
Spiritual Intelligence in Healthcare Practice and Servant Leadership as Predictors of Work Life Quality in Peruvian Nurses



Abstract
1. Introduction
2. Methods
2.1. Study Design and Population
2.2. Instruments
2.3. Procedure
2.4. Ethical Considerations
2.5. Data Analysis
3. Results
3.1. Sociodemographic Characteristics of the Sample
3.2. Preliminary Analysis of the Variables
3.3. Assessment of Preliminary Assumptions
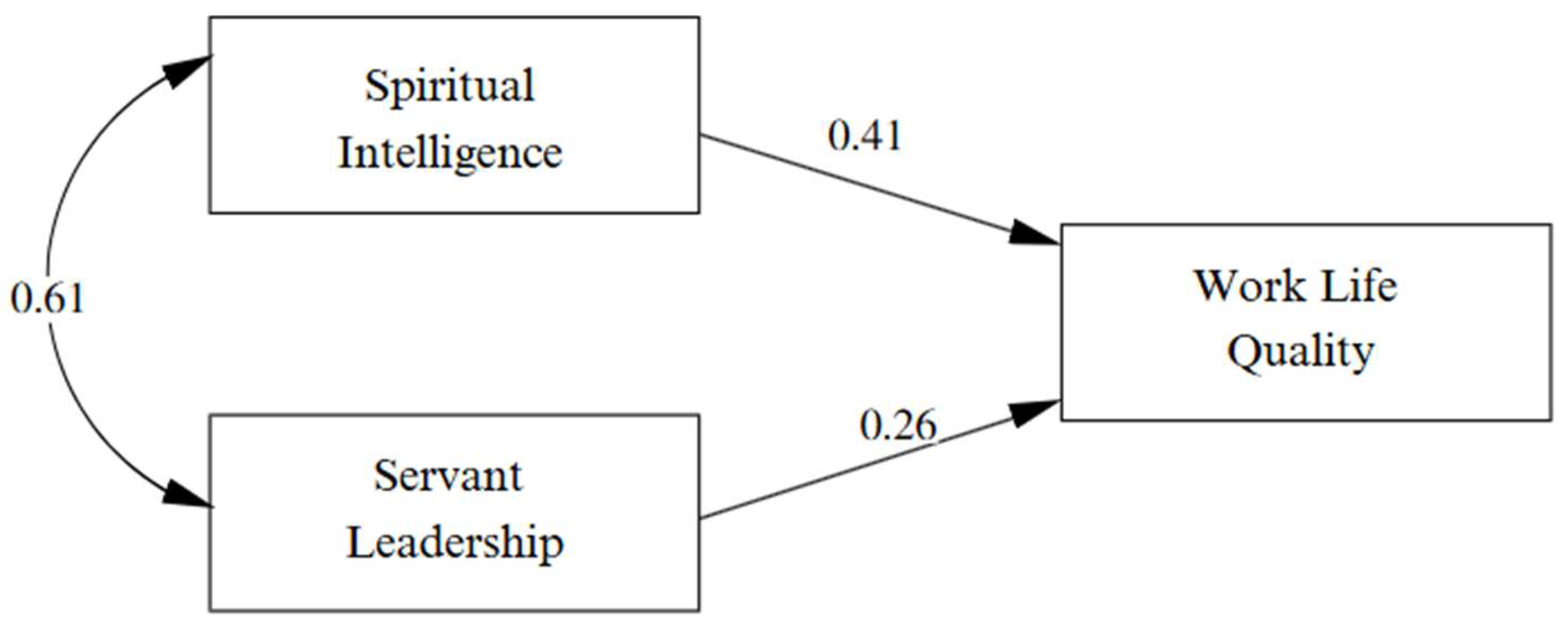
3.4. Structural Model
4. Discussion
4.1. Implications
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Use of Artificial Intelligence
Conflicts of Interest
References
- Shdaifat, E.; Al-Shdayfat, N.; Al-Ansari, N. Professional Quality of Life, Work-Related Stress, and Job Satisfaction among Nurses in Saudi Arabia: A Structural Equation Modelling Approach. J. Environ. Public Health 2023, 2023, 2063212. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Fernández, M.D.; Pérez-García, E.; Ortega-Galán, Á.M. Quality of life in nursing professionals: Burnout, fatigue, and compassion satisfaction. Int. J. Environ. Res. Public Health 2020, 17, 1253. [Google Scholar] [CrossRef] [PubMed]
- Sibuea, Z.M.; Sulastiana, M.; Fitriana, E. Factor Affecting the Quality of Work Life Among Nurses: A Systematic Review. J. Multidiscip. Healthc. 2024, 17, 491–503. [Google Scholar] [CrossRef] [PubMed]
- García-Sierra, R.; Fernández-Castro, J. Relationships between leadership, structural empowerment, and engagement in nurses. J. Adv. Nurs. 2018, 74, 2809–2819. [Google Scholar] [CrossRef]
- Hyson, P. The spirited leader: The potential of spiritual intelligence to improve leadership. Int. J. Leadersh. Public Serv. 2013, 9, 109–115. [Google Scholar] [CrossRef]
- Kourkouta, L.; Papathanasiou, I. Communication in Nursing Practice. Mater. Socio Medica 2014, 26, 65–67. [Google Scholar] [CrossRef]
- Fukada, M. Nursing Competency: Definition, Structure and Development. Yonago Acta Med. 2018, 61, 1–7. [Google Scholar] [CrossRef]
- Zohar, D. Spiritual Intelligence: The Ultimate Intelligence; Bloomsbury Publishing: London, UK, 2012. [Google Scholar]
- Moradnezhad, M.; Seylani, K.; Navab, E.; Esmaeilie, M. Spiritual intelligence of nurses working at the intensive care units of hospitals affiliated with Tehran University of Medical Sciences. Nurs. Pract. Today 2017, 4, 170–179. [Google Scholar]
- Alrashidi, N.; Alreshidi, M.S.; Dator, W.L.; Maestrado, R.; Villareal, S.; Buta, J.; Pangket, P.; Mostoles, R.J.; Gonzales, A.; Mina, E.; et al. The Mediating Role of Spiritual Intelligence on Well-Being and Life Satisfaction among Nurses in the Context of the COVID-19 Pandemic: A Path Analysis. Behav. Sci. 2022, 12, 515. [Google Scholar] [CrossRef]
