
ADHD and Sluggish Cognitive Tempo: Comparing Executive Functioning Response Patterns


 , , , and
, , , and
Abstract
1. Introduction
Executive Function in ADHD and SCT: Similarities and Differences
2. Materials and Methods
2.1. Participants
- The presence of symptoms for more than 6 months.
- The presence of a significant deterioration in academic, emotional or social activity.
- The absence of a diagnosis of schizophrenia, psychotic disorder, or any other neurodevelopmental disorder, intellectual disability, and/or sensory or motor deficits.
- An IQ ≥ 80 on the fifth edition on the Wechsler Intelligence Scale for Children (WISC-V).
- The presence of symptoms for more than 6 months.
- The presence of a significant deterioration in academic, emotional or social activity.
- The absence of a diagnosis of schizophrenia, psychotic disorder, or any other neurodevelopmental disorder, intellectual disability, and/or sensory or motor deficits.
- An IQ ≥ 80 on the fifth edition on the Wechsler Intelligence Scale for Children (WISC-V).
2.2. Instrument
2.3. Procedure
2.4. Statistical Analysis
3. Results
4. Discussion
4.1. Emotional Self-Regulation and Self-Motivation
4.2. Self-Restraint and Inhibition
4.3. Time Self-Management, Self-Organization and Problem Solving
5. Conclusions
6. Study Limitations and Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Compared Subsamples | Subscales | Total Scale | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Time | Problem | Inhibition | Motivatation | Emotion | ||||||||
| p | d | p | d | p | d | p | d | p | d | p | d | |
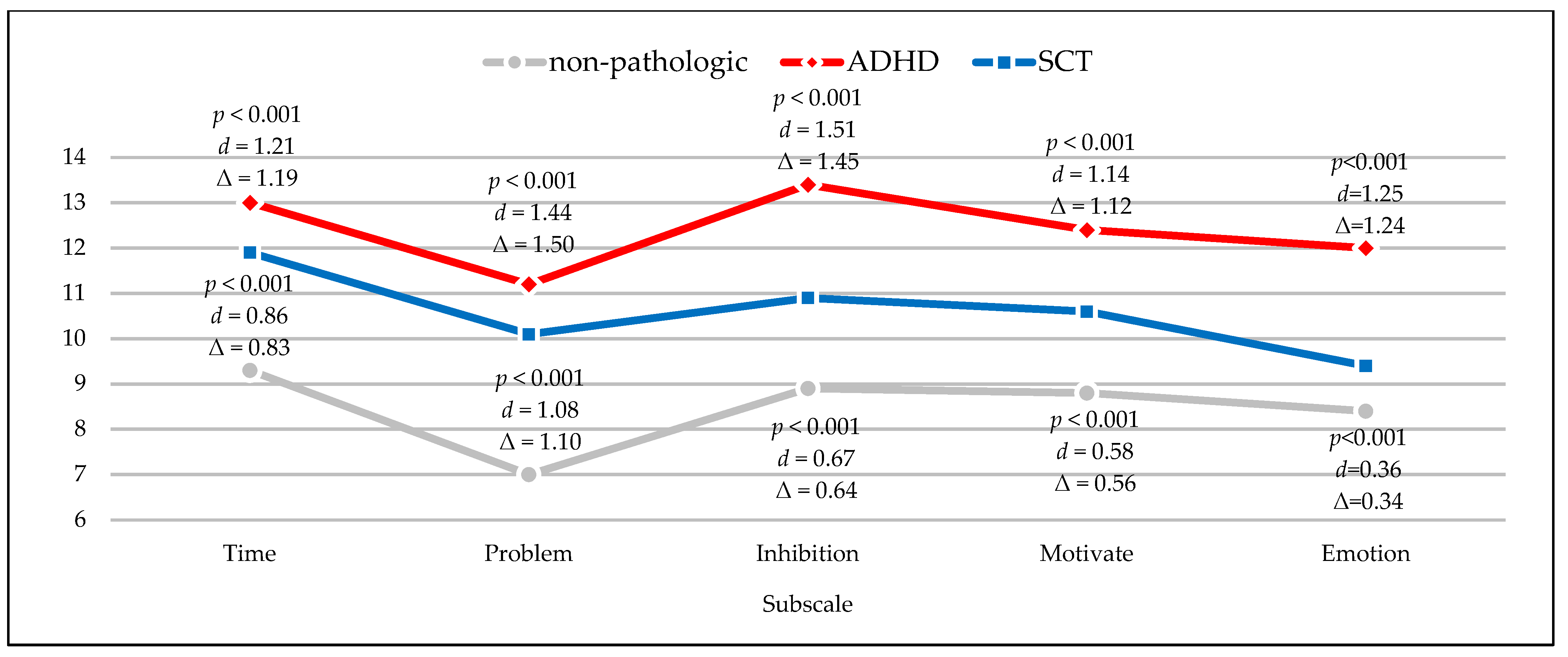
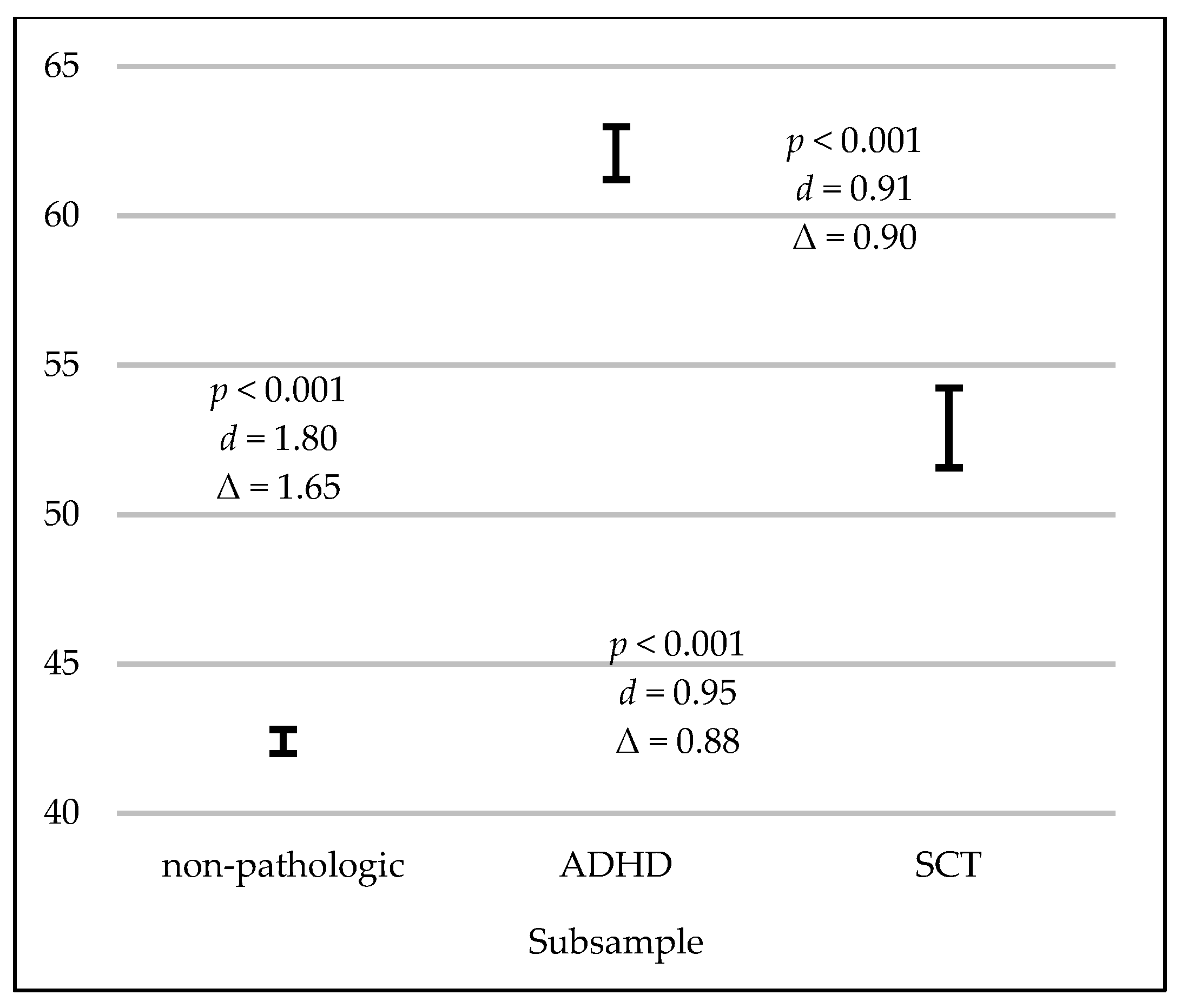
| Non-pathologic and ADHD | <0.001 | 1.21 | <0.001 | 1.44 | <0.001 | 1.51 | <0.001 | 1.14 | <0.001 | 1.25 | <0.001 | 1.80 |
| Non-pathologic and SCT | <0.001 | 0.86 | <0.001 | 1.08 | <0.001 | 0.67 | <0.001 | 0.58 | 0.022 | 0.36 | <0.001 | 0.95 |
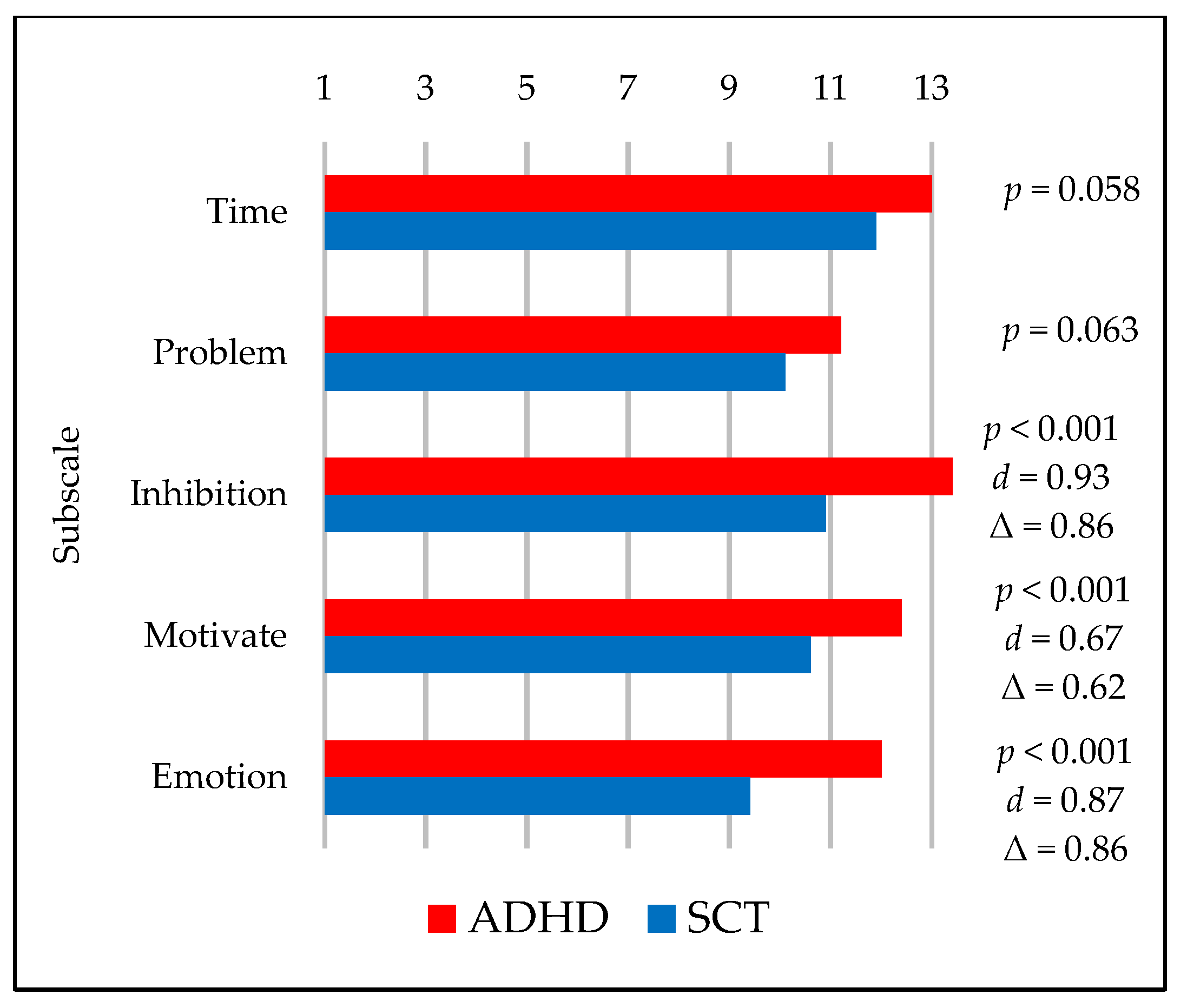
| ADHD and SCT | 0.058 | 0.40 | 0.063 | 0.31 | <0.001 | 0.93 | 0.001 | 0.67 | <0.001 | 0.87 | <0.001 | 0.91 |
References
- Luria, A.R. Higher Cortical Functions in Man, 1st ed.; Springer: Boston, MA, USA, 1966. [Google Scholar] [CrossRef]
- Lezak, M.D. The problem of assessing executive functions. Int. J. Psychol. 1982, 17, 281–297. [Google Scholar] [CrossRef]
- Norman, D.A.; Shallice, T. Attention to action. In Consciousness and Self-Regulation, 1st ed.; Davidson, R.J., Schwartz, G.E., Shapiro, D., Eds.; Springer: Boston, MA, USA, 1986; pp. 1–18. [Google Scholar] [CrossRef]
- Stuss, D.T.; Benson, D.F. Neuropsychological studies of the frontal lobes. Psychol. Bull. 1984, 95, 3–28. [Google Scholar] [CrossRef] [PubMed]
- Damasio, A.R. Emotion in the perspective of an integrated nervous system. Brain Res. Rev. 1998, 26, 83–86. [Google Scholar] [CrossRef]
