The previous section has presented the results found using the methodology described in this paper. This section aims to explain what the results implicate, both in general and how the results matter for traffic and urban planners. This section also aims to discuss how the quality of data and the methods for data collection might have affected the results and why that matters for future trials of similar sorts, such as the one presented in this paper.
5.1. The Clustering in General
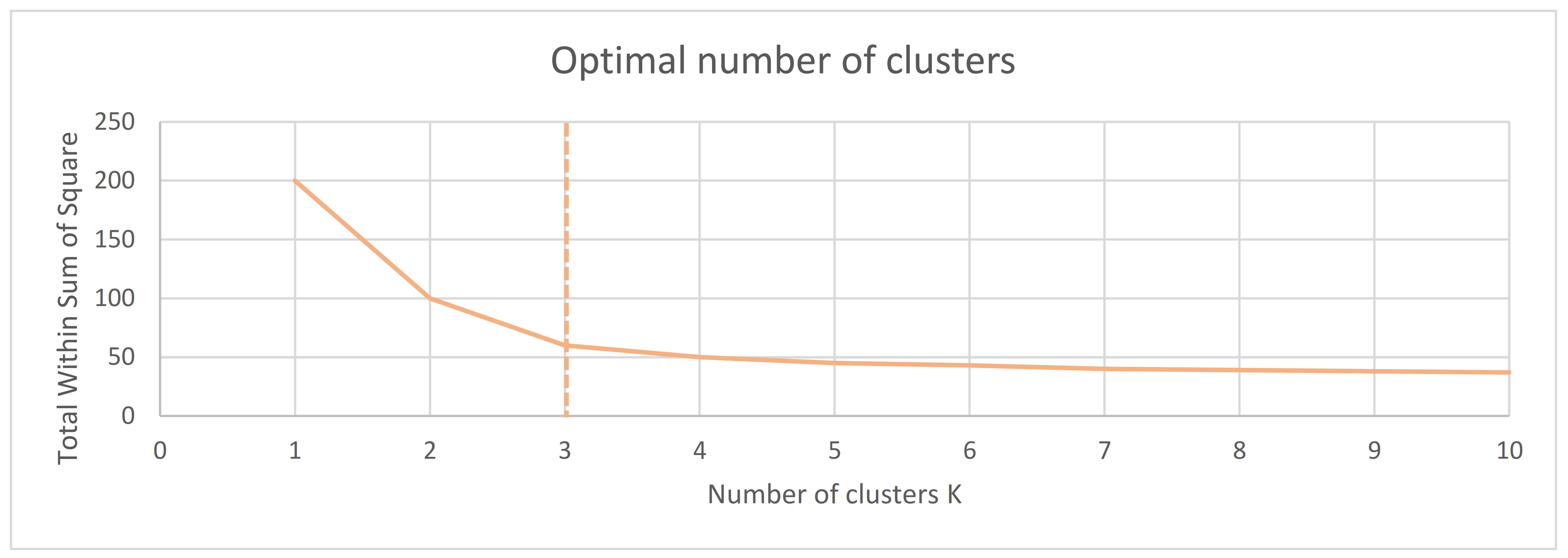
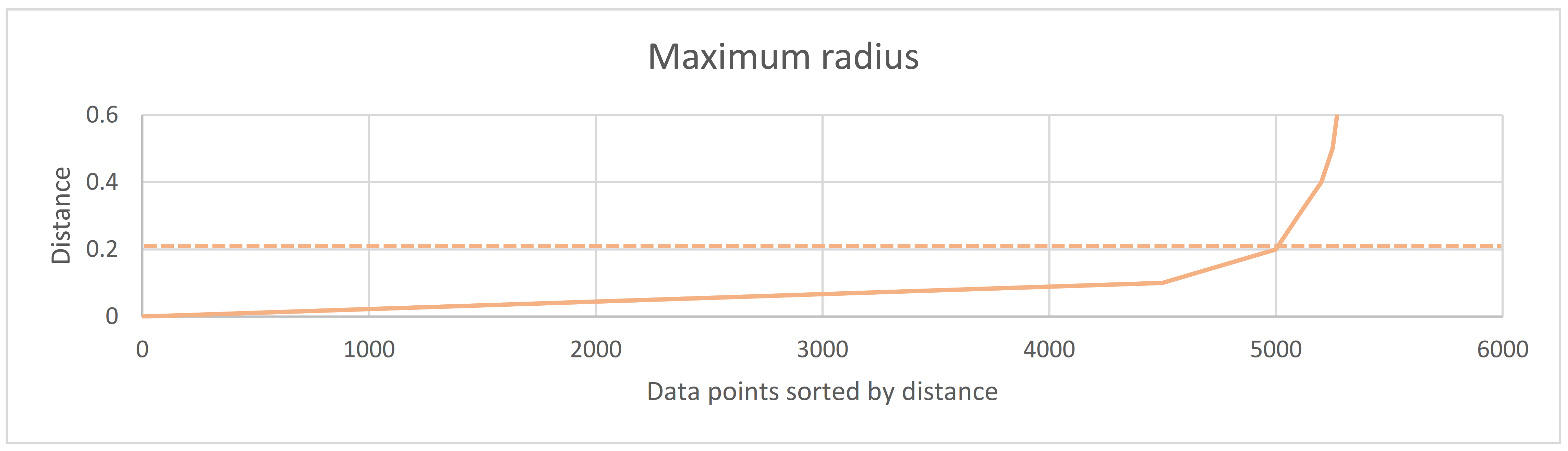
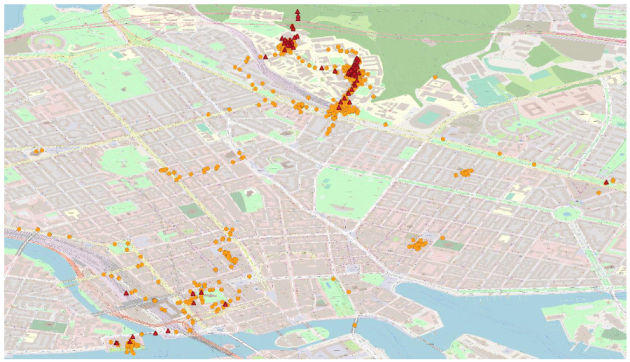
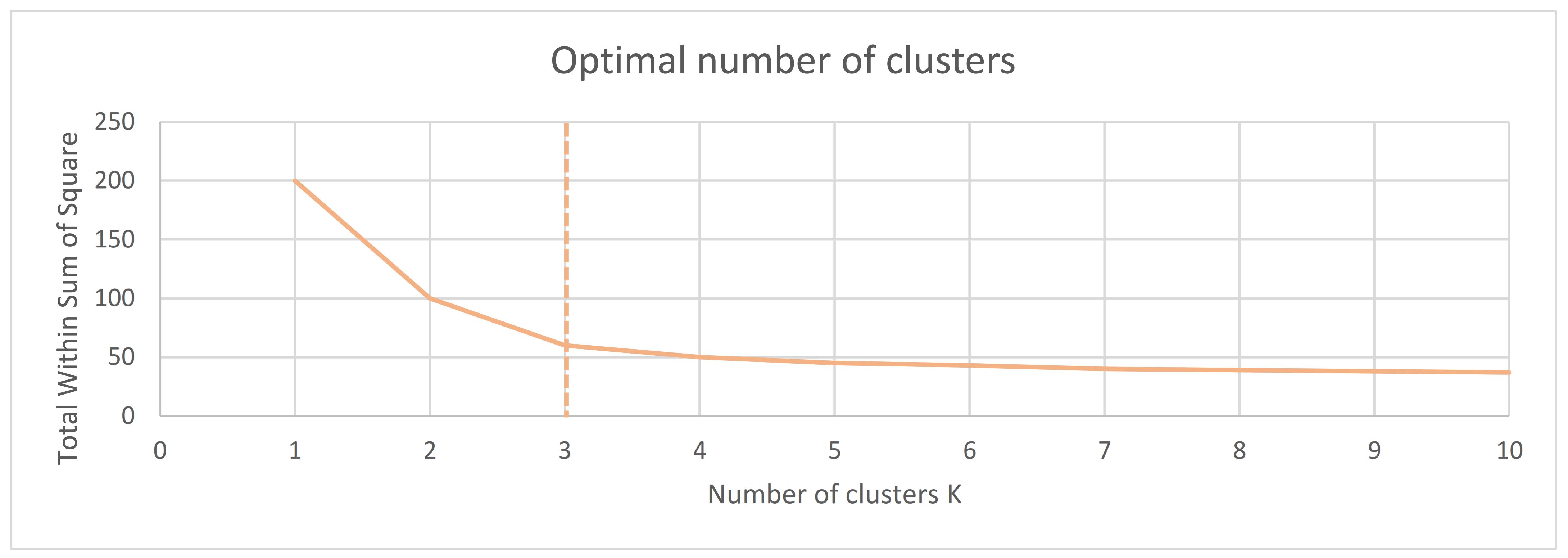
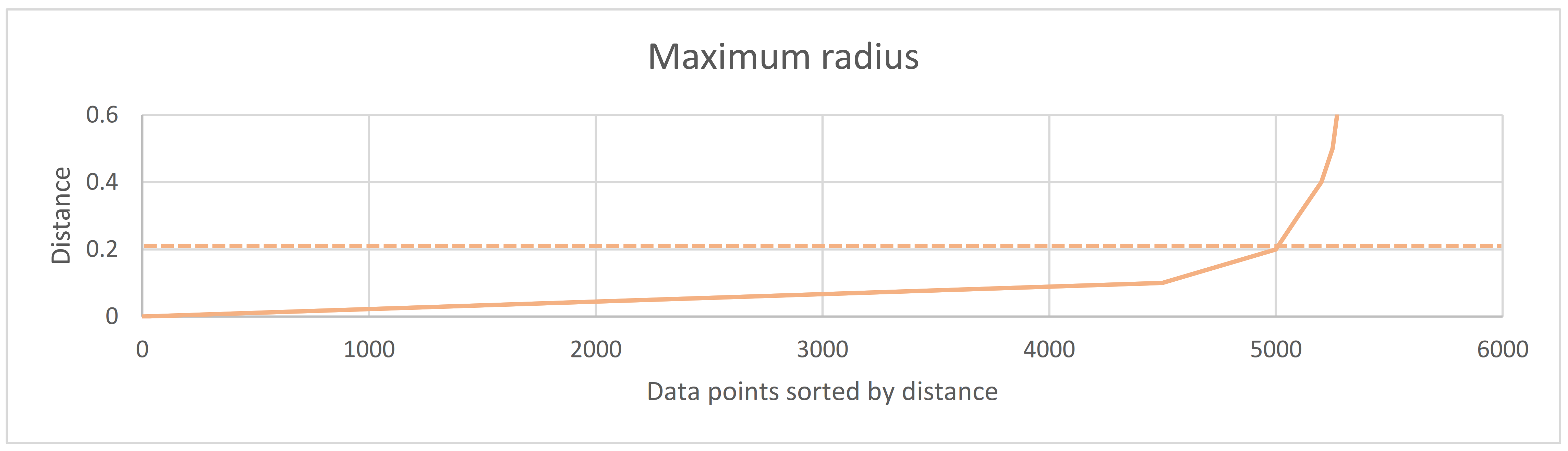
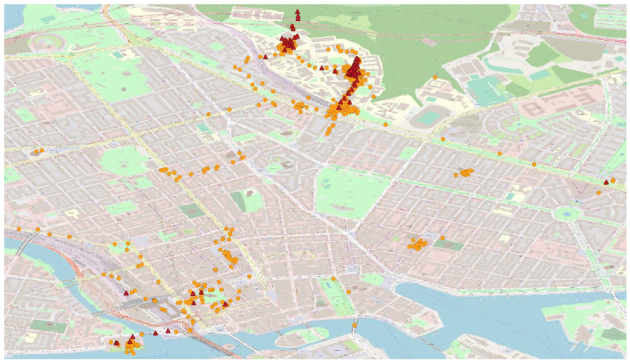
