
Approach to Thromboprophylaxis for Prevention of Venous Thromboembolism in COVID-19: Global Updates and Clinical Insights from India


Abstract
1. Introduction
2. Methods
3. Incidence
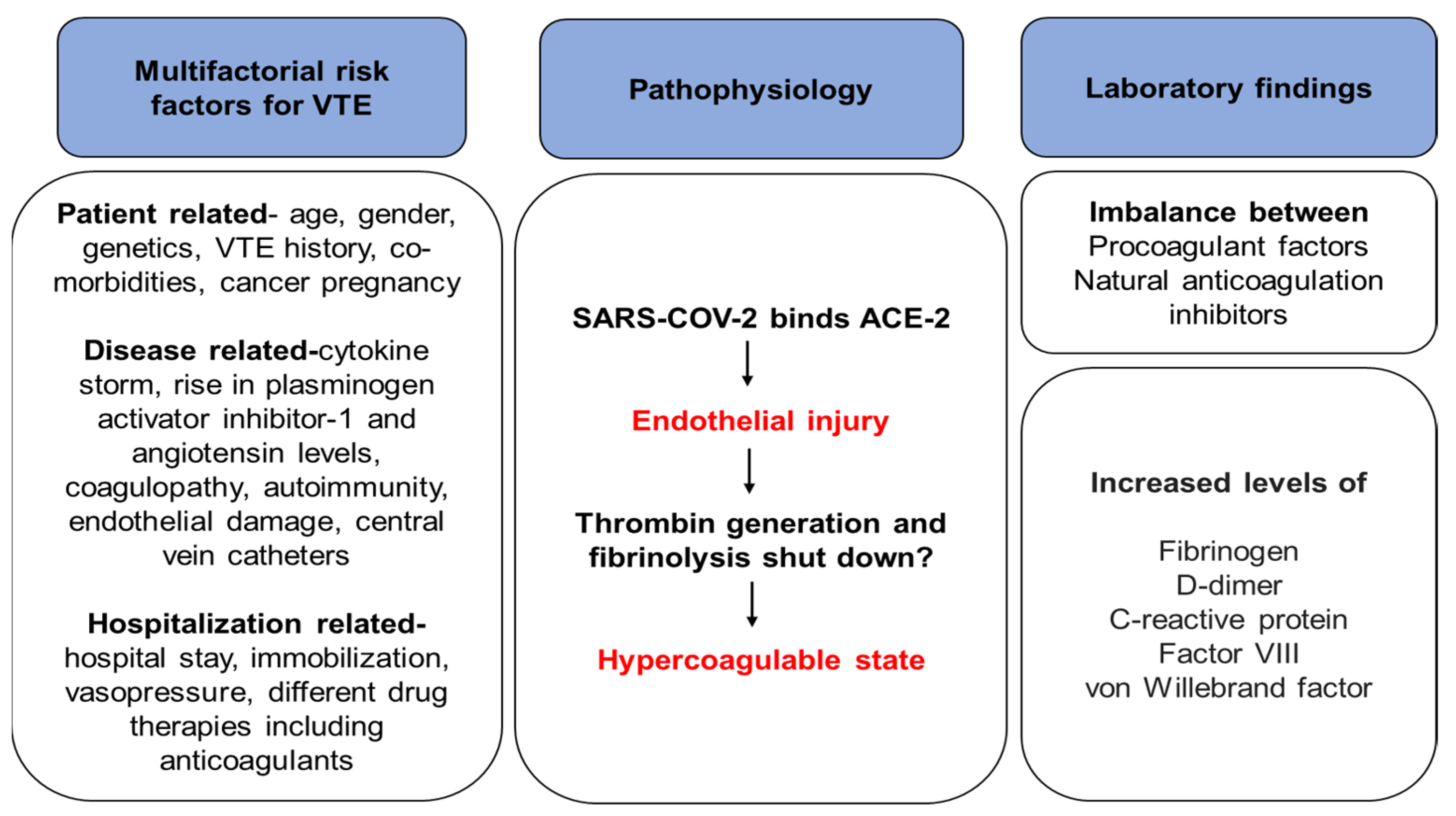
4. Pathophysiology
5. Risk Factors Associated with VTE in COVID-19
6. Predictors of VTE in COVID-19
- ○
- Elevated D-dimer levels are independently associated with thrombotic events, which could indicate an early coagulopathy and severity of COVID-19.
- ○
- Elevation of D-dimer levels precedes multiorgan failure and overt DIC resulting in increased mortality.
- ○
- High mortality rates are associated with elevated D-dimer levels at admission and marked increases in D-dimer levels over time (three- to four-fold).
- ○
- A patient with COVID-19 should not be admitted or undergo imaging for DVT/PE if D-dimer levels are elevated alone without any additional symptoms or signs of VTE.
- ○
- Rapidly increased D-dimer with clinical deterioration should raise suspicion of PE.