- Miyake, A.; Friedman, N.P. The nature and organization of individual differences in executive functions: Four general conclusions. Curr. Dir. Psychol. Sci. 2012, 21, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.E. A New Understanding of ADHD in Children and Adults: Executive Function Impairments, 1st ed.; Routledge: London, UK, 2013. [Google Scholar] [CrossRef]
- Tirapu, J.; Muñoz-Céspedes, J.M.; Pelegrín, C. Funciones Ejecutivas: Necesidad de una integración conceptual. Rev. Neurol. 2002, 34, 673–685. [Google Scholar] [CrossRef]
- Diamond, A. Executive Functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef]
- Barkley, R.A. Barkley Deficits in Executive Functioning Scale-Children and Adolescents (BDEFS-CA); Guilford Press: New York, NY, USA, 2012. [Google Scholar]
- Bronowski, J. A Sense of the Future, 1st ed.; MIT Press: Cambridge, MA, USA, 1977. [Google Scholar]
- Fuster, J. The Prefrontal Cortex, 3rd ed.; Lippincott-Raven: Philadelphia, PA, USA, 1997. [Google Scholar]
- Barkley, R.A. Behavioral Inhibition, Sustained Attention, and Executive Functions: Constructing a unifying theory of ADHD. Psychol. Bull. 1997, 121, 65–94. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Castellanos, F.X.; Tannock, R. Neuroscience of attention-deficit/hyperactivity disorder: The search for endophenotypes. Nat. Rev. Neurosci. 2002, 3, 617–628. [Google Scholar] [CrossRef]
- Epstein, J.N.; Casey, B.J.; Tonev, S.T.; Davidson, M.C.; Reiss, A.L.; Garrett, A.; Hinshaw, S.P.; Greenhill, L.L.; Glover, G.; Shafritz, K.M.; et al. ADHD-and medication-related brain activation effects in concordantly affected parent–child dyads with ADHD. J. Child Psychol. Psychiatry 2007, 48, 899–913. [Google Scholar] [CrossRef]
- Fenollar Cortés, J.; Servera, M.; Becker, S.P.; Burns, G.L. External Validity of ADHD iInattention and Sluggish Cognitive Tempo Dimensions in Spanish Children with ADHD. J. Atten. Disord. 2014, 21, 655–666. [Google Scholar] [CrossRef]
- Tirapu, J.; Ruiz-García, B.M.; Luna, P.; Hernáez, P. Tempo Cognitivo Lento: Una revisión actualizada. Rev. Neurol. 2015, 61, 323–331. [Google Scholar] [CrossRef]
- Becker, S.P.; Barkley, R.A. Sluggish Cognitive Tempo. In Oxford Textbook of Attention Deficit Hyperactivity Disorder, 1st ed.; Banaschewski, T., Coghill, D., Zuddas, A., Eds.; Oxford University Press: Oxford, UK, 2018. [Google Scholar]
- Volk, H.E.; Todorov, A.A.; Hay, D.A.; Todd, R.D. Simple identification of complex ADHD subtypes using current symptom counts. J. Am. Acad. Child Psychiatry 2009, 48, 441–450. [Google Scholar] [CrossRef] [PubMed]
- Fassbender, C.; Krafft, C.E.; Schweitzer, J.B. Differentiating SCT and inattentive symptoms in ADHD using fMRI measures of cognitive control. Neuroimage Clin. 2015, 8, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Barkley, R.A. Distinguishing Sluggish Cognitive Tempo from ADHD in Children and Adolescents: Executive Functioning, Impairment, and Comorbidity. J. Clin. Child Adolesc. Psychol. 2013, 42, 161–173. [Google Scholar] [CrossRef]
