1. Introduction
The clavicle is among the more unique human bones. It serves as a strut for the upper extremity and is the only bony connection between it and the axial skeleton. Loads on the upper extremity are transmitted to the thorax through the clavicle. Combined with its superficial location, these factors make the clavicle the most fractured human bone, with a shape unlike all others [
1,
2].
Middle one-third clavicle fractures account for approximately 80% of clavicle fractures and have traditionally been treated non-operatively based on Neer’s work [
3]. However, Hill et al. studied non-operatively treated displaced mid-shaft clavicle fracture outcomes, and found that patients with displaced fractures often fared poorly [
4]. So, they recommended operative fixation for displaced mid-shaft clavicle fractures. In a randomized clinical trial, the Canadian Orthopaedic Trauma Society found that operative fixation of displaced adult mid-shaft clavicle fractures resulted in improved functional outcomes and lower rates of nonunion as well as malunion when compared with non-operative treatment [
5].
Unfortunately, the orthopedic and vascular literature contains reports of both early and late limb-threatening complications associated with plate-screw constructs for mid-shaft clavicle fractures [
6,
7,
8,
9,
10,
11,
12,
13,
14,
15,
16]. Unicortical screw fixation may reduce vascular injury risk to subclavian vessels near mid-shaft fractures as the inferior clavicular cortex is not violated with instrumentation utilizing this technique. A hybrid approach utilizing central unicortical locked screws was proposed, whose biomechanical utility was shown [
17]. However, it is unclear if unicortical screws alone (and associated plate fixation) are biomechanically adequate for mid-shaft clavicle fractures. We hypothesized that 3.5 mm pelvic reconstruction plates with only unicortical screw fixation would provide comparable stability to more traditional bicortical compression screw constructs with the same plate type in a transverse mid-shaft fracture model.
2. Materials and Methods
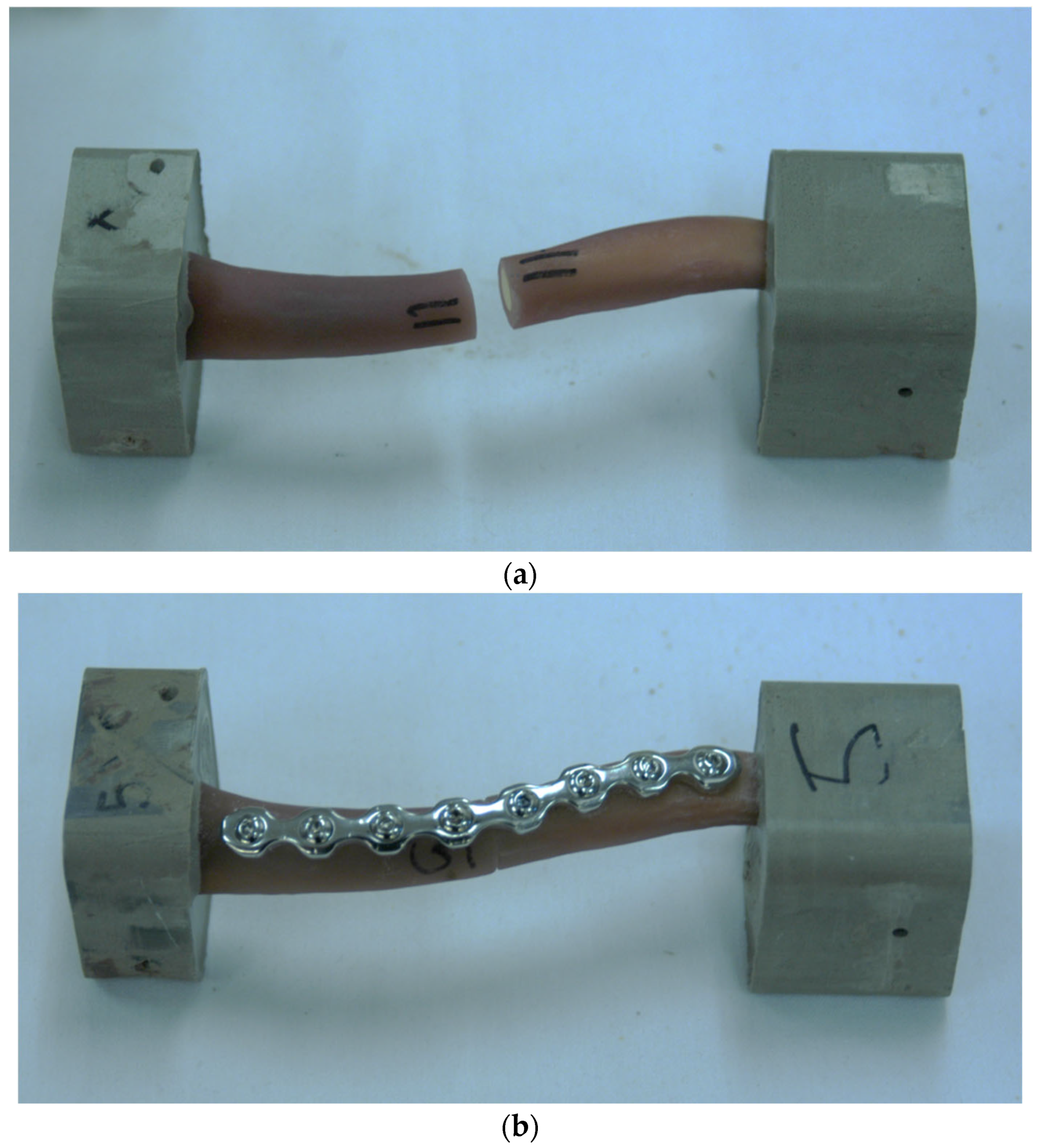