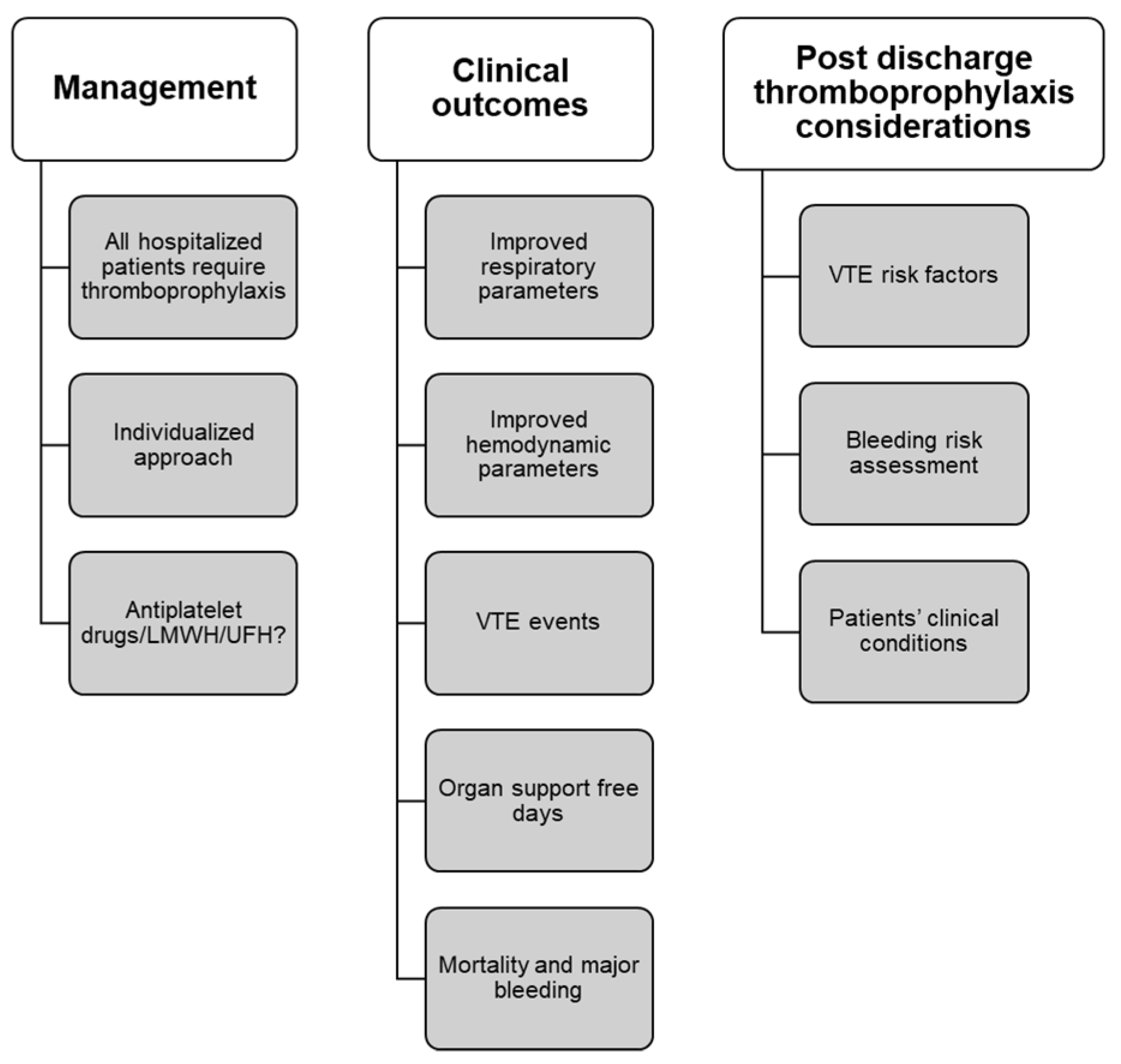
7. Thromboprophylaxis
- ○
- LMWH is preferred due to lesser exposure to health workers and partial thromboplastin time monitoring is not required [59].
- ○
- UFH is less preferred due to drawbacks such as increased staff exposure, need for laboratory monitoring, and occurrence of thrombocytopenia [59].
- ○
- Mechanical thromboprophylaxis is used when pharmacological thromboprophylaxis is contraindicated. However, its additional use is not recommended in critically ill patients receiving pharmacological prophylaxis [59].
- ○
- For hospitalized patients:
- Acutely ill/critically ill: With the absence of contraindication, anticoagulant (AC) thromboprophylaxis should be used over no AC prophylaxis [14].
- Acutely ill: AC prophylaxis with LMWH or fondaparinux over UFH; LMWH/fondaparinux/UFH should be used over DOACs [14].
- All patients: In-patient thromboprophylaxis is preferred over in-patient plus extended thromboprophylaxis [14].
8. Standard vs. Intermediate vs. Therapeutic Regimens or Intensity
9. Duration of Thromboprophylaxis; in-Hospital vs. Extended
- ○
- A standard dose of LMWH should be considered in all hospitalized patients after assessing bleeding risk [63].
- ○
- Prophylactic doses of anticoagulation are preferred over therapeutic doses in patients with COVID-19 who do not have suspected or confirmed VTE [13].
- ○
- In the case of presumed VTE, the dose may be escalated from a prophylactic to a therapeutic or an intermediate dose [11].
- ○
- Extended thromboprophylaxis is not recommended routinely and should only be considered if VTE risk continues to be high during discharge with low bleeding risk [14].
10. Considerations in Special Population
10.1. Renal Impairment
10.2. Cancer
10.3. Overweight or Obese
10.4. Pregnancy
- ○
- The available data suggest that LMWH can accumulate in patients with a creatinine clearance < 30 mL/min with therapeutic doses. This can increase the patient’s risk of bleeding by two-fold as compared to the patients with normal creatinine clearance [88].
- ○
- ○
- High-risk out-patients with cancer with a Khorana score of two or higher before initiating new systemic chemotherapy may be offered thromboprophylaxis with apixaban, rivaroxaban, or LMWH [92].
- ○
- Hospitalized cancer patients with creatinine clearance of ≥ 30 mL/min, LMWH or fondaparinux or UFH. DOACs are not recommended routinely [93].
- ○
- Thromboprophylaxis with a weight-adjusted dose of LMWH is preferred in patients with obesity [74].
11. Clinical Implications of VTE in COVID-19 in Indian Scenario
12. Limitations and Future Directions
13. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclosures
References
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/region/searo/country/in (accessed on 3 February 2022).