- Becker, S.P.; Langberg, J.M. Sluggish Cognitive Tempo among young adolescents with ADHD: Relations to mental health, academic, and social functioning. J. Atten. Disord. 2013, 17, 681–689. [Google Scholar] [CrossRef]
- Becker, S.P.; Luebbe, A.M.; Fite, P.J.; Stoppelbein, L.; Greening, L. Sluggish cognitive tempo in psychiatrically hospitalized children: Factor structure and relations to internalizing symptoms, social problems, and observed behavioral dysregulation. J. Abnorm. Child Psychol. 2014, 42, 49–62. [Google Scholar] [CrossRef]
- Marshall, S.A.; Evans, S.W.; Eiraldi, R.B.; Becker, S.P.; Power, T.J. Social and academic impairment in youth with ADHD, predominately inattentive type and Sluggish Cognitive Tempo. J. Abnorm. Child Psychol. 2014, 42, 77–90. [Google Scholar] [CrossRef]
- Bauermeister, J.J. Tempo cognitivo lento: Un constructo controvertido en evolución. Rev. Mex. Investig. Psicol. 2016, 8, 163–174. [Google Scholar]
- Servera, M.; Sáez, B.; Burns, G.L.; Becker, S.P. Clinical differentiation of Sluggish Cognitive Tempo and Attention-Deficit/Hyperactivity Disorder in children. J. Abnorm. Psychol. 2018, 127, 818–829. [Google Scholar] [CrossRef]
- Bauermeister, J.J.; Barkley, R.A.; Bauermeister, J.A.; Martínez, J.V.; McBurnett, K. Validity of the Sluggish Cognitive Tempo, inattention, and hyperactivity symptom dimensions: Neuropsychological and psychosocial correlates. J. Abnorm. Child Psychol. 2012, 40, 683–697. [Google Scholar] [CrossRef]
- Jarrett, M.A.; Rapport, H.F.; Rondon, A.T.; Becker, S.P. ADHD dimensions and Sluggish Cognitive Tempo symptoms in relation to self-report and laboratory measures of neuropsychological functioning in college students. J. Atten. Disord. 2014, 21, 673–683. [Google Scholar] [CrossRef]
- Lahey, B.B.; Applegate, B.; Waldman, I.D.; Loft, J.D.; Hankin, B.L.; Rick, J. The structure of child and adolescent psychopathology: Generating new hypotheses. J. Abnorm. Psychol. 2004, 113, 358–385. [Google Scholar] [CrossRef]
- Becker, S.P.; Langberg, J.M. Attention-Deficit/Hyperactivity Disorder and Sluggish Cognitive Tempo dimensions in relation to Executive Functioning in adolescents with ADHD. Child Psychiatry Hum. Dev. 2014, 45, 1–11. [Google Scholar] [CrossRef]
- Araujo, E.A.; Jané, M.C.; Bonillo, A.; Arrufat, F.J.; Serra, R. Executive Functioning in children and adolescents with symptoms of Sluggish Cognitive Tempo and ADHD. J. Atten. Disord. 2015, 19, 507–514. [Google Scholar] [CrossRef]
- Sergeant, J.A.; Geurts, H.; Oosterlaan, J. How specific is a deficit of Executive Functioning for Attention-Deficit/Hyperactivity Disorder? Behav. Brain Res. 2002, 130, 3–28. [Google Scholar] [CrossRef]
