Abstract
With the aim of moving towards a more sustainable society, hospital buildings are challenged to decrease their environmental impact while continuing to offer affordable and qualitative medical care. The aim of this paper was to gain insight into the main drivers of the environmental impacts and costs of healthcare facilities, and to identify methodological obstacles for a quantitative assessment. More specifically, the objective was to assess the environmental and financial impacts of the general hospital Sint Maarten in Mechelen (Belgium) by using a life cycle approach. The hospital building was analyzed based on a combination of a simplified life cycle assessment and life cycle costing. The “MMG+_KULeuven” assessment tool was used for the calculation of environmental impacts and financial costs. The study revealed that the environmental impact was mainly caused by electricity use for appliances and lighting, cleaning processes, material production, and spatial heating, while building construction and electricity use caused the highest financial costs. The most relevant impact categories identified were global warming, eutrophication, acidification, human toxicity (cancer and non-cancer effects), and particulate matter. Various methodological challenges were identified, such as the adaptation of existing methods to ensure applicability to hospital buildings and the extraction of data from a Revit model.
1. Introduction
Hospital buildings play a major role in healing people, yet at the same time they are highly dependent on natural resources and cause significant environmental burdens due to, amongst others, greenhouse gas emissions, waste production, regular renovation due to technological innovations, and daily cleaning. European hospitals with their supply chains are responsible for 5% of the yearly CO2 emissions in Europe [1]. While, in the past decade, an increased interest has been noticed in reducing the negative impacts of hospitals, these settings seem to fail to address sustainability issues fully [2]. This stems from the fact that in a patient-oriented sector, medical preconditions, such as safety and hygiene, prevail over all others when it comes to providing affordable and qualitative medical care. Moreover, as hospitals are very complex buildings, housing different building typologies within the same ‘shell’, evaluating their sustainability represents a real challenge.
McGain and Naylor [3] reviewed the literature on hospital sustainability, focusing mainly on environmental issues and dividing literature into seven topics: Hospital design, energy, water, travel, procured goods, waste, and staff behavior. From their study, McGain and Naylor acknowledged the importance of future research in the areas of measuring hospital environmental ‘footprints’, technological, clinical and organizational innovations, social aspects and psychological research, policy research, and finally, assessing the effects of environmental and climate change on health [3].
The increasing concern about the sustainability of healthcare buildings is furthermore reflected in the proliferation of guides and certification schemes specifically developed to assess these facilities within the existing qualitative methods, such as BREEAM, LEED, CASBEE and DGNB [4]. Being easy to use from the very first phases of project design, these methods gained popularity among urban planners, architects and engineers. As the assessment of sustainability with these types of tools are based on subjective scoring, doubts have risen about whether using such methods leads to truly sustainable buildings [5,6]. Furthermore, their static character—due to their approach of checking the application of a list of measures—does not allow a response to the rapidly changing requirements and needs of healthcare buildings. A critical analysis comparing four sustainability certification schemes for healthcare buildings, namely BREEAM New Constructions, LEED for healthcare, CASBEE for New Constructions and Green Star Healthcare v1 can be found in Castro, Mateus and Bragança [4]. In their study, the authors explored the similarities and differences between the methods and how they meet the CEN EN 15643-2, EN 15643-3, EN 15643-4, and ISO 21929-1 standards in the context of sustainable construction. Castro, Mateus and Bragança [4] concluded that the existing qualitative methods were mostly in line with the standards, but differed in the choice of indicators necessary to assess the economic dimension and in the life cycle stages considered. In addition, the authors recognized the importance of using life cycle costing (LCC) and environmental life cycle assessment (LCA) when evaluating the economic and environmental sustainability of a hospital building. Although Castro, Mateus and Bragança [4] included environmental and financial indicators based on LCA and LCC in their newly proposed healthcare building sustainability assessment method [7,8], they did not provide detailed methodological rules specifying the LCA and LCC methods in more detail for the specific aim of evaluating hospital buildings and left this open to the user.
The shift towards sustainability assessment in the construction sector using approaches based on the life cycle thinking perspective has been reflected in various recent studies. Though not strictly focusing on hospital buildings, Zabalza et al. [9], for example, discussed using both LCA and LCC as a tool to evaluate energy savings to help building practitioners in better decision making. Fouche and Crawford [10] reviewed the literature of studies implementing both methods synchronously at a building level, acknowledging the importance of such an integrated approach to address life cycle greenhouse gas (GHG) emissions. Furthermore, the authors confirmed the lack of studies combining LCA and LCC in hospital buildings.
Quantifying the environmental and economic burdens of hospital buildings is, hence, seen as an important challenge to gain better insight and improve the sustainability of healthcare facilities. LCA and LCC are, however, relatively new in the healthcare sector [3]. So far, these two internationally recognized methodologies have been applied at the level of procured goods (surgical equipment, laryngeal masks, etc.), as in Campion et al. [11], Eckelman et al. [12], and Stripple, Westman, and Holm [13], waste management, as in Soares et al. [14] and Ali, Wang, and Chaudhry [15], and operating procedures, as in Thiel et al. [16]. Harris and Fitzgerald [17] studied the LCC of various floor finishes, with the aim of comparing hard and soft flooring materials in order to inform decision makers about the long-term costs of ownership, followed by safety, durability, and aesthetic factors.
Based on a literature review, it can be concluded that LCA and LCC have neither separately nor simultaneously been applied at the level of hospital buildings. Nevertheless, during the past few years, the certification schemes have been updated and have incorporated LCA into their frameworks, with the intention of bridging this gap. Schmidt [18], however, argues that the quantified environmental performance of building materials in these schemes is still not sufficiently brought to the fore, with materials and products accounting for only about 6% of the total sustainability score.