- Yu, Y.; Tu, J.; Lei, B.; Shu, H.; Zou, X.; Li, R.; Huang, C.; Qu, Y.; Shang, Y. Incidence and Risk Factors of Deep Vein Thrombosis in Hospitalized COVID-19 Patients. Clin. Appl. Thromb. Hemost. 2020, 26, 1076029620953217. [Google Scholar] [CrossRef]
- Ray, G.; Behera, M. VTE- Indian perspective. Med. Update 2010, 20, 1–6. [Google Scholar]
- Benzakoun, J.; Hmeydia, G.; Delabarde, T.; Hamza, L.; Meder, J.F.; Ludes, B.; Mebazaa, A. Excess out of hospital deaths during COVID-19 outbreak: Evidence of pulmonary embolism as a main determinant. Eur. J. Heart Fail. 2020, 22, 1046–1047. [Google Scholar] [CrossRef]
- Malas, M.B.; Naazie, I.N.; Elsayed, N.; Mathlouthi, A.; Marmor, R.; Clary, B. Thromboembolism risk of COVID-19 is high and associated with a higher risk of mortality: A systematic review and meta-analysis. EClinicalMedicine 2020, 29, 100639. [Google Scholar] [CrossRef]
- Lee, A.D.; Stephen, E.; Agarwal, S.; Premkumar, P. Venous Thrombo-embolism in India. Eur. J. Vasc. Endovasc. Surg. 2009, 37, 482–485. [Google Scholar] [CrossRef]
- Mai, V.; Tan, B.K.; Mainbourg, S.; Potus, F.; Cucherat, M.; Lega, J.C.; Lega, J.C.; Provencher, S. VTE in COVID-19 compared to non-COVID-19 cohorts: A systematic review with meta-analysis. Vascul Pharmacol. 2021, 139, 106882. [Google Scholar] [CrossRef] [PubMed]
- Tang, N.; Bai, H.; Chen, X.; Gong, J.; Li, D.; Sun, Z. Anticoagulant treatment is associated with decreased mortality in severe coronavirus disease 2019 patients with coagulopathy. J. Thromb. Haemost. 2020, 18, 1094–1099. [Google Scholar] [CrossRef] [PubMed]
- Zhai, Z.; Li, C.; Chen, Y.; Gerotziafas, G.; Zhang, Z.; Wan, J.; Liu, P.; Elalamy, I.; Wang, C.; Prevention Treatment of VTE Associated with COVID-19 Infection Consensus Statement Group. Prevention and treatment of VTE associated with coronavirus disease 2019 infection: A Consensus Statement before Guidelines. Thromb. Haemost. 2020, 120, 937–948. [Google Scholar] [CrossRef]
- Thachil, J.; Tang, N.; Gando, S.; Falanga, A.; Cattaneo, M.; Levi, M.; Clark, C.; Iba, T. ISTH interim guidance on recognition and management of coagulopathy in COVID-19. J. Thromb. Haemost 2020, 18, 1023–1026. [Google Scholar] [CrossRef]
- Schulman, S.; Sholzberg, M.; Spyropoulos, A.C.; Zarychanski, R.; Resnick, H.E.; Bradbury, C.A.; Broxmeyer, L.; Connors, J.M.; Falanga, A.; Iba, T.; et al. International Society on Thrombosis and Haemostasis. ISTH guidelines for antithrombotic treatment in COVID-19. J. Thromb. Haemost 2022. [Google Scholar] [CrossRef]
- Cuker, A.; Tseng, E.K.; Nieuwlaat, R.; Angchaisuksiri, P.; Blair, C.; Dane, K.; Davila, J.; DeSancho, M.T.; Diuguid, D.; Griffin, D.O.; et al. American Society of Hematology 2021 guidelines on the use of anticoagulation for thromboprophylaxis in patients with COVID-19. Blood Adv. 2021, 5, 872–888. [Google Scholar] [CrossRef]
- Moores, L.K.; Tritschler, T.; Brosnahan, S.; Carrier, M.; Collen, J.F.; Doerschug, K.; Holley, A.B.; Jimenez, D.; Le Gal, G.; Rali, P.; et al. Prevention, Diagnosis, and Treatment of VTE in Patients With Coronavirus Disease 2019: CHEST Guideline and Expert Panel Report. Chest 2020, 158, 1143–1163. [Google Scholar] [CrossRef]
- Venous Thromboembolism in Adults. Quality Standard [QS201] Published. 19 August 2021. Available online: https://www.nice.org.uk/guidance/qs201 (accessed on 6 June 2022).
- Nopp, S.; Moik, F.; Jilma, B.; Pabinger, I.; Ay, C. Risk of VTE in patients with COVID-19: A systematic review and meta-analysis. Res. Pract. Thromb. Haemost. 2020, 4, 1178–1191. [Google Scholar] [CrossRef]
- Lu, Y.F.; Pan, L.Y.; Zhang, W.W.; Cheng, F.; Hu, S.S.; Zhang, X.; Jiang, H.Y. A meta-analysis of the incidence of venous thromboembolic events and impact of anticoagulation on mortality in patients with COVID-19. Int. J. Infect. Dis. 2020, 100, 34–41. [Google Scholar] [CrossRef]
- Bilaloglu, S.; Aphinyanaphongs, Y.; Jones, S.; Iturrate, E.; Hochman, J.; Berger, J.S. Thrombosis in Hospitalized Patients With COVID-19 in a New York City HealtSystem. JAMA 2020, 324, 799–801. [Google Scholar] [CrossRef]
- Al-Samkari, H.; Karp Leaf, R.S.; Dzik, W.H.; Carlson, J.C.T.; Fogerty, A.E.; Waheed, A.; Goodarzi, K.; Bendapudi, P.K.; Bornikova, L.; Gupta, S.; et al. COVID-19 and coagulation: Bleeding and thrombotic manifestations of SARS-CoV-2 infection. Blood 2020, 136, 489–500. [Google Scholar] [CrossRef]
- Hippensteel, J.A.; Burnham, E.L.; Jolley, S.E. Prevalence of VTE in critically ill patients with COVID-19. Br. J. Haematol. 2020, 190, e134–e137. [Google Scholar] [CrossRef]
- Jenner, W.J.; Kanji, R.; Mirsadraee, S.; Gue, Y.X.; Price, S.; Prasad, S.; Gorog, D.A. Thrombotic complications in 2928 patients with COVID-19 treated in intensive care: A systematic review. J. Thromb. Thrombolysis. 2021, 51, 595–607. [Google Scholar] [CrossRef]
- Di Minno, A.; Ambrosino, P.; Calcaterra, I.; Di Minno, M.N.D. COVID-19 and VTE: A Meta-analysis of Literature Studies. Semin. Thromb. Hemost. 2020, 46, 763–771. [Google Scholar]
- Yuan, X.; Tong, X.; Wang, Y.; Wang, H.; Wang, L.; Xu, X. Coagulopathy in elderly patients with coronavirus disease 2019. Aging Med. (Milton) 2020, 3, 260–265. [Google Scholar] [CrossRef]
- Wang, S.Y.; Singh, A.; Eder, M.D.; Vadlamani, L.; Lee, A.I.; Chun, H.J.; Desai, N.R. Association of obesity with VTE and myocardial injury in COVID-19. Obes. Res. Clin. Pract. 2021, 15, 512–514. [Google Scholar] [CrossRef] [PubMed]
