
Connections between Healthy Behaviour, Perception of Olive Oil Health Benefits, and Olive Oil Consumption Motives



Abstract
:1. Introduction
1.1. Olive Oil Consumption Motives
1.2. Olive Oil Health Benefits
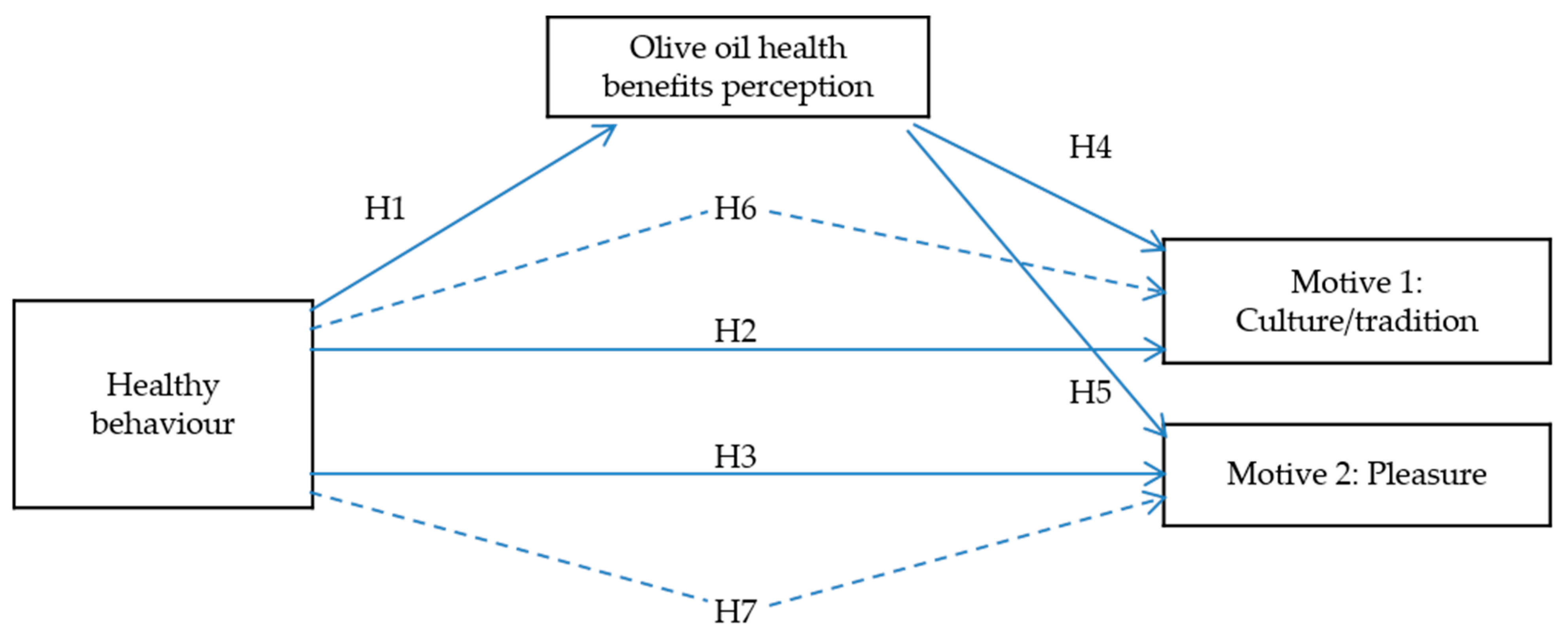
1.3. Perception of Health Benefits and Knowledge of Olive Oil and Healthy Behaviour
2. Materials and Methods
2.1. Data Collection
2.2. Data Analysis and Measurement
3. Results
3.1. Confirmatory Factor Analysis
3.2. Findings of the SEM and Construct Relationships
4. Discussion
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Clodoveo, M.L.; Camposeo, S.; De Gennaro, B.; Pascuzzi, S.; Roselli, L. In the ancient world, virgin olive oil was called “liquid gold” by Homer and “the great healer” by Hippocrates. Why has this mythic image been forgotten? Food Res. Int. 2014, 62, 1062–1068. [Google Scholar] [CrossRef]
- Corallo, A.; Latino, M.E.; Menegoli, M.; Spennato, A. A Survey to Discover Current Food Choice Behaviors. Sustainability 2019, 11, 5041. [Google Scholar] [CrossRef] [Green Version]
- Tourila, H.; Recchia, A. Olive Oil Sensory Science, Chapter Sensory Perception and Other Factors Affecting Consumer Choice of Olive Oil; John Wiley & Sons Ltd.: Hoboken, NJ, USA, 2014. [Google Scholar]
- Moyano, M.J.; Heredia, F.J.; Meléndez-Martínez, A.J. The Color of Olive Oils: The Pigments and Their Likely Health Benefits and Visual and Instrumental Methods of Analysis. Compr. Rev. Food Sci. Food Saf. 2010, 9, 278–291. [Google Scholar] [CrossRef]
- Peršurić, A.S.I. Segmenting Olive Oil Consumers Based on Consumption and Preferences toward Extrinsic, Intrinsic and Sensorial Attributes of Olive Oil. Sustainability 2020, 12, 6379. [Google Scholar] [CrossRef]
- Beauchamp, G.K.; Keast, R.; Morel, D.; Lin, J.; Pika, J.; Han, Q.; Lee, C.-H.; Smith, A.B.; Breslin, P.A.S. Ibuprofen-like activity in extra-virgin olive oil. Nat. Cell Biol. 2005, 437, 45–46. [Google Scholar] [CrossRef] [PubMed]
- Pardo, J.E.; Alvarez-Orti, M.; Araniti, V.; Banza, M.; Rubio, M.; Zied, D.C.; Silvestre, A. Argentinian consumers extra virgin olive oil preference. La Riv. Ital. Delle Sostanze Grasse 2018, 95, 105–110. [Google Scholar]
- Antonialli, F.; Mesquita, D.L.; Valadares, G.C.; De Rezende, D.C.; De Oliveira, A.F. Olive oil consumption: A preliminary study on Brazilian consumers. Br. Food J. 2018, 120, 1412–1429. [Google Scholar] [CrossRef]