- Sonuga-Barke, E.J.; Dalen, L.; Daley, D.; Remington, B. Are planning, working memory, and inhibition associated with individual differences in preschool ADHD symptoms? Dev. Neuropsychol. 2002, 21, 255–272. [Google Scholar] [CrossRef]
- Ptacek, R.; Weissenberger, S.; Braaten, E.; Klicperova-Baker, M.; Goetz, M.; Raboch, J.; Vnukova, M.; Stefano, G.B. Clinical implications of the perception of time in Attention Deficit Hyperactivity Disorder (ADHD): A review. Med. Sci. Monit. 2019, 25, 3918–3924. [Google Scholar] [CrossRef]
- Shanahan, M.A.; Pennington, B.F.; Yerys, B.E.; Scott, A.; Boada, R.; Willcutt, E.G.; Olson, R.K.; DeFries, J.C. Processing speed deficits in Attention Deficit/Hyperactivity Disorder and reading disability. J. Abnorm. Child Psychol. 2006, 34, 584–601. [Google Scholar] [CrossRef]
- Willcutt, E.G.; Sonuga-Barke, E.J.; Nigg, J.T.; Sergeant, J.A. Recent developments in neuropsychological models of childhood psychiatric disorders. Adv. Biol. Psychiatry 2008, 24, 195–226. [Google Scholar] [CrossRef]
- Goth-Owens, T.L.; Martinez-Torteya, C.; Martel, M.M.; Nigg, J.T. Processing speed weakness in children and adolescents with non-hyperactive but inattentive ADHD (ADD). Child Neuropsychol. 2010, 16, 577–591. [Google Scholar] [CrossRef]
- Wåhlstedt, C.; Bohlin, G. DSM-IV-defined inattention and Sluggish Cognitive Tempo: Independent and interactive relations to neuropsychological factors and comorbidity. Child Neuropsychol. 2010, 16, 350–365. [Google Scholar] [CrossRef]
- Willcutt, E.G.; Chhabildas, N.; Kinnear, M.; DeFries, J.C.; Olson, R.K.; Leopold, D.R.; Keenan, J.M.; Pennington, B.F. The internal and external validity of Sluggish Cognitive Tempo and its relation with DSM–IV ADHD. J. Abnorm. Child Psychol. 2014, 42, 21–35. [Google Scholar] [CrossRef]
- Jacobson, L.A.; Geist, M.; Mahone, E.M. Sluggish Cognitive Tempo, processing speed, and internalizing symptoms: The moderating effect of age. J. Abnorm. Child Psychol. 2018, 46, 127–135. [Google Scholar] [CrossRef]
- Skirbekk, B.; Hansen, B.H.; Oerbeck, B.; Kristensen, H. The relationship between Sluggish Cognitive Tempo, subtypes of Attention-Deficit/Hyperactivity Disorder, and anxiety disorders. J. Abnorm. Child Psychol. 2011, 39, 513–525. [Google Scholar] [CrossRef]
- Wood, W.L.; Potts, H.E.; Lewandowski, L.J.; Lovett, B.J. Sluggish Cognitive Tempo and speed of performance. J. Atten. Disord. 2017, 21, 684–690. [Google Scholar] [CrossRef]
- Cook, N.E.; Braaten, E.B.; Vuijk, P.J.; Lee, B.A.; Samkavitz, A.R.; Doyle, A.E.; Surman, C.B. Slow processing speed and Sluggish Cognitive Tempo in pediatric Attention-Deficit/Hyperactivity Disorder: Evidence for differentiation of functional correlates. Child Psychiatry Hum. Dev. 2019, 50, 1049–1057. [Google Scholar] [CrossRef]