Ten fourth-generation composite clavicle models (Sawbones, Pacific Research Laboratories, Vashon, WA, USA) were used in this study. Each of these synthetic clavicles was designed to replicate the properties of real human bone and had a manufactured mid-shaft osteotomy, meaning an artificial fracture was introduced at the middle section of the bone. These clavicle specimens were randomly assigned to one of two experimental groups for further study. In many biomechanical fracture studies, cadaveric specimens are used. However, bone density, quality, and size can differ significantly between specimens. We wished to change only one variable with our study: screw type.
To ensure consistency in the surgical technique, each clavicle was carefully realigned (reduced) and surgically repaired using standard orthopedic trauma procedures. A single author (CWH, a resident with four years of experience) performed all repairs under the close supervision of two experienced attending orthopedic surgeons (EVF and MAM). For each specimen, a contoured, eight-hole, second-generation 3.5 mm locking pelvic reconstruction plate (Synthes, Paoli, PA, USA) was placed on the superior surface of the clavicle to provide structural support and stabilization (
Figure 1).
This study divided the specimens into two groups based on the type of screw used for fixation. In the first group, standard bicortical compression screws were used to secure the plate. These screws were tightened to a precise torque using a 1.5 Newton-meter (Nm) torque-limiting driver to ensure uniform tension and secure fixation. In the second group, unicortical locking screws were used instead, also tightened with the same 1.5 Nm torque-limiting driver. To maintain consistency, all plates were shaped in the same way using standard handheld plate benders before being affixed to the bone models. In both groups, four screws were placed on each side of the osteotomy to ensure a balanced and stable repair.
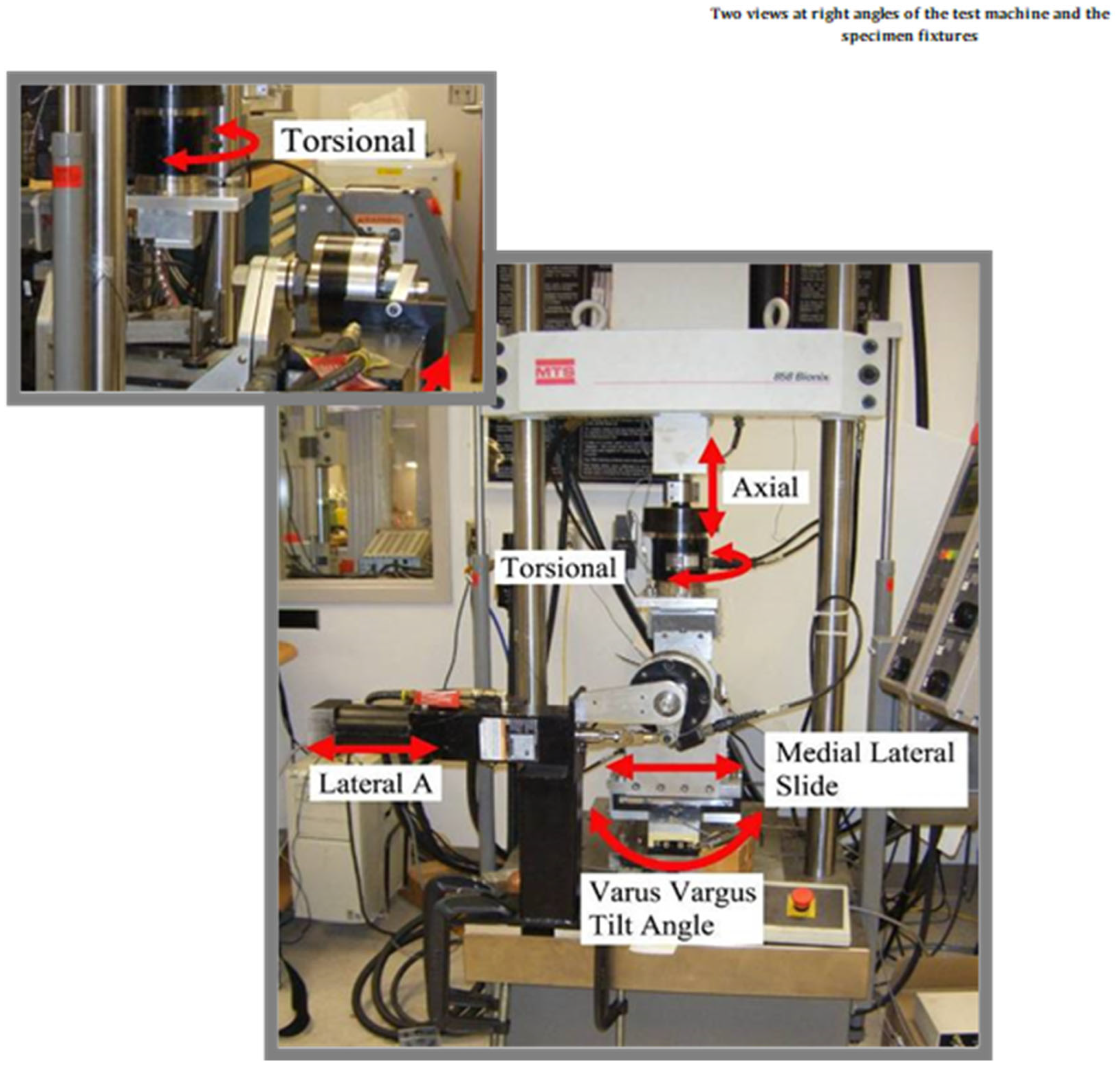