Most important design decisions are taken during the early design phase. Supporting tools, which can be used from this phase onwards and which are specifically appropriate for the design of healthcare facilities, are therefore seen as crucial, but are lacking. The need for a quantitative assessment tool to evaluate the environmental and financial impacts of a hospital building during the early design phase is thus identified.
Scope of the Study
The present paper aimed at gaining insight into the life cycle environmental impacts and financial costs of hospital buildings in Flanders (Belgium). A newly built hospital building, the general hospital Sint Maarten in Mechelen that opened in 2018, was analyzed. It was selected as a case study because of data availability, as it was designed by the company collaborating in this research, and because it could be seen as a representative, newly-built monoblock hospital building in Flanders. The aim of the assessment was to identify methodological challenges when studying the life cycle environmental impact and cost of a hospital building, and to identify hotspots from both an environmental and economic point of view. The latter allowed the identification of priorities for reducing life cycle impacts and costs. The outcomes are seen as valuable cornerstones for the development of a quantitative sustainability assessment method for hospitals in a Belgian context.
2. Materials and Methods
As defined in Wittstock et al. [19] and discussed by Simonen [20], different types of LCA analyses (i.e., screening LCA, simplified LCA, and complete LCA) are possible. Their relationship, as well as the links between time, effort, and overall data quality (Figure 1) can be found in Simonen [20] and the International Reference Life Cycle Data System (ILCD) Handbook [21].
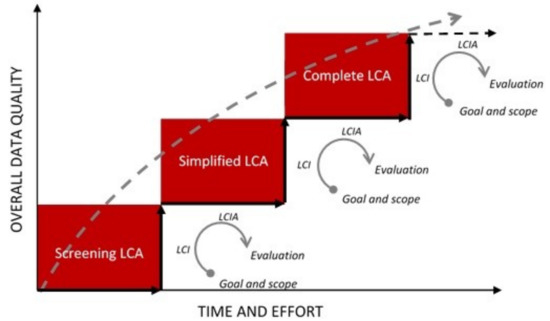
Figure 1.
The iterative nature of life cycle assessment (LCA) [20,21].
Screening LCA provides a quick overview of the environmental impacts of a building, without requiring high quality data and large amounts of time. Such a study typically focuses on the main contributors to the system under assessment, including (but not limited to) the input materials, water and energy use, and the transportation of users, if relevant [19]. Compared to a screening LCA, where generic assumptions are often used, simplified LCA studies are based on information that is already available from the company. As mentioned in the European Energy Efficient Building Guide (EeBGuide) [19], for a simplified LCA study, specific quantitative environmental information on building elements, products, materials, components, and services should be used wherever possible. A complete LCA is in line with the ISO 14040 and ISO 14044 standards and takes into account the whole life cycle of a building, i.e., from cradle to grave. When applying this level of the study, recommendations from the ILCD Handbook [21] should be followed [19]. A complete LCA often results from an iterative analysis in order to include complete inventories and high-quality data, which ensure a more accurate and comprehensive study.
For the purpose of our study, a simplified LCA and LCC were chosen as the preferred methods. As our study was not intended for comparative assertions, benchmarking, or design decisions, a higher level of accuracy was found unnecessary and not appropriate in the early design phase of the buildings.
2.1. Integrated Life Cycle Thinking Approach
LCA is a standardized methodology to estimate the environmental impact of a process or product, including buildings, over the entire life cycle. Though still advancing, LCA has become an internationally-recognized method that quantifies the inputs from, and outputs to, nature [22]. The broad acceptance is reflected in the international standards ISO 14040 [23] and ISO 14044 [24], and in the European standards EN15804 [25] and EN15978 [26], focusing on construction products and buildings, respectively.
In addition to the environmental impact, costs are an important issue in a sustainability context. Considering that the cost of environmentally beneficial measures will not only guarantee affordability, but also prioritize the most efficient measures within a limited budget, LCC is a widely accepted economic calculation method to estimate the life cycle costs of a building [27].
Although social sustainability is another important aspect when dealing with the assessment of hospital buildings, it was not included in this study. Social LCA (S-LCA) is currently under development, but was not found mature enough to be included in the assessment of a hospital building.
In this paper, an integrated approach combining LCA and LCC was used to assess both the environmental and economic impacts of hospital buildings. This approach has already been applied to various other building types and/or parts of buildings [28,29,30,31,32,33] and proved appropriate. The subsequent subsections describe the LCA and LCC methods used in more detail. The life cycle phases considered in our study are shown in Figure 2.
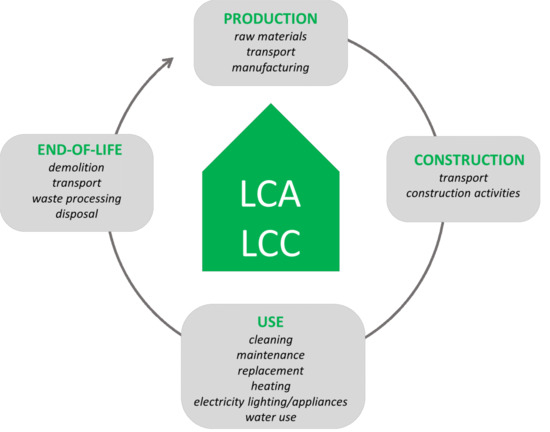
Figure 2.
Life cycle phases of a building. Adapted from [34].
2.2. Life Cycle Assessment (LCA)
The environmental impact of the general hospital Sint Maarten was assessed with the MMG (Milieugerelateerde Materiaalprestatie van Gebouwelementen, translated into English under the title “Environmental profile of building elements”) method commissioned by the Public Waste Agency of Flanders (OVAM). The MMG method is the Belgian LCA method for building elements and buildings [34] and is in line with European standards EN 15804 [25] and EN 15978 [26]. The method considered two sets of impact categories. The first set covered the seven impact categories, as defined in the CEN TC350 standards (Table 1, left column). These categories were further referred to as CEN categories. Additionally, based on the ILCD Handbook [21] and in consultation with Flemish–Belgian policy makers, a list of additional impact categories was added, further referred to as CEN+ categories (Table 1, right column).