- Brocki, K.C.; Eninger, L.; Thorell, L.B.; Bohlin, G. Interrelations between Executive Function and symptoms of hyperactivity/impulsivity and inattention in preschoolers: A two year longitudinal study. J. Abnorm. Child Psychol. 2010, 38, 163–171. [Google Scholar] [CrossRef]
- Langberg, J.M.; Becker, S.P.; Dvorsky, M.R. The association between Sluggish Cognitive Tempo and academic functioning in youth with Attention-Deficit/Hyperactivity Disorder (ADHD). J. Abnorm. Child Psychol. 2014, 42, 91–103. [Google Scholar] [CrossRef] [PubMed]
- Becker, S.P.; Luebbe, A.M.; Langberg, J.M. Attention-Deficit/Hyperactivity Disorder dimensions and Sluggish Cognitive Tempo symptoms in relation to college students’ sleep functioning. Child Psychiatry Hum. Dev. 2014, 45, 675–685. [Google Scholar] [CrossRef] [PubMed]
- Hurtig, T.; Ebeling, H.; Taanila, A.; Miettunen, J.; Smalley, S.L.; McGought, J.J.; Loo, S.K.; Järvelin, M.-R.; Moilanen, I.K. ADHD symptoms and subtypes: Relationship between childhood and adolescent symptoms. J. Am. Acad. Child Adolesc. Psychiatry 2007, 46, 1605–1613. [Google Scholar] [CrossRef] [PubMed]
- Burns, G.L.; Becker, S.P. Sluggish Cognitive Tempo and ADHD symptoms in a nationally representative sample of US children: Differentiation using categorical and dimensional approaches. J. Clin. Child Adolesc. Psychol. 2021, 50, 267–280. [Google Scholar] [CrossRef]
- Garner, A.A.; Marceaux, J.C.; Mrug, S.; Patterson, C.; Hodgens, B. Dimensions and correlates of Attention Deficit/Hyperactivity Disorder and Sluggish Cognitive Tempo. J. Abnorm. Child Psychol. 2010, 38, 1097–1107. [Google Scholar] [CrossRef]
- Baytunca, M.B.; Inci, S.B.; Ipci, M.; Kardas, B.; Bolat, G.U.; Ercan, E.S. The neurocognitive nature of children with ADHD comorbid Sluggish Cognitive Tempo: Might SCT be a disorder of vigilance? Psychiatry Res. 2018, 270, 967–973. [Google Scholar] [CrossRef]
- Becker, S.P.; Leopold, D.R.; Burns, G.L.; Jarrett, M.A.; Langberg, J.M.; Marshall, S.A.; McBurnett, K.; Waschbusch, D.; Willcutt, E.G. The internal, external, and diagnostic validity of sluggish cognitive tempo: A meta-analysis and critical review. J. Am. Acad. Child Adolesc. Psychiatry 2016, 55, 163–178. [Google Scholar] [CrossRef]
- Reeves, C.B.; Palmer, S.; Gross, A.M.; Simonian, S.J.; Taylor, L.; Willingham, E.; Mulhern, R.K. Brief report: Sluggish Cognitive Tempo among pediatric survivors of acute lymphoblastic leukemia. J. Pediatr. Psychol. 2010, 32, 1050–1054. [Google Scholar] [CrossRef]
- Conde, C.; Gómez, A.F.; Melero, R.; Narbona, N.; Onandia-hinchado, I.; Rodríguez-Melchor, G.; Rodríguez-Ortíz, P. Guía para la Evaluación Neuropsicológica del Trastorno por Déficit de Atención e Hiperactividad, 1st ed.; Consorcio de Neuropsicología: Madrid, Spain, 2021; ISBN 978-84-09-29318-6. [Google Scholar]