Once the repairs were complete, all specimens were securely embedded (potted) in liquid molding plastic to hold them in place for mechanical testing. The repaired clavicles were then subjected to stiffness testing using a four-axis MTS servohydraulic testing machine. This machine operated under displacement control and tested the specimens under three different loading conditions: axial rotation, anterior/posterior bending, and cephalad/caudad bending (
Figure 2). These loading modes simulated different types of mechanical stress that clavicles may experience in real-life situations, such as twisting, forward-and-backward bending, and upward-and-downward bending.
The mechanical testing procedure included an initial warm-up loop to condition the specimens before data collection. After this, three continuous cycles of mechanical loading were performed, with data recorded at a rate of 100 Hz. The range of displacement for each test was determined by conducting a preliminary scouting trial. The final testing parameters were set as follows: axial rotation was tested with a range of ±8.0 degrees, anterior/posterior bending with a range of ±7.2 degrees, and cephalad/caudad bending with a range of +7.2 degrees to −3.6 degrees.
The first loading test conducted was anterior/posterior (AP) bending. In this test, the proximal (closer to the center of the body) end of the clavicle specimen was firmly fixed to the testing machine, while the distal (farther from the center of the body) end was placed in a custom-built movable fixture. This fixture allowed the specimen to bend naturally at the osteotomy site while minimizing unwanted shear forces. Next, the specimens were rotated 180 degrees to undergo cephalad/caudad bending testing, using the same fixture setup. Finally, the axial rotation test was performed by applying torque to the specimen through a piston actuator, simulating a twisting force on the clavicle.
To analyze the results, the collected data were grouped based on the type of screw used for fixation. Descriptive statistical analysis was performed to compare the stiffness of the two groups. A two-sample t-test was used to determine whether there were significant differences between the groups. The significance threshold was set at a p-value of ≤0.05, meaning that differences with a p-value at or below this level were considered statistically significant.