- O’Gallagher, K.; Shek, A.; Bean, D.M.; Bendayan, R.; Papachristidis, A.; Teo, J.T.H.; Dobson, R.; Shah, A.M.; Zakeri, R. Pre-existing cardiovascular disease rather than cardiovascular risk factors drives mortality in COVID-19. BMC Cardiovasc. Disord. 2021, 21, 327. [Google Scholar] [CrossRef]
- Giannis, D.; Ziogas, I.A.; Gianni, P. Coagulation disorders in coronavirus infected patients: COVID-19, SARS-CoV-1, MERS-CoV and lessons from the past. J. Clin. Virol. 2020, 127, 104362. [Google Scholar] [CrossRef]
- Ozsu, S.; Gunay, E.; Konstantinides, S.V. A review of VTE in COVID-19: A clinical perspective. Clin. Respir. J. 2021, 15, 506–512. [Google Scholar] [CrossRef]
- Bhatt, H.; Singh, S. VTE and COVID-19: A case report and review of the literature. J. Med. Case Rep. 2020, 14, 188. [Google Scholar] [CrossRef]
- Skendros, P.; Mitsios, A.; Chrysanthopoulou, A.; Mastellos, D.C.; Metallidis, S.; Rafailidis, P.; Ntinopoulou, M.; Sertaridou, E.; Tsironidou, V.; Tsigalou, C.; et al. Complement and tissue factor-enriched neutrophil extracellular traps are key drivers in COVID-19 immunothrombosis. J. Clin. Invest. 2020, 130, 6151–6157. [Google Scholar] [CrossRef]
- Hanff, T.C.; Mohareb, A.M.; Giri, J.; Cohen, J.B.; Chirinos, J.A. Thrombosis in COVID-19. Am. J. Hematol. 2020, 95, 1578–1589. [Google Scholar] [CrossRef] [PubMed]
- Colling, M.E.; Kanthi, Y. COVID-19-associated coagulopathy: An exploration of mechanisms. Vasc. Med. 2020, 25, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Zaid, Y.; Puhm, F.; Allaeys, I.; Naya, A.; Oudghiri, M.; Khalki, L.; Limami, Y.; Zaid, N.; Sadki, K.; Ben El Haj, R.; et al. Platelets Can Associate with SARS-Cov-2 RNA and Are Hyperactivated in COVID-19. Circ Res. 2020, 127, 1404–1418. [Google Scholar] [CrossRef] [PubMed]
- Sakr, Y.; Giovini, M.; Leone, M.; Pizzilli, G.; Kortgen, A.; Bauer, M.; Tonetti, T.; Duclos, G.; Zieleskiewicz, L.; Buschbeck, S.; et al. Pulmonary embolism in patients with coronavirus disease-2019 (COVID-19) pneumonia: A narrative review. Ann. Intensive. Care. 2020, 10, 124. [Google Scholar] [CrossRef] [PubMed]
- Bikdeli, B.; Madhavan, M.V.; Jimenez, D.; Chuich, T.; Dreyfus, I.; Driggin, E.; Nigoghossian, C.; Ageno, W.; Madjid, M.; Guo, Y.; et al. COVID-19 and Thrombotic or Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and Follow-Up: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 75, 2950–2973. [Google Scholar] [CrossRef] [PubMed]
- Voicu, S.; Delrue, M.; Chousterman, B.G.; Stépanian, A.; Bonnin, P.; Malissin, I.; Deye, N.; Neuwirth, M.; Ketfi, C.; Mebazaa, A.; et al. Imbalance between procoagulant factors and natural coagulation inhibitors contributes to hypercoagulability in the critically ill COVID-19 patient: Clinical implications. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 9161–9168. [Google Scholar] [PubMed]
- Khan, I.H.; Savarimuthu, S.; Leung, M.S.T.; Harky, A. The need to manage the risk of thromboembolism in COVID-19 patients. J. Vasc. Surg. 2020, 72, 799–804. [Google Scholar] [CrossRef]
- Gratz, J.; Wiegele, M.; Maleczek, M.; Herkner, H.; Schöchl, H.; Chwala, E.; Knöbl, P.; Schaden, E. Risk of clinically relevant VTE in critically ill patients with COVID-19: A Systematic Review and Meta-Analysis. Front Med. (Lausanne) 2021, 8, 647917. [Google Scholar] [CrossRef]
- Hasbal, N.B. Thrombotic microangiopathy: COVID-19 or hydroxychloroquine? Kidney Int. 2020, 98, 1619–1620. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Warren, K.; Adler, H.; Mangano, A.; Sansbury, J.; Duff, R. A retrospective review of outcomes in intensive care unit patients infected with SARS-Cov2 in correlation to Admission Acute Physiologic Assessment and Chronic Health Evaluation II Scores. Cureus 2021, 13, e14051. [Google Scholar] [CrossRef]
- Zeng, D.X.; Xu, J.L.; Mao, Q.X.; Liu, R.; Zhang, W.Y.; Qian, H.Y.; Xu, L. Association of Padua prediction score with in-hospital prognosis in COVID-19 patients. QJM 2020, 113, 789–793. [Google Scholar] [CrossRef]
- Iba, T.; Arakawa, M.; Mochizuki, K.; Nishida, O.; Wada, H.; Levy, J.H. Usefulness of measuring changes in sofa score for the prediction of 28-day mortality in patients with sepsis-associated disseminated intravascular coagulation. Clin. Appl. Thromb. Hemost. 2019, 25, 1076029618824044. [Google Scholar] [CrossRef]
- Caprini, J.A. Thrombosis risk assessment as a guide to quality patient care. Dis. Mon. 2005, 51, 70–78. [Google Scholar] [CrossRef]
- Caprini, J.A. Individual risk assessment is the best strategy for thromboembolic prophylaxis. Dis. Mon. 2010, 56, 552–559. [Google Scholar] [CrossRef]
- Soomro, Q.; Yousuf, N.; Bhutto, A.A.; Abro, H.A.; Memon, A.A. VTE (VTE): Risk assessment in hospitalized patients. J. Coll. Physicians Surg. Pak. 2014, 7, 455–458. [Google Scholar]
- Zakai, N.A.; Wright, J.; Cushman, M. Risk factors for venous thrombosis in medical inpatients: Validation of a thrombosis risk score. J. Thromb. Haemost. 2004, 2, 2156–2161. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Favaloro, E.J. D-dimer is associated with severity of coronavirus disease 2019: A Pooled Analysis. Thromb. Haemost. 2020, 120, 876–878. [Google Scholar] [CrossRef] [PubMed]
- Dujardin, R.W.G.; Hilderink, B.N.; Haksteen, W.E.; Middeldorp, S.; Vlaar, A.P.J.; Thachil, J.; Müller, M.; Juffermans, N.P. Biomarkers for the prediction of VTE in critically ill COVID-19 patients. Thromb. Res. 2020, 196, 308–312. [Google Scholar] [CrossRef]