- Kofler, M.J.; Irwin, L.N.; Sarver, D.E.; Fosco, W.D.; Miller, C.E.; Spiegel, J.A.; Becker, S.P. What cognitive processes are “sluggish” in Sluggish Cognitive Tempo? J. Consult. Clin. Psychol. 2019, 87, 1030–1042. [Google Scholar] [CrossRef]
- Hartman, C.A.; Willcutt, E.G.; Rhee, S.H.; Pennington, B.F. The relation between Sluggish Cognitive Tempo and DSM-IV ADHD. J. Abnorm. Child Psychol. 2004, 32, 491–503. [Google Scholar] [CrossRef]
- Mikami, A.Y.; Huang-Pollock, C.L.; Pfiffner, L.J.; McBurnett, K.; Hangai, D. Social skills differences among Attention-Deficit/Hyperactivity Disorder types in a chat room assessment task. J. Abnorm. Child Psychol. 2007, 35, 509–521. [Google Scholar] [CrossRef]
- Willard, V.W.; Hardy, K.K.; Allen, T.M.; Hwang, E.I.; Gururangan, S.; Hostetter, S.A.; Bonner, M.J. Sluggish Cognitive Tempo in survivors of pediatric brain tumors. Neuro-Oncology 2013, 114, 71–78. [Google Scholar] [CrossRef]
- Derefinko, K.J.; Adams, Z.W.; Milich, R.; Fillmore, M.T.; Lorch, E.P.; Lynam, D.R. Response style differences in the inattentive and combined subtypes of Attention-Deficit/Hyperactivity Disorder. J. Abnorm. Child Psychol. 2008, 36, 745–758. [Google Scholar] [CrossRef][Green Version]
- Kaiser, M.L.; Schoemaker, M.M.; Albaret, J.M.; Geuze, R.H. What is the evidence of impaired motor skills and motor control among children with Attention Deficit Hyperactivity Disorder (ADHD)? Systematic review of the literature. Res. Dev. Disabil. 2015, 36, 338–357. [Google Scholar] [CrossRef] [PubMed]
- Goulardins, J.B.; Marques, J.C.; De Oliveira, J.A. Attention Deficit Hyperactivity Disorder and motor impairment: A critical review. Percept. Mot. Ski. 2017, 124, 425–440. [Google Scholar] [CrossRef] [PubMed]
- Fredrick, J.W.; Becker, S.P. Sluggish Cognitive Tempo symptoms, but not ADHD or internalizing symptoms, are uniquely related to self-reported mind-wandering in adolescents with ADHD. J. Atten. Disord. 2020, 25, 1605–1611. [Google Scholar] [CrossRef] [PubMed]
- Becker, S.P.; Barkley, R.A. Field of daydreams? Integrating mind wandering in the study of Sluggish Cognitive Tempo and ADHD. JCPP Adv. 2021, 1, e12002. [Google Scholar] [CrossRef]
- Graziano, P.A.; Garcia, A. Attention-Deficit Hyperactivity Disorder and children’s emotion dysregulation: A meta-analysis. Clin. Psychol. Rev. 2016, 46, 106–123. [Google Scholar] [CrossRef] [PubMed]
- Smith, Z.R.; Langberg, J.M.; Cusick, C.N.; Green, C.D.; Becker, S.P. Academic motivation deficits in adolescents with ADHD and associations with academic functioning. J. Abnorm. Child Psychol. 2020, 48, 237–249. [Google Scholar] [CrossRef] [PubMed]
- Flannery, A.J.; Becker, S.P.; Luebbe, A.M. Does emotion dysregulation mediate the association between Sluggish Cognitive Tempo and college students’ social impairment? J. Atten. Disord. 2016, 20, 802–812. [Google Scholar] [CrossRef] [PubMed]
