Climate Change and Healthcare Sustainability in the Agincourt Sub-District, Kruger to Canyons Biosphere Region, South Africa


Abstract
1. Introduction
2. Background
2.1. Climate Change and Health in Sub-Saharan Africa
2.2. Human Resources in Health
2.3. Health and Environmental Study Findings in Agincourt, South Africa
2.4. Significance and Limitations in the Field
3. Materials and Methods
3.1. Research Objective
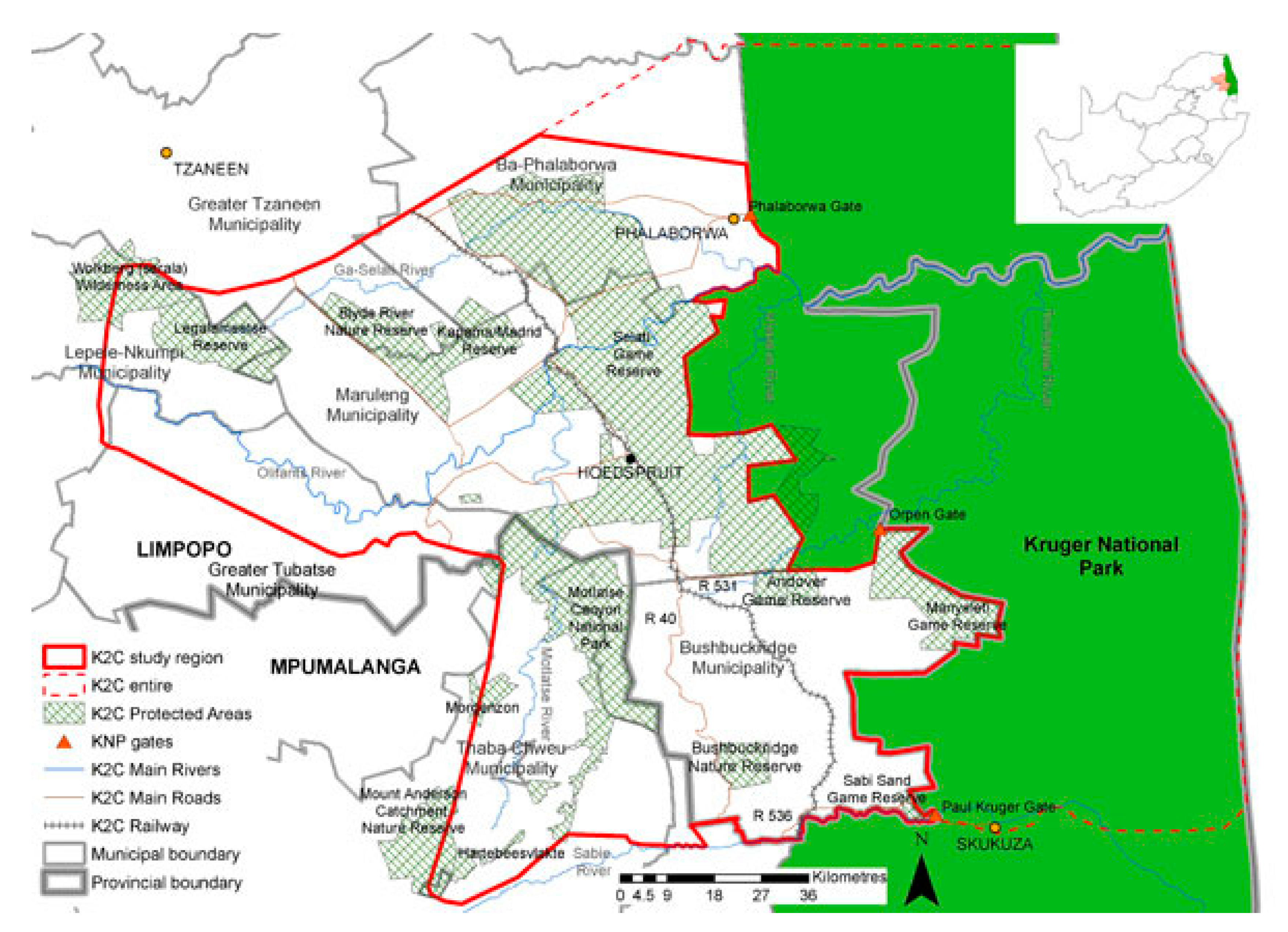
3.2. Case Study Setting
3.3. Data Sources
3.4. Data Analysis
3.5. Ethical Considerations
3.6. Study Limitations
4. Results
4.1. Facility, Infrastructure, and Accessibility Factors
4.2. Cross-Referrals and Professional Support
4.3. Professional Staff Component
4.4. Services Offered
4.5. Training Opportunities
4.6. Staff Shortages and Human Resources Needs
4.7. Perceived Effects of Changes in Climate at a Healthcare Facility Level
5. Discussion
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Martens, P. Health and Climate Change: Modelling the Impacts of Global Warming and Ozone Depletion; Earthscan Publications Ltd.: Abingdon, UK, 1998; ISBN-10 0415848806. [Google Scholar]
- Wright, C.Y.; Garland, R.M.; Norval, M.; Vogel, C. Human health impacts in a changing South African climate. S. Afr. Med. J. 2014, 104, 579–582. [Google Scholar] [CrossRef] [PubMed]
- The International Social Science Council and the United Nations Educational, Scientific and Cultural Organization. World Social Science Report 2013, Changing Global Environments; OEDC Publishing and UNESCO Publishing: Paris, France, 2013. [Google Scholar]
- Watts, N.; Adger, W.N.; Agnolucci, P.; Blackstock, J.; Byass, P.; Cai, W.; Chaytor, S.; Colbourn, T.; Collins, M.; Cooper, A.; et al. Health and climate change: Policy responses to protect public health. Lancet 2015, 386. [Google Scholar] [CrossRef]
- Wang, H.; Horton, R. Tackling climate change: The greatest opportunity for global health. Lancet 2015. [Google Scholar] [CrossRef]
- King, M. Health is a sustainable state. Lancet 1990, 336, 664–667. [Google Scholar] [CrossRef]
- Leary, N.; Adejuwon, J.; Barros, V.; Burton, I.; Kulkarni, J.; Lasco, R. (Eds.) Climate Change and Adaptation; The International START Secretariat, Earthscan: London, UK, 2008. [Google Scholar]
- Kedler, A.M. Rural Poverty Report 2001—The Challenge of Ending Rural Poverty; International Fund Agriculture Development; Oxford University Press: Oxford, UK, 2001. [Google Scholar]
- DARA. Climate vulnerability monitor. In A Guide to the Cold Calculus of a Hot Planet, 2nd ed.; DARA: Madrid, Spain, 2012. [Google Scholar]
- McMichael, A.J.; Campbell-Lendrum, D.H.; Corvalán, C.F.; Ebi, K.L.; Githeko, A.K.; Scheraga, J.D.; Woodward, A. Climate Change and Human Health: Risks and Responses; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Short, E.E.; Caminade, C.; Thomas, B.N. Climate change contribution to the emergence and re-emergence or parasitic diseases. Infect. Dis. 2017, 10. [Google Scholar] [CrossRef] [PubMed]