- Kampouri, E.; Filippidis, P.; Viala, B.; Méan, M.; Pantet, O.; Desgranges, F.; Tschopp, J.; Regina, J.; Karachalias, E.; Bianchi, C.; et al. RegCOVID Research Group. Predicting Venous Thromboembolic Events in Patients with Coronavirus Disease 2019 Requiring Hospitalization: An Observational Retrospective Study by the COVIDIC Initiative in a Swiss University Hospital. Biomed. Res. Int. 2020, 2020, 9126148. [Google Scholar] [CrossRef]
- Cohen, S.L.; Gianos, E.; Barish, M.A.; Chatterjee, S.; Kohn, N.; Lesser, M.; Giannis, D.; Coppa, K.; Hirsch, J.S.; Northwell Health COVID-19 Research Consortium; et al. Prevalence and Predictors of VTE or Mortality in Hospitalized COVID-19 Patients. Thromb. Haemost. 2021, 121, 1043–1053. [Google Scholar] [CrossRef]
- Yu, H.H.; Qin, C.; Chen, M.; Wang, W.; Tian, D.S. D-dimer level is associated with the severity of COVID-19. Thromb Res. 2020, 195, 219–225. [Google Scholar] [CrossRef]
- Connors, J.M.; Levy, J.H. COVID-19 and its implications for thrombosis and anticoagulation. Blood 2020, 135, 2033–2040. [Google Scholar] [CrossRef]
- Mouhat, B.; Besutti, M.; Bouiller, K.; Grillet, F.; Monnin, C.; Ecarnot, F.; Behr, J.; Capellier, G.; Soumagne, T.; Pili-Floury, S.; et al. Elevated D-dimers and lack of anticoagulation predict PE in severe COVID-19 patients. Eur. Respir J. 2020, 56, 2001811. [Google Scholar] [CrossRef]
- Skeik, N.; Westergard, E. Recommendations for VTE prophylaxis in medically ill patients. Ann. Vasc. Dis. 2020, 13, 38–44. [Google Scholar] [CrossRef]
- Hunt, B.J.; De Paula, E.V.; McLintock, C.; Dumantepe, M. Prophylactic anticoagulation for patients in hospital with covid-19. Erratum BMJ 2021, 372, n487. [Google Scholar]
- Samama, M.M.; Cohen, A.T.; Darmon, J.Y.; Desjardins, L.; Eldor, A.; Janbon, C.; Leizorovicz, A.; Nguyen, H.; Olsson, C.G.; Turpie, A.G.; et al. A comparison of enoxaparin with placebo for the prevention of VTE in acutely ill medical patients. Prophylaxis in Medical Patients with Enoxaparin Study Group. N. Engl. J. Med. 1999, 341, 793–800. [Google Scholar]
- Kahn, S.R.; Lim, W.; Dunn, A.S.; Cushman, M.; Dentali, F.; Akl, E.A.; Cook, D.J.; Balekian, A.A.; Klein, R.C.; Le, H.; et al. Prevention of VTE in nonsurgical patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012, 141 (Suppl. S2), e195S–e226S. [Google Scholar] [CrossRef]
- Di Castelnuovo, A.; Costanzo, S.; Antinori, A.; Berselli, N.; Blandi, L.; Bonaccio, M.; Cauda, R.; Guaraldi, G.; Menicanti, L.; Mennuni, M.; et al. Heparin in COVID-19 patients is associated with reduced in-hospital mortality: The multicentre Italian CORIST Study. Thromb. Haemost. 2021, 121, 1054–1065. [Google Scholar] [CrossRef] [PubMed]
- Grandone, E.; Tiscia, G.; Pesavento, R.; De Laurenzo, A.; Ceccato, D.; Sartori, M.T.; Mirabella, L.; Cinnella, G.; Mastroianno, M.; Dalfino, L.; et al. Use of low-molecular weight heparin, transfusion and mortality in COVID-19 patients not requiring ventilation. J. Thromb. Thrombolysis. 2021, 52, 772–778. [Google Scholar] [CrossRef] [PubMed]
- Dutch COVID & Thrombosis Coalition; Kaptein, F.H.J.; Stals, M.A.M.; Grootenboers, M.; Braken, S.J.E.; Burggraaf, J.L.I.; van Bussel, B.; Cannegieter, S.C.; Ten Cate, H.; Endeman, H.; et al. Incidence of thrombotic complications and overall survival in hospitalized patients with COVID-19 in the second and first wave. Thromb. Res. 2021, 199, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Flaczyk, A.; Rosovsky, R.P.; Reed, C.T.; Bankhead-Kendall, B.K.; Bittner, E.A.; Chang, M.G. Comparison of published guidelines for management of coagulopathy and thrombosis in critically ill patients with COVID 19: Implications for clinical practice and future investigations. Crit. Care. 2020, 24, 559. [Google Scholar] [CrossRef] [PubMed]
- Aly, R.; Gupta, S.; Singh, B.; Kaur, P.; Kim, K.; Gupta, S. The use of direct acting oral anticoagulants in patients with COVID-19 infection. J. Community Hosp. Intern. Med. Perspect. 2021, 11, 184–186. [Google Scholar] [CrossRef] [PubMed]
- Testa, S.; Prandoni, P.; Paoletti, O.; Morandini, R.; Tala, M.; Dellanoce, C.; Giorgi-Pierfranceschi, M.; Betti, M.; Danzi, G.B.; Pan, A.; et al. Direct oral anticoagulant plasma levels’ striking increase in severe COVID-19 respiratory syndrome patients treated with antiviral agents: The Cremona experience. J. Thromb. Haemost. 2020, 18, 1320–1323. [Google Scholar] [CrossRef] [PubMed]
- Testa, S.; Legnani, C.; Antonucci, E.; Paoletti, O.; Dellanoce, C.; Cosmi, B.; Pengo, V.; Poli, D.; Morandini, R.; Testa, R.; et al. Drug levels and bleeding complications in atrial fibrillation patients treated with direct oral anticoagulants. J. Thromb. Haemost. 2019, 17, 1064–1072. [Google Scholar] [CrossRef] [PubMed]
- Rosovsky, R.P.; Sanfilippo, K.M.; Wang, T.F.; Rajan, S.K.; Shah, S.; Martin, K.A.; Ní Áinle, F.; Huisman, M.; Hunt, B.J.; Kahn, S.R.; et al. Anticoagulation Practice Patterns in COVID-19: A Global Survey. Res. Pract. Thromb. Haemost. 2020, 4, 969–983. [Google Scholar] [CrossRef] [PubMed]
- Klok, F.A.; Kruip, M.J.H.A.; van der Meer, N.J.M.; Arbous, M.S.; Gommers, D.A.M.P.J.; Kant, K.M.; Kaptein, F.; van Paassen, J.; Stals, M.; Huisman, M.V.; et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb. Res. 2020, 191, 145–147. [Google Scholar] [CrossRef] [PubMed]
- Llitjos, J.F.; Leclerc, M.; Chochois, C.; Monsallier, J.M.; Ramakers, M.; Auvray, M.; Merouani, K. High incidence of venous thromboembolic events in anticoagulated severe COVID-19 patients. J. Thromb. Haemost. 2020, 18, 1743–1746. [Google Scholar] [CrossRef]