- Becker, S.P.; Fite, P.J.; Garner, A.A.; Greening, L.; Stoppelbein, L.; Luebbe, A.M. Reward and punishment sensitivity are differentially associated with ADHD and Sluggish Cognitive Tempo symptoms in children. J. Res. Pers. 2013, 47, 719–727. [Google Scholar] [CrossRef]
- Penny, A.M.; Waschbusch, D.A.; Klein, R.M.; Corkum, P.; Eskes, G. Developing a measure of Sluggish Cognitive Tempo for children: Content validity, factor structure, and reliability. Psychol. Assess. 2009, 21, 380–389. [Google Scholar] [CrossRef]
- Serrano, J. Aplicación On-line y Tratamiento Informático de Cuestionarios. Rev. Esp. Pedagog. 2012, 70, 61–75. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Capdevila-Brophy, C.; Artigas-Pallarés, J.; Obiols-Llandrich, J.E. Tempo Cognitivo Lento: ¿Síntomas del Trastorno de Déficit de Atención/Hiperactividad predominantemente desatento o una nueva entidad clínica. Rev. Neurol. 2006, 42, 127–134. [Google Scholar] [CrossRef]
- Lahey, B.B.; Schaughency, E.A.; Frame, C.L.; Strauss, C.C. Teacher ratings of attention problems in children experimentally classified as exhibiting attention deficit disorder with and without hyperactivity. J. Am. Acad. Child Adolesc. Psychiatry 1985, 24, 613–616. [Google Scholar] [CrossRef]
- Barkley, R.A.; Fischer, M.; Edelbrock, C.S.; Smallish, L. The adolescent outcome of hyperactive children diagnosed by research criteria: I. An 8-year prospective follow-up study. J. Am. Acad. Child Adolesc. Psychiatry 1990, 29, 546–557. [Google Scholar] [CrossRef]
- Becker, S.P.; Marshall, S.A.; McBurnett, K. Sluggish Cognitive Tempo in abnormal child psychology: An historical overview and introduction to the special section. J. Abnorm. Child Psychol. 2014, 42, 1–6. [Google Scholar] [CrossRef]
- Yung, T.W.; Lai, C.Y.; Chan, J.Y.; Ng, S.S.; Chan, C.C. Neuro-physiological correlates of Sluggish Cognitive Tempo (SCT) symptoms in school-aged children. Eur. Child Adolesc. Psychiatry 2020, 29, 315–326. [Google Scholar] [CrossRef]



| Sex | Age Group | Total | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 6–8 Years | 9–11 Years | 12–14 Years | 15–18 Years | |||||||
| n | % | n | % | n | % | n | % | n | % | |
| Male | 127 | 14.6 | 136 | 15.7 | 97 | 11.2 | 60 | 6.9 | 420 | 48.4 |
| Female | 148 | 17.1 | 137 | 15.8 | 104 | 12.0 | 58 | 6.7 | 447 | 51.6 |
| Total | 275 | 31.7 | 273 | 31.5 | 201 | 23.2 | 118 | 13.6 | 867 | 100 |
| Sex | Age Group | Total | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 6–8 Years | 9–11 Years | 12–14 Years | 15–18 Years | |||||||
| n | % | n | % | n | % | n | % | n | % | |
| Male | 17 | 13.7 | 29 | 23.4 | 23 | 18.5 | 20 | 16.1 | 89 | 71.8 |
| Female | 7 | 5.6 | 14 | 11.3 | 9 | 7.3 | 5 | 4.0 | 35 | 28.2 |
| Total | 24 | 19.4 | 43 | 34.7 | 32 | 25.8 | 25 | 20.2 | 124 | 100 |
| Sex | Age Group | Total | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 6–8 Years | 9–11 Years | 12–14 Years | 15–18 Years | |||||||