The clustering of data showed that it is possible to find locations and areas where the heart rate is consistent over time, as well as locations and areas where the heart rate deviates. The K-means clustering visualisations indicate that an increased amount of collected data points in an area give more opportunity for peak heart rates to be collected in the same area. This is further confirmed with the density-based clustering, as we can see that the areas with more significant amounts of collected data experience both deviations and regular heart rate. Further data collections should be performed in these areas with added dimensions relating to the level of stress or cognitive load the participant is experiencing. Many factors can affect how the heart rate increases and decreases in a single area, and these factors need to be found and accounted for.
However, the results of the PB-model better describe how the participant was affected and which factors played a role in it. In the following,
Section 5.2, the results of the PB-model will be discussed, and in
Section 5.3, there will be a discussion on the implications of these findings on urban planning.
5.2. The Results of the PB-Model
The results of the PB-model showed how the different variables affected the normalised heart rate. With an adjusted R of 0.516, one could argue that the model fits quite well, given that it is a model for human subjects with a lot of noise, however it can and should be improved in future work.
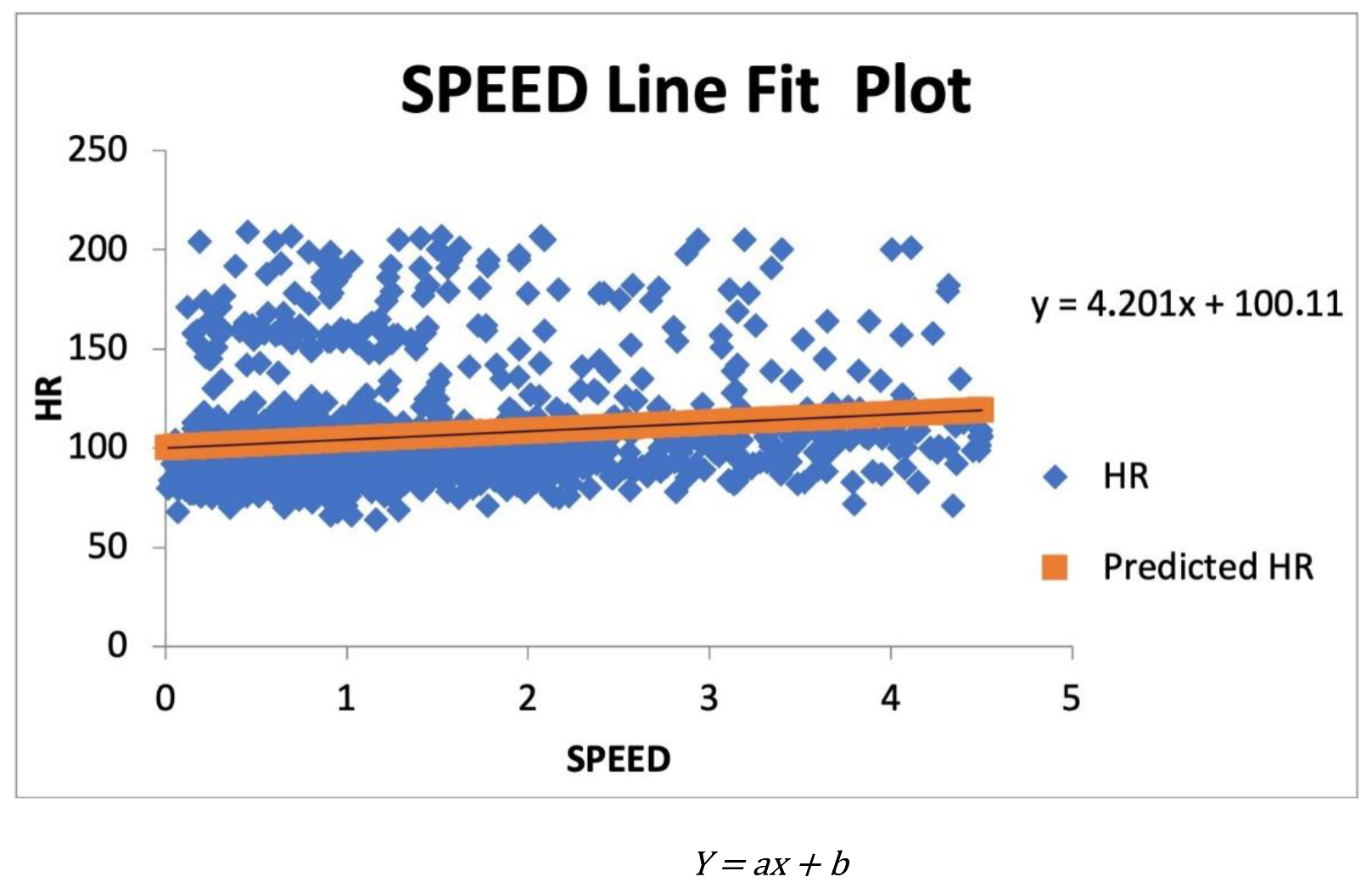
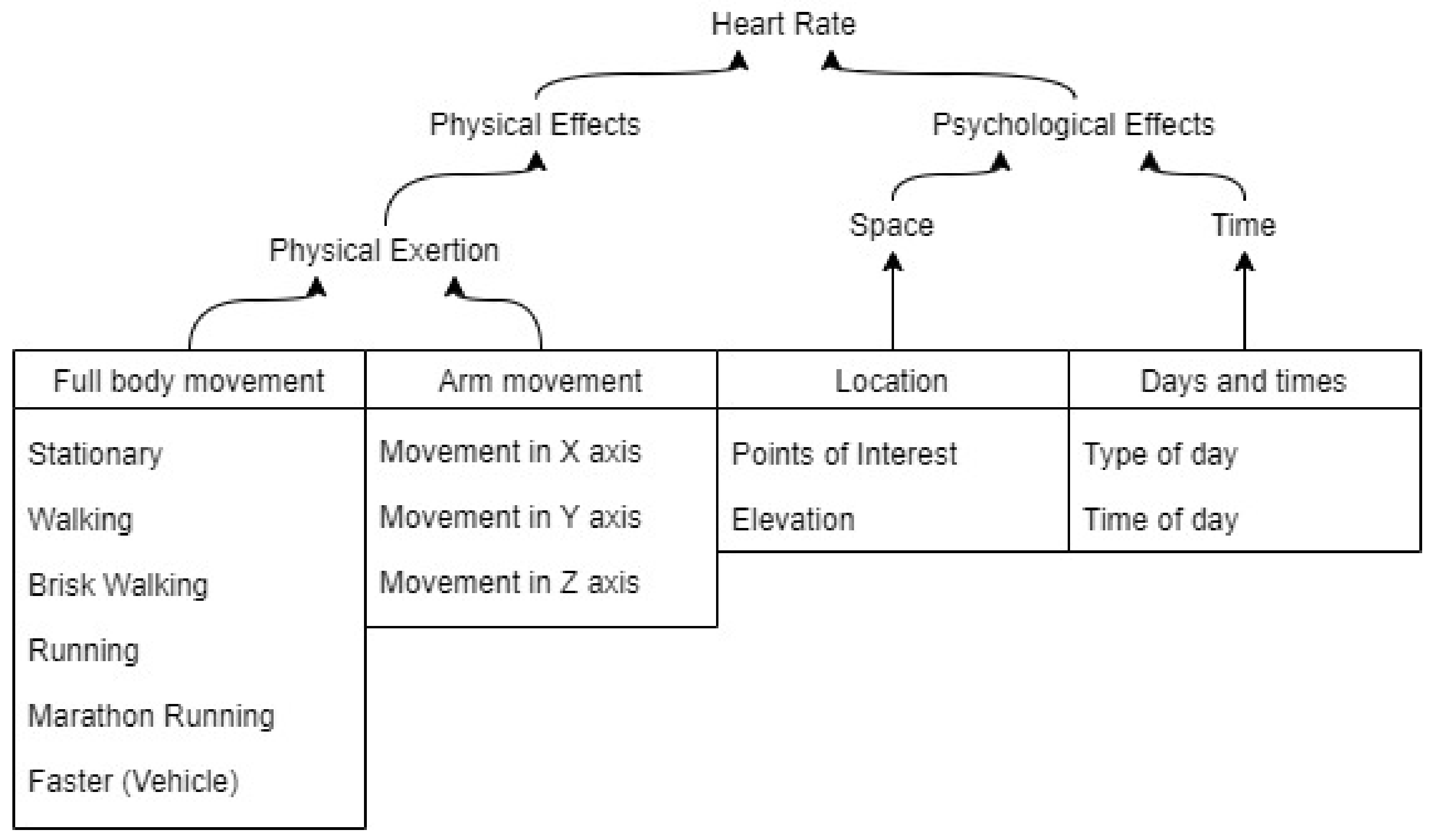
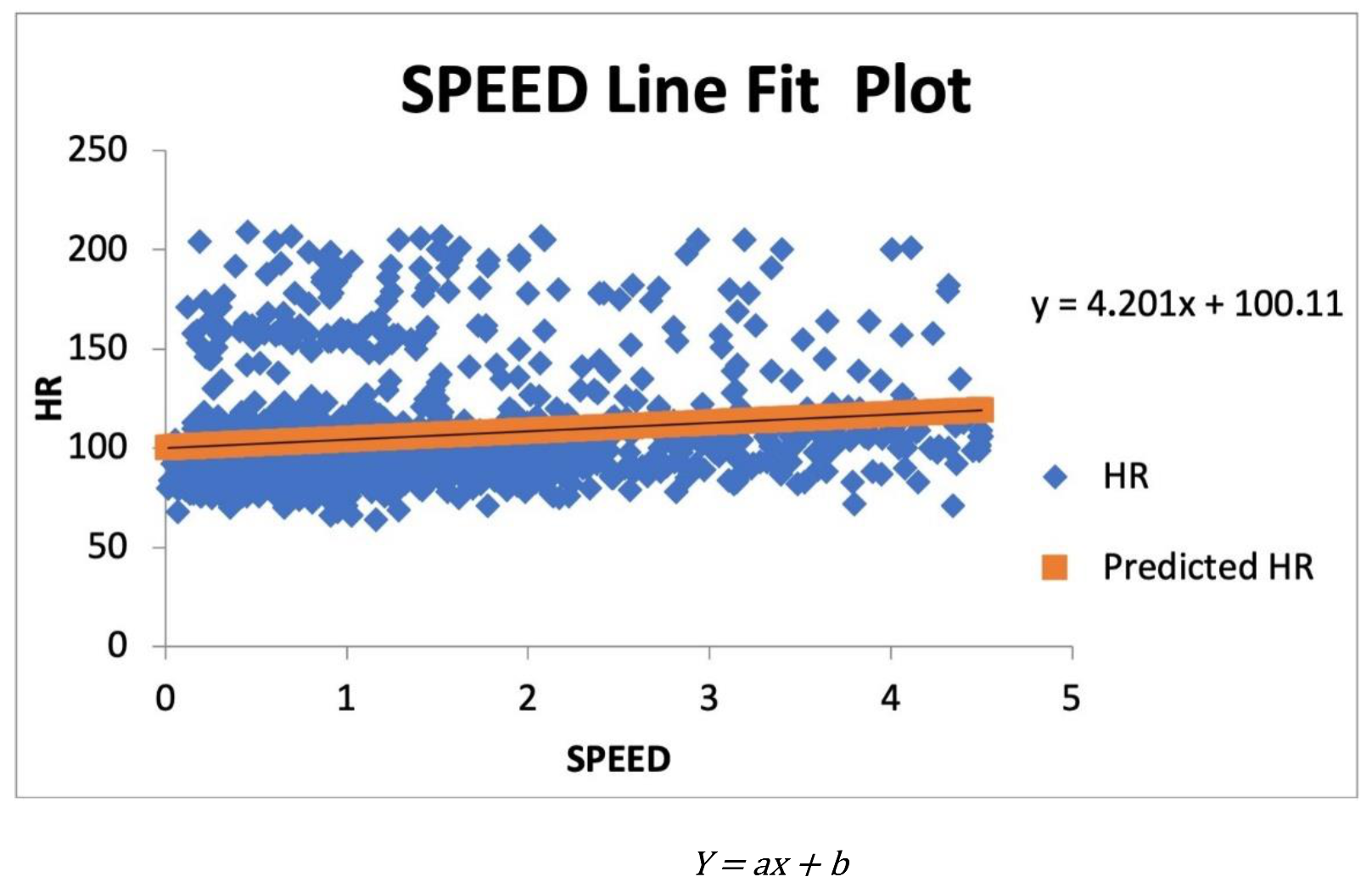
What is interesting to see is that the speed of the person is rather insignificant in the sense that its t-value is within the range for rejecting the hypothesis that it might be affecting the heart rate. For this dataset, that range would be −1.960 to 1.960 for 95% confidence. However, what must be taken into consideration is that these states are only compared to the stationary state and the data consisted of many more data points where the participant was stationary than mobile. It is also interesting to see that the higher speeds are affecting the heart rate negatively, meaning that the faster the participant has travelled, the lower the heart rate has become. By looking at the pattern of the speed coefficients, it is indicative that there seems to be a threshold where this happens. A reason for why it might be like that is, as both Gorny et al. [
18] an Wang et al. [
67] have concluded, that the more a participant moves their body, the less accurate a wrist-worn PPG sensor will be, meaning that if the participant is moving by themselves at high speeds, it might be difficult to read the heart rate with the device used in this study. Another reason might be that once a person has gotten into a vehicle, in theory the person should no longer be affected by the speed itself. However, a person is still susceptible to the changes in speed while in a vehicle and for future iterations of the model, both the difference in speed and acceleration should be included. However, given the control for such factors, the results of this study should show that future work might be able to obtain more accurate readings than previous studies have.