- Vasconcelos, A.F. Spiritual intelligence: A theoretical synthesis and work-life potential linkages. Int. J. Organ. Anal. 2020, 28, 109–134. [Google Scholar] [CrossRef]
- Metwally, F.G.; Mohamed, H.M. Spiritual Intelligence as a Predictor of Work Engagement and Quality of Work Life among Nurses. Egypt. J. Health Care 2021, 12, 1218–1233. [Google Scholar] [CrossRef]
- Greenleaf, R.K. Servant leadership: A journey into the nature of legitimate power and greatness. In Business Horizons; Paulist Press: Mahwah, NJ, USA, 1977. [Google Scholar] [CrossRef]
- Eva, N.; Robin, M.; Sendjaya, S.; van Dierendonck, D.; Liden, R.C. Servant Leadership: A systematic review and call for future research. Leadersh. Q. 2019, 30, 111–132. [Google Scholar] [CrossRef]
- Liden, R.C.; Wayne, S.J.; Liao, C.; Meuser, J.D. Servant leadership and serving culture: Influence on individual and unit performance. Acad. Manag. J. 2014, 57, 1434–1452. [Google Scholar] [CrossRef]
- Sousa, M.; van Dierendonck, D. Servant Leadership and the Effect of the Interaction Between Humility, Action, and Hierarchical Power on Follower Engagement. J. Bus. Ethic 2015, 141, 13–25. [Google Scholar] [CrossRef]
- Cruz, J.P.; Alquwez, N.; Mesde, J.H.; Almoghairi, A.M.A.; Altukhays, A.I.; Colet, P.C. Spiritual climate in hospitals influences nurses’ professional quality of life. J. Nurs. Manag. 2020, 28, 1589–1597. [Google Scholar] [CrossRef]
- Ato, M.; López, J.; Benavente, A. Un sistema de clasificación de los diseños de investigación en psicología. Anales de Psicología 2013, 29, 1038–1059. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; Cuarta, Ed.; Guilford Press: New York, NY, USA, 2016. [Google Scholar]
- Soper, D. A-Priori Sample Size Calculator for Structural Equation Models [Software]; Daniel Soper: Fullerton, CA, USA, 2024. [Google Scholar]
- Moreno, M.P.; Baltazar, R.G.; Beltrán, C.A.; Núñez, F.E. Fiabilidad y validez factorial del instrumento para medir calidad de vida en el trabajo “CVT-Gohisalo”(versión breve). Rev. Salud Uninorte 2018, 34, 68–75. [Google Scholar]
- Sanchez, P.; Rojas, W.; Terrones, S.; Quinteros, D.; Carranza, R. Liderazgo de servicio como predictor del rendimiento laboral en colaboradores municipales de la provincia de San Martín, en el contexto de COVID-19. Rev. Asoc. Española Espec. Med. Trab. 2023, 31, 45–53. [Google Scholar]
- Dennis, R.; Winston, B.E. A factor analysis of Page and Wong’s servant leadership instrument. Leadersh. Organ. Dev. J. 2003. [Google Scholar] [CrossRef]
- Becerra Canales, B.; Becerra Huaman, D. Diseño y validación de la escala de Inteligencia Espiritual en la práctica sanitaria, Ica-Perú. Enfermería Global 2020, 349–378. [Google Scholar] [CrossRef]
- Little, R.J.A.; Rubin, D.B. Statistical Analysis with Missing Data; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2014. [Google Scholar] [CrossRef]