- Kassie, D.; Bourgaral, M.; Roger, F. Climate Change and Ebola Outbreaks: Are They Connected? In Proceedings of the Our Common Future under Climate Change Conference, Paris, France, 2–10 July 2015. [Google Scholar]
- Chan, M. The Impact of Climate Change on Human Health; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- McCoy, D.; Montgomery, H. Climate change and human survival. Br. Med. J. 2014, 348, 2351. [Google Scholar] [CrossRef] [PubMed]
- Friel, S.; Vlahov, D.; Buckley, R.M. No data, no problem, no action: Addressing urban health inequity in the 21st Century. J. Urban Health 2011, 88, 858–895. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.; Young, T.; Galloway, M.; Manyike, P.; Tucker, T. Responding to climate change in Southern Africa—The role of research. S. Afr. Med. J. 2011, 101, 820–822. [Google Scholar] [PubMed]
- McMichael, A.J. Climate change and human health. In Commonwealth Health Minister’s Update 2009; Commonwealth Secretariat, Ed.; Pro-Brook Publishing Ltd.: Woodbridge, UK, 2009; ISBN-10 0850928729. [Google Scholar]
- Fields, S. Continental divide: Why Africa’s climate change burden is greater. Environ. Health Perspect. 2005, 113, A534–A537. [Google Scholar] [CrossRef]
- The Joint United Nations Programme on HIV/AIDS. The Gap Report; Joint United Nations Programme on HIV/AIDS (UNAIDS): Geneva, Switzerland, 2014. [Google Scholar]
- Myers, J.E.; Rother, H.-A. Public health impact of and response to climate change in South Africa. In South African Health Review; Health Systems Trust: Durban, South Africa, 2012. [Google Scholar]
- Thompson, A.A.; Matamale, L.; Kharidza, S.D. Impact of climate change on children’s health in Limpopo province, South Africa. Int. J. Environ. Res. Public Health 2012, 9, 831–854. [Google Scholar] [CrossRef]
- Scovronick, N.; Armstrong, B. The impact of housing type on temperature-related mortality in South Africa, 1996–2015. Environ. Res. 2012, 113, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Talman, A.; Bolton, S.; Walson, J.A. Interactions between HIV/AIDS and the environment: Toward a syndemic framework. Am. J. Public Health 2013, 103, 253–261. [Google Scholar] [CrossRef]
- Egondi, T.; Kyobutungi, C.; Kovats, S.; Muindi, K.; Ettarh, R.; Rocklöv, J. Time-series analysis of weather and mortality patterns in Nairobi’s informal settlements. Glob. Health Action 2012, 5, 10. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Health Report 2006: Working Together for Health; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Dussault, G.; Franceschini, M.C. Not enough there, too many here: Understanding geographical imbalances in the distribution of the health workforce. Hum. Resour. Health 2006, 4, 12. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Zurn, P.; Diallo, K.; Dal Poz, M.R. Uses of population census data for monitoring geographical imbalance in the health workforce: Snapshots from three developing countries. Int. J. Equity Health 2003, 2, 11. [Google Scholar] [CrossRef] [PubMed]