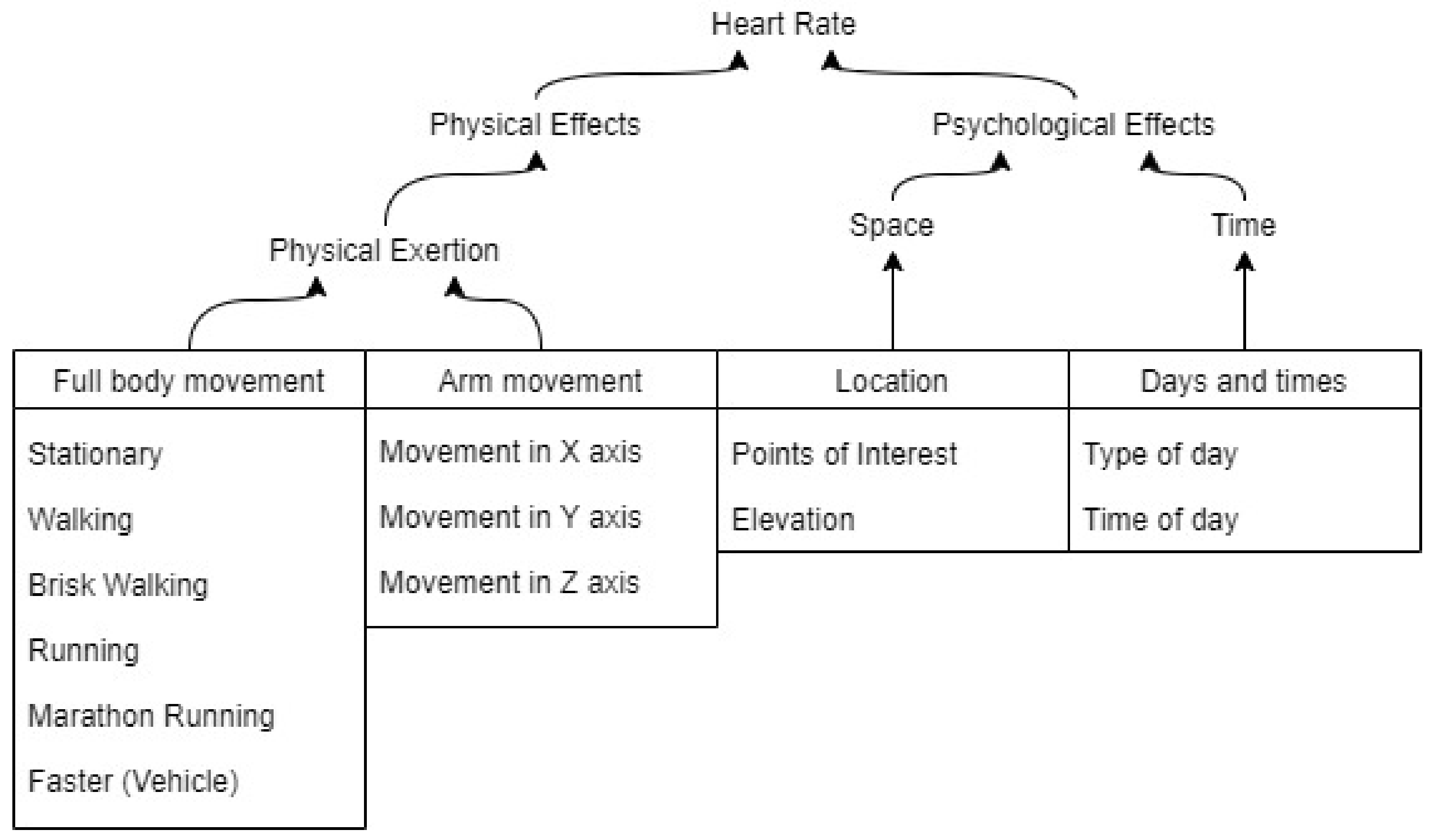
The accelerometer data indicate the gravitational pull on the participant’s device, which could be used as an indicator for the intensity of the activities being conducted. For this data collection, the sample rate was set to one sample per minute, or 0.017 Hz; however, with a higher sample rate, it would not only be possible to better understand how much a person is moving but also what type of activity is being performed if gyroscopic data were added as well. Both the software MERGEN and the PB-model should be updated to include this, as it would give a better indication of how much the activity of the person is influencing the heart rate. With the data collected, however, it is possible to see that the readings are rather significant by looking at their t-values, which might mean that there is more information to be found here.
The significance of the elevation also seems to be rather high. For this iteration of the software, no elevation data were collected with the rest of the data; it was rather gathered by comparing the spatial data to registers of elevation at specific locations. This means that only elevation changes outdoors were accounted for and no elevation changes within a building could be collected. However, the significance of this variable unsurprisingly shows that there is more information to be gathered and explored related to elevation. A variable such as elevation change since the last collected data point would give a better explanation of how the elevation is affecting the person. The absolute values being used now only show that the higher the altitudes, in general, the lower the heart rate of a person, which could be because of thinner air or other reasons.
The Points of Interest (POI) were used to show how a location can affect a person, and both POIs of the model are compared to a third category called “other,” which is neither home nor office. It is interesting to see that the persons heart rate is positively affected by both being located at home and at the office compared to other locations. Naively, this could be interpreted as if the person has an easier time being away from home and the office since the heart rate would be lower, however, that could be since the “other” category contains every other location possible within the realm of the data collection. Therefore, POIs within the “other” category could include locations which could be able to lower the heart rate, such as spas or similar POIs. This means that a broader range of POIs could be useful to find how the heart rate is affected by them. This is particularly interesting for urban planners, as they can choose their POIs as the locations where they will change or have changed the built environment to see whether the impact on the heart rate has increased, lowered, or is the same. More about this will be discussed in
Section 5.3.