3. Results
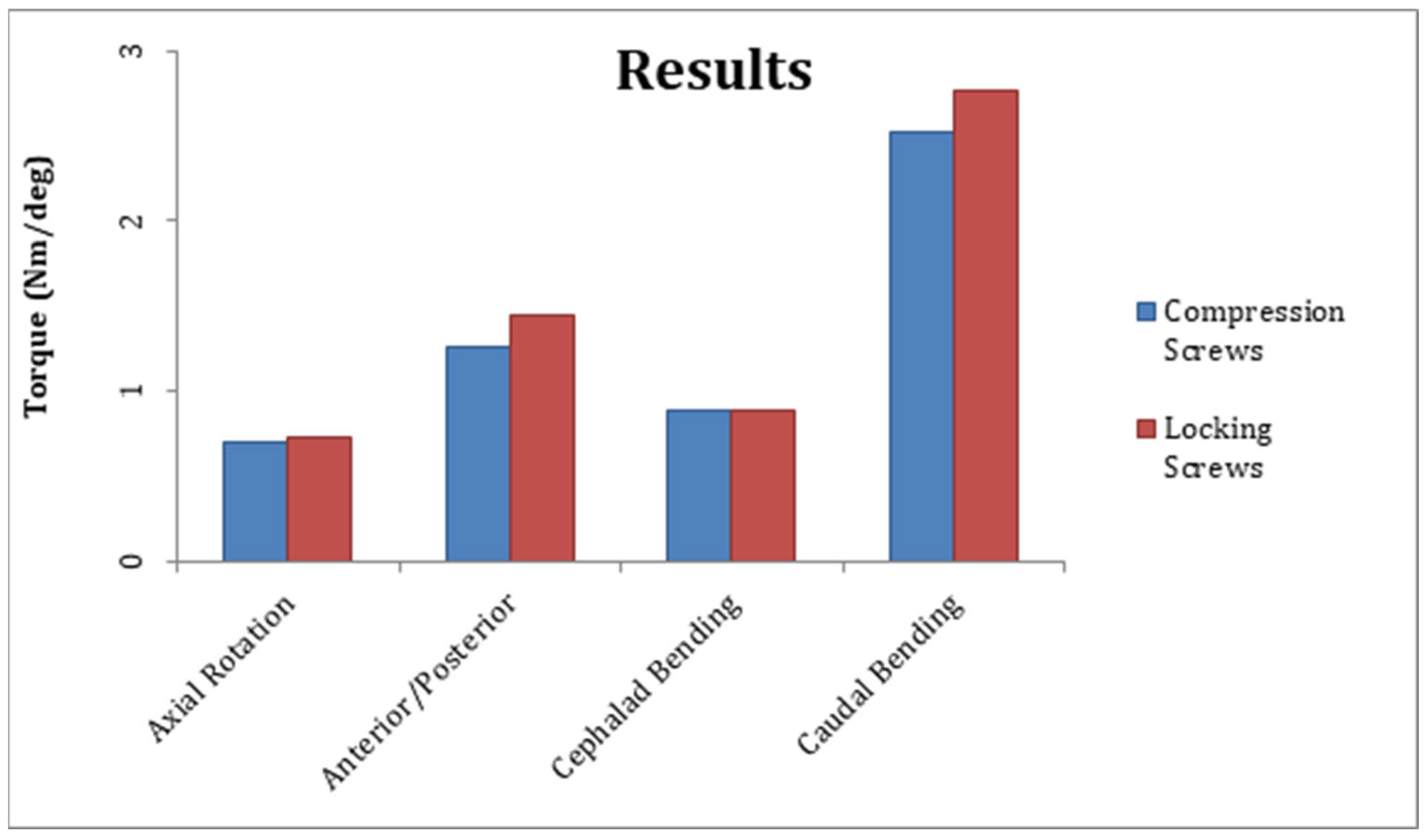
The mean steady-state construct stiffness for axial rotation, cephalad bending, and caudal bending was similar between groups one and two but differed significantly in AP bending (
Table 1,
Figure 3). The mean steady-state construct stiffness for AP bending was 1.255 ± 0.058 Nm/deg for group one and 1.442 ± 0.065 Nm/deg for group two; the difference was statistically significant (
p = 0.0013). The mean steady-state construct stiffness for axial rotation was 0.701 ± 0.08 Nm/deg for group one and 0.726 ± 0.03 Nm/deg for group two; the difference was not significant (
p = 0.581). The mean steady-state construct stiffness for cephalad bending was 0.889 ± 0.064 Nm/deg for group one and 0.880 ± 0.044 Nm/deg for group two; the difference was not significant (
p = 0.807). The mean steady-state construct stiffness for caudal bending was 2.523 ± 0.29 Nm/deg for group one and 2.774 ± 0.25 Nm/deg for group two; the difference was not significant (
p = 0.182).