- Romo-Muñoz, R.; Romo-Muñoz, F.; Dote-Pardo, J.S.; Troncoso-Sepúlveda, R. Incidence of psychographic variables on purchasing behavior in an emerging olive oil market. Br. Food J. 2018, 120, 2924–2936. [Google Scholar] [CrossRef]
- Martínez, M.G.; Aragonés, Z.; Poole, N. A repositioning strategy for olive oil in the UK market. Agribusiness 2002, 18, 163–180. [Google Scholar] [CrossRef]
- Sandalidou, E.; Baourakis, G.; Siskos, Y. Customers’ perspectives on the quality of organic olive oil in Greece. Br. Food J. 2002, 104, 391–406. [Google Scholar] [CrossRef]
- Krystallis, A.; Ness, M. Consumer preferences or quality foods from a South European Perspective: A conjoint analysis implementation on Greek Olive Oil. Int. Food Agribus. Manag. Rev. 2005, 8, 62–91. [Google Scholar]
- Bernabéu, R.; Díaz, M. Preference for olive oil consumption in the Spanish local market. Span. J. Agric. Res. 2016, 14, e0108. [Google Scholar] [CrossRef] [Green Version]
- Cavallo, C.; Caracciolo, F.; Cicia, G.; Del Giudice, T. Extra-virgin olive oil: Are consumers provided with the sensory quality they want? A hedonic price model with sensory attributes. J. Sci. Food Agric. 2017, 98, 1591–1598. [Google Scholar] [CrossRef]
- Bendinelli, B.; Masala, G.; Saieva, C.; Salvini, S.; Calonico, C.; Sacerdote, C.; Agnoli, C.; Grioni, S.; Frasca, G.; Mattiello, A.; et al. Fruit, vegetables, and olive oil and risk of coronary heart disease in Italian women: The EPICOR Study. Am. J. Clin. Nutr. 2010, 93, 275–283. [Google Scholar] [CrossRef] [Green Version]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.A.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Sup-plemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 379, 1388–1389. [Google Scholar]
- Martinez-Gonzalez, M.A.; Dominguez, L.J.; Delgado-Rodríguez, M. Olive oil consumption and risk of CHD and/or stroke: A meta-analysis of case–control, cohort and intervention studies. Br. J. Nutr. 2014, 112, 248–259. [Google Scholar] [CrossRef] [Green Version]
- Guasch-Ferré, M.; Liu, G.; Li, Y.; Sampson, L.; Manson, J.E.; Salas-Salvadó, J.; Martínez-González, M.A.; Stampfer, M.J.; Willett, W.C.; Sun, Q.; et al. Olive Oil Consumption and Cardiovascular Risk in U.S. Adults. J. Am. Coll. Cardiol. 2020, 75, 1729–1739. [Google Scholar] [CrossRef] [PubMed]
- Perito, M.A.; Sacchetti, G.; Di Mattia, C.D.; Chiodo, E.; Pittia, P.; Saguy, I.; Cohen, E. Buy Local! Familiarity and Preferences for Extra Virgin Olive Oil of Italian Consumers. J. Food Prod. Mark. 2019, 25, 462–477. [Google Scholar] [CrossRef]