Table 1.
Environmental impact categories of the MMG method, distinguishing CEN and CEN+ categories [35].
In addition to the characterized scores per impact category, the MMG method allowed the calculation of an external environmental cost, expressed in monetary values (Euro). External costs were calculated based on two methods, i.e., damage and prevention cost methods. The damage cost method calculated how emissions and resource depletion affected agriculture and public health, which lead to welfare losses in terms of additional costs (e.g., medicine costs), loss of income (e.g., sick leave), or comfort (e.g., pain). The monetary valuation of these impacts used different methods and data, such as market data and data from scientific literature to value pain or loss of life expectancy, based on revealed or stated willingness to pay. The prevention cost method (also referred to as the control or abatement costs method) valued an impact based on the marginal cost to meet a policy objective for a specific impact. This required a clear policy objective, information about all potential prevention measures in different sectors, and their cost-effectiveness. The cost of the least cost-efficient measure to meet the target was an indicator of the value society was willing to pay or impose to control the environmental problem and was defined as the prevention cost. A more detailed explanation regarding the external cost calculation can be found in Allacker [28] and Allacker et al. [35].
The overview of the monetary values for each impact category, including a median, minimum, and maximum scenario, is provided in Table 2. In this paper, the median values were used. The external cost of a certain impact category was calculated by multiplying the characterized environmental impact with the monetary value of the unit flow. By adding the monetary values of all impact categories, an overall environmental cost (single score) was obtained [35]. As explained by Trigaux et al. [36], similar to the financial cost calculation, discounting of future environmental cost was applied based on a real social discount rate of 1% (Table 3).
Table 2.
Overview of the monetary values (median, minimum, and maximum scenarios) for the CEN and CEN+ indicators [35].
Table 3.
Economic parameters used for the financial and environmental costs (real rates above the inflation), based on Allacker et al. [35].
The method was translated into an Excel-based tool in the research division of Architectural Engineering at KU Leuven. Further in the text, the calculation tool will be referred to as the MMG+_KULeuven tool. This tool was used for the assessment of the hospital building. For the life cycle inventory (LCI) within this tool, the Ecoinvent database (version 2.2) was used, with preference given to Western European processes to ensure representativeness of the Belgian context [35]. The vast majority of the materials and processes occurring in the hospital building were already included in the calculation tool, however several were found to be lacking, as the MMG+_KULeuven tool was originally developed for residential buildings. The missing materials were modelled and exported from the SimaPro software (version 8.3) and integrated into the tool.
The considered life cycle stages were in line with the EN 15978 standard [26] and the system boundary covered the following: Production, construction, use, and end-of-life (EOL) processes. The modules, from A1 to C4, included in each stage are presented in Figure 3. In the MMG+_KULeuven tool, module B2, referring to maintenance, was divided into three parts considering cleaning, small maintenance, and big maintenance. Additionally, the operational energy use module was divided into operational energy use for heating and the operational energy use for electricity (lighting and appliances). The following life cycle stages were excluded: Release of substances from building materials in the local environment (use—B1) and replacements due to accidental damage or failure (repair—B3).
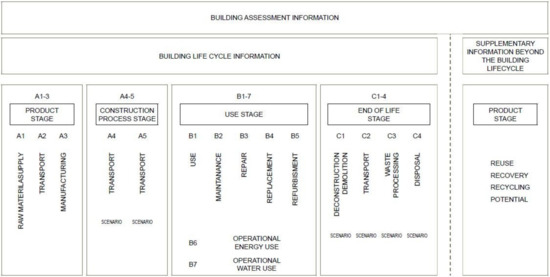
Figure 3.
Life cycle stages as defined in CEN 15978 standard [26].
2.3. Life Cycle Costing (LCC)
The costs included in the LCC analysis were investment costs (construction materials, labor, and indirect costs for construction), costs for cleaning, maintenance, replacements, refurbishment of building elements, operational energy and operational water use, and the demolition and waste treatment costs.
In the Excel-based MMG+_KULeuven tool, a module to calculate the building life cycle costs was included. The financial data were mostly based on the Belgian cost database, ASPEN [37,38]. Missing costs in the ASPEN database were collected from other sources, such as the British Spon’s Price Books External Works and Landscape Price book [39], for example, for the cost of sliding doors. The life cycle financial cost was calculated as the sum of the present values (for the reference year 2015) of all costs occurring during the life cycle of the hospital building. Regarding the economic parameters in real terms, these were based on Belgian statistical data and are summarized in Table 2 [36].
2.4. System Boundaries, Functional Units, and Data Collection
For the assessment of the general hospital Sint Maarten, the system boundary was set to the scale of the building excluding its surroundings. The infrastructure to access the hospital campus and the energy for user transportation were excluded. All building parts were included, except for the technical installations for heating, ventilation, and air-conditioning (HVAC), as well as medical apparatus. The HVAC system was analyzed in a later phase of the research. An estimated building service life of 30 years was assumed, after which a thorough renovation of the hospital building is necessary.