4. Discussion
Following the Canadian Orthopaedic Society’s findings that operative fixation of displaced adult mid-shaft fractures resulted in improved functional outcomes with reduced nonunion and malunion (when compared with non-operative treatment), one assumes that clavicle fixation rates would increase [
5]. Yet, clavicle fracture fixation is not without risk. Intra-operative or even post-operative vascular injury can be limb-threatening [
6,
7,
8,
9,
10,
11,
12,
13,
14,
15,
16]. Plates and screws are familiar to orthopedic surgeons and provide excellent clavicular shaft rotational control, and constructs that do not violate the inferior clavicular cortex may allow surgical treatment while reducing vascular injury risk. Therefore, the purpose of this study was to perform a biomechanical comparison of mid-shaft clavicle fracture fixation constructs with only unicortical locked screws and those with standard bicortical compression screws.
Previously, Collinge et al. described anterior clavicular plate fixation to improve rigidity and decrease vascular injury risk [
18]. But this technique requires some deltoid detachment laterally and may not allow vascular protection in all due to anatomic vascular variability. Moreover, Robertson et al. suggested anterior–inferior reconstruction plates might be subjected to loads that could cause early mechanical failure [
19]. In fact, Iannotti et al. found that superior plating of mid-shaft clavicle osteotomies was biomechanically advantageous to anterior plating [
20]. They also found that 3.5 mm limited-contact dynamic compression (LCDC) plates were better than 2.7 mm dynamic compression (DC) plates or 3.5 mm reconstruction plates. But it is unclear if improved stability afforded by LCDC plates is clinically important. Also of note, the Canadian group found that hardware removal incidence declined with contoured plates [
5]. Finally, in a radiological study, Sinha et al. defined safe zones for drilling when fixing clavicle fractures, but Hussey et al. showed no difference in neurovascular injury risk between superior and anterior plate placement [
21,
22].
Mid-shaft clavicle fracture morphology may vary. Some include comminution and others include spiral components that allow interfragmentary fixation. Our simplification of this mid-shaft clavicle fracture was to allow perfect fracture reproduction in identical specimens without differences in interfragmentary fixation. Our goal was to compare standard bicortical compression screws with unicortical screws, eliminating other controllable variables. We wanted to only change one (screw type) to make it as scientific as possible. Also of note, the simple fracture line, when reduced anatomically, provides inherent stability. We chose to study the fracture construct in this fashion and for this reason eliminated the comminution issue given its infinite number of permutations. We believe the findings of this in vitro study need to be further examined in clinical trial settings in which one would utilize unicortical screws in place of bicortical compression screws in a randomized fashion to ensure baseline comparability (more specifically, transverse fracture lines or oblique fractures in which excellent interfragmentary screw fixation can be obtained).
Our study is not without limitations. We did not create a gap at the fracture site to simulate comminution. We are not of the opinion that simulated comminution and/or poor reduction are well simulated with gaps, as this biomechanical simulation can be oversimplified, given we know that the biologic environment changes continually (and with it the stability). Second, we only tested a transverse fracture model. However, oblique fracture lines frequently allow the utilization of an interfragmentary screw that can dramatically stabilize constructs and are quite variable. We felt the utilization of a transverse fracture line would be more reproducible and eliminate interfragmentary screws to allow comparison of bicortical compression and unicortical locking screws. Third, we utilized fourth-generation composite fracture models. It is possible that cadaver specimens may have changed our results. However, we wished to eliminate bone density variability as one variable that could significantly alter results, so we used consistent specimens. Fourth, we utilized second-generation pelvic reconstruction plates that may not be used by some surgeons. However, these plates also allow excellent contouring to bony surfaces. One senior surgeon (EVF) has used 3.5 mm pelvic reconstruction plates extensively for this indication as he learned from a mentor that has used them for over 30 years for both acute fractures and non-unions. The plate contours nicely versus often poorly fitting “anatomic” plating systems and LCDC and DC plates. Fifth, it is unclear if greater AP stiffness translates to improved surgical outcomes as this is beyond the scope of this study. Greater AP stiffness could potentially lead to stress shielding or other issues including peri-prosthetic fractures. Stress shielding, related to repetitive stress, could lead to weakening of the bone between screws and/or at the ends of the plate that put the bone at risk for fracture. Moreover, with increased AP bending stiffness, repetitive loading in this plane in vivo or in vitro may stress a construct so stiff that peri-prosthetic fractures occur at screw penetration sites and the ends of the plate due to hardware stress risers in these areas. Sixth, our sample size is small, five in each group. A larger sample size may have led to a more robust study, but we were limited by cost. We recognize that these limitations may not allow our results to be generalizable to all clavicle fractures or the plating systems used to address them. Yet, these limitations do not affect our ability to adequately evaluate the biomechanical differences between unicortical locked screw fixation constructs versus standard bicortical screw fixation constructs in a transverse osteotomy mid-shaft clavicle fracture model in fourth-generation composite specimens.
