A Case of Nasopharyngeal Tuberculosis with Cervical Lymph Node Tuberculosis Suspected of Cervical Malignant Disease at the First Examination

 ,
, {kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
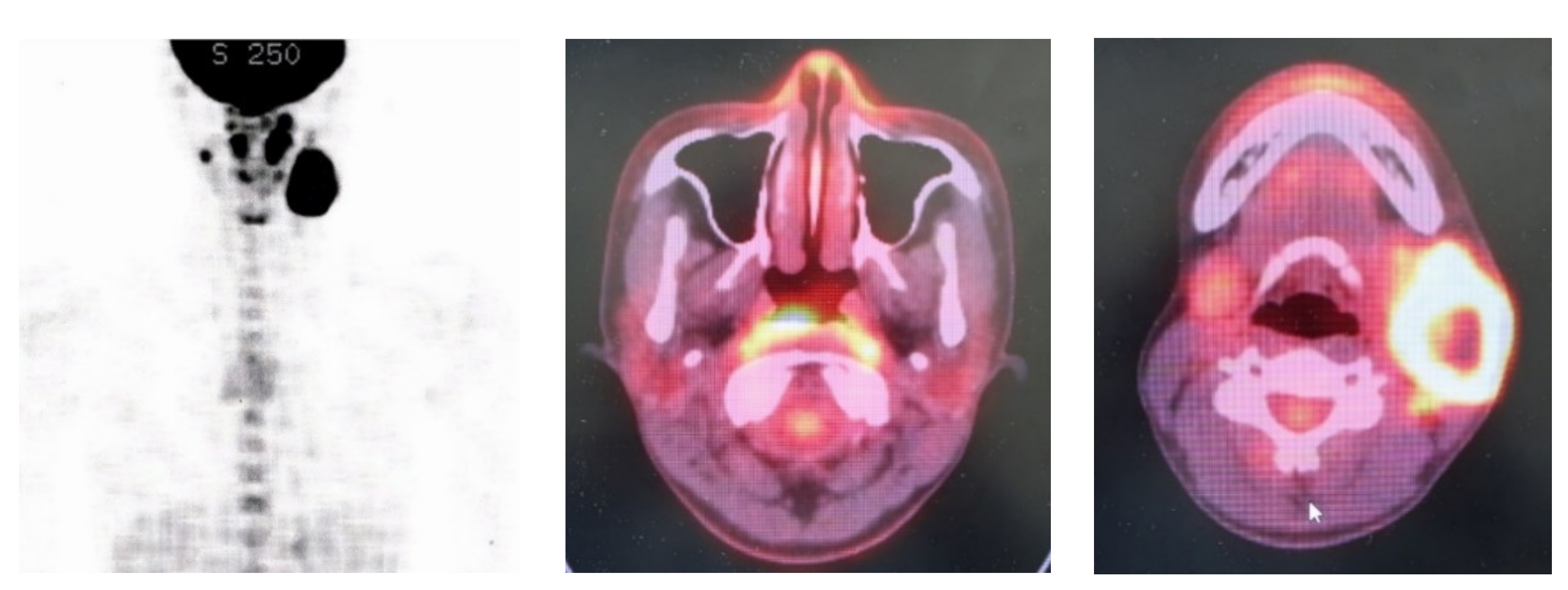
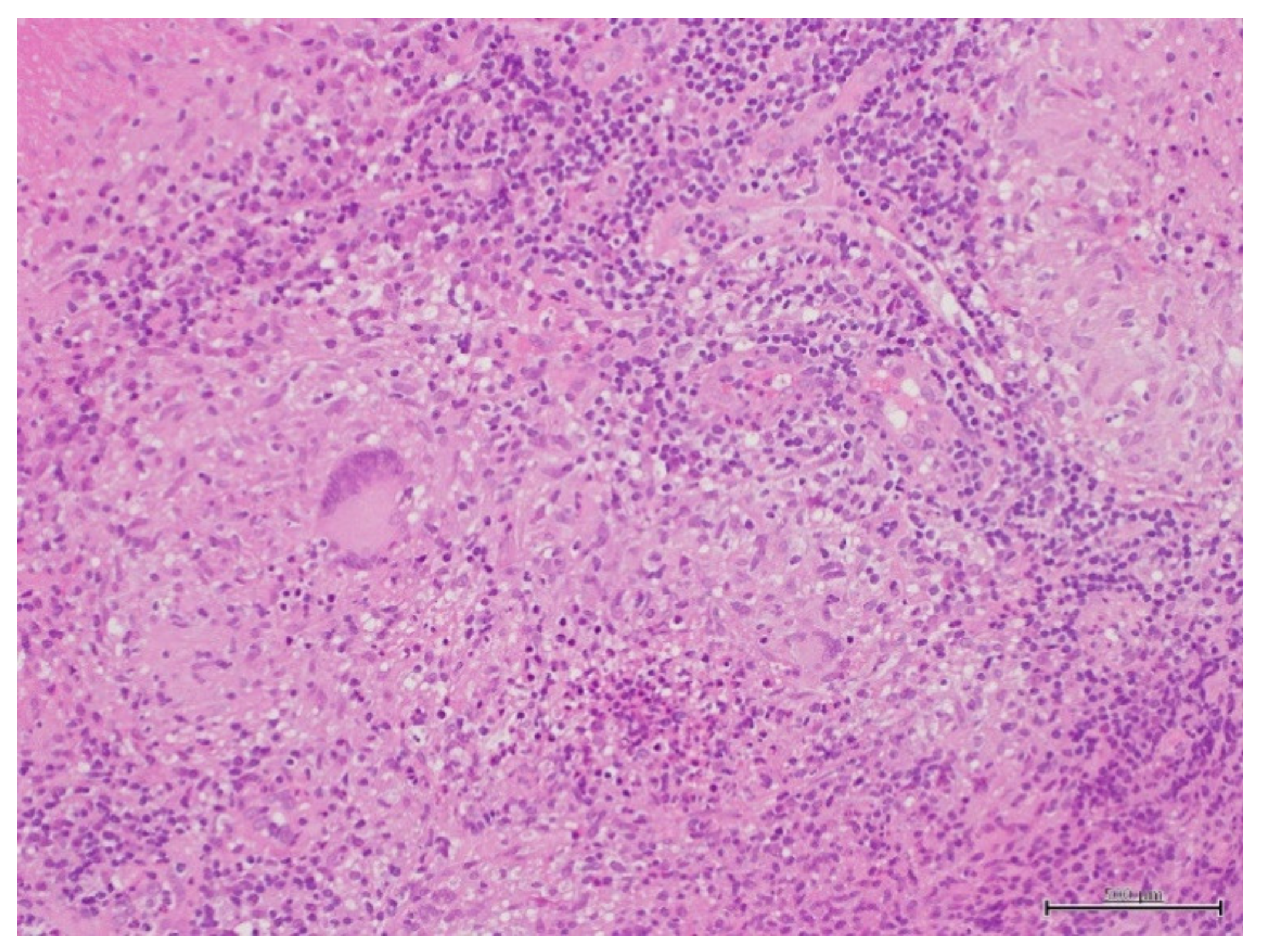
2. Case Report
3. Discussion
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kusunoki, T. Recent tuberculosis trends and practical points of the cervical lymph node tuberculosis. Pract. Otol. 2018, 111, 786–787. [Google Scholar] [CrossRef]
- Basal, Y.; Emisler, B.; Eryilmaz, A.; Ertuğrul, B. Two rare of head and neck tuberculosis. BMJ Case Rep. 2015, 2015. [Google Scholar] [CrossRef] [PubMed]
- Champion, L. Nasopharygeal tuberculosis incidentally diagnosed on 18F-FDG PET/CT. Int. J. Infect. Dis. 2020, 93, 295–296. [Google Scholar] [PubMed]
- Darouassi, Y.; Aljalil, A.; Hanine, A.; Enneouali, A.; Bouaity, B.; Touati, M.M.; Ammar, H. Nasopaharyngeal tuberculosis:report of four cases and review of the literature. Pan. Afr. Med. J. 2019, 27, 150. [Google Scholar]
- Mahindra, S.; Bazas, M.G.; Sohail, M. Primary tuberculosis of adenoids. Acta Otolaryngol. 1981, 92, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Lim, C.C.; Misron, K.; Loong, S.P.; Liew, Y.T.; Sawali, H. Primary adenotonsillar tuberculosis in an immunocomptent child—A case report. Iran. J. Otorhinolaryngol. 2019, 31, 319–322. [Google Scholar] [PubMed]