- European Comission. Regulation of the European Parliaments and of the Council of 20 December 2006 on nutrition and health claims made on food. Off. J. Eur. Union 2006, 404, 9–25. [Google Scholar]
- Harwood, J.L.; Yaqoob, P. Nutritional and health aspects of olive oil. Eur. J. Lipid Sci. Technol. 2002, 104, 685–697. [Google Scholar] [CrossRef]
- The World Cancer Research Fund Report: Food, Nutrition, and the Prevention of Cancer; A Global Perspective; AICR: Washington, DC, USA, 2007.
- Delgado, C.; Guinard, J.-X. Sensory Properties of Californian and Imported Extra Virgin Olive Oils. J. Food Sci. 2011, 76, S170–S176. [Google Scholar] [CrossRef]
- Grunert, K.G.; Scholderer, J.; Rogeaux, M. Determinants of consumer understanding of health claims. Appetite 2011, 56, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Banks, A.P.; Egan, B.; Hodgkins, C.E.; Peacock, M.; Raats, M.M. The role of causal models and beliefs in interpreting health claims. Br. J. Heal. Psychol. 2018, 23, 933–948. [Google Scholar] [CrossRef] [PubMed]
- Beardsworth, A.; Bryman, A.; Keil, T.; Goode, J.; Haslam, C.; Lancashire, E. Women, men and food: The significance of gender for nutritional attitudes and choices. Br. Food J. 2002, 104, 470–491. [Google Scholar] [CrossRef]
- Owen, R.W.; Giacosa, A.; E Hull, W.; Haubner, R.; Würtele, G.; Spiegelhalder, B.; Bartsch, H. Olive-oil consumption and health: The possible role of antioxidants. Lancet Oncol. 2000, 1, 107–112. [Google Scholar] [CrossRef]
- Stark, A.H.; Madar, Z. Olive oil as a functional food: Epidemiology and nutritional approaches. Nutr. Rev. 2002, 60, 170–176. [Google Scholar] [CrossRef]
- Saba, A.; Sinesio, F.; Moneta, E.; Dinnella, C.; Laureati, M.; Torri, L.; Peparaio, M.; Civitelli, E.S.; Endrizzi, I.; Gasperi, F.; et al. Measuring consumers attitudes towards health and taste and their association with food-related life-styles and preferences. Food Qual. Prefer. 2019, 73, 25–37. [Google Scholar] [CrossRef]
- Brucks, M. The effects of product class knowledge on information search behaviour. J. Consum. Res. 1985, 12, 1–16. [Google Scholar] [CrossRef]
- Aertsens, J.; Mondelaers, K.; Verbeke, W.; Buysse, J.; Van Huylenbroeck, G. The influence of subjective and objective knowledge on attitude, motivations and consumption of organic food. Br. Food J. 2011, 113, 1353–1378. [Google Scholar] [CrossRef]
- Tourist Board of Istria. 2018. Available online: http://www.istra.hr/hr/smjestaj (accessed on 25 March 2019).