| n | % | n | % | n | % | n | % | n | % | |
| Male | 10 | 17.2 | 13 | 22.4 | 16 | 27.6 | 11 | 19 | 50 | 86.2 |
| Female | 2 | 3.4 | 3 | 5.2 | 2 | 3.4 | 1 | 1.7 | 8 | 13.8 |
| Total | 12 | 20.7 | 16 | 27.6 | 18 | 31.0 | 12 | 20.7 | 58 | 100 |
| Subsamples | Subscales | Total Scale | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Time | Problem | Inhibition | Motivation | Emotion | ||||||||
| M | SD | M | SD | M | SD | M | SD | M | SD | M | SD | |
| Non-pathologic | 9.3 | 3.1 | 7 | 2.8 | 8.9 | 3.1 | 8.8 | 3.2 | 8.4 | 2.9 | 42.4 | 11.9 |
| ADHD | 13 | 2.5 | 11.2 | 3.5 | 13.4 | 2.6 | 12.4 | 2.7 | 12 | 2.9 | 62.1 | 9.9 |
| SCT | 11.9 | 2.9 | 10.1 | 3.4 | 10.9 | 2.9 | 10.6 | 2.9 | 9.4 | 3 | 52.9 | 10.2 |
| Compared Subsamples | Subscale | B | S.E. | Wald | p | OR | C.I. (95%) |
|---|---|---|---|---|---|---|---|
| Non-pathologicand ADHD | Time | 0.14 | 0.050 | 7.488 | 0.006 | 1.15 | 1.04–1.26 |
| Problem | 0.19 | 0.038 | 24.156 | <0.001 | 1.21 | 1.12–1.30 | |
| Inhibition | 0.26 | 0.053 | 24.440 | <0.001 | 1.30 | 1.17–1.44 | |
| Emotion | 0.12 | 0.053 | 5.604 | 0.018 | 1.13 | 1.02–1.26 | |
| Constant | −9.45 | 0.704 | 180.142 | <0.001 | 0.001 | ||
| Non-pathologicand SCT | Time | 0.15 | 0.054 | 7.478 | 0.006 | 1.16 | 1.04–1.29 |
| Problem | 0.23 | 0.049 | 22.081 | <0.001 | 1.26 | 1.14–1.38 | |
| Constant | −6.21 | 0.590 | 110.941 | <0.001 | 0.002 | ||
| ADHD and SCT | Inhibition | 0.20 | 0.08 | 6.960 | 0.008 | 1.22 | 1.05–1.42 |
| Emotion | 0.16 | 0.07 | 4.976 | 0.026 | 1.18 | 1.02–1.37 | |
| Constant | −3.52 | 0.82 | 18.31 | <0.001 | 0.030 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Collado-Valero, J.; Navarro-Soria, I.; Delgado-Domenech, B.; Real-Fernández, M.; Costa-López, B.; Mazón-Esquiva, I.; Lavigne-Cerván, R. ADHD and Sluggish Cognitive Tempo: Comparing Executive Functioning Response Patterns. Sustainability 2021, 13, 10506. https://doi.org/10.3390/su131910506
Collado-Valero J, Navarro-Soria I, Delgado-Domenech B, Real-Fernández M, Costa-López B, Mazón-Esquiva I, Lavigne-Cerván R. ADHD and Sluggish Cognitive Tempo: Comparing Executive Functioning Response Patterns. Sustainability. 2021; 13(19):10506. https://doi.org/10.3390/su131910506
Chicago/Turabian StyleCollado-Valero, Joshua, Ignasi Navarro-Soria, Beatriz Delgado-Domenech, Marta Real-Fernández, Borja Costa-López, Isabel Mazón-Esquiva, and Rocío Lavigne-Cerván. 2021. "ADHD and Sluggish Cognitive Tempo: Comparing Executive Functioning Response Patterns" Sustainability 13, no. 19: 10506. https://doi.org/10.3390/su131910506
APA StyleCollado-Valero, J., Navarro-Soria, I., Delgado-Domenech, B., Real-Fernández, M., Costa-López, B., Mazón-Esquiva, I., & Lavigne-Cerván, R. (2021). ADHD and Sluggish Cognitive Tempo: Comparing Executive Functioning Response Patterns. Sustainability, 13(19), 10506. https://doi.org/10.3390/su131910506