5. Clinical Relevance
Several studies have revealed good outcomes following plate/screw fixation of displaced mid-shaft clavicle fractures [
4,
5,
18]. Catastrophic vascular injury risk mitigation with familiar fixation that does not violate inferior clavicular cortices may influence mid-shaft clavicle fracture treatment options. We believe that future studies should also include the use of smaller constructs that are more appropriate for a smaller bone such as the clavicle.
6. Conclusions
In a transverse mid-shaft clavicle osteotomy model, superiorly placed bicortical fixation with 3.5 mm pelvic reconstruction plates did not provide greater rigidity than similarly placed unicortical locking 3.5 mm pelvic reconstruction plate/screw fixation constructs. Unicortical locking fixation provided greater rigidity in AP bending but we are unsure of the clinical significance of this.
Author Contributions
Conceptualization of this project was the work of E.V.F., M.A.M., C.W.H., N.C.B. and H.H.; the methodology was conceived of by H.H. and C.W.H.; appropriate software, validation, and jig configuration was the work of H.H. Formal analysis was performed by H.H. and C.W.H.; the investigation was performed and the resources solicited from Synthes by M.A.M., C.W.H. and N.C.B.; data curation was performed by N.C.B. and C.W.H.; original draft preparation was performed by C.W.H. and E.V.F.; review and editing was performed by B.P.Z., T.J.L. and E.V.F.; visualization and instrumentation was performed by M.A.M., N.C.B. and C.W.H.; supervision was performed by E.V.F. and H.H.; project administrator was performed by C.W.H.; and funding acquisition was through C.W.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by a Depuy-Synthes grant as well as their donation of all hardware and instrumentation.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data is unavailable due to privacy restrictions from Synthes.
Conflicts of Interest
The authors declare no conflicts of interest as they relate to this study. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| MDPI | Multidisciplinary Digital Publishing Institute |
| DOAJ | Directory of open access journals |
| TLA | Three-letter acronym |
| LD | Linear dichroism |
References
- Post, M. Current Concepts in the Treatment of Fractures of the Clavicle. Clin. Orthop. Relat. Res. 1989, 245, 89–101. [Google Scholar] [CrossRef]
- Harrington, M.; Keller, T.; Seiler, J.; Weikert, D.; Moeljanto, E.; Schwartz, H. Geometric properties and the predicted mechanical behavior of adult human clavicles. J. Biomech. 1993, 26, 417–426. [Google Scholar] [CrossRef] [PubMed]
- Neer, C.S., II. Nonunion of the clavicle. JAMA 1960, 172, 1006–1011. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.M.; McGuire, M.H.; Crosby, L.A. Closed treatment of displaced middle-third fractures of the clavicle gives poor results. J. Bone. Jt. Surg. Br. 1997, 79, 537–539. [Google Scholar] [CrossRef] [PubMed]
- Canadian Orthopaedic Trauma Society. Nonoperative treatment compared with plate fixation of displaced midshaft clavicular fractures. A multicenter, randomized clinical trial. J. Bone Jt. Surg. 2007, 89, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Johnson, B.; Thursby, P. Subclavian artery injury caused by a screw in a clavicular compression plate. Cardiovasc. Surg. 1996, 4, 414–415. [Google Scholar] [CrossRef]
- Bostman, O.; Manninen, M.; Pihlajamaki, H. Complications of plate fixation in fresh displaced midclavicular fractures. J. Trauma 1997, 43, 778–783. [Google Scholar] [CrossRef]