- Veal, A.J. Research Methods for Leisure and Tourism: A Practical Guide; Pearson Education Limited: Essex, UK, 2006; p. 446. [Google Scholar]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis, 7th ed.; Pearson Education Inc.: London, UK, 2010; p. 761. [Google Scholar]
- Cicerale, S.; Liem, G.; Keast, R.S. Consumer Perception, Attitudes, Liking and Preferences for Olive Oil. Prod. Olive Tree 2016, 157–172. [Google Scholar] [CrossRef] [Green Version]
- Samoggia, A.; Riedel, B. Consumers’ Perceptions of Coffee Health Benefits and Motives for Coffee Consumption and Purchasing. Nutrients 2019, 11, 653. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salazar-Ordóñez, M.; Rodríguez-Entrena, M.; Cabrera, E.R.; Henseler, J. Understanding product differentiation failures: The role of product knowledge and brand credence in olive oil markets. Food Qual. Prefer. 2018, 68, 146–155. [Google Scholar] [CrossRef]
- Hayes, A. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Publications: New York, NY, USA, 2013; pp. 1–692. [Google Scholar]
- Rizzo, G.; Borrello, M.; Guccione, G.D.; Schifani, G.; Cembalo, L. Organic Food Consumption: The Relevance of the Health Attribute. Sustainability 2020, 12, 595. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristic | Options | Frequency | Percentage |
|---|---|---|---|
| Gender | Male | 262 | 39.6 |
| Female | 400 | 60.4 | |
| Age | Up to 25 | 33 | 5.0 |
| 25 to 34 | 104 | 15.7 | |
| 35 to 44 | 195 | 29.5 | |
| 45 to 54 | 145 | 21.9 | |
| 55 to 64 | 137 | 20.7 | |
| 65 and more | 48 | 7.2 | |
| Country of origin | Austria | 187 | 28.3 |
| Germany | 175 | 26.4 | |
| UK | 109 | 16.5 | |
| Russia | 31 | 4.7 | |
| Croatia | 96 | 14.5 | |
| Italy | 53 | 8.0 | |
| Other | 11 | 1.6 | |
| Education level | Primary school | 31 | 4.7 |
| High school | 251 | 37.9 | |
| Higher education | 380 | 57.4 | |
| Profession | Self-employed | 122 | 18.4 |
| Manager | 72 | 10.9 | |
| Employee | 351 | 53.0 | |
| Retired | 64 | 9.7 | |
| Other | 53 | 8.0 | |
| Personal net monthly income | Up to €1000 | 98 | 14.8 |
| €1001–€2000 | 206 | 31.1 | |
| €2001–€3000 | 171 | 25.8 | |
| €3001–€4000 | 97 | 14.7 | |
| €4001 and more | 90 | 13.6 | |
| Monthly spending for olive oil | Up to € 10 | 399 | 60.2 |
| €10–€20 | 187 | 28.3 | |
| €21–€40 | 50 | 7.6 | |
| €41 and more | 26 | 3.9 | |
| Olive oil consumption per month | Up to 1 L | 96 | 14.5 |
| 1 L to 2 L | 160 | 24.2 | |
| 3 L to 5 L | 171 | 25.8 | |
| More than 5 L | 235 | 35.5 |
| Factor | Item | Mean | SD | Standard Load |
|---|---|---|---|---|
| Motive 1 Culture /tradition | Olive oil consumption is a family tradition. | 4.1 | 1.11 | 0.939 |
| Olive oil consumption is part of one’s cultural background. | 4.1 | 1.14 | 0.839 | |
| Extensive knowledge about olive oil. | 4.0 | 1.10 | 0.774 | |
| Motive 2 Pleasure | Product is good for my health. | 2.9 | 1.45 | 0.786 |
| Olive oil is a natural product. | 2.7 | 1.47 | 0.783 | |