- O’Connell, C.; Escalante, C.P.; Goldhaber, S.Z.; McBane, R.; Connors, J.M.; Raskob, G.E. Treatment of Cancer-Associated VTE with Low-Molecular-Weight Heparin or Direct Oral Anticoagulants: Patient Selection, Controversies, and Caveats. Oncologist 2021, 26, e8–e16. [Google Scholar] [CrossRef]
- INSPIRATION Investigators; Sadeghipour, P.; Talasaz, A.H.; Rashidi, F.; Sharif-Kashani, B.; Beigmohammadi, M.T.; Farrokhpour, M.; Sezavar, S.H.; Payandemehr, P.; Dabbagh, A.; et al. Effect of intermediate-dose vs. standard-dose prophylactic anticoagulation on thrombotic events, extracorporeal membrane oxygenation treatment, or mortality among patients with COVID-19 admitted to the intensive care unit: The INSPIRATION randomized clinical trial. JAMA 2021, 325, 1620–1630. [Google Scholar] [PubMed]
- REMAP-CAP Investigators; ACTIV-4a Investigators; ATTACC Investigators; Goligher, E.C.; Bradbury, C.A.; McVerry, B.J.; Lawler, P.R.; Berger, J.S.; Gong, M.N.; Carrier, M.; et al. Therapeutic Anticoagulation with Heparin in Critically Ill Patients with Covid-19. N. Engl. J. Med. 2021, 385, 777–789. [Google Scholar]
- Ramacciotti, E.; Barile Agati, L.; Calderaro, D.; Aguiar, V.C.R.; Spyropoulos, A.C.; de Oliveira, C.C.C.; Lins Dos Santos, J.; Volpiani, G.G.; Sobreira, M.L.; Joviliano, E.E.; et al. Rivaroxaban versus no anticoagulation for post-discharge thromboprophylaxis after hospitalisation for COVID-19 (MICHELLE): An open-label, multicentre, randomised, controlled trial. Lancet 2022, 399, 50–59. [Google Scholar] [CrossRef]
- Spyropoulos, A.C.; Goldin, M.; Giannis, D.; Diab, W.; Wang, J.; Khanijo, S.; Mignatti, A.; Gianos, E.; Cohen, M.; Sharifova, G.; et al. Efficacy and Safety of Therapeutic-Dose Heparin vs. Standard Prophylactic or Intermediate-Dose Heparins for Thromboprophylaxis in High-risk Hospitalized Patients With COVID-19: The HEP-COVID Randomized Clinical Trial. JAMA Intern. Med. 2021, 181, 1612–1620. [Google Scholar] [CrossRef]
- Albani, F.; Sepe, L.; Fusina, F.; Prezioso, C.; Baronio, M.; Caminiti, F.; Di Maio, A.; Faggian, B.; Franceschetti, M.E.; Massari, M.; et al. Thromboprophylaxis with enoxaparin is associated with a lower death rate in patients hospitalized with SARS-CoV-2 infection. A cohort study. EClinicalMedicine. 2020, 27, 100562. [Google Scholar] [CrossRef] [PubMed]
- ATTACC Investigators; ACTIV-4a Investigators; REMAP-CAP Investigators; Lawler, P.R.; Goligher, E.C.; Berger, J.S.; Neal, M.D.; McVerry, B.J.; Nicolau, J.C.; Gong, M.N.; et al. Therapeutic Anticoagulation with Heparin in Noncritically Ill Patients with Covid-19. N. Engl. J. Med. 2021, 385, 790–802. [Google Scholar]
- COVID-19 and VTE/Anticoagulation: Frequently Asked Questions. Available online: https://www.hematology.org/covid-19/covid-19-and-vte-anticoagulation (accessed on 18 February 2021).
- Spyropoulos, A.C.; Levy, J.H.; Ageno, W.; Connors, J.M.; Hunt, B.J.; Iba, T.; Levi, M.; Samama, C.M.; Thachil, J.; Giannis, D.; et al. Scientific and Standardization Committee communication: Clinical guidance on the diagnosis, prevention, and treatment of VTE in hospitalized patients with COVID-19. J. Thromb. Haemost. 2020, 18, 1859–1865. [Google Scholar] [CrossRef]
- Spyropoulos, A.C.; Ageno, W.; Albers, G.W.; Elliott, C.G.; Halperin, J.L.; Hiatt, W.R.; Maynard, G.A.; Steg, P.G.; Weitz, J.I.; Suh, E.; et al. Rivaroxaban for Thromboprophylaxis after Hospitalization for Medical Illness. N. Engl. J. Med. 2018, 379, 1118–1127. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.T.; Spiro, T.E.; Büller, H.R.; Haskell, L.; Hu, D.; Hull, R.; Mebazaa, A.; Merli, G.; Schellong, S.; Spyropoulos, A.C.; et al. Rivaroxaban for thromboprophylaxis in acutely ill medical patients. N. Engl. J. Med. 2013, 368, 513–523. [Google Scholar] [CrossRef] [PubMed]
- Schunemann, H.J.; Cushman, M.; Burnett, A.E.; Kahn, S.R.; Beyer-Westendorf, J.; Spencer, F.A.; Rezende, S.M.; Zakai, N.A.; Bauer, K.A.; Dentali, F.; et al. American Society of Hematology 2018 guidelines for management of VTE: Prophylaxis for hospitalized and non-hospitalized medical patients. Blood Adv. 2018, 2, 3198–3225. [Google Scholar] [CrossRef]
- Salisbury, R.; Iotchkova, V.; Jaafar, S.; Morton, J.; Sangha, G.; Shah, A.; Untiveros, P.; Curry, N.; Shapiro, S. Incidence of symptomatic, image-confirmed VTE following hospitalization for COVID-19 with 90-day follow-up. Blood Adv. 2020, 4, 6230–6239. [Google Scholar] [CrossRef]
- Roberts, L.N.; Whyte, M.B.; Georgiou, L.; Giron, G.; Czuprynska, J.; Rea, C.; Vadher, B.; Patel, R.K.; Gee, E.; Arya, R. Postdischarge VTE following hospital admission with COVID-19. Blood 2020, 136, 1347–1350. [Google Scholar] [CrossRef]
- Giannis, D.; Allen, S.L.; Tsang, J.; Flint, S.; Pinhasov, T.; Williams, S.; Tan, G.; Thakur, R.; Leung, C.; Snyder, M.; et al. Post discharge thromboembolic outcomes and mortality of hospitalized patients with COVID-19: The CORE-19 registry. Blood 2021, 137, 2838–2847. [Google Scholar] [CrossRef]
- Kollias, A.; Kyriakoulis, K.G.; Stergiou, G.S.; Syrigos, K. Heterogeneity in reporting venous thromboembolic phenotypes in COVID-19: Methodological issues and clinical implications. Br. J. Haematol. 2020, 190, 529–532. [Google Scholar] [CrossRef] [PubMed]
- Enoxaparin Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2009/020164s085lbl.pdf (accessed on 14 June 2021).