- Habte, D.; Dussault, G.; Dovlo, D. Challenges confronting the health workforce in sub-Saharan Africa. World Hosp. Health Serv. J. 2004, 40, 23–26, 40–41. [Google Scholar]
- Zurn, P.; Dal Poz, M.R.; Stilwell, B.; Adams, O. Imbalance in the health workforce. Hum. Resour. Health 2004, 2, 13. [Google Scholar] [CrossRef] [PubMed]
- Ricketts, T.; Hart, L.; Pirani, M. How many rural doctors do we have? J. Rural Health 2000, 16, 198–207. [Google Scholar] [CrossRef]
- Ataguba, J.E.-O.; McIntyre, D. Who benefits from health services in South Africa? Health Econ. Policy Law 2013, 8, 21–46. [Google Scholar] [CrossRef]
- National Department of Health, Republic of South Africa. Human Resources for Health South Africa: HRH Strategy for the Health Sector: 2012/13 to 2016/17; National Department of Health: Pretoria, South Africa, 2011.
- Hamilton, K.; Yau, J. The Global Tug-of-War for Health Care Workers. Migration Information Source: Migration Policy Institute, 2004. Available online: https://www.migrationpolicy.org/article/global-tug-war-health-care-workers (accessed on 14 December 2017).
- George, G.; Quinlan, T.; Reardon, C. Human Resources for Health: A Needs and Gaps Analysis of HRH in South Africa; Health Economics and HIV & AIDS Research Division (HEARD): Durban, South Africa, 2009. [Google Scholar]
- Hugo, J.; Allan, L. Doctors for Tomorrow: Family Medicine in South Africa; NISC (Pty) Ltd.: Grahamstown, South Africa, 2008. [Google Scholar]
- Goudge, J.; Gilson, L.; Russell, S.; Gumede, T.; Mills, A. Affordability, availability and acceptability barriers to health care for the chronically ill: Longitudinal case studies from South Africa. BMC Health Serv. Res. 2009, 9, 75. [Google Scholar] [CrossRef]
- Hatcher, A.M.; Onah, M.; Kornik, S.; Peacocke, J.; Reid, S. Placement, support, and retention of health professionals: National, cross-sectional findings from medical and dental community service officers in South Africa. Hum. Resour. Health 2014, 12, 14. [Google Scholar] [CrossRef] [PubMed]
- Kabudula, C.W.; Tollman, S.; Mee, P.; Ngobeni, S.; Silaule, B.; Gómez-Olivé, F.X.; Collinson, M.; Kahn, K.; Byass, P. Two decades of mortality change in rural northeast South Africa. Glob. Health Action 2014, 7, 25596. [Google Scholar] [CrossRef] [PubMed]
- Statistics South Africa. Census 2011. Available online: http://www.statssa.gov.za/?page_id=3836 (accessed on 26 June 2017).
- Tollman, S.M.; Kahn, K.; Sartorius, B.; Collinson, M.A.; Clark, S.J.; Garenne, M.L. Implications of mortality transition for primary health care in rural South Africa: A population-based surveillance study. Lancet 2008, 372, 893–901. [Google Scholar] [CrossRef]
- Kimani-Murage, E.W.; Kahn, K.; Pettifor, J.M.; Tollman, S.M.; Klipstein-Grobusch, K.; Norris, S.A. Predictors of adolescent weight status and central obesity in rural South Africa. Public Health Nutr. 2011, 14, 1114–1122. [Google Scholar] [CrossRef] [PubMed]
- Byass, P.; Collinson, M.A.; Kabudula, C.; Gómez-Olivé, F.X.; Wagner, R.G.; Ngobeni, S.; Silaule, B.; Mee, P.; Coetzee, M.; Twine, W.; et al. The long road to elimination: Malaria mortality in a South African cohort over 21 years old. Glob. Health Epidemiol. Genom. 2017, 2. [Google Scholar] [CrossRef] [PubMed]
- Byass, P. Climate change and population health in Africa: Where are the scientists? Glob. Health Action 2009, 2, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Hunter, L.M.; Twine, W.; Johnson, A. Adult mortality and natural resource use in rural South Africa: Evidence from the Agincourt health and demographic surveillance site. Soc. Natl. Resour. 2011, 24, 256–275. [Google Scholar] [CrossRef]
- Matsika, R.; Erasmus, B.F.N.; Twine, W.C. A tale of two villages: Assessing the dynamics of fuelwood supply in communal landscapes in South Africa. Environ. Conserv. 2012, 40, 71–83. [Google Scholar] [CrossRef]
- Williams, J.R.; Schatz, E.; Clark, B.D.; Collinson, M.A.; Clark, S.J.; Menken, J.; Kahn, K.; Tollman, S.M. Improving public health training and research capacity in Africa: A replicable model for linking training to health and socio-demographic surveillance data. Glob. Health Action 2010, 3, 5287. [Google Scholar] [CrossRef]
- Thorogood, M.; Connor, M.D.; Tollman, S.M.; Lewando-Hundt, G.; Fowkes, G.; Marsh, J. A cross-sectional study of vascular risk factors in a rural South African population: Data from the Southern African stroke prevention initiative (SASPI). BMC Public Health 2007, 7, 326. [Google Scholar] [CrossRef]
- Hunter, L.M.; Twine, W.; Patterson, L. “Locusts are now our beef”: Adult mortality and household dietary use of local environmental resources in rural South Africa. Scand. J. Public Health 2007, 35, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Twine, W.; Hunter, L. Aids Mortality and the Role of Natural Resources in Household Food Security in a Rural District in South Africa. Policy Brief; International Food Policy Research Institute: Washington, DC, USA, 2008. [Google Scholar]
- Bradshaw, D.; Nannan, N.; Laubscher, R.; Groenewald, P.; Joubert, J.; Nojilana, B.; Norman, R.; Pieterse, D.; Schneider, M. South African National Burden of Disease Study 2000: Estimates of Provincial Mortality; Medical Research Council: Cape Town, South Africa, 2004. [Google Scholar]
- Myers, J.; Young, T.; Galloway, M.; Manyike, P.; Tucker, T. A public health approach to the impact of climate change on health in Southern Africa—Identifying priority modifiable risks. S. Afr. Med. J. 2011, 101, 817–820. [Google Scholar] [PubMed]
- Stimson, G.V.; Fitch, C.; Rhodes, T. The Rapid Assessment and Response Guide on Injecting Drug Use (IDU–RAR). Social Change and Mental Health; World Health Organization: London, UK, 1998. [Google Scholar]
- Stimson, G.V.; Fitch, C.; Rhodes, T. Rapid Assessment and Response Guide on Injecting Drug Use: Draft for Field Testing; World Health Organization/The Joint United Nations Programme on HIV/AIDS: Geneva, Switzerland, 1998. [Google Scholar]
- Stimson, G.V.; Fitch, C.; Rhodes, T. The Rapid Assessment and Response Guide on Substance Use and Sexual Risk Behaviour: Draft for Field Testing; World Health Organization/The Joint United Nations Programme on HIV/AIDS: Geneva, Switzerland, 1998. [Google Scholar]
- Stimson, G.V.; Fitch, C.; Rhodes, T. The Rapid Assessment and Response Guide on Psychoactive Substance Use and Especially Vulnerable Young People: Draft for Field Testing; World Health Organization/The Joint United Nations Programme on HIV/AIDS: Geneva, Switzerland, 1998. [Google Scholar]
- Rhodes, T.; Fitch, C.; Stimson, G.V.; Suresh Kumar, M. Rapid assessment in the drugs field. Int. J. Drug Policy 2000, 11, 1–11. [Google Scholar] [CrossRef]
- Braam, R.; Verbraeck, H.; Trautmann, F. Rapid Assessment and Response (RAR) on Problematic Substance Use among Refugees, Asylum Seekers and Illegal Immigrants. A Manual, 2nd extended ed.; Landschaftsverb and Westfalen-Lippe: Münster, Germany, 2005. [Google Scholar]
- Trautmann, F. Rapid assessment and response (RAR) methodology. In Empowering NGOs in Drug Demand Reduction; Franke, S., Sande, M., Eds.; Care: Vienna, Austria, 2004. [Google Scholar]
- United Nations. Sustainable Development Goals: 17 Goals to Transform the World. Available online: http://www.un.org/sustainabledevelopment/ (accessed on 25 January 2018).
- Kruger to Canyons Biosphere Region. Available online: http://www.kruger2canyons.org/index.html (accessed on 15 December 2017).
- Babbie, E.; Mouton, J. The Practice of Social Research, 13th ed.; Oxford University Press: Oxford, UK, 2012; ISBN-10 1133049796. [Google Scholar]
- Breakwell, G.M.; Smith, J.A.; Wright, D.B. Research Methods in Psychology, 4th ed.; SAGE Publications Ltd.: London, UK, 2012; ISBN-10 0857022644. [Google Scholar]
- World Health Organization. Evolution of the National Adolescent-Friendly Clinic Initiative in South Africa; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Discussion Document: South Africa’s Intended Nationally Determined Contribution, 2015. ISBN 978-0-621-41180-5. Available online: https://www.environment.gov.za/sites/default/files/docs/sanational_determinedcontribution.pdf (accessed on 5 November 2018).
- Niang, I.; Ruppel, O.C.; Abdrabo, M.A.; Essel, A.; Lennard, C.; Padgham, J.; Urquhart, P. Africa. In Climate Change 2014: Impacts, Adaptation, and Vulnerability. Part B: Regional Aspects. Contribution of Working Group II to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; Barros, V.R., Field, C.B., Dokken, D.J., Mastrandrea, M.D., Mach, K.J., Bilir, T.E., Chatterjee, M., Ebi, K.L., Estrada, Y.O., Genova, R.C., et al., Eds.; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2014; pp. 1199–1265. [Google Scholar]
- National Planning Commission. National Planning Commission. Our Future—Make It Work: National Development Plan 2030; The Presidency: Pretoria, South Africa, 2011. Available online: https://www.gov.za/sites/default/files/NDP-2030-Our-future-make-it-work_r.pdf (accessed on 5 November 2018).
- National Department of Health. National Core Standards for Health Establishments in South Africa; National Department of Health: Tshwane, South Africa, 2011.
- Shepherd, P.; Hinsch, M.; Fourie, A.; Dupper, E. Variability in rainfall, and how to manage it. Civ. Eng. 2017, 25, 8–9. [Google Scholar]
- Diaz, J.; Linares, C.; Tobías, A. Impact of extreme temperatures on daily mortality in Madrid (Spain) among the 45–64 age-group. Int. J. Biometeorol. 2006, 50, 342–348. [Google Scholar] [CrossRef] [PubMed]
- Gasparrini, A.; Armstrong, B. The impact of heat waves on mortality. Epidemiology 2011, 22, 68–73. [Google Scholar] [CrossRef]
- Martineau, A.R.; Nhamoyebonde, S.; Oni, T.; Rangaka, M.X.; Marais, S.; Bangani, N.; Tsekela, R.; Bashe, L.; de Azevedo, V.; Caldwell, J.; et al. Reciprocal seasonal variation in vitamin D status and tuberculosis notifications in Cape Town, South Africa. Proc. Natl. Acad. Sci. USA 2011, 108, 19013–19017. [Google Scholar] [CrossRef]
- Davis, R.E.; Rossier, C.E.; Enfield, K.B. The impact of weather on influenza and pneumonia mortality in New York City, 1975–2002: A retrospective study. PLoS ONE 2012, 7. [Google Scholar] [CrossRef]
- Tinling, M.; Ralston, M.; Thie, L.; Fitz-Simons, T.; Choudry, M.; Ali, S.; Shehee, M.; Barros, N.; Dang, G. North Carolina Climate-Related Health Indicators: Cancer. Occupational and Environmental Health 2013. Available online: http://epi.publichealth.nc.gov/oee/climate/ncclimateandcancer_051413.pdf (accessed on 6 January 2019).
- Lichtman, J.H.; Jones, S.B.; Wang, Y.; Leifheit-Limson, E.C.; Goldstein, L.B. Seasonal variation in 30-day mortality after stroke: Teaching versus nonteaching hospitals. Stroke 2013, 44, 531–533. [Google Scholar] [CrossRef]
- Madrigano, J.; Mittleman, M.A.; Baccarelli, A.; Goldberg, R.; Melly, S.; von Klot, S.; Schwartz, J. Temperature, myocardial infarction, and mortality: Effect modification by individual and area-level characteristics. Epidemiology 2013, 24, 439–446. [Google Scholar] [CrossRef]
- Lin, Y.-K.; Chang, C.-K.; Wang, Y.-C.; Ho, T.-J. Acute and prolonged adverse effects of temperature on mortality from cardiovascular diseases. PLoS ONE 2013, 8. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Peng, L.; Kan, H.; Xu, J.; Chen, R.; Liu, Y.; Wang, W. Effects of meteorological factors on daily hospital admissions for asthma in adults: A time series analysis. PLoS ONE 2014, 9. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.J.; Wang, X.; Zheng, D.N.; Robinson, T.; Hong, D.Q.; Richtering, S.; Leong, T.H.; Salam, A.; Anderson, C.; Hackett, M.I. Air pressure, humidity and stroke occurrence: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2016, 13. [Google Scholar] [CrossRef] [PubMed]
- Honing, A.; Eliahou, R.; Pikkel, Y.Y.; Leker, R.R. Drops in barometric pressure are associated with deep intercerebral hemorrhage. J. Stroke Cerebrovasc. Dis. 2006, 25, 872–876. [Google Scholar] [CrossRef] [PubMed]
- Venero, S.J.; González, F.J.; Suárez, R.; Fabré, D.; Fernández, H.M. Epidemiology of asthma mortality in Cuba and its relation to climate, 1989 to 2003. Medicc Rev. 2008, 10, 24–29. [Google Scholar] [PubMed]
- Horn, L.M.; Hajat, A.; Sheppard, L.; Quinn, C.; Colborn, J.; Zermoglio, M.F.; Gudo, E.S.; Marrufo, T.; Ebi, K.L. Association between percipitaiton and diarrheal diesase in Mozambique. Int. J. Environ. Res. Public Health 2018, 15, 709. [Google Scholar] [CrossRef]
- Peterson, A.T. Shifting suitability for malaria vectors across Africa with warming climates. BMC Infect. Dis. 2009, 9, 59. [Google Scholar] [CrossRef]
- Rauf, S.; Bakhsh, K.; Abbas, A.; Hassan, S.; Ali, A.; Kächele, H. How hard they hit? Perception, adaptation and public health implications of heat waves in urban and peri-urban Pakistan. Environ. Sci. Pollut. Res. 2017, 24, 10630–10639. [Google Scholar] [CrossRef]
- Wright, C. Climate change, human health and the role of environmental health practitioners. S. Afr. Med. J. 2014, 104, 8. [Google Scholar] [CrossRef]
- Stead, J.G.; Stead, W.E. Sustainable Strategic Management, 2nd ed.; Green Leaf Publishing Limited: Sheffield, UK, 2014. [Google Scholar]
- Smith, K.R.; Woodward, A.; Campbell-Lendrum, D.; Chadee, D.D.; Honda, Y.; Liu, Q.; Olwoch, J.M.; Revich, B.; Sauerborn, R. Human health: Impacts, adaptation, and co-benefits. In Climate Change 2014: Impacts, Adaptation, and Vulnerability. Part A: Global and Sectoral Aspects. Contribution of Working Group II to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; Field, C.B., Barros, V.R., Dokken, D.J., Mach, K.J., Mastrandrea, M.D., Bilir, T.E., Chatterjee, M., Ebi, K.L., Estrada, Y.O., Genova, R.C., et al., Eds.; Cambridge University Press: Cambridge, UK; New York, NY, USA, 2014; pp. 709–754. [Google Scholar]
- Holden, E.; Linnerud, K.; Banister, D.; Schwanitz, V.J.; Wierling, A. The Imperatives of Sustainable Development: Needs, Justice, Limits; Routledge, Taylor & Francis Group: London, UK, 2018; ISBN 978-1138714267. [Google Scholar]
- Hodson, M.; Marvin, S. After Sustainable Cities? Routledge: London, UK, 2014; ISBN 978-0415659871. [Google Scholar]
- Berman, P.A. Health sector reform: Making health development sustainable. Health Policy 1995, 32, 13–28. [Google Scholar] [CrossRef]
- Guidotti, T.L. Health and Sustainability: An Introduction; Oxford University Press: New York, NY, USA, 2015. [Google Scholar]
- Bell, E. Readying health services for climate change: A policy framework for regional development. Am. J. Public Health 2011, 101, 804–813. [Google Scholar] [CrossRef] [PubMed]
- McMichael, A.J.; Friel, S.; Nyong, A.; Corvalan, C. Global environmental change and health: Impacts, inequalities, and the health sector. Br. Med. J. 2008, 336, 191–194. [Google Scholar] [CrossRef] [PubMed]
- Kotze, P.M.J. Wanvoeding: ’n Kontekstuele Benadering. Master’s Dissertation, University of South Africa, Pretoria, South Africa, 1990. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Facility | No. of Hours Open | No. of Days Open per Week | Catchement Population | Total Patient Headcount per Month | Adequate Patient Seating | Planned Patient Transport | Facility has Own Entrance | Accessabile by a Good Road Infrastructure | Facility has Running Water | Closest Airport | Computer/IT Access | Secure Patient Filing System |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| * PHC1 | 8 | 7 | 11,821 | 3202–3365 | No | No | No, via casualty | Yes | Yes | Kruger MP Int. Airport | Yes | Yes |
| * PHC2 | 8 | 7 | 13,270 | 2956–3134 | No | No | No, via casualty | No | Yes | Kruger MP Int. Airport | Yes | Yes |
| * PHC3 | 8 | 7 | 9967 | 2436–2704 | No | No | No, via casualty | No | Yes | Kruger MP Int. Airport | Yes | No |
| * PHC4 | 8 | 7 | 9958 | 2178–2519 | Yes | No | No, via casualty | Yes | Yes | Kruger MP Int. Airport | Yes | Yes |
| * PHC5 | 8 | 7 | Unknown | 2098–2173 | No | No | No, via casualty | No | Yes | Kruger MP Int. Airport | Yes | Yes |
| * PHC6 | 8 | 7 | Unknown | 2084–2171 | No | No | No, via casualty | No, need 4 × 4 | No | Kruger MP Int. Airport | Yes | No |
| ** CHC1 | 24 | 7 | Unknown | 4200–5400 | Yes | No | No | Yes | Yes | Kruger MP Int. Airport | Yes | Yes |
| ** CHC2 | 8 | 7 | Unknown | 2000–3050 | Yes | No | No | No | Yes | Kruger MP Int. Airport | Yes | Yes |
| Facility | District Hospital Support | Easy Referral to District Hospital | Easy Referral to CHC | Telephonic Access to Doctors | Laboratory Services | Reliability of District and Provincial Management Support |
|---|---|---|---|---|---|---|
| PHC1 | Yes, Matikwane | Mostly | No | Mostly | Yes (Matikwane NHLS) | Mostly |
| PHC2 | Yes, Matikwane | Yes | No | Yes | Yes (Matikwane NHLS) | Yes |
| PHC3 | Yes, Matikwane | Yes | Yes | Yes | Yes (Matikwane NHLS) | Yes |
| PHC4 | Yes, Matikwane | Mostly | No | Sometimes | Yes (Matikwane NHLS) | Mostly |
| PHC5 | Yes, Matikwane | Mostly | Mostly | Yes | Yes (Matikwane NHLS) | Yes |
| PHC6 | Yes, Mapulane | Mostly | Mostly | Yes | Yes (Matikwane NHLS) | Mostly |
| CHC1 | N/A | Mostly | N/A | Rarely | Yes | Mostly |
| CHC2 | N/A | Mostly | N/A | Yes | Yes | Mostly |
| Facility | No. of Professional Nurses (PN) & Time Spent Consulting | No. of Enrolled Nurses (EN) & Time Spent Consulting | No. of Enrolled Nursing Assistants (ENA) & Time Spent Consulting | No. of Consulting/Sessional Medical Doctors & Time Spent Consulting | CEO/Facility Manager | No. of Data Capturers (Full-Time) | No. of Administrative Officers (Full-Time) | No. of Physio-Therapists (Sessional) | No. of Occupational Therapists (Sessional/Full-Time) | No. of Speech and Hearing Therapists (Sessional) |
|---|---|---|---|---|---|---|---|---|---|---|
| PHC1 | 5 20 min | 2 5 min | 1 5 min | 1 consulting 15 min | 1 PN | 1 | 1 | 1 | 1 sessional | 0 |
| PHC2 | 6 17.5 min | 2 5 min | 1 5 min | 1 consulting 20 min | 1 PN | 1 | 0 | 1 | 0 | 0 |
| PHC3 | 6 15 min | 2 4 min | 0 0 min | 1 consulting 10 min | 0 | 1 | 0 | 1 | 1 sessional | 1 |
| PHC4 | 6 22.5min | 5 12.5 min | 0 0 min | 0 0 min | 0 | 1 | 0 | 1 | 0 | 0 |
| PHC5 | 5 10 min | 4 7.5 min | 0 0 min | 0 0 min | 0 | 1 | 0 | 2 | 2 (1 sessional & 1 full-time) | 0 |
| PHC6 | 4 30 min | 2 5 min | 0 0 min | 0 0 min | 0 | 1 | 0 | 0 | 0 | 0 |
| CHC1 | 16 10 min | 4 50 min | 2 7 min | 2 sessional 15 min | 1 PN | 1 | 3 | 0 | 0 | 0 |
| CHC2 | 6 10 min | 1 5 min | 1 5 min | 2 full-time 1 consulting 15–20 min | 1 PN | 3 | 4 | 0 | 0 | 0 |
| Facility | No. of Pharmacists (Full-Time/Sessional/) | No. of Basic Pharmacist Assistants (Full-Time) | No. of Social Workers (Full-Time/Sessional) | No. of Environmental Health Practitioners (Sessional) | Outreach Health Promotors (Sessional) | No. of Community Outreach Workers (Home Based Carers) (Full-Time) | No. of Community Liason Offiers (Full-Time) | No. of HCT Counsellors (Full-Time/Sessional) | No. of Cleaners (Full-Time) | No. of Security Guards (Full-Time) |
|---|---|---|---|---|---|---|---|---|---|---|
| PHC1 | 0 | 0 | 0 | 1 | 0 | 12 | 0 | 1 | 2 | 6 |
| PHC2 | 0 | 0 | 0 | 1 | 0 | 20 | 0 | 2 | 2 | 6 |
| PHC3 | 0 | 0 | 0 | 1 | 0 | 23 | 0 | 3 | 1 | 6 |
| PHC4 | 0 | 0 | 1 full-time | 0 | 0 | 29 | 0 | 2 | 2 | 6 |
| PHC5 | 0 | 0 | 0 | 1 | 1 | unknown | 24 | 2 | 2 | 6 |
| PHC6 | 0 | 0 | 0 | 0 | 1 | unknown | 0 | 2 | 2 | 6 |
| CHC1 | 0 | 0 | 2 full-time | 1 | 0 | 20 | 0 | 4 | 3 | 6 |
| CHC2 | 1 full-time | 1 full-time | 0 | 0 | 0 | unknown | 0 | 6 | 1 | 4 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
dos Santos, M.; Howard, D.; Kruger, P.; Banos, A.; Kornik, S. Climate Change and Healthcare Sustainability in the Agincourt Sub-District, Kruger to Canyons Biosphere Region, South Africa. Sustainability 2019, 11, 496. https://doi.org/10.3390/su11020496
dos Santos M, Howard D, Kruger P, Banos A, Kornik S. Climate Change and Healthcare Sustainability in the Agincourt Sub-District, Kruger to Canyons Biosphere Region, South Africa. Sustainability. 2019; 11(2):496. https://doi.org/10.3390/su11020496
Chicago/Turabian Styledos Santos, Monika, David Howard, Pieter Kruger, Arnaud Banos, and Saul Kornik. 2019. "Climate Change and Healthcare Sustainability in the Agincourt Sub-District, Kruger to Canyons Biosphere Region, South Africa" Sustainability 11, no. 2: 496. https://doi.org/10.3390/su11020496
APA Styledos Santos, M., Howard, D., Kruger, P., Banos, A., & Kornik, S. (2019). Climate Change and Healthcare Sustainability in the Agincourt Sub-District, Kruger to Canyons Biosphere Region, South Africa. Sustainability, 11(2), 496. https://doi.org/10.3390/su11020496