| Food smells and tastes better with olive oil. | 2.6 | 1.33 | 0.718 | |
| Olive oil benefits perception | Olive oil provides health benefits. | 3.5 | 1.18 | 0.867 |
| Olive oil regulates blood cholesterol levels. | 3.5 | 1.17 | 0.774 | |
| Olive oil is good for my health. | 3.4 | 1.18 | 0.784 | |
| Olive oil is good for blood vessels’ health. | 3.3 | 1.21 | 0.846 | |
| Olive oil is good for physical fitness and memory. | 3.1 | 1.27 | 0.769 | |
| Healthy | Limitation of sugar intake. | 3.9 | 1.03 | 0.953 |
| behaviour | Limitation of fat intake. | 4.0 | 1.05 | 0.890 |
| Limitation of salt intake. | 3.5 | 1.17 | 0.691 | |
| Increase in fibre intake. | 3.9 | 1.01 | 0.844 | |
| Increase in vitamin intake. | 3.7 | 1.05 | 0.723 |
| CR | AVE | Motive 1: Culture/Tradition | Healthy Behaviour | Olive Oil Benefits Perception | Motive 2: Pleasure | |
|---|---|---|---|---|---|---|
| Motive 1: Culture/tradition | 0.807 | 0.582 | 0.763 | |||
| Healthy behaviour | 0.904 | 0.654 | 0.326 *** | 0.809 | ||
| Olive oil benefits perception | 0.914 | 0.683 | 0.622 *** | 0.452 *** | 0.826 | |
| Motive 2: Pleasure | 0.889 | 0.728 | 0.558 *** | 0.318 *** | 0.541 *** | 0.853 |
| H | Relationship | β | R2 | Decision |
|---|---|---|---|---|
| H1 | Healthy behaviour → olive oil benefits perception | 0.447 *** | 0.238 | Supported |
| H2 | Healthy behaviour → motive 1 | −0.033 | 0.529 | Not supported |
| H3 | Olive oil benefits perception → motive 1 | 0.732 *** | Supported | |
| H4 | Healthy behaviour → motive 2 | 0.099 ** | 0.31 | Supported |
| H5 | Olive oil benefits perception → motive 2 | 0.503 *** | Supported |
| H | Relationship | β | Confidence Interval | Decision | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| H6 | Healthy behaviour → olive oil benefits Perception → motive 1 | 0.316 *** | 0.262 | 0.370 | Supported |
| H7 | Healthy behaviour → olive oil benefits Perception → motive 2 | 0.249 *** | 0.205 | 0.309 | Supported |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ilak Peršurić, A.S.; Težak Damijanić, A. Connections between Healthy Behaviour, Perception of Olive Oil Health Benefits, and Olive Oil Consumption Motives. Sustainability 2021, 13, 7630. https://doi.org/10.3390/su13147630
Ilak Peršurić AS, Težak Damijanić A. Connections between Healthy Behaviour, Perception of Olive Oil Health Benefits, and Olive Oil Consumption Motives. Sustainability. 2021; 13(14):7630. https://doi.org/10.3390/su13147630
Chicago/Turabian StyleIlak Peršurić, Anita Silvana, and Ana Težak Damijanić. 2021. "Connections between Healthy Behaviour, Perception of Olive Oil Health Benefits, and Olive Oil Consumption Motives" Sustainability 13, no. 14: 7630. https://doi.org/10.3390/su13147630
APA StyleIlak Peršurić, A. S., & Težak Damijanić, A. (2021). Connections between Healthy Behaviour, Perception of Olive Oil Health Benefits, and Olive Oil Consumption Motives. Sustainability, 13(14), 7630. https://doi.org/10.3390/su13147630