- Hughes, S.; Szeki, I.; Nash, M.J.; Thachil, J. Anticoagulation in chronic kidney disease patients-the practical aspects. Clin. Kidney J. 2014, 7, 442–449. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, N.A.; Brenner, B. Thrombosis and Hemostasis Issues in Cancer Patients with COVID-19. Semin. Thromb. Hemost. 2020, 46, 785–788. [Google Scholar] [CrossRef]
- Brenner, B.; Ay, C.; Le Gal, G.; Carrier, M.; Muñoz, A.J.; Agnelli, G.; Rocha, A.T.C.; Abdel-Razeqh, H.; Elalamy, I.; Falanga, A. Venous thromboembolism risk, prophylaxis and management in cancer patients with COVID-19: An unmet medical need. Thromb. Update 2022, 6, 100098. [Google Scholar] [CrossRef]
- Paredes-Ruiz, D.; Gómez-Cuervo, C.; Gómez-Martín, C.; Sánchez-Guerrero, Á.; González-Olmedo, J.; López-López, F.; Bover-Larroya, M.; Yarza-Barrio, R.; Jara-Casas, D.D.; Castelo-Laureiro, A.; et al. Incidence of VTE in patients with non-hematological cancer admitted for COVID-19 at a third-level hospital in Madrid. J. Thromb. Thrombolysis. 2022, 52, 471–478. [Google Scholar] [CrossRef]
- Coronavirus (COVID-19) Infection in Pregnancy. Royal College of Obstetricians and Gynaecologists. Available online: https://www.rcog.org.uk/media/xsubnsma/2022-03-07-coronavirus-covid-19-infection-in-pregnancy-v15.pdf (accessed on 2 May 2022).
- Lim, W.; Dentali, F.; Eikelboom, J.W.; Crowther, M.A. Meta-analysis: Low-molecular-weight heparin and bleeding in patients with severe renal insufficiency. Ann. Intern. Med. 2006, 144, 673–684. [Google Scholar] [CrossRef]
- Hoffmann, P.; Keller, F. Increased major bleeding risk in patients with kidney dysfunction receiving enoxaparin: A meta-analysis. Eur. J. Clin. Pharmacol. 2012, 68, 757–765. [Google Scholar] [CrossRef] [PubMed]
- Siguret, V.; Gouin-Thibault, I.; Pautas, E.; Leizorovicz, A. No accumulation of the peak anti-factor Xa activity of tinzaparin in elderly patients with moderate-to-severe renal impairment: The IRIS substudy. J. Thromb. Haemost. 2011, 9, 1966–1972. [Google Scholar] [CrossRef] [PubMed]
- Scotte, F.; Rey, J.B.; Launay-Vacher, V. Thrombosis, cancer and renal insuf’ ficiency: Low molecular weight heparin at the crossroads. Support Care Cancer 2012, 20, 3033–3042. [Google Scholar] [CrossRef] [PubMed]
- Key, N.S.; Khorana, A.A.; Kuderer, N.M.; Bohlke, K.; Lee, A.Y.Y.; Arcelus, J.I.; Wong, S.L.; Balaban, E.P.; Flowers, C.R.; Francis, C.W.; et al. Venous Thromboembolism Prophylaxis and Treatment in Patients With Cancer: ASCO Clinical Practice Guideline Update. J. Clin. Oncol. 2020, 38, 496–520. [Google Scholar] [CrossRef]
- Farge, D.; Frere, C.; Connors, J.M.; Ay, C.; Khorana, A.A.; Munoz, A.; Brenner, B.; Kakkar, A.; Rafii, H.; International Initiative on Thrombosis and Cancer (ITAC) advisory panel; et al. 2019 international clinical practice guidelines for the treatment and prophylaxis of venous thromboembolism in patients with cancer. Lancet Oncol. 2019, 20, e566–e581. [Google Scholar] [CrossRef]
- Kamerkar, D.R.; John, M.J.; Desai, S.C.; Dsilva, L.C.; Joglekar, S.J. Arrive: A retrospective registry of Indian patients with VTE. Indian J. Crit. Care Med. 2016, 20, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Ramakrishnan, N.; Detect-Dvt Investigators. Prophylaxis and Incidence of Symptomatic Deep Vein Thrombosis in Indian Patients with Sepsis: DETECT-Deep Vein Thrombosis Registry. Indian J. Crit. Care Med. 2017, 21, 765–771. [Google Scholar]
- Liew, N.C.; Alemany, G.V.; Angchaisuksiri, P.; Bang, S.M.; Choi, G.; DE Silva, D.A.; Hong, J.M.; Lee, L.; Li, Y.J.; Rajamoney, G.N.; et al. Asian VTE guidelines: Updated recommendations for the prevention of VTE. Int. Angiol. 2017, 36, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Liew, N.C.; Chang, Y.H.; Choi, G.; Chu, P.H.; Gao, X.; Gibbs, H.; Ho, C.O.; Ibrahim, H.; Kim, T.K.; Kritpracha, B.; et al. Asian Venous Thrombosis Forum. Asian venous thromboembolism guidelines: Prevention of venous thromboembolism. Int. Angiol. 2012, 31, 501–516. [Google Scholar] [PubMed]
- AIIMS/ICMR-COVID-19 National Task Force/Joint Monitoring Group (Dte.GHS) Ministry of Health & Family Welfare, Government of India Clinical Guidance for Management of Adult COVID-19 Patients. Available online: https://www.icmr.gov.in/pdf/covid/techdoc/COVID_Clinical_Management_14012022.pdf (accessed on 7 June 2022).