The data collection of a complex system such as a building requires a systematic collection, in order to avoid data gaps or double counting. In line with the MMG method, the BB/SfB (The BB/SfB system is the official Belgian version of the internationally recognised CI/SfB classification system. CI/SfB is the Construction Index/ Samarbetskommitten for Byggnadsfragor, a Scandinavian classification system intended for the construction industry.) classification system was used [40] to subdivide the building into smaller components, i.e., building elements. More specifically, the building elements were classified into ten categories: (1) Floor on ground (Table S_A1 describes the build-up of each floor type, impacts and costs are shown in Figure S_A1 to Figure S_A7.), (2) external wall (Table S_B1 describes the build-up of each wall type, impacts and costs are shown in Figure S_B1 to Figure S_B7), (3) loadbearing internal wall (Table S_C1 describes the build-up of each wall type, impacts and costs are shown in Figure S_C1 to Figure S_C6), (4) non-loadbearing internal wall (Table S_D1 describes the build-up of each wall type, impacts and costs are shown in Figure S_D1 to Figure S_D7), (5) story floor (Table S_E1 to Table S_E24 describe the build-up of each floor type, impacts and costs are shown in Figure S_E1 to Figure S_E7), (6) stairs (impacts and costs are shown in Figure S_F1 to Figure S_F7), (7) free-standing column (impacts and costs are shown in Figure S_G1 to Figure S_G7), (8) flat roof (Table S_H1 describes the build-up of each roof type, impacts and costs are shown in Figure S_H1 to Figure S_H7), (9) windows and exterior doors (impacts and costs are shown in Figure S_I1 to Figure S_I7), and (10) internal doors (impacts and costs are shown in Figure S_J1 to Figure S_J7).
A two-step procedure was used for the life cycle inventory of the building. Firstly, quantities of building elements were determined, and their composition of various materials inventoried. For each of the materials occurring, specifications were searched for. Estimations were investigated for the operational energy and operational water use. These data were all provided by VK Architects & Engineers. The information consisted of building plans extracted from a Revit model using Autodesk® Design Review 2013, detailed specifications of materials, Excel files with quantities of building elements, as well as energy (both electricity and gas) and water consumption. Based on this information, 93 building elements were defined as the main construction components of the hospital. The bill of quantities of all building elements are given in Table S_I3. Secondly, the inventories for each of the materials and processes identified were collected. As mentioned before, the majority of the materials were already included in the MMG+_KULeuven tool. Materials not included in MMG+_KULeuven tool’s database were the following: Several floor finishes made of polyvinylchloride, sandwich panels, a cavity floor system made of steel, a polished concrete floor, and a ceiling finish made of steel slats. These were modelled in Simapro and exported to the MMG+_KULeuven calculation tool. Finally, free-standing columns of reinforced concrete were not yet included in the calculation tool and were added.
The yearly operational energy use for heating was based on the energy benchmarking for Flemish hospitals received from VK Architects & Engineers. The gross heating demand equaled 118 kWh/m2 per year, with an assumed system efficiency of 85% and heated with gas. For the electricity demand, an estimated consumption of 136 kWh/m2 per year was used, based on the VIPA’s (Flemish Infrastructure Fund for Person-related Matters) standards. This demand covered the electricity for ventilation, lighting, and medical apparatus. For water use, a yearly consumption per square meter of floor area was assumed to be 1363 liters, based on the average value of 500 L/bed in Belgian general hospitals [41]. For cleaning, it was assumed that floors were cleaned on a daily basis, while walls, windows, and doors were assumed to be cleaned once a week (52 times per year). The cleaning processes were based on the existing ones available in the MMG+_KULeuven tool.
2.5. Description of the Case Study
The case study chosen for the analysis was a project resulting from the collaboration between VK Architects & Engineers and Ingenium. VK Architects & Engineers are specialized in designing and engineering healthcare buildings, while Ingenium is a consultancy office focusing on sustainable solutions in the building sector. The competition for the general hospital in Mechelen aimed at merging three campuses of the Sint Maarten network into one new construction. The building houses 723 accredited beds and is located near the ring road of Mechelen. VK Architects & Engineers provided the solutions for the architecture, hospital programming, landscape design and fire safety, façade, and acoustical engineering, whereas Ingenium was responsible for the implementation of all technical equipment of the hospital. To achieve a more compact building, and therefore reduce the building envelope, construction cost, and energy use, the architects decided to design a monoblock hospital (hospital building typology is described in Prasad [2] and Wagenaar [42] (Figure 4)). The net floor area of the hospital is 96,860 m2. The net floor area equals the sum of all floor surfaces used, excluding the surfaces in contact with the internal and external walls. The hospital has seven floors in total; six floors above ground and one underground floor. The floors above ground include the entrance hall, consultation rooms, patient wards, laboratories, administration offices, operating theatres, technical rooms, shops, pharmacy, etc. All supporting departments and functions, such as ICT, sterilization, kitchen, linen cleaning, mortuary, staff restaurant, archive, and technical rooms, are located on the underground floor. Radiotherapy is also situated on this floor.

Figure 4.
The construction site, November 2015 (© VK Architects & Engineers).
The loadbearing core structure of the hospital was made of precast concrete elements for faster construction, with the internal free-standing columns made of in-situ reinforced concrete. Only the diagonal columns at the entrance hall, seen in Figure 4, are made of precast concrete. White architectural concrete was used for the façade finishing, while the major choices for internal wall finishing were gypsum board with acrylic paint. Regarding the floor finishes, polyvinyl chloride is the most represented material, and the ceilings are mostly a suspended type with mineral fiber boards.
3. Results
Although the results focused on the impact of the hospital at building level, the structuring of the model in various building elements allowed an investigation into the contribution of each of the elements, and to analyze each of these in detail. The subsequent paragraphs focus on the overall building impact. The results of each building element are given in the Supplementary Material, except for the story floors, which are presented in Section 3.2.