- Brown, T. Confirmatory Factor Analysis for Applied Research; Guildford Press: New York, NY, USA, 2006. [Google Scholar]
- Bentler, P. Comparative fit indices in structural models. Psychol. Bull. 1990, 107, 238–246. [Google Scholar] [CrossRef] [PubMed]
- MacCallum, R.C.; Browne, M.W.; Sugawara, H.M. Power Analysis and determination of sample size for covariance structure modeling of fit involving a particular measure of model. Psychol. Methods 1996, 13, 130–149. [Google Scholar] [CrossRef]
- Browne, M.W.; Cudeck, R. Alternative Ways of Assessing Model Fit. Sociol. Methods Res. 1992, 21, 230–258. [Google Scholar] [CrossRef]
- Allaire, J.J. RStudio: Integrated Development Environment for R; R Foundation for Statistical Computing: Vienna, Austria, 2018. [Google Scholar]
- Rosseel, Y. lavaan: An R Package for Structural Equation Modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef]

{kind=link}
| Characteristic | Category | n | % |
|---|---|---|---|
| Years of Experience | >10 years | 51 | 38.10% |
| 1 year | 7 | 5.20% | |
| 2–5 years | 32 | 23.90% | |
| 6–10 years | 44 | 32.80% | |
| Marital Status | Married | 53 | 39.60% |
| Divorced | 7 | 5.20% | |
| Single | 74 | 55.20% | |
| Has Children | No | 68 | 50.70% |
| Yes | 66 | 49.30% | |
| Educational Level | Specialist | 68 | 50.70% |
| Bachelor’s Degree | 43 | 32.10% | |
| Master’s Degree | 7 | 5.20% | |
| Other | 16 | 11.90% |
| Variable | M | DE | α | ω | A | K | 1 | 2 | 3 |
|---|---|---|---|---|---|---|---|---|---|
| 1. Spiritual Intelligence | 40.38 | 4.41 | 0.91 | 0.91 | −2.14 | 6.55 | — | ||
| 2. Servant Leadership | 65.93 | 8.32 | 0.95 | 0.93 | −1.41 | 2.73 | 0.44 ** | — | |
| 3. Work Life Quality | 76.27 | 13.92 | 0.93 | 0.92 | −0.79 | 0.14 | 0.40 ** | 0.53 ** | — |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dávila-Valencia, P.K.; Gala-Espinoza, B.J.; Morales-García, W.C. Spiritual Intelligence in Healthcare Practice and Servant Leadership as Predictors of Work Life Quality in Peruvian Nurses. Nurs. Rep. 2025, 15, 249. https://doi.org/10.3390/nursrep15070249
Dávila-Valencia PK, Gala-Espinoza BJ, Morales-García WC. Spiritual Intelligence in Healthcare Practice and Servant Leadership as Predictors of Work Life Quality in Peruvian Nurses. Nursing Reports. 2025; 15(7):249. https://doi.org/10.3390/nursrep15070249
Chicago/Turabian StyleDávila-Valencia, Paula K., Belvi J. Gala-Espinoza, and Wilter C. Morales-García. 2025. "Spiritual Intelligence in Healthcare Practice and Servant Leadership as Predictors of Work Life Quality in Peruvian Nurses" Nursing Reports 15, no. 7: 249. https://doi.org/10.3390/nursrep15070249
APA StyleDávila-Valencia, P. K., Gala-Espinoza, B. J., & