A Bibliometric Analysis and Visualization of Medical Big Data Research





Abstract
1. Introduction
2. Data and Methods
3. Results
3.1. The Current Status of MBD Study
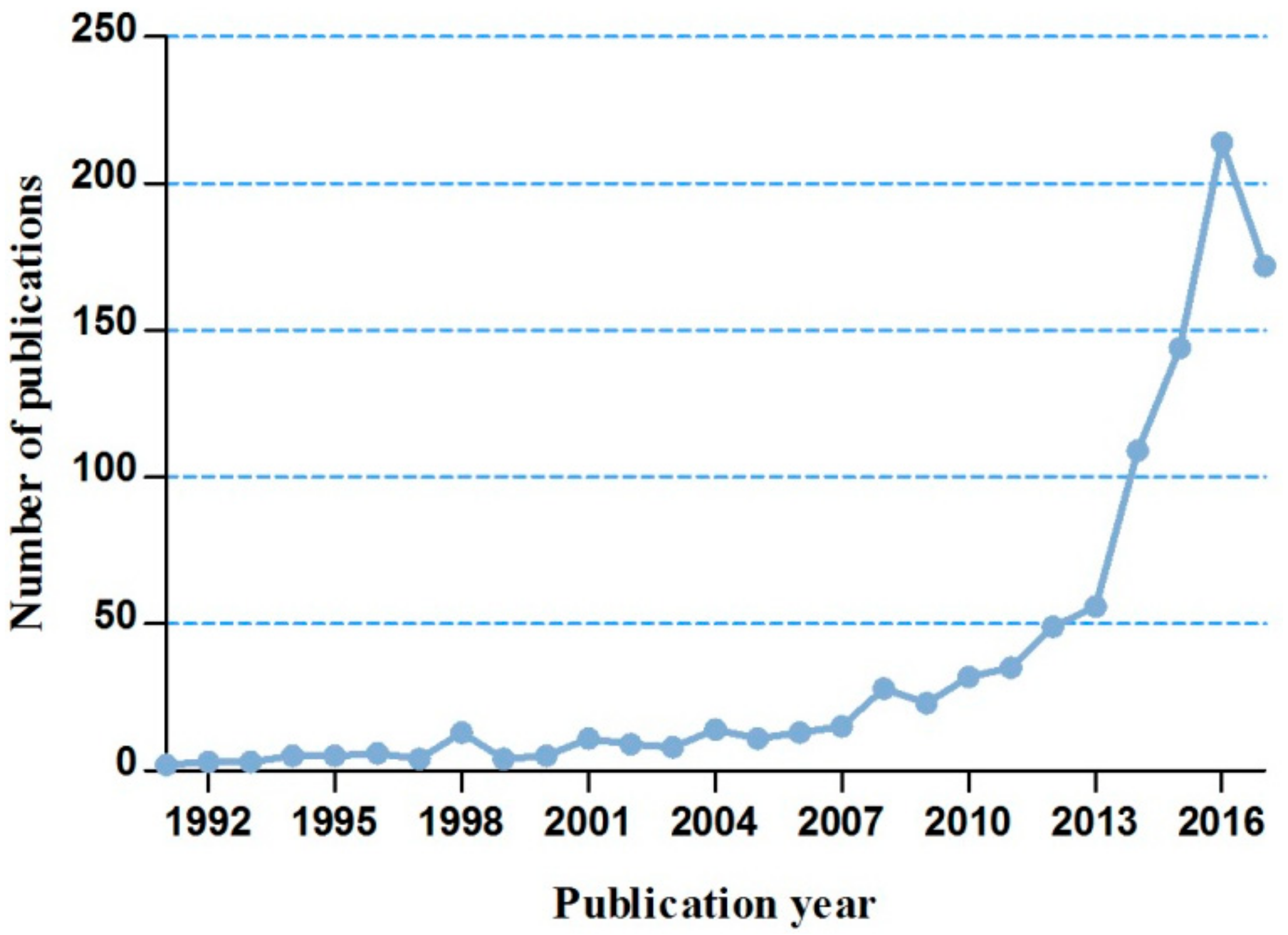
3.1.1. The Annual Trends of MBD-Related Publications
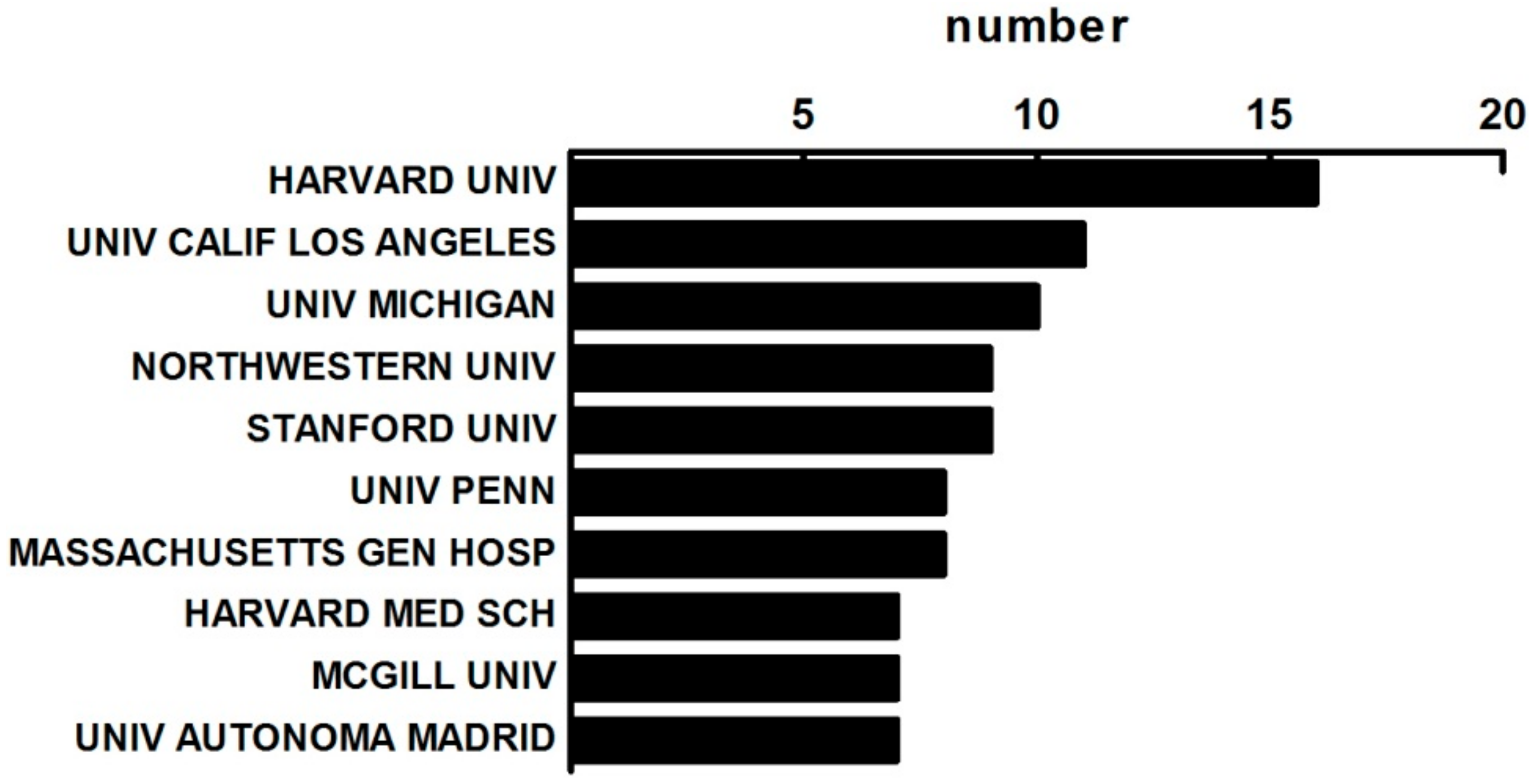
3.1.2. The Distribution of Institutes on MBD Study
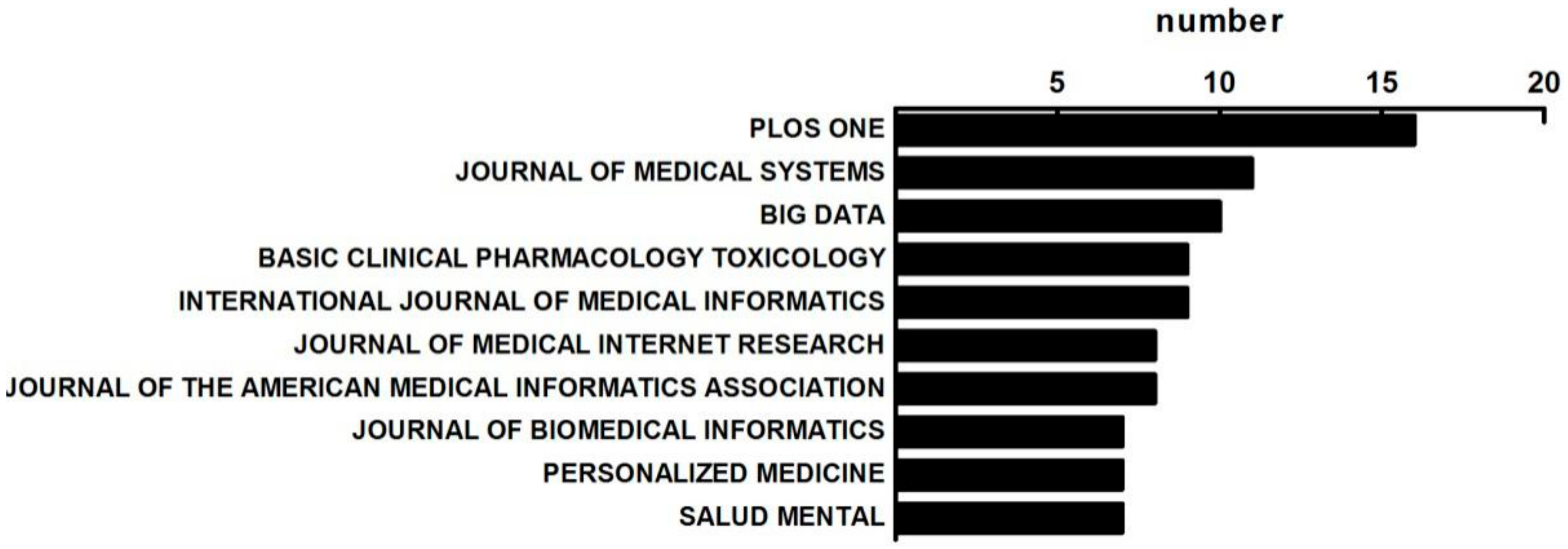
3.1.3. The Distribution of Published Journals on MBD Study
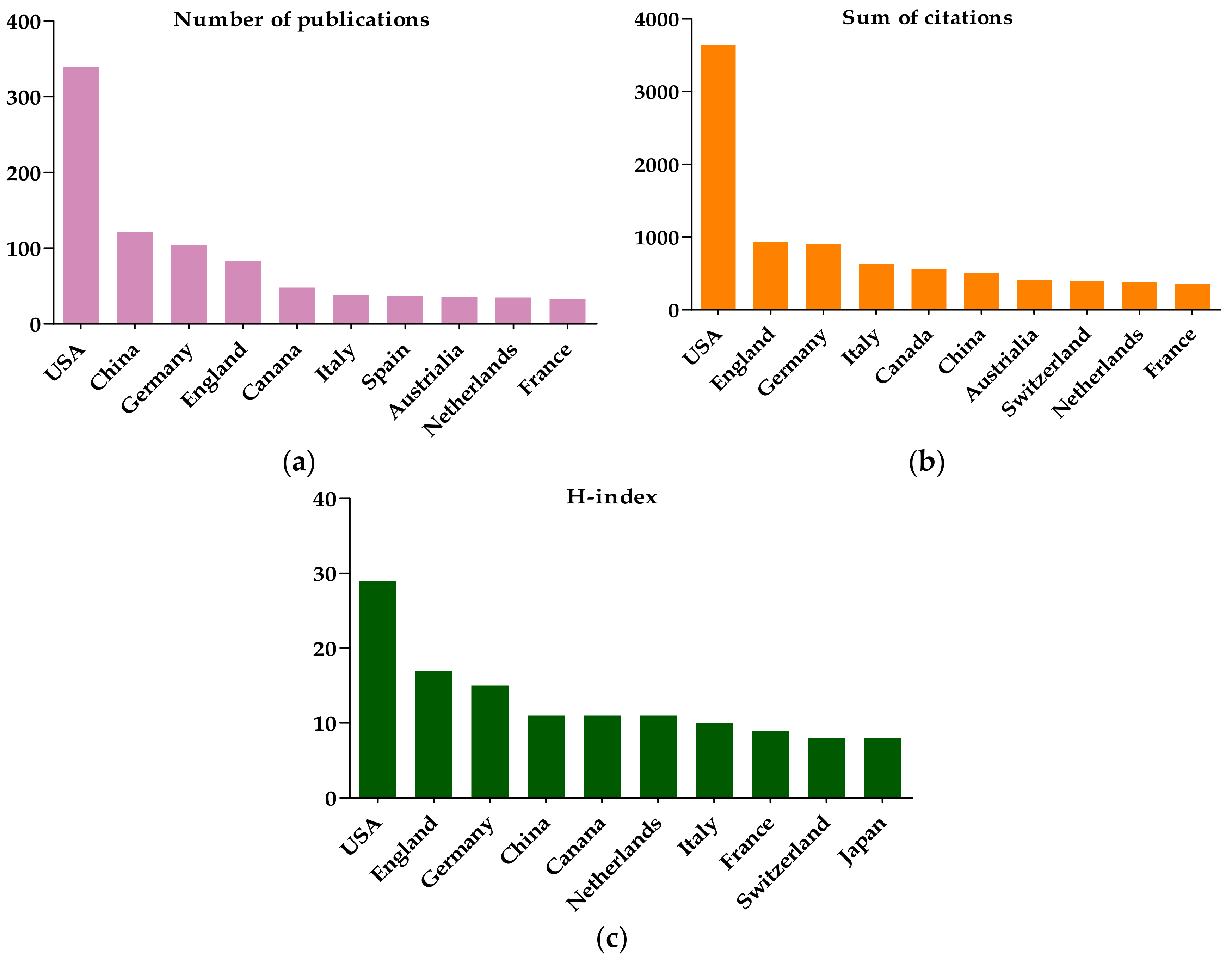
3.1.4. The Citation and H-Index Analysis
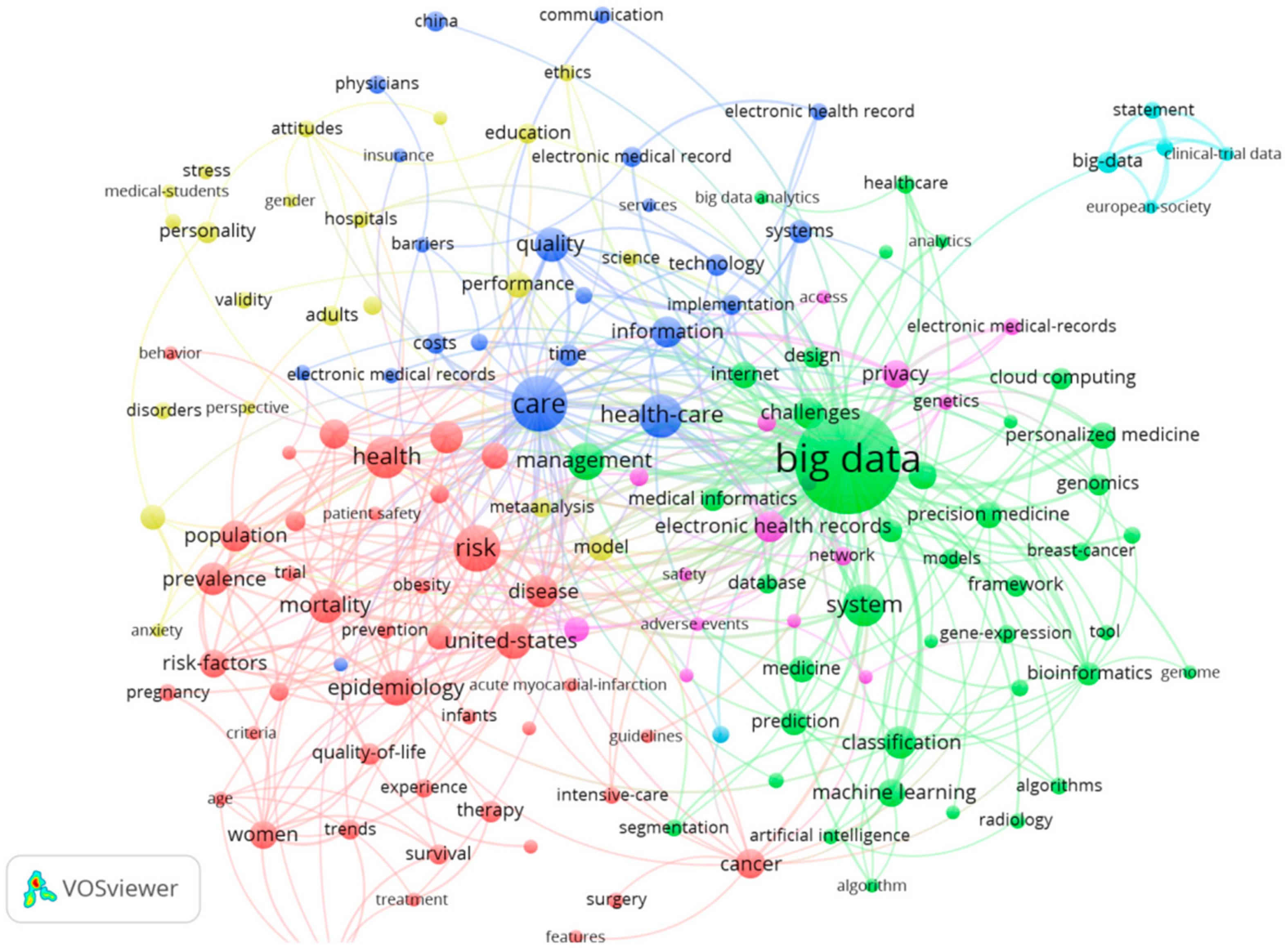
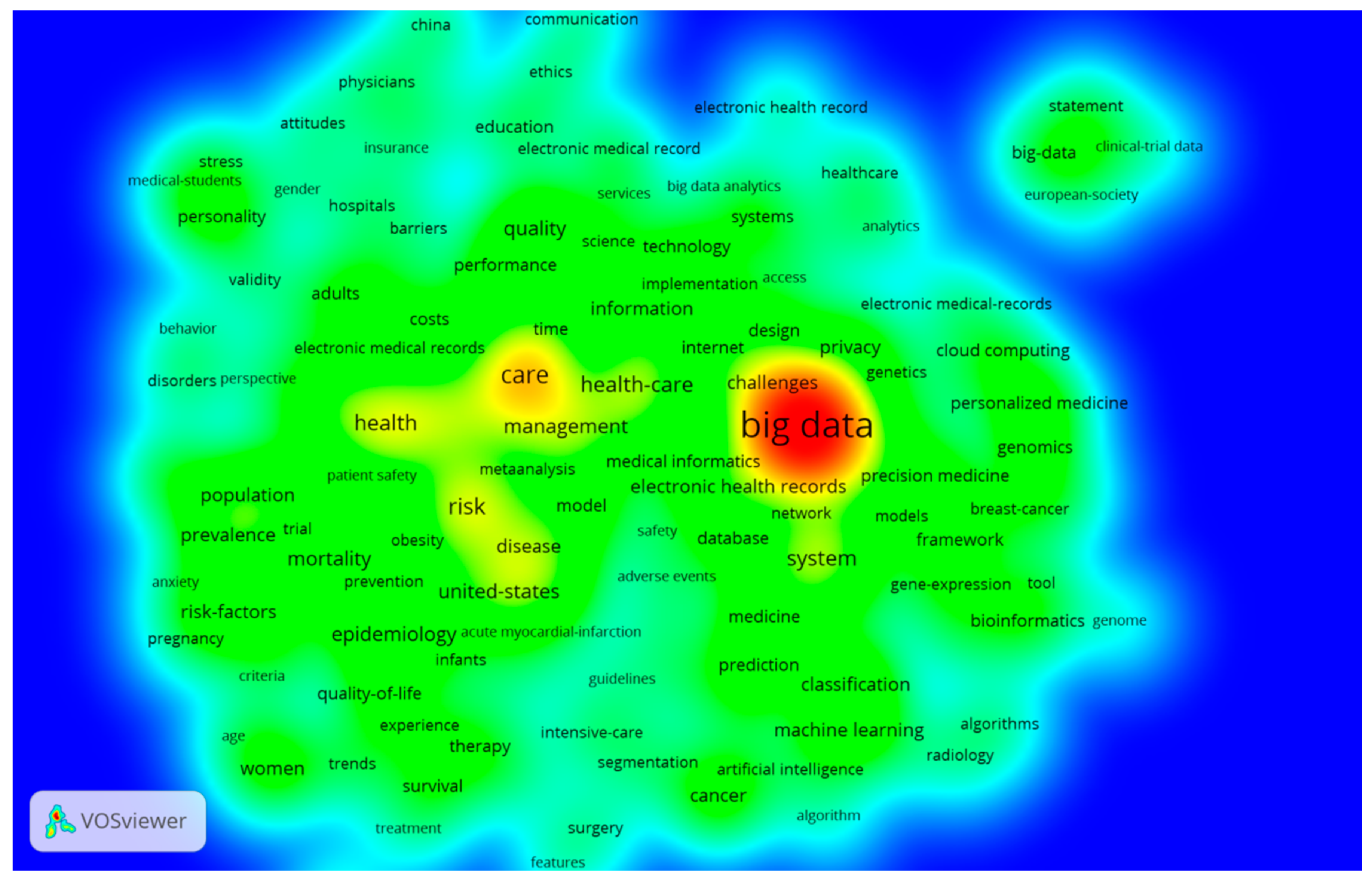
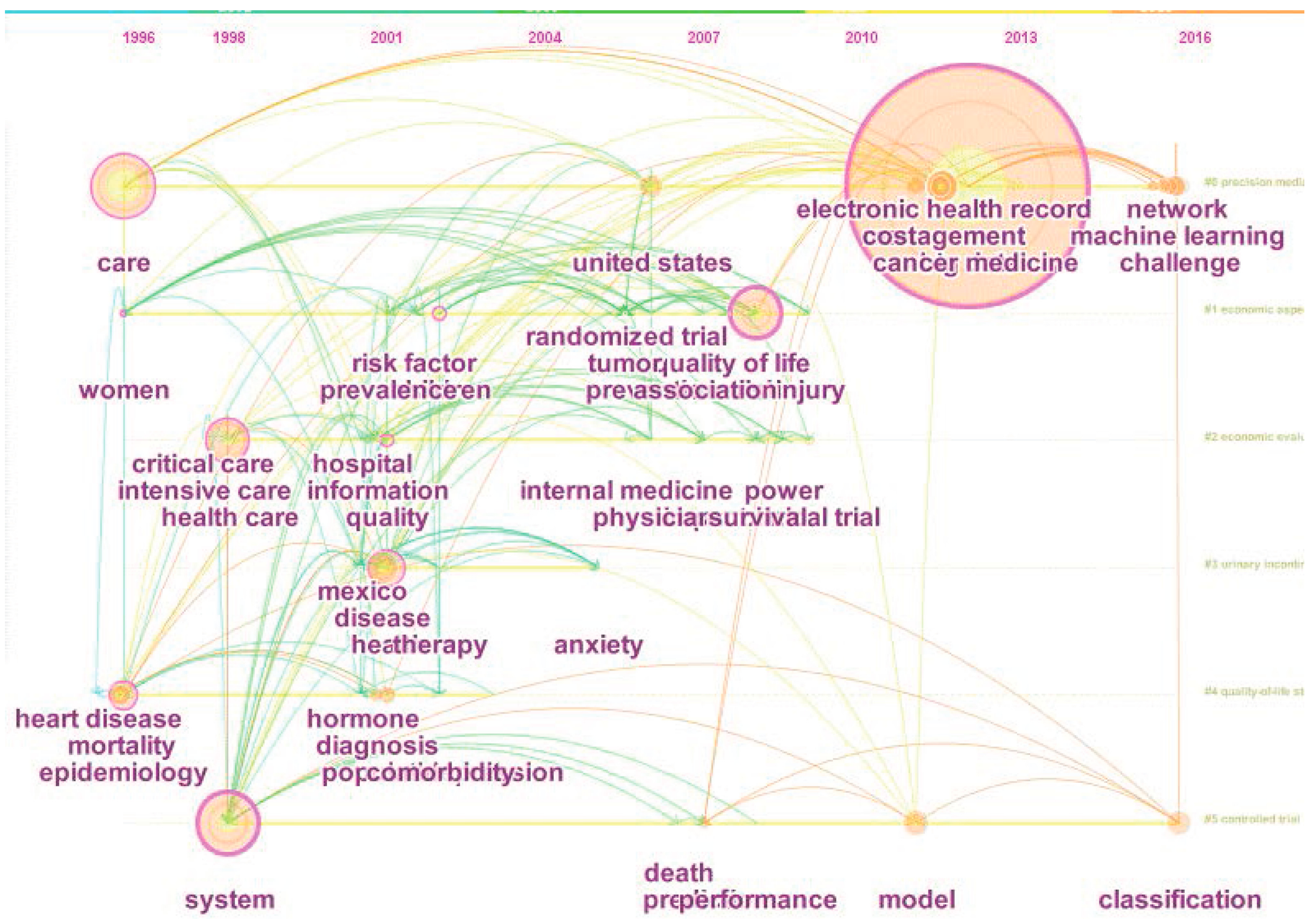
3.2. The Keywords Analysis of Research Hotspots on MBD Study
3.3. The Co-Authorship Analysis on MBD
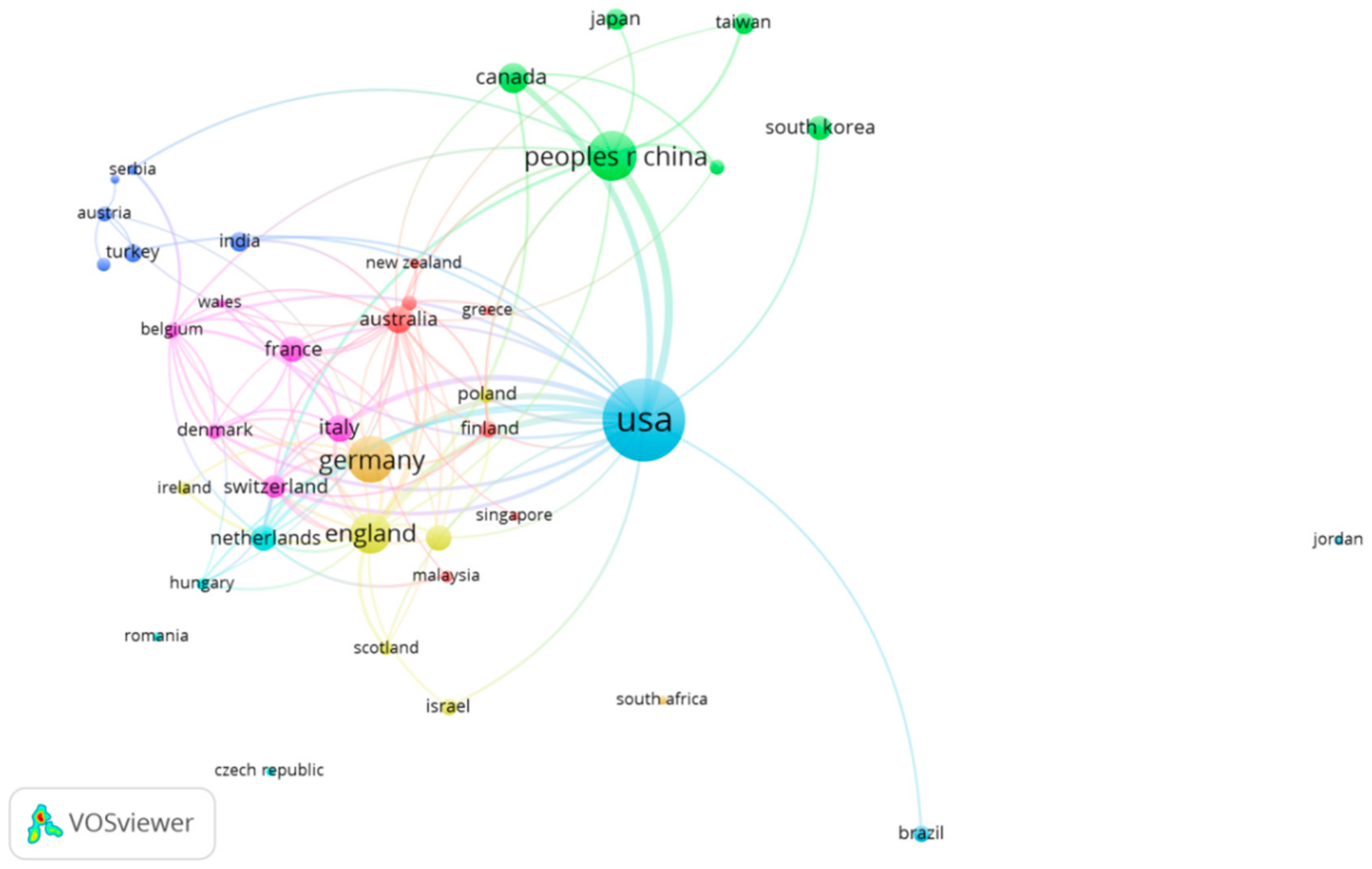
3.3.1. The Country Co-Authorship Analysis
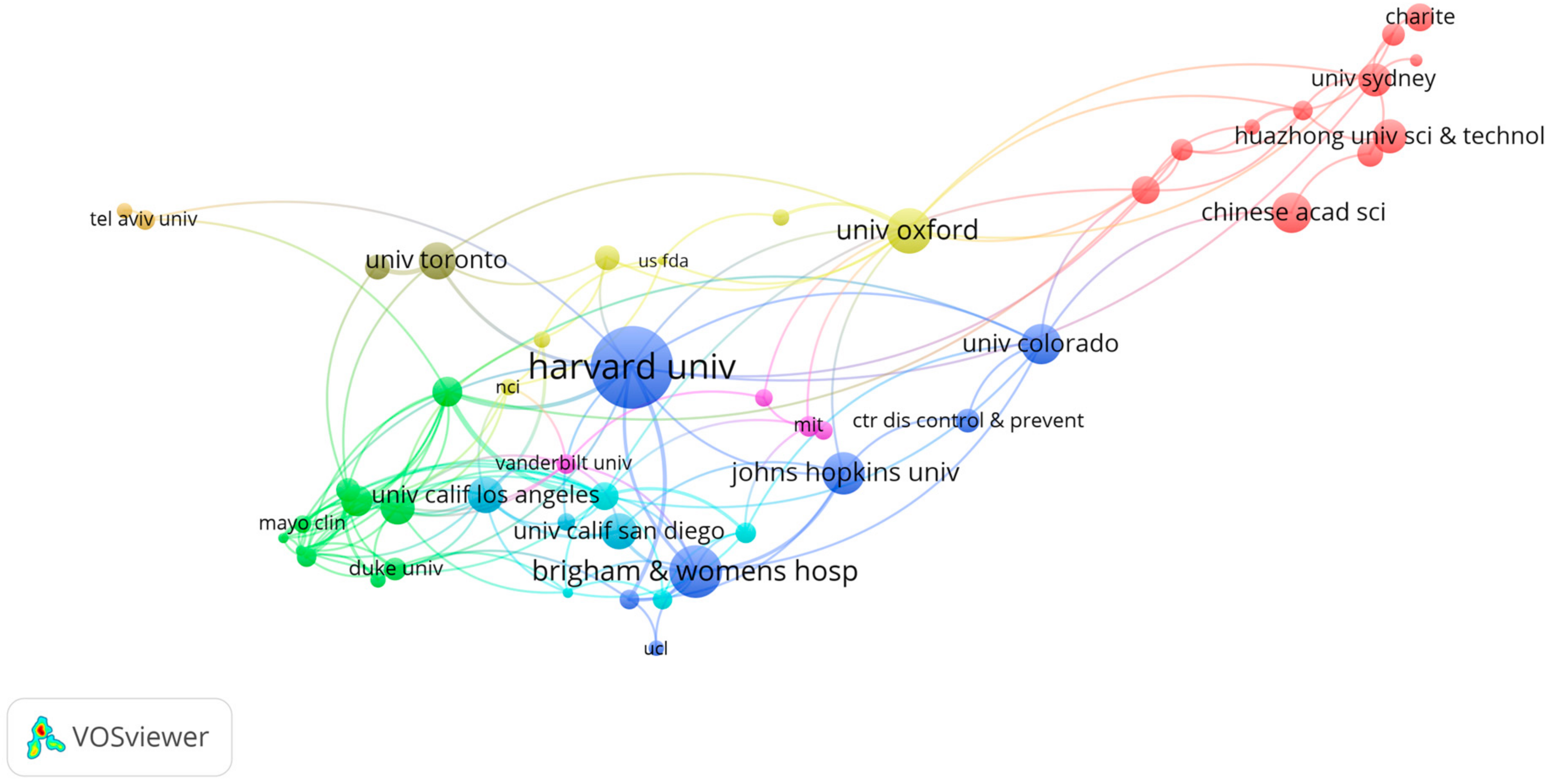
3.3.2. The Institute Co-Authorship Analysis
3.3.3. The Highly Cited MBD-Related Publications
3.4. The Co-Citation Analysis on MBD-Related Publications
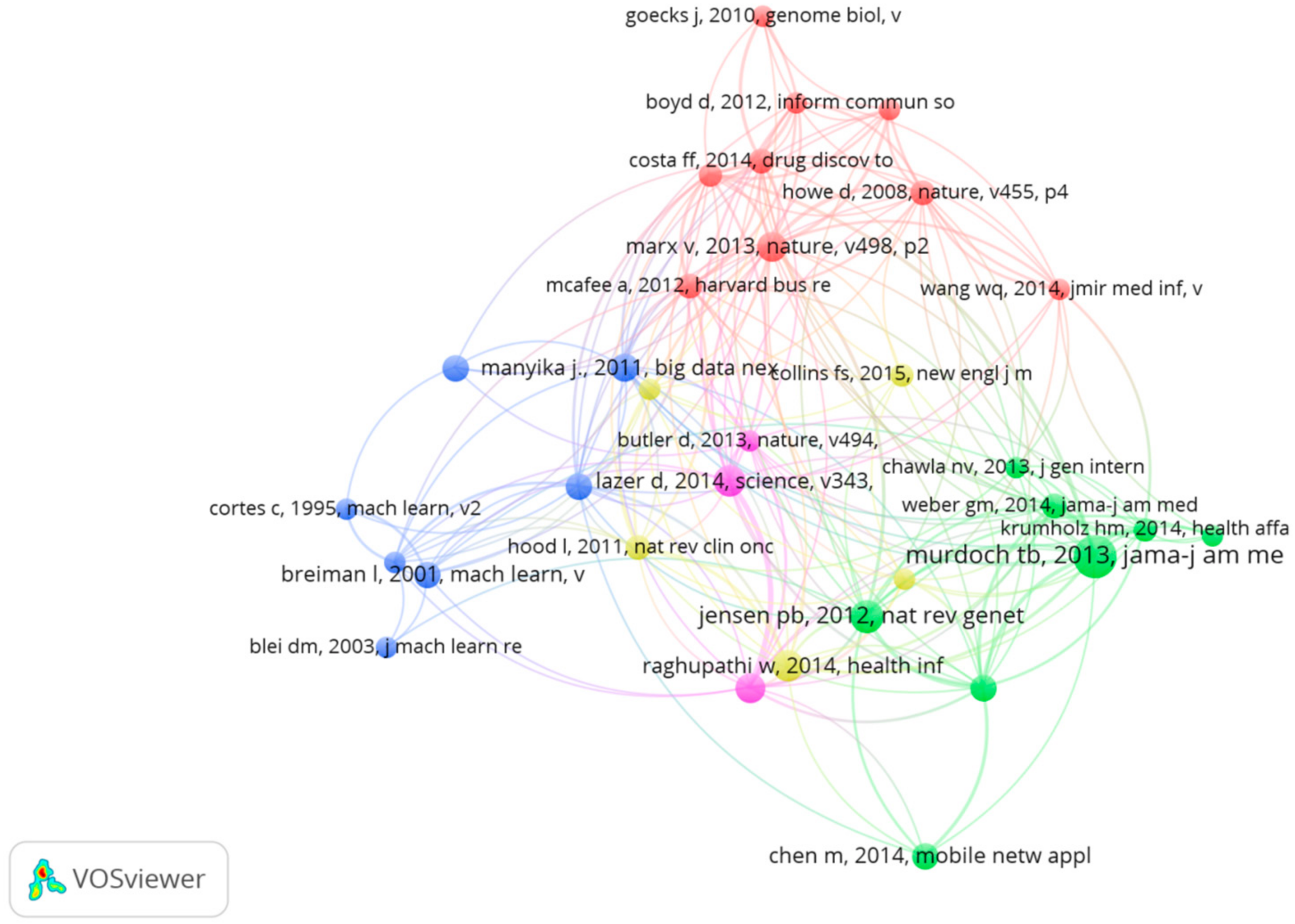
3.4.1. The Reference Co-Citation Analysis
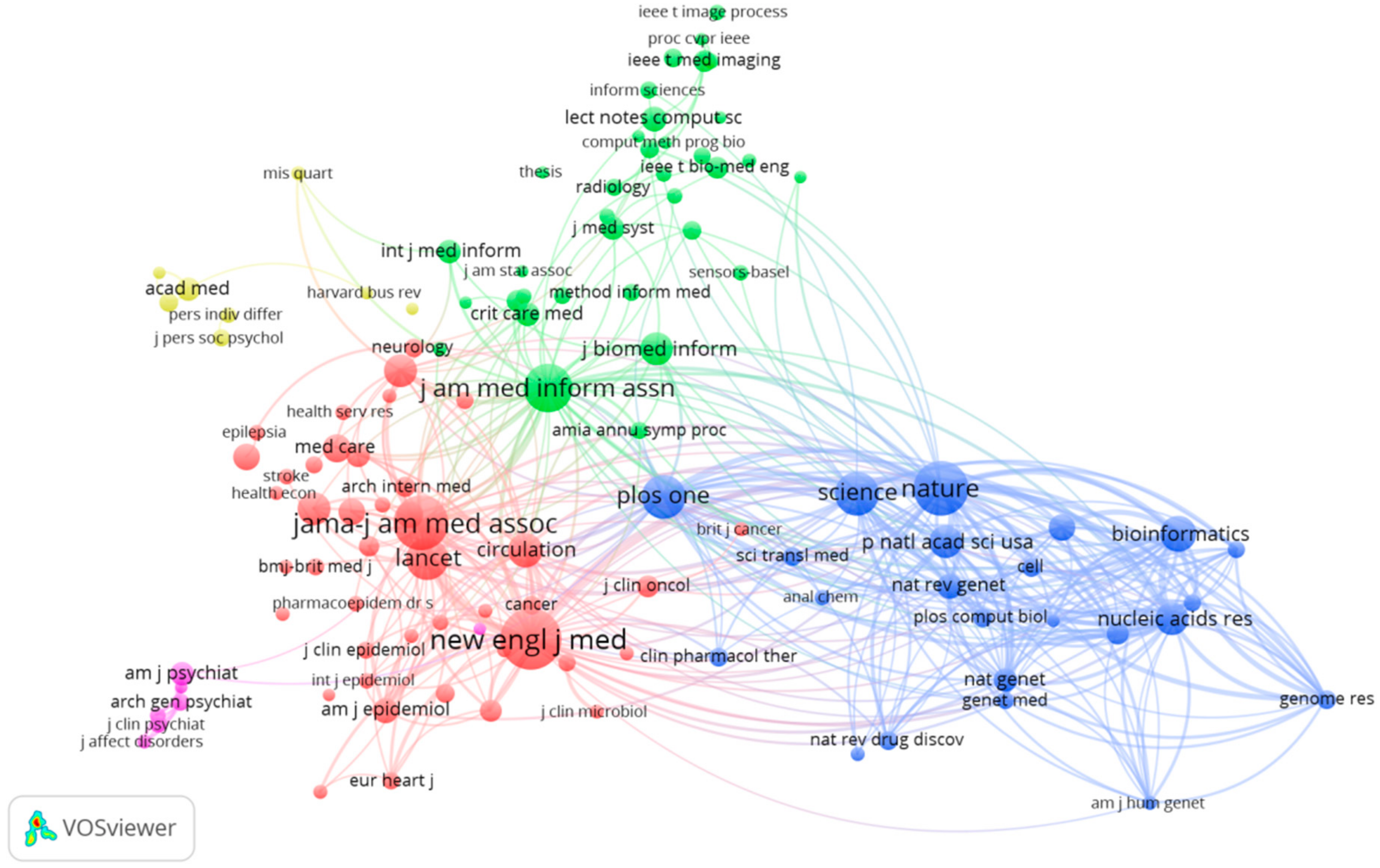
3.4.2. The Journal Co-Citation Analysis
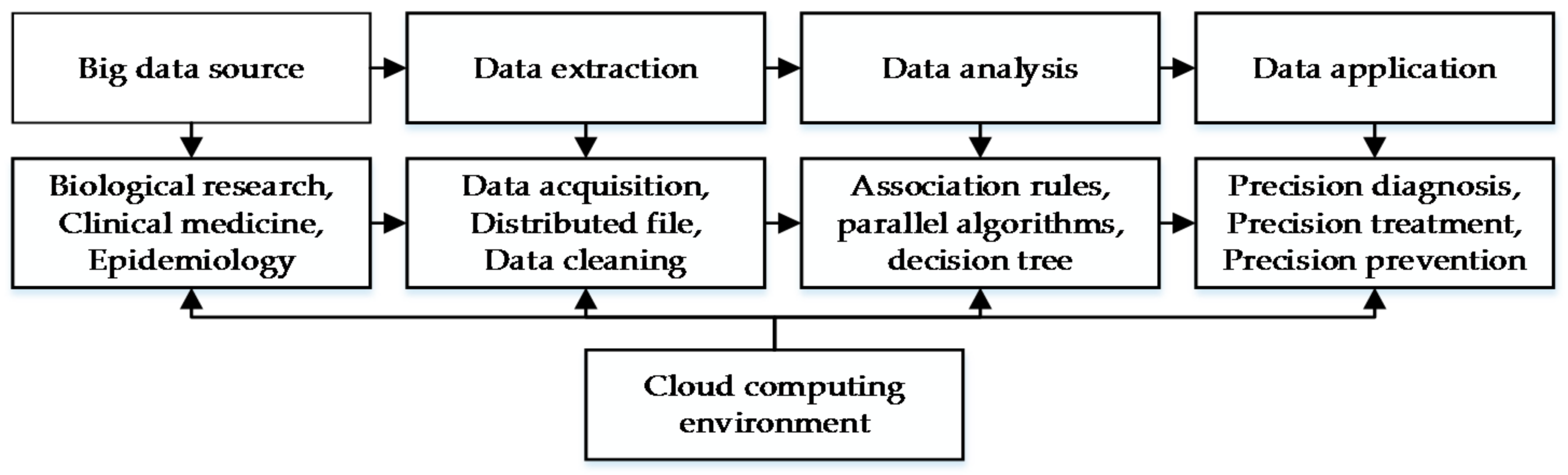
4. Discussions and Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Jin, X.L.; Wah, B.W.; Chen, X.Q.; Wang, Y.Z. Significance and challenges of big data research. Big Data Res. 2015, 2, 59–64. [Google Scholar] [CrossRef]
- Binder, H.; Blettner, M. Big data in medical science-A biostatistical view. Dtsch. Arztebl. Int. 2015, 112, 137–142. [Google Scholar] [PubMed]
- Katal, A.; Wazid, M.; Goudar, R.H. Big data: Issues, challenges, tools and good practices. In Proceedings of the Sixth International Conference on Contemporary Computing (IC3), Noida, India, 8–10 August 2013; pp. 404–409. [Google Scholar]
- Wamba, S.F.; Akter, S.; Edwards, A.; Chopin, G.; Gnanzou, D. How ‘big data’ can make big impact: Findings from a systematic review and a longitudinal case study. Int. J. Prod. Econ. 2015, 165, 234–246. [Google Scholar] [CrossRef]
- Alles, M.G. Drivers of the use and facilitators and obstacles of the evolution of big data by the audit profession. Account. Horiz. 2015, 29, 439–449. [Google Scholar] [CrossRef]
- Huwe, T.K. Big data, big future. Comput. Lib. 2012, 32, 20–22. [Google Scholar]
- Li, G.J.; Cheng, X.Q. Research status and scientific thinking of big data. Bull. Chin. Acad. Sci. 2012, 6, 647–657. [Google Scholar]
- Jee, K.; Kim, G.H. Potentiality of big data in the medical sector: Focus on how to reshape the healthcare system. Healthc. Inform. Res. 2013, 19, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Chawla, N.V.; Davis, D.A. Bringing big data to personalized healthcare: A patient-centered framework. J. Gen. Intern. Med. 2013, 28, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Antman, E.M.; Benjamin, E.J.; Harrington, R.A.; Houser, S.R.; Peterson, E.D.; Bauman, M.A.; Brown, N.; Bufalino, V.; Califf, R.M.; Creager, M.A.; et al. Acquisition, analysis, and sharing of data in 2015 and beyond: A survey of the landscape. J. Am. Heart Assoc. 2015, 4, e002810. [Google Scholar] [CrossRef] [PubMed]
- Merigó, J.M. Academic research in innovation: A country analysis. Scientometrics 2016, 108, 559–593. [Google Scholar] [CrossRef]
- Železnik, D.; Vošner, H.B.; Kokol, P. A bibliometric analysis of the Journal of Advanced Nursing, 1976–2015. J. Adv. Nurs. 2017, 73, 2407–2419. [Google Scholar] [CrossRef] [PubMed]
- Merigó, J.M.; Mas-Tur, A.; Roig-Tierno, N.; Ribeiro-Soriano, D. A bibliometric overview of the Journal of Business Research between 1973 and 2014. J. Bus. Res. 2015, 68, 2645–2653. [Google Scholar] [CrossRef]
- Osareh, F. Bibliometrics, citation analysis and co-citation analysis: A review of literature I. Libri 2009, 49, 149–158. [Google Scholar] [CrossRef]
- Yeung, A.W.K.; Goto, T.K.; Leung, W.K. A bibliometric review of research trends in neuroimaging. Curr. Sci. 2017, 112, 725–734. [Google Scholar] [CrossRef]
- Sweileh, W.M.; Al-Jabi, S.W.; Sawalha, A.F.; AbuTaha, A.S.; Saed, H.Z. Bibliometric analysis of publications on Campylobacter: (2000–2015). J. Health Popul. Nutr. 2016, 35, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Merigó, J.M.; Blanco-Mesa, F.; Gil-Lafuente, A.M.; Yager, R.R. Thirty years of the International Journal of Intelligent Systems: A bibliometric review. Int. J. Intell. Syst. 2017, 32, 526–554. [Google Scholar] [CrossRef]
- Merigó, J.M.; Yang, J.B. A bibliometric analysis of operations research and management science. Omega 2016, 97, 1–16. [Google Scholar] [CrossRef]
- Kostoff, R.N. The underpublishing of science and technology results. Scientist 2000, 14, 6. [Google Scholar]
- Liu, W.S.; Liao, H.C. A bibliometric analysis of fuzzy decision research during 1970–2015. Int. J. Fuzzy Syst. 2017, 19, 1–14. [Google Scholar] [CrossRef]
- Yu, D.J.; Liao, H.C. Visualization and quantitative research on intuitionistic fuzzy studies. J. Intell. Fuzzy Syst. 2016, 30, 3653–3663. [Google Scholar] [CrossRef]
- Powell, T.H.; Kouropalatis, Y.; Morgan, R.E.; Karhu, P. Mapping knowledge and innovation research themes: Using bibliometrics for classification, evolution, proliferation and determinism. Int. J. Entrep. Innov. Manag. 2016, 20, 174–199. [Google Scholar] [CrossRef]
- Garousi, V.; Mantyla, M.V. Citations, research topics and active countries in software engineering. Comput. Sci. Rev. 2016, 19, 56–77. [Google Scholar] [CrossRef]
- Chen, C.M. CiteSpace II: Detecting and visualizing emerging trends and transient patterns in scientific literature. J. Assoc. Inf. Sci. Tech. 2006, 57, 359–377. [Google Scholar] [CrossRef]
- Chen, C.M.; Hu, Z.; Liu, S.; Tseng, H. Emerging trends in regenerative medicine: A scientometric analysis in CiteSpace. Expert Opin. Biol. Ther. 2012, 12, 593–608. [Google Scholar] [CrossRef] [PubMed]
- Van Eck, N.J.; Waltman, L. Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics 2010, 84, 523–538. [Google Scholar] [CrossRef] [PubMed]
- Cobo, M.J.; López-Herrera, A.G.; Herrera-Viedma, E.; Herrera, F. Science mapping software tools: Review, analysis, and cooperative study among tools. J. Assoc. Inf. Sci. Tech. 2011, 62, 1382–1402. [Google Scholar] [CrossRef]
- Bates, D.W.; Saria, S.; Ohnomachado, L.; Shah, A.; Escobar, G. Big data in health care: Using analytics to identify and manage high-risk and high-cost patients. Health Affair. 2014, 33, 1123–1131. [Google Scholar] [CrossRef] [PubMed]
- Tahamtan, I.; Afshar, A.S.; Ahamdzadeh, K. Factors affecting number of citations: A comprehensive review of the literature. Scientometrics 2016, 107, 1195–1225. [Google Scholar] [CrossRef]
- Bertolibarsotti, L.; Lando, T. A theoretical model of the relationship between the h-index and other simple citation indicators. Scientometrics 2017, 111, 1–34. [Google Scholar]
- Bornmann, L.; Daniel, H.D. What do we know about the h index? J. Am. Soc. Inf. Sci. Technol. 2007, 58, 1381–1385. [Google Scholar] [CrossRef]
- Díaz, I.; Cortey, M.; Olvera, À.; Segalés, J. Use of H-index and other bibliometric indicators to evaluate research productivity outcome on swine diseases. PLoS ONE 2016, 11, e0149690. [Google Scholar] [CrossRef] [PubMed]
- Li, H.J.; An, H.Z.; Wang, Y.; Huang, J.C.; Gao, X.Y. Evolutionary features of academic articles co-keyword network and keywords co-occurrence network: Based on two-mode affiliation network. Phys. A 2016, 450, 657–669. [Google Scholar] [CrossRef]
- Gu, D.X.; Li, J.J.; Li, X.G.; Liang, C.Y. Visualizing the knowledge structure and evolution of big data research in healthcare informatics. Int. J. Med. Inform. 2017, 98, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Pinto, M.; Pulgarín, A.; Escalona, M.I. Viewing information literacy concepts: A comparison of two branches of knowledge. Scientometrics 2014, 98, 2311–2329. [Google Scholar] [CrossRef]
- Chung, K.F. Personalised medicine in asthma: Time for action. Eur. Respir. Rev. 2017, 26, 170064. [Google Scholar] [CrossRef] [PubMed]
- Schulkes, K.J.G.; Nguyen, C.; van den Bos, F.; Hamaker, M.E.; van Elden, L.J. Patient-centered outcome measures in lung cancer trials. Lung 2016, 94, 647–652. [Google Scholar] [CrossRef] [PubMed]
- Reyes, G.L.; Gonzalez, C.N.B.; Veloso, F. Using co-authorship and citation analysis to identify research groups: A new way to assess performance. Scientometrics 2016, 108, 1171–1191. [Google Scholar] [CrossRef]
- Von Haehling, S.; Anker, S.D. Cachexia as a major underestimated and unmet medical need: Facts and numbers. J. Cachexia Sarcopenia Muscle 2010, 1, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Robinson, P.B.; Sexton, E.A. The effect of education and experience on self-employment success. J. Bus. Ventur. 1994, 9, 141–156. [Google Scholar] [CrossRef]
- Regan, M.M.; Neven, P.; Giobbie-Hurder, A.; Goldhirsch, A.; Ejlertsen, B.; Mauriac, L.; Forbes Fracs, J.F.; Lang, I.; Wardley, A.; Rabaglio, M.; et al. Assessment of letrozole and tamoxifen alone and in sequence for postmenopausal women with steroid hormone receptor-positive breast cancer: The BIG 1-98 randomised clinical trial at 8.1 years median follow-up. Lancet Oncol. 2011, 12, 1101–1108. [Google Scholar] [CrossRef]
- Zhang, B.T.; Muhlenbein, H. Balancing accuracy and parsimony in genetic programming. Evol. Comput. 1995, 3, 17–38. [Google Scholar] [CrossRef]
- Small, H. Co-citation in the scientific literature: A new measure of the relationship between two documents. J. Am. Soc. Inform. Sci. 1973, 24, 265–269. [Google Scholar] [CrossRef]
- Boyack, K.W.; Klavans, R. Co-citation analysis, bibliographic coupling, and direct citation: Which citation approach represents the research front most accurately? J. Assoc. Inf. Sci. Technol. 2010, 61, 2389–2404. [Google Scholar] [CrossRef]
- Murdoch, T.B.; Detsky, A.S. The inevitable application of big data to health care. JAMA J. Am. Med. Assoc. 2013, 309, 1351–1352. [Google Scholar] [CrossRef] [PubMed]
- Hu, C.P.; Hu, J.M.; Gao, Y.; Zhang, Y.K. A journal co-citation analysis of library and information science in China. Scientometrics 2011, 86, 657–670. [Google Scholar] [CrossRef]
- Mirnezami, R.; Nicholson, J.; Darzi, A. Preparing for Precision Medicine. N. Engl. J. Med. 2012, 366, 489–491. [Google Scholar] [CrossRef] [PubMed]
- Hammer, M.J. Precision medicine and the changing landscape of research ethics. Oncol. Nurs. Forum 2016, 43, 149–150. [Google Scholar] [CrossRef] [PubMed]
- Jameson, J.L.; Longo, D.L. Precision medicine—Personalized, problematic, and promising. N. Engl. J. Med. 2015, 372, 2229–2234. [Google Scholar] [CrossRef] [PubMed]
- Wishart, D.S. Emerging applications of metabolomics in drug discovery and precision medicine. Nat. Rev. Drug Discov. 2016, 17, 473–484. [Google Scholar] [CrossRef] [PubMed]
- Aronson, S.J.; Rehm, H.L. Building the foundation for genomics in precision medicine. Nature 2015, 526, 336–342. [Google Scholar] [CrossRef] [PubMed]
- Costa, F.F. Big data in biomedicine. Drug Discov. Today 2014, 19, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Kayaalp, M. Patient privacy in the era of big data. Balk. Med. J. 2017. [Google Scholar] [CrossRef] [PubMed]
- Cios, K.J.; Moore, G.W. Uniqueness of medical data mining. Artif. Intell. Med. 2002, 26, 1–24. [Google Scholar] [CrossRef]
- Huang, T.; Lan, L.; Fang, X.; An, P.; Min, J.; Wang, F. Promises and challenges of big data computing in health sciences. Big Data Res. 2015, 2, 2–11. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Document | Frequency | Proportion |
|---|---|---|
| Article | 807 | 81.7 |
| Review | 98 | 10.7 |
| Editorial material | 36 | 3.6 |
| Proceedings paper | 25 | 2.5 |
| Meeting abstract | 12 | 1.2 |
| Book chapter | 5 | 0.5 |
| Letter | 2 | 0.2 |
| Book review | 1 | 0.1 |
| Correction | 1 | 0.1 |
| News item | 1 | 0.1 |
| Total | 988 | 100 |
| Rank | Keywords | Frequency | Total Link Strength |
|---|---|---|---|
| 1 | Big data | 203 | 597 |
| 2 | Care | 70 | 220 |
| 3 | Risk | 50 | 172 |
| 4 | Health-care | 45 | 152 |
| 5 | System | 43 | 139 |
| 6 | Health | 43 | 121 |
| 7 | Management | 34 | 94 |
| 8 | The United States | 33 | 123 |
| 9 | Epidemiology | 32 | 118 |
| 10 | Quality | 31 | 95 |
| Periods | Keywords |
|---|---|
| Before 2000 | mortality, care, internet, women, intensive care system |
| 2001–2010 | Diagnosis, impact, the United States, clinical trial, quality of life, risk, model, predication, cost, stress, death, anxiety, simulation, complication, birth, association, cohort, breast cancer |
| After 2010 | Personalized medicine, machine learning, framework, database, datasharing, statement, privacy, personality, China, data mining |
| Title | Journal | Authors | Year | Citation | IN | CN |
|---|---|---|---|---|---|---|
| Cachexia as a major underestimated and unmet medical need: facts and numbers | Journal of Cachexia Sarcopenia and Muscle | von Haehling & Anker | 2010 | 216 | 1 | 1 |
| The effect of education and experience on self-employment success | Journal of Business Venturing | Robinson & Sexton | 1994 | 190 | 2 | 2 |
| Assessment of letrozole and tamoxifen alone and in sequence for postmenopausal women with steroid hormone receptor-positive breast cancer: the BIG 1-98 randomised clinical trial at 8.1 years median follow-up | Lancet Oncology | Regan et al. | 2011 | 157 | 14 | 9 |
| Balancing accuracy and parsimony in genetic programming | Evolutionary Computation | Zhang & Muhlenbein | 1995 | 113 | 1 | 1 |
| Galactomannan detection for invasive aspergillosis in immunocompromized patients | Cochrane Database of Systematic Reviews | Leeflang, Debets-Ossenkopp & Visser | 2008 | 112 | 1 | 1 |
| Meta-analysis in clinical trials revisited | Contemporary Clinical Trials | DerSimonian & Laird | 2015 | 105 | 1 | 1 |
| Evaluation of noise-induced hearing loss in young people using a web-based survey technique | Pediatrics | Chung, Des Roches & Meunier | 2005 | 98 | 2 | 1 |
| Big data in health care: Using analytics to identify and manage high-risk and high-cost patients | Health Affairs | Bates, Saria & Ohno-Machado | 2014 | 96 | 5 | 1 |
| Multimorbidity and quality of life: A closer look | Health and Quality of Life Outcomes | Fortin, Dubois & Hudon | 2007 | 92 | 1 | 1 |
| ‘Big data’, Hadoop and cloud computing in genomics | Journal Biomedical Informatics | O’Driscoll, Daugelaite & Sleator | 2013 | 90 | 1 | 1 |
| Frequency | Betweenness Centrality | Author | Year |
|---|---|---|---|
| 29 | 0.16 | Murdoch TB | 2013 |
| 17 | 0.04 | Jensen PB | 2012 |
| 15 | 0 | Lazer D | 2014 |
| 15 | 0 | Raghupathi W | 2014 |
| 14 | 0.04 | Marx V | 2013 |
| 13 | 0 | Ginsberg J | 2009 |
| 11 | 0 | Mayer-schonberger V | 2013 |
| 11 | 0 | Manyika J | 2011 |
| 10 | 0.08 | Bates DW | 2014 |
| 9 | 0.02 | Dean J | 2008 |
| Frequency | Centrality | Sources | Subject |
|---|---|---|---|
| 253 | 0.25 | JAMA-J AM MED ASSOC | Computer science, healthcare sciences& Services, Information science &Library Science, Medical Informatics |
| 240 | 0.18 | NEW ENGL J MED | General & Internal Medicine |
| 177 | 0.24 | LANCET | General & Internal Medicine |
| 163 | 0.10 | NATURE | Science & Technology |
| 162 | 0.10 | PLOS ONE | Science &Technology |
| 134 | 0.13 | SCIENCE | Science & Technology |
| 132 | 0.14 | J AM MED INFORM ASSN | Computer Science |
| Health Care Sciences & Services | |||
| Information Science & Library Science | |||
| Medical Informatics | |||
| 114 | 0.09 | BRIT MED J | General & Internal Medicine |
| 86 | 0.09 | HEALTH AFFAIRS | Health Care Sciences & Services |
| 84 | 0.06 | ANN INTERN MED | General & Internal Medicine |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liao, H.; Tang, M.; Luo, L.; Li, C.; Chiclana, F.; Zeng, X.-J. A Bibliometric Analysis and Visualization of Medical Big Data Research. Sustainability 2018, 10, 166. https://doi.org/10.3390/su10010166
Liao H, Tang M, Luo L, Li C, Chiclana F, Zeng X-J. A Bibliometric Analysis and Visualization of Medical Big Data Research. Sustainability. 2018; 10(1):166. https://doi.org/10.3390/su10010166
Chicago/Turabian StyleLiao, Huchang, Ming Tang, Li Luo, Chunyang Li, Francisco Chiclana, and Xiao-Jun Zeng. 2018. "A Bibliometric Analysis and Visualization of Medical Big Data Research" Sustainability 10, no. 1: 166. https://doi.org/10.3390/su10010166
APA StyleLiao, H., Tang, M., Luo, L., Li, C., Chiclana, F., & Zeng, X.-J. (2018). A Bibliometric Analysis and Visualization of Medical Big Data Research. Sustainability, 10(1), 166. https://doi.org/10.3390/su10010166