3.1. Environmental Impact of the Hospital Building
The environmental impact, expressed in external costs per life cycle phase for both CEN and CEN+ indicators are presented in Figure 5. Considering the CEN indicators, the most impactful process was the electricity use for ventilation, lighting, and medical devices, accounting for 139.16 €/m2 of the net floor area, i.e., 49.5% of the life cycle environmental cost of the CEN indicators. The electricity mix for Belgium as available in the Ecoinvent database (version 2.2) is modelled based on national and international statistics. The mix is dominated by nuclear and electricity from natural gas, with the latter being responsible for the highest amount of environmental impact in the global warming category. The complete energy list for the Belgian electricity mix can be found in Supplementary Information Table S_I4. In addition to this electricity use, the three most impactful processes were production of the construction materials with 29.53 €/m2 of the net floor area, cleaning processes with 33.90 €/m2 of the net floor area, and heating energy with 72.11 €/m2 of the net floor area, i.e., 10.5%, 12%, and 26% of the life cycle CEN environmental costs, respectively. The environmental impact of the cleaning processes was mainly due to the daily cleaning of the hospital floors. The transport of the construction products to site and the construction process were responsible for less than 1% of the life cycle CEN environmental cost, with 1.52 and 1.65 €/m2 of the net floor area, i.e., 0.53% and 0.58% of the life cycle CEN environmental costs, respectively. The environmental impact of the operational water use represented 1.16 €/m2 of the net floor area, i.e., only 0.42% of the life cycle CEN environmental impact. Finally, the maintenance, replacements, refurbishment (both of work sections and elements), demolition, transport to EOL, and EOL phases had a negligible impact, contributing to around 0.2% of the life cycle CEN environmental cost.
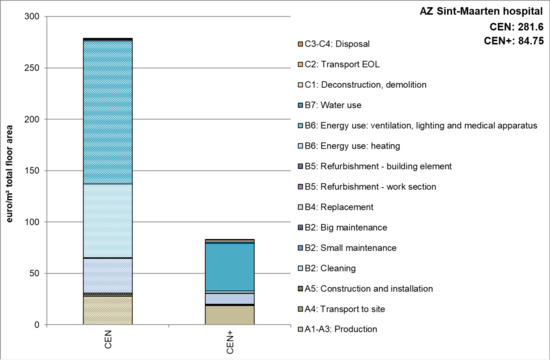
Figure 5.
General hospital Sint Maarten: Environmental impacts expressed as environmental costs per life cycle phase.
A sensitivity analysis was carried out to determine how the results would change in case the electricity mix changed to a fully renewable mix from the Ecoinvent database, consisting of 50% wind power and 50% electricity from photovoltaic panels. The main hotspots after this change were the operational energy use for heating, cleaning, and material production processes. Thus, the energy mix had a high influence on the results.
Looking at the CEN+ indicators, the electricity use for ventilation, lighting, and medical devices again caused the highest impact, with 46.55 €/m2 of the net floor area, i.e., 55% of the life cycle environmental cost of the CEN+ indicators. The second most impactful process was the production of building materials, with 20.28 €/m2 of the net floor area representing 24% of the life cycle CEN+ environmental cost. The cleaning processes were responsible for 12.20% of the life cycle CEN+ environmental cost, with 10.32 €/m2 of the net floor area, while operational energy use for heating and deconstruction processes each represented 2.50% of the life cycle CEN+ cost, with 2.09 and 2.13 €/m2 of the net floor area. Similar to the case of the CEN indicators, the remaining processes had negligible environmental impacts, contributing to 3.8% of the life cycle CEN+ environmental cost.
Detailed results of the environmental impact per life cycle phase can be found in Table S_H1 (expressed in monetary values) and Figure S_K1 (expressed in impact equivalents per impact category).
The contribution of impact categories to the overall life cycle environmental impact showed that the most significant ones in terms of CEN indicators were global warming, acidification of land and water sources, and eutrophication. These three categories were responsible for 258.27 (92%), 3.15 (1.10%), and 19.97 (7%) €/m2 of the net floor area, respectively. The main drivers of these three impacts were electricity for ventilation, lighting and medical apparatus, energy for heating, and the production processes. Within the CEN+ indicators, the impacts predominantly were related to human toxicity, both cancer and non-cancer effects, with 37.39 and 13.15 €/m2 of the net floor area (44% and 15.50%), particulate matter with 29.21 €/m2 of the net floor area being 34.50%, and land use of 2.88 €/m2 of the net floor area being 3.40% of the mentioned indicators (Figure 6). The major drivers in both human toxicity cancer effects and non-cancer effects were production of material (predominantly coming from concrete) and electricity. In the case of particulate matter, three phases were responsible for the main causes, being production, electricity, and deconstruction. As for land use, the major causes were production, cleaning, and electricity.
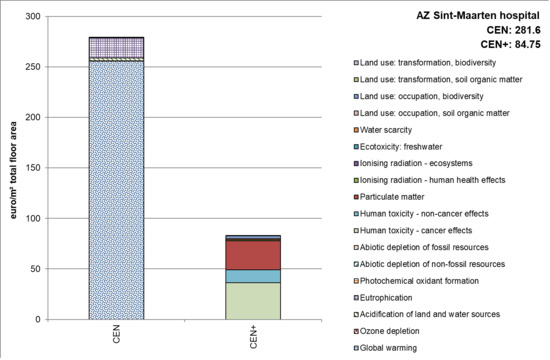
Figure 6.
General hospital Sint Maarten: Environmental impacts expressed as environmental costs per impact category.
3.2. Financial Cost of the Hospital Building
The life cycle financial cost of the general hospital Sint Maarten equaled 2969.85 €/m2 of the net floor area (without technical services; Figure 6 and Table S_I.2). The investment cost equaled 965.87 €/m2 of the net floor area, being the most expensive phase of the project (i.e., 32.50% of the life cycle cost). The building elements with the highest financial share in the investment phase were the following:
- External walls made of precast concrete (thickness of 24 cm) with architectural concrete as external finishing;
- Non-loadbearing internal gypsum walls, 11 cm thickness; and
- Story floors with mineral fiber panels as ceiling finish and a PVC floor finish on an anhydrite screed.
For a better understanding of the aforementioned building elements, an overview of all the construction layers for each element is given in Table 4.
Table 4.
Composition of the three most occurring building elements in the general hospital Sint Maarten with all layers included.