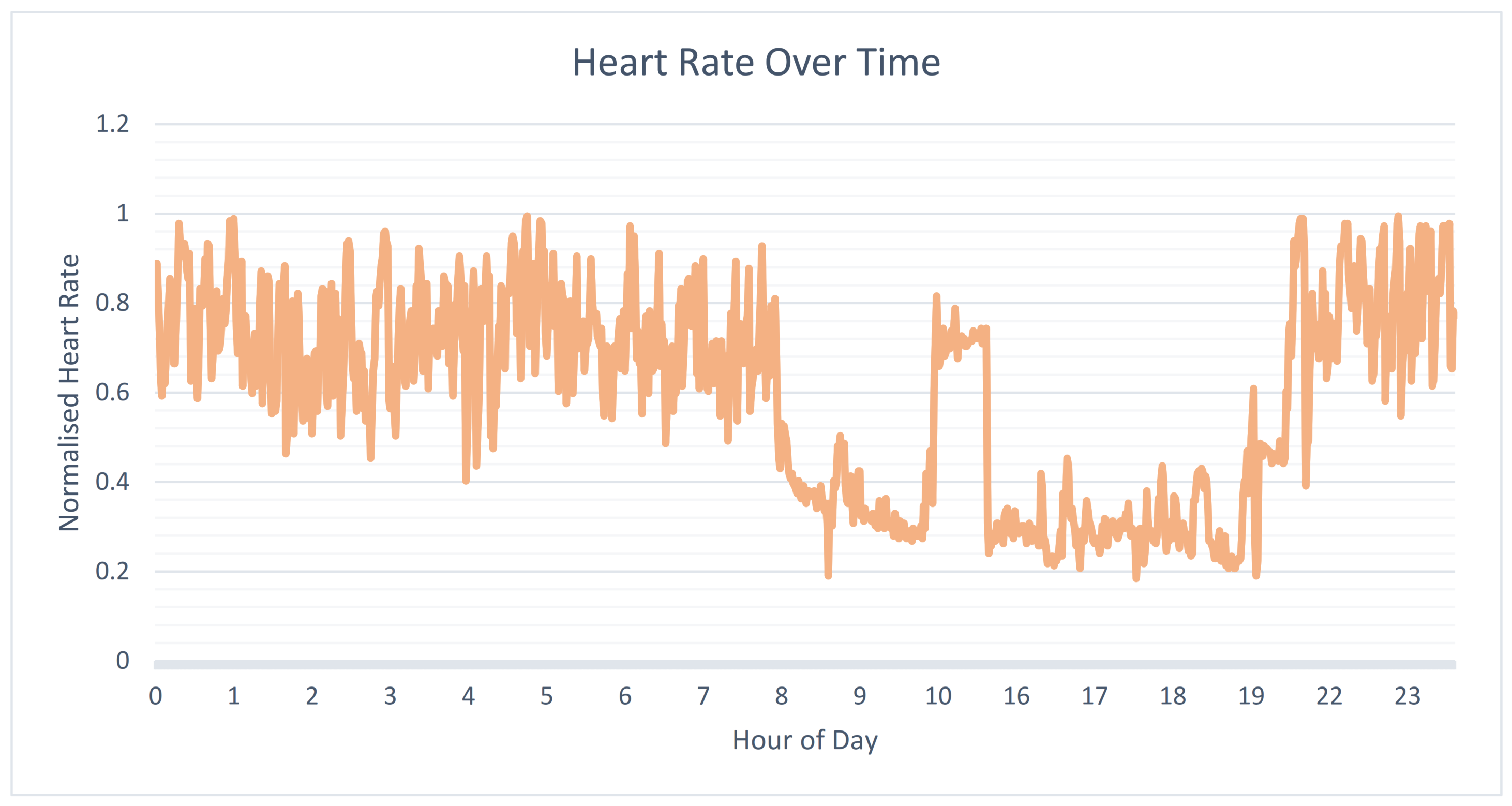
The weekdays and times of day are all significant variables that affect the heart rate of a person. The reason as to why the heart rate would be lower during weekdays than weekends might be because when the person is working at their office, they are less physically active than in their weekends where they might have activities which require more physical activities, such as going for walks or performing different forms of sport.
The interpretations could be further investigated by performing interviews with the participant to see whether or not they might be correct, something which could be implemented in future trials.
5.3. Implications for Urban Planning
With the results found in this trial, the framework can be found useful for traffic and urban planners. By collecting the biometric data at more locations over a longer time, it will be possible to find areas that have had participants experience both regular heart rate patterns and deviations. By analysing these areas and finding the correlation between the activities performed in the area and the heart rate, it will be possible to rule out which factors, such as walking or running, are affecting the person. When finding several areas with the same characteristics, it will then become possible to compare the features of those areas until correlations between said features and the heart rate patterns can be found. This is not unlike the works of Prelipcean et al. [
4] and Allström et al. [
5], to name a few; however, the difference here is that instead of just correlating activities to locations, this type of data can uncover the effects of locations. Building up a data library of such features can then help in planning future areas where the planners want no, or want to encourage, effects from the built environment on the inhabitants or travellers. With the dawn of smart cities, where every citizen can be connected to smart services, the utilisation of such frameworks as the one trialled in this paper will provide additional information on how cities can be planned to be less intrusive on the wellbeing of the inhabitants as the technology becomes available to a broader audience than before.