- Sugimoto, I.; Miyawaki, H. A case of primary nasopharyngeal tuberculosis. Pract. Otol. 2008, 101, 275–279. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kusunoki, T.; Homma, H.; Kidokoro, Y.; Yoshikawa, A.; Tanaka, K.; Kubo, S.; Wada, R.; Ikeda, K. A Case of Nasopharyngeal Tuberculosis with Cervical Lymph Node Tuberculosis Suspected of Cervical Malignant Disease at the First Examination. Clin. Pract. 2021, 11, 43-46. https://doi.org/10.3390/clinpract11010008
Kusunoki T, Homma H, Kidokoro Y, Yoshikawa A, Tanaka K, Kubo S, Wada R, Ikeda K. A Case of Nasopharyngeal Tuberculosis with Cervical Lymph Node Tuberculosis Suspected of Cervical Malignant Disease at the First Examination. Clinics and Practice. 2021; 11(1):43-46. https://doi.org/10.3390/clinpract11010008
Chicago/Turabian StyleKusunoki, Takeshi, Hirotomo Homma, Yoshinobu Kidokoro, Akihisa Yoshikawa, Kumiko Tanaka, Satoko Kubo, Ryo Wada, and Katsuhisa Ikeda. 2021. "A Case of Nasopharyngeal Tuberculosis with Cervical Lymph Node Tuberculosis Suspected of Cervical Malignant Disease at the First Examination" Clinics and Practice 11, no. 1: 43-46. https://doi.org/10.3390/clinpract11010008
APA StyleKusunoki, T., Homma, H., Kidokoro, Y., Yoshikawa, A., Tanaka, K., Kubo, S., Wada, R., & Ikeda, K. (2021). A Case of Nasopharyngeal Tuberculosis with Cervical Lymph Node Tuberculosis Suspected of Cervical Malignant Disease at the First Examination. Clinics and Practice, 11(1), 43-46. https://doi.org/10.3390/clinpract11010008