These three elements were identified as the most occurring ones in the Sint Maarten hospital, representing the total of 13,727 m2 of external walls, 49,770 m2 of non-loadbearing internal walls and 35,374 m2 of story floors respectively. To analyze the reliability of the investment cost calculated with the generic databases (ASPEN and Spon), the investment cost was compared with the cost provided by VK Architects & Engineers. The latter was found to be 8% higher. Based on this validation, it was concluded that the result from the simplified LCC analysis was sufficiently accurate.
The second most costly life cycle phase/process was electricity use for ventilation, lighting, and medical devices, responsible for 833.00 €/m2 of the net floor area, representing 28% of the life cycle financial cost (Figure 7). This was followed by cleaning and energy for spatial heating, with 707.50 €/m2 of the net floor area (representing 24%) and 217.10 €/m2 of the net floor area (representing 7.3%), respectively. Finally, operational water use amounted to 140.80 €/m2 of the net floor area, being 4.70% of the life cycle financial cost. The remaining 3.50% was caused by transport, construction, maintenance, replacement, refurbishment, deconstruction, transport to EOL, and EOL.
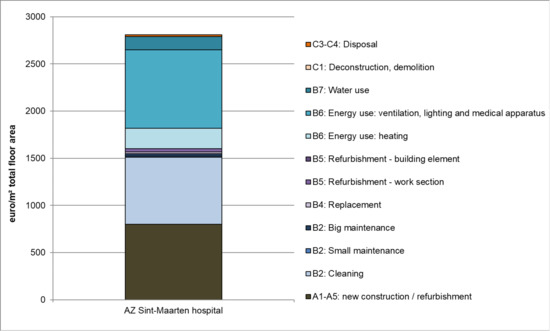
Figure 7.
General hospital Sint Maarten: Financial cost per life cycle phase.
3.3. Total Cost of the Hospital Building
Finally, a total cost was calculated by adding the financial and environmental cost. The total life cycle cost of the Sint Maarten hospital building equaled 2328.50 €/m2 for the net floor area (Figure 8). The financial cost clearly dominated the total cost. From both a financial and environmental point of view, the use phase clearly induced the highest cost. The EOL phase was the least impactful phase, both from financial and environmental perspectives.
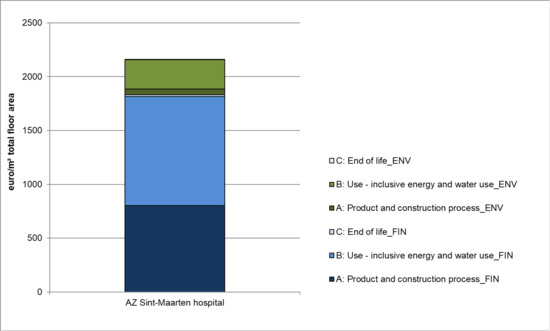
Figure 8.
General hospital Sint Maarten: Total life cycle cost expressed as the sum of financial and environmental costs.
4. Conclusions
In this paper, the economic and environmental impact of the general hospital Sint Maarten was simultaneously assessed by combining a simplified LCA and LCC. The results of the analysis are seen as valuable steps in the development of a more holistic sustainability assessment method for hospital buildings. The analysis has led to several relevant learnings.
Firstly, the MMG+_KULeuven tool was predominantly developed for the analysis of residential buildings and needs adaptations to ensure its applicability to hospital facilities. Various elements and construction products which are common for hospitals were lacking and had to be added, such as free-standing reinforced concrete columns (often used for the main corridors to provide wide open spaces), and hermetically sealed hospital doors. The latter differ largely from the doors used in residential buildings, due to cleaning regimes and the prevention of cross-contamination through bacteria. Several other elements and materials were added, such as specific floor finishes, sandwich panels for the cold storage and freezer units in hospital kitchens, cavity floor systems made of steel and polished concrete floors typically used in technical rooms, and a suspended ceiling made of steel slats to hide technical pipes.
Secondly, the extraction of inventory data from the Revit model often revealed problems, because the structuring in the Revit model was not always in line with that of the LCA/LCC tool. This resulted in a time-consuming calculation of the correct amounts of building materials. It is hence recommended to better align Building Information Modeling (BIM) models with the LCA data inventory structure in the future to allow for a time efficient data gathering step.
Thirdly, hotspots were identified for environmental and financial impacts. From an environmental perspective, electricity use for appliances was identified as the most impactful process, with 51% of the life cycle impact. In terms of environmental impacts, the priority is therefore to decrease the hospital electricity demand where possible. The second most impactful process considering the CEN indicators was the energy for heating, whereas in terms of CEN+ indicators, the production phase takes the second place. The cleaning process was identified as the third most environmentally impactful process from the CEN indicators perspective, closely followed by the production processes. However, in terms of the CEN+ indicators, the impact of the production processes was almost two times the impact of the cleaning processes. From a financial perspective, the production phase was identified as most costly, representing 32.50% of the life cycle financial cost.
Finally, the simplified LCA and LCC of a hospital building is a first, but crucial step in the overall aim of developing a quantitative sustainability assessment method for hospital buildings in Flanders. Based on the outcomes of this study, it is clearly necessary to create an extensive database with predefined technical solutions for each of the building elements, which can be used in the conceptual phase of the project. Such a database would allow the assessment of LCA and LCC in the early design phase to occur faster and without the need for extensive data input.
In the subsequent research step, a detailed study will be made of the HVAC systems used in hospitals and their environmental impact and cost will be assessed. This will furthermore be integrated into the building model. This will be followed by developing a large database of technical solutions of all building elements for hospital buildings to be used in the early design phase by VK Architects & Engineers. Moreover, a benchmark for each building element will be calculated, which represents current common practice and can support architects in their design process. Finally, based on the research outcomes, a tool will be developed for VK Architects & Engineers to assess the life cycle environmental impact and cost of their hospital designs during the early design phase.
Supplementary Materials
The following are available online at http://www.mdpi.com/2071-1050/11/3/856/s1, Figure S1: title, Table S1: title, Video S1: title.