- Mehta, Y.; Chaudhry, D.; Abraham, O.C.; Chacko, J.; Divatia, J.; Jagiasi, B.; Kar, A.; Khilnani, G.C.; Krishna, B.; Kumar, P.; et al. Critical care for COVID-19 affected patients: Updated position statement of the Indian Society of Critical Care Medicine. Indian J. Crit. Care Med. 2020, 24 (Suppl. S5), S225–S230. [Google Scholar] [PubMed]
- Clinical Trial NCT04730856. Available online: https://clinicaltrials.gov/ct2/show/NCT04730856?term=prophylactic+anticoagulants+for+thromboembolism+in+covid-19&draw=4&rank=20#contacts (accessed on 2 June 2021).
- Clinical Trial NCT04623177. Available online: https://clinicaltrials.gov/ct2/show/NCT04623177?term=prophylactic+anticoagulants+for+thromboembolism+in+covid-19&draw=4&rank=17 (accessed on 2 June 2021).
- Clinical Trial NCT04616846. Available online: https://clinicaltrials.gov/ct2/show/NCT04616846?term=prophylactic+anticoagulants+for+thromboembolism+in+covid-19&draw=2 (accessed on 2 June 2021).
- Clinical Trial NCT04542408. Available online: https://clinicaltrials.gov/ct2/show/NCT04542408 (accessed on 2 June 2021).
- Clinical Trial NCT04528888. Available online: https://clinicaltrials.gov/ct2/show/NCT04528888?term=prophylactic+anticoagulants+for+thromboembolism+in+covid-19&draw=4&rank=11 (accessed on 2 June 2021).
- Clinical Trial NCT04512079. Available online: https://clinicaltrials.gov/ct2/show/NCT04512079?term=prophylactic+anticoagulants+for+thromboembolism+in+covid-19&draw=4&rank=14#contacts (accessed on 2 June 2021).
- Clinical Trial NCT04505774. Available online: https://clinicaltrials.gov/ct2/show/NCT04505774?term=prophylactic+anticoagulants+for+thromboembolism+in+covid-19&draw=4&rank=19#contacts (accessed on 2 June 2021).
- Clinical Trial NCT04492254. Available online: https://clinicaltrials.gov/ct2/show/NCT04492254?term=prophylactic+anticoagulants+for+thromboembolism+in+covid-19&draw=4&rank=13 (accessed on 2 June 2021).
- Clinical Trial NCT04486508. Available online: https://clinicaltrials.gov/ct2/show/NCT04486508?term=prophylactic+anticoagulants+for+thromboembolism+in+covid-19&draw=4&rank=15 (accessed on 2 June 2021).
- Clinical Trial NCT04420299. Available online: https://clinicaltrials.gov/ct2/show/NCT04420299?term=prophylactic+anticoagulants+for+thromboembolism+in+covid-19&draw=2&rank=7#contacts (accessed on 2 June 2021).
- Clinical Trial NCT04416048. Available online: https://clinicaltrials.gov/ct2/show/NCT04416048?term=prophylactic+anticoagulants+for+thromboembolism+in+covid-19&draw=2&rank=2 (accessed on 2 June 2021).
- Clinical Trial NCT04409834. Available online: https://clinicaltrials.gov/ct2/show/NCT04409834?term=prophylactic+anticoagulants+for+thromboembolism+in+covid-19&draw=4&rank=16#contacts (accessed on 2 June 2021).
- Clinical Trial NCT04408235. Available online: https://clinicaltrials.gov/ct2/show/NCT04408235?term=prophylactic+anticoagulants+for+thromboembolism+in+covid-19&draw=4&rank=12#contacts (accessed on 2 June 2021).
- Clinical Trial NCT04406389. Available online: https://clinicaltrials.gov/ct2/show/NCT04406389?term=prophylactic+anticoagulants+for+thromboembolism+in+covid-19&draw=5&rank=21#contacts (accessed on 2 June 2021).
- Clinical Trial NCT04401293. Available online: https://clinicaltrials.gov/ct2/show/NCT04401293 (accessed on 2 June 2021).
- Clinical Trial NCT04367831. Available online: https://clinicaltrials.gov/ct2/show/NCT04367831?term=prophylactic+anticoagulants+for+thromboembolism+in+covid-19&draw=2&rank=1 (accessed on 2 June 2021).
- Clinical Trial NCT04373707. Available online: https://clinicaltrials.gov/ct2/show/NCT04373707?term=prophylactic+anticoagulants+for+thromboembolism+in+covid-19&draw=2&rank=4 (accessed on 2 June 2021).
- Clinical Trial NCT04360824. Available online: https://clinicaltrials.gov/ct2/show/NCT04360824?term=prophylactic+anticoagulants+for+thromboembolism+in+covid-19&draw=4&rank=18#contacts (accessed on 2 June 2021).
- Clinical Trial NCT04345848. Available online: https://clinicaltrials.gov/ct2/show/NCT04345848?term=prophylactic+anticoagulants+for+thromboembolism+in+covid-19&draw=2&rank=9 (accessed on 2 June 2021).
- Clinical Trial NCT04662684. Available online: https://clinicaltrials.gov/ct2/show/NCT04662684?term=anticoagulant+therapy+in+patients+with+COVID-19&cond=Venous+Thromboembolism&draw=2&rank=1 (accessed on 2 June 2021).
- Clinical Trial NCT04508023. Available online: https://clinicaltrials.gov/ct2/show/NCT04508023?term=covid-19 (accessed on 2 June 2021).


{kind=link}
{kind=link}
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramakrishnan, N.; Ramasubban, S.; Hegde, A.; Govil, D. Approach to Thromboprophylaxis for Prevention of Venous Thromboembolism in COVID-19: Global Updates and Clinical Insights from India. Clin. Pract. 2022, 12, 766-781. https://doi.org/10.3390/clinpract12050080
Ramakrishnan N, Ramasubban S, Hegde A, Govil D. Approach to Thromboprophylaxis for Prevention of Venous Thromboembolism in COVID-19: Global Updates and Clinical Insights from India. Clinics and Practice. 2022; 12(5):766-781. https://doi.org/10.3390/clinpract12050080
Chicago/Turabian StyleRamakrishnan, Nagarajan, Suresh Ramasubban, Ashit Hegde, and Deepak Govil. 2022. "Approach to Thromboprophylaxis for Prevention of Venous Thromboembolism in COVID-19: Global Updates and Clinical Insights from India" Clinics and Practice 12, no. 5: 766-781. https://doi.org/10.3390/clinpract12050080
APA StyleRamakrishnan, N., Ramasubban, S., Hegde, A., & Govil, D. (2022). Approach to Thromboprophylaxis for Prevention of Venous Thromboembolism in COVID-19: Global Updates and Clinical Insights from India. Clinics and Practice, 12(5), 766-781. https://doi.org/10.3390/clinpract12050080