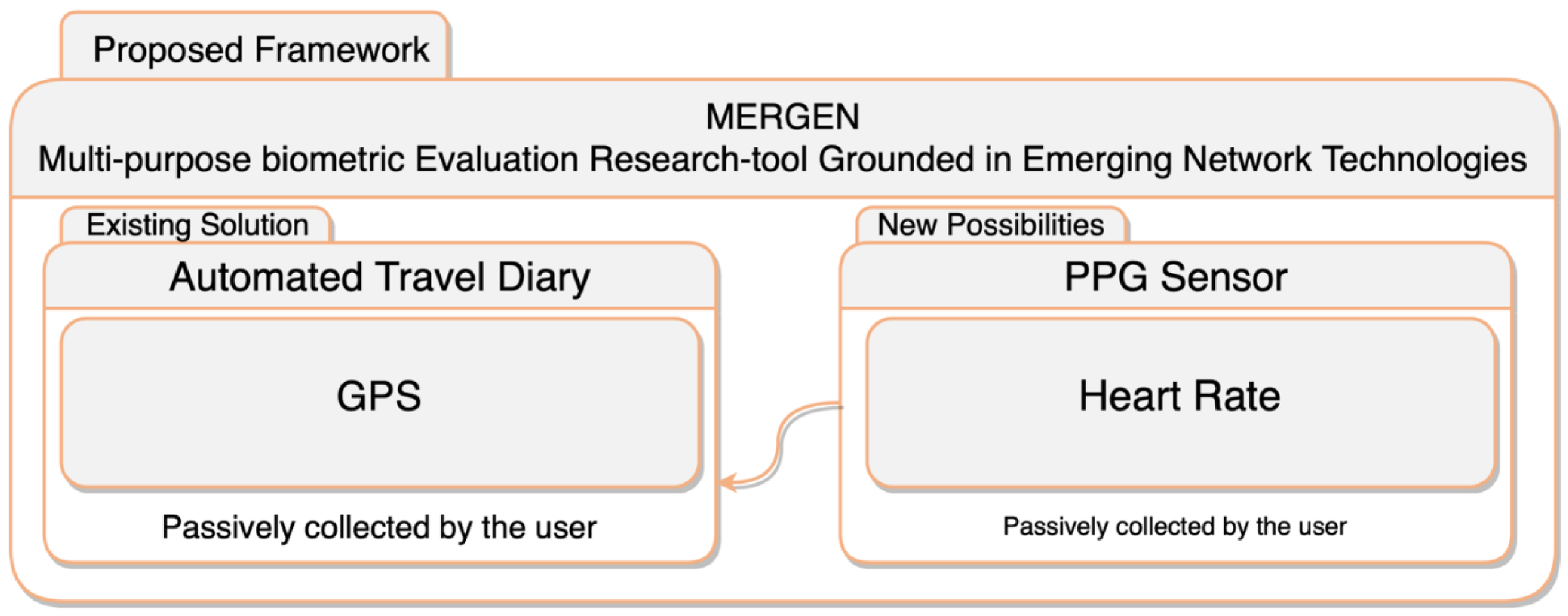
However, the unique selling point which needs to be addressed is the fact that these data are collected directly from the participant without any psychological interpretations handling the data before it is being collected. This is beneficial for several reasons, mainly two, which are: (1) the removal of the human factor by collecting data directly from the source leads to fewer mistakes which could have created inadequate or faulty data, and (2) the removal of the need to interpret questions from surveys also eliminates interpretation errors which could have caused data that could have been either biased or completely faulty. By measuring biometric data and referring to methods for psychophysiological extraction of mental states and conditions [
19,
20,
21,
22,
23,
24,
25], one could reveal more reliable results given that the hardware and software used is of the best quality possible [
68].
5.4. Risks
All the data analysis in this paper has been performed based on the assumption that the data have been collected correctly and that all sensors have been calibrated accordingly during the manufacturing process. That being said, there can, of course, be deviations in the data that are caused by misuse or faulty equipment, and there is no safe way to tell if this has happened. However, all deviations in the data have, for the sake of the data analysis in this trial, been treated as deviations in the sources, meaning that heart rate deviations in the collected data have been treated as ground truth deviations in the participant’s heart rate since, just as Gorny et al. [
18] and Benedetto et al. [
17] conclude, the aggregated data of future studies could be deemed truthful with a large enough group of participants.
The elevation data used in the data analysis had a much lower resolution than the data collected in this trial. By finding the closest value and using that, there might be many data points that share the same elevation data, when in reality the participant has walked uphill and downhill between two data points, which cannot be discovered using the current dataset. That being said, there is, of course, the possibility to redo the analysis with higher resolution data, however there will not be any possibility of collecting ground truth elevation data with the use of the chosen equipment for this trial.
By using time-dependent data collection, it has been made sure that no heart rate changes are missed in a static location; however, depending on the speed of the traveller, both increases and decreases in heart rate while travelling quickly might be missed. For future trials, a fusion of location-based and time-based collection can be used, where the software collects a sample every X meters and Y seconds, whichever comes first.
The lack of demographic data, giving information regarding health background as well as routine data such as diet and exercise programs, makes it harder to draw conclusions on the effects found when performing the analysis on a group. In this study, the data show indications on where and how the participant was affected by external factors, but that is with the assumption that no other factors play a part in affecting the participant.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}