Author Contributions
Conceptualization; formal analysis; investigation; writing—original draft, M.S. M.S. devised the main conceptual ideas and proof outline of the research. She conducted the research and investigation process, performed the analysis and reported the results. M.S. prepared and presented the published work and wrote the original draft of the manuscript. Supervision; writing—review and editing, K.A. and S.V. K.A. and S.V. supervised the research activity and provided their mentorship throughout the study. Both K.A. and S.V. revised the manuscript and gave their critical review and comments on the language and presentation of the results.
Funding
The study is part of a doctoral research, funded by Flanders Innovation & Entrepreneurship (VLAIO), formerly known as Agency for Innovation by Science and Technology (IWT).
Acknowledgments
The authors would like to express their gratitude to Erik Vereecken, Tom Debacker, Bruno Vanquaethem, Cindy Puystjens and Jos Vanbesien from VK Architects & Engineers for providing necessary data for the analysis.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Roberts, J. Reducing the climate footprint: The EU’s legislative framework and the healthcare sector. 2014. Available online: https://noharm-europe.org/documents/reducing-climate-footprint-eu%E2%80%99s-legislative-framework-and-healthcare-sector-0 (accessed on 31 July 2016).
- Prasad, S. Changing Hospital Architecture; RIBA Publications: London, UK, 2008; p. 288. [Google Scholar]
- McGain, F.; Naylor, C. Environmental sustainability in hospitals—A systematic review and research agenda. J. Health Serv. Res. Policy 2014, 9, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Castro, M.D.F.; Mateus, R.; Bragança, L. A critical analysis of building sustainability assessment methods for healthcare buildings. Environ. Dev. Sustain. 2014, 17, 1381–1412. [Google Scholar] [CrossRef]
- Aspinal, S.; Sertyesilisik, B.; Sourani, A.; Tunstall, A. How Accurately Does Breeam Measure Sustainability? Creat. Educ. 2012, 3, 1–8. [Google Scholar] [CrossRef]
- Reijnders, L.; Van Roekel, A. Comprehensiveness and adequacy of tools for the environmental improvement of buildings. J. Clean. Prod. 1999, 7, 221–225. [Google Scholar] [CrossRef]
- Castro, M.D.F.; Mateus, R.; Bragança, L. Proposal for a Healthcare Building Sustainability Assessment (HBSA) Method. In World SB14 Barcelona; Green Building Council: Madrid, España, 2014; pp. 607–613. [Google Scholar]
- Castro, M.D.F.; Mateus, R.; Bragança, L. Healthcare Building Sustainability Assessment tool—Sustainable Effective Design criteria in the Portuguese context. Environ. Impact Assess. Rev. 2017, 67, 49–60. [Google Scholar] [CrossRef]
- Zabalza, I.; Scarpellini, S.; Aranda, A.; Llera, E.; Jáñez, A. Use of LCA as a tool for building ecodesign. A case study of a low energy building in Spain. Energies 2013, 6, 3901–3921. [Google Scholar] [CrossRef]
- Fouche, M.; Crawford, R.H. Towards an Integrated Approach for Evaluating both the Life Cycle Environmental and Financial Performance of a Building: A Review. Procedia Eng. 2017, 118–127. [Google Scholar] [CrossRef]
- Campion, N.; Thiel, C.L.; Woods, N.C.; Swanzy, L.; Landis, A.E.; Bilec, M.M. Sustainable healthcare and environmental life-cycle impacts of disposable supplies: A focus on disposable custom packs. J. Clean. Prod. 2015, 94, 46–55. [Google Scholar] [CrossRef]
- Eckelman, M.; Mosher, M.; Gonzalez, A.; Sherman, J. Comparative Life Cycle Assessment of Disposable and Reusable Laryngeal Mask Airways. Anesth. Analg. 2012, 114, 1067–1072. [Google Scholar] [CrossRef] [PubMed]
- Stripple, H.; Westman, R.; Holm, D. Development and environmental improvements of plastics for hydrophilic catheters in medical care: An environmental evaluation. J. Clean. Prod. 2008, 16, 1764–1776. [Google Scholar] [CrossRef]
- Soares, S.R.; Finotti, A.R.; da Silva, V.P.; Alvarenga, R.A. Applications of life cycle assessment and cost analysis in health care waste management. Waste Manag. 2013, 33, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.; Wang, W.; Chaudhry, N. Application of life cycle assessment for hospital solid waste management: A case study. J. Air Waste Manag. Assoc. 2016, 66, 1012–1018. [Google Scholar] [CrossRef] [PubMed]
- Thiel, C.L.; Eckelman, M.; Guido, R.; Huddleston, M.; Landis, A.E.; Sherman, J.; Shrake, S.O.; Copley-Woods, N.; Bilec, M.M. Environmental Impacts of Surgical Procedures: Life Cycle Assessment of Hysterectomy in the United States. Environ. Sci. Technol. 2015, 49, 1779–1786. [Google Scholar] [CrossRef] [PubMed]
- Harris, D.D.; Fitzgerald, L. A life-cycle cost analysis for flooring materials for healthcare facilities. J. Hosp. Adm. 2015, 4, 92–100. [Google Scholar] [CrossRef]
- Schmidt, A. Analysis of Five Approaches to Environmental Assessment of Building Components in A Whole Building Context (Eurima Report); FORCE Technology: Lyngby, Denmark, 2012. [Google Scholar]
- Wittstock, B.; Gantner, J.; Saunders, T.; Anderson, J.; Lenz, K.; Carter, C.; Gyetvai, Z.; Kreißig, J.; Braune, A.; Lasvaux, S. EeBGuide Guidance Document Part. B: Buildings. 2012. Available online: https://www.eebguide.eu/?page_id=704 (accessed on 3 February 2019).
