | 1,898,642,621 | 773,383,379 | 309,151,060 | 114,349,865 | 55,857,674 |
| Payback Period (year) | 2029 | 2023 | 2024 | 2024 | 2026 | 2028 |
| Average Debt Service Cover Ratio (ADSCR) | 2.02 | 48.92 | 21.86 | 9.74 | 4.38 | 2.75 |
| Equity Internal Rate of Return (IRR)equity | 11.66 | 38.65 | 32.52 | 26.13 | 19.33 | 14.86 |
| Project Internal Rate of Return (IRR)project | 10.91 | 37.47 | 30.72 | 24.04 | 17.44 | 13.51 |
| Weighted Average Cost of Capital—WACC (%) | 6.38 | 6.98 | 6.84 | 6.68 | 6.51 | 6.43 |
| Average Financial Leverage | 1.19 | 0.65 | 0.76 | 0.88 | 1.03 | 1.13 |
| a | b | c | d | e | |
|---|---|---|---|---|---|
| a | 0 | 1 | 1 | 1 | 0 |
| b | 1 | 0 | 1 | 1 | 1 |
| c | 1 | 1 | 0 | 0 | 0 |
| d | 1 | 1 | 0 | 0 | 0 |
| e | 0 | 1 | 0 | 0 | 0 |
| a | b | c | d | e | f | |
|---|---|---|---|---|---|---|
| a | 0 | 1 | 1 | 1 | 1 | 1 |
| b | 1 | 0 | 1 | 1 | 0 | 0 |
| c | 1 | 1 | 0 | 0 | 1 | 1 |
| d | 1 | 1 | 0 | 0 | 0 | 0 |
| e | 1 | 0 | 1 | 0 | 0 | 0 |
| f | 1 | 0 | 1 | 0 | 0 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moro-Visconti, R. Networking Digital Platforms and Healthcare Project Finance Bankability. Sustainability 2021, 13, 5061. https://doi.org/10.3390/su13095061
Moro-Visconti R. Networking Digital Platforms and Healthcare Project Finance Bankability. Sustainability. 2021; 13(9):5061. https://doi.org/10.3390/su13095061
Chicago/Turabian StyleMoro-Visconti, Roberto. 2021. "Networking Digital Platforms and Healthcare Project Finance Bankability" Sustainability 13, no. 9: 5061. https://doi.org/10.3390/su13095061
APA StyleMoro-Visconti, R. (2021). Networking Digital Platforms and Healthcare Project Finance Bankability. Sustainability, 13(9), 5061. https://doi.org/10.3390/su13095061