- Shackford, S.R. Taming of the screw: A case report and literature review of limb-threatening complications after plate osteosynthesis of a clavicular nonunion. J. Trauma 2003, 55, 840–843. [Google Scholar] [CrossRef] [PubMed]
- Kitsis, C.K.; Marino, A.J.; Krikler, S.J.; Birch, R. Late complications following clavicular fractures and their operative management. Injury 2003, 34, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Ding, M.; Hu, J.; Ni, J.; Lv, H.; Song, D.; Shu, C. Iatrogenic subclavian arteriovenous fistula: Rare complication of plate osteosynthesis of a clavicle fracture. Orthopedics 2012, 35, e287–e289. [Google Scholar] [CrossRef] [PubMed]
- Clitherow, H.D.; Bain, G.I. Association between screw prominence and vascular complications after clavicle fixation. Int. J. Shoulder Surg. 2014, 8, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Perera, K.G.; Clifford, C.; Maddock, L.J. Subclavian artery injury secondary to clavicular plate fixation: A novel operative approach. J. Surg. Case Rep. 2015, 2015, rjv044. [Google Scholar] [CrossRef] [PubMed]
- Stillwell, A.; Ioannou, C.; Daniele, L.; Tan, S.L. Osteosynthesis for clavicle fractures: How close are we to penetration of neurovascular structures. Injury 2017, 48, 460–463. [Google Scholar] [CrossRef] [PubMed]
- Pallett, S.J.C.; Singh, I.; Rady, N.; Goshai, H. Delayed Subclavian Artery Aneurysm Following Fixation of a Clavicular Fracture. Vasc. Endovasc. Surg. 2018, 52, 459–462. [Google Scholar] [CrossRef]
- Lewis, S.D.; Chew, F.S. Clavicle fixation screw impingement causing subclavian artery pseudoaneurysm. Radiol. Case Rep. 2019, 14, 1148–1150. [Google Scholar] [CrossRef]
- Chuaychoosakoon, C.; Suwanno, P.; Boonriong, T.; Suwannaphisit, S.; Klabklay, P.; Parinyakhup, W.; Maliwankul, K.; Duangnumsawang, Y.D.; Tangtrakulwanich, B. Patient Position is Related to the Risk of Neurovascular Injury in Clavicular Plating: A Cadaveric Study. Clin. Orthop. Relat. Res. 2019, 477, 2761–2768. [Google Scholar] [CrossRef]
- Rawlings, M.; Knox, D.; Patel, M.; Ackland, D. A hybrid approach to mid-shaft clavicle fixation. Injury 2016, 47, 893–898. [Google Scholar] [CrossRef] [PubMed]
- Collinge, C.; Devinney, S.; Herscovici, D.; DiPasquale, T.; Sanders, R. Anterior-inferior plate fixation of middle-third fractures and non-unions of the clavicle. J. Orthop. Trauma 2006, 20, 680–686. [Google Scholar] [CrossRef] [PubMed]
- Robertson, C.; Celestre, P.; Mahar, A.; Schwartz, A. Reconstruction Plates for Stabilization of Mid-Shaft Clavicle Fractures: Differences between Nonlocked and Locked Plates in Two Different Positions. J. Shoulder Elb. Surg. 2008, 18, 204–209. [Google Scholar] [CrossRef]
- Iannotti, M.R.; Crosby, L.A.; Stafford, P.; Grayson, G.; Goulet, R. Effects of plate location and selection on the stability of midshaft clavicle osteotomies: A biomechanical study. J. Shoulder Elb. Surg. 2002, 11, 457–462. [Google Scholar] [CrossRef] [PubMed]
- Sinha, A.; Edwin, J.; Sreeharsha, B.; Bhalaik, V.; Brownson, P. A radiological study to define safe zones for drilling during plating of clavicle fractures. J. Bone Jt. Surg. Br. Vol. 2011, 93, 1247–1252. [Google Scholar] [CrossRef] [PubMed]
- Hussey, M.M.; Chen, Y.; Fajardo, R.A.; Dutta, A.K. Analysis of neurovascular safety between superior and anterior plating techniques of clavicle fractures. J. Orthop. Trauma 2013, 27, 627–632. [Google Scholar] [CrossRef] [PubMed]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 

{kind=link}
{kind=link}
{kind=link}