- Simonen, K. Life Cycle Assessment; Smith, R.E., Ed.; Routledge: Abingdon, VA, USA, 2014. [Google Scholar]
- European Commission. General guide for Life Cycle Assessment—Detailed guidance; International Reference Life Cycle Data System (ILCD) Handbook; European Commission: Luxembourg City, Luxembourg, 2010; p. 398. [Google Scholar]
- Trusty, W.B.; Horst, S.; Thena, T.A.; Materials, S.; Street, J.; Box, P.O. Integrating LCA Tools in Green Building Rating Systems. Athena. 2007. Available online: https://www.irbnet.de/daten/iconda/CIB2759.pdf (accessed on 17 March 2017).
- ISO 14040. Environmental Management—Life Cycle Assessment—Principles and Framework; International Organization for Standardization: Genève, Switzerland, 2006; Volume 3, p. 20. [Google Scholar]
- ISO 14044. Environmental Management—Life Cycle Assessment—Requirements and Guidelines; International Organization for Standardization: Location, UK, 2006; pp. 652–668. [Google Scholar]
- CEN (Ed.) EN 15804:2012+A1 Sustainability of construction works—Environmental product declaration - Core rules for the product category of construction products. 2013. Available online: https://edu.mynbn.be/nbnframework/index.php/pdfMeta/497954 (accessed on 11 December 2018).
- CEN (Ed.) EN 15978 Sustainability assessment of construction works—assessment of environmental performance of buildings—calculation method. 2012. Available online: https://edu.mynbn.be/nbnframework/index.php/pdfMeta/429889 (accessed on 23 March 2017).
- CEN (Ed.) EN 15643-4:2012—Sustainability of construction works—Assessment of buildings—Part 4: Framework for the assessment of economic performance. 2012. Available online: https://edu.mynbn.be/nbnframework/index.php/pdfMeta/439184 (accessed on 17 April 2018).
- Allacker, K. Sustainable building: The development of an evaluation method. Ph.D. Dissertation, Katholieke Universiteit Leuven, Heverlee, Belgium, September 2010. [Google Scholar]
- Biernacki, M. Integration of life cycle assessment and life cycle costing in decision process. In Radīt nākotni: komunikācija, izglītība bizness; Biznesa augstskolas Turība: Riga, Latvia, 2013; pp. 180–194. [Google Scholar]
- Dattilo, C.; Negro, P.; Landolfo, R. An Integrated Approach for Sustainability (IAS): Life Cycle Assessment (LCA) as a Supporting Tool for Life Cycle Costing (LCC) and Social Issues. In Portugal SB10: Sustainable Building Affordable to All; Technical University of Lisbon: Lisbon, Portugal, 2010. [Google Scholar]
- Heijungs, R.; Settanni, E.; Guinée, J. Toward a computational structure for life cycle sustainability analysis: Unifying LCA and LCC. Int. J. Life Cycle. Assess. 2013, 18, 1722–1733. [Google Scholar] [CrossRef]
- Trigaux, D.; De Troyer, F.; Allacker, K.; Paduart, A.; Debacker, W.; De Temmerman, N. LCC and LCA of dynamic construction in the context of social housing Short Summary. In SB13 Graz—Sustainable Buildings, Construction Products & Technologies; Verlag der Technischen Universität Graz: Graz, Austria, 2013; pp. 437–447. [Google Scholar]
- Wijnants, L.; Allacker, K.; De Troyer, F. Environmental and Financial Life Cycle Assessment of ‘Open-renovation-systems’: Methodology and Case Study. Energy Procedia. 2016, 96, 529–539. [Google Scholar] [CrossRef]
- Trigaux, D.; Allacker, K.; De Troyer, F. A simplified Approach to integrate Energy Calculations in the Life Cycle Assessment of Neighbourhoods. In PLEA 2014 Book of Proceedings; Cept University Press: Ahmedabad, India, 2014. [Google Scholar]
- Allacker, K.; Debacker, W.; Delem, L.; De Nocker, L.; De Troyer, F.; Janssen, A. Environmental Profile of Building Elements (MMG report). Towards an Integrated Environmental Assessment of the Use of Materials in Buildings; OVAM: Mechelen, Belgium, 2013. [Google Scholar]
- Trigaux, D.; Wijnants, L.; De Troyer, F.; Allacker, K. Life cycle assessment and life cycle costing of road infrastructure in residential neighbourhoods. Int. J. Life Cycle Assess. 2016, 22, 1–14. [Google Scholar] [CrossRef]
- ASPEN (Ed.) ASPENINDEX Regio België—Nieuwbouw [ASPENINDEX Region. Belgium—New construction]; ASPEN INDEX: Antwerpen, Belgium, 2015. [Google Scholar]
- ASPEN (Ed.) ASPENINDEX Regio België—Ombouw [ASPENINDEX Region. Belgium—Renovation]; ASPEN INDEX: Antwerpen, Belgium, 2015. [Google Scholar]
- Spon Press (Ed.) Spon’s Architects’ and Builders’ Price Book, 140th ed.; AECOM: London, UK, 2015. [Google Scholar]
- Trigaux, D.; Allacker, K.; De Troyer, F. Model for the environmental impact assessment of neighbourhoods. In Environmental Impact I; WITpress: Southampton, UK, 2014; pp. 103–114. [Google Scholar]
- Vercaemst, P.; Vandenbroek, A.; Hoessels, M.; Witters, H.; Dijkmans, R. Beste Beschikbare Technieken (BBT) voor ziekenhuizen en andere verzorgingsinstellingen. Vito Mol. 2003. Available online: https://emis.vito.be/sites/emis.vito.be/files/pages/migrated/BBT_rapport_ziekenhuizen_volledig_rapport.pdf (accessed on 10 August 2017).
- Wagenaar, C. The Architecture of Hospitals; NAi Publishers: Rotterdam, Netherlands, 2006; p. 54. [Google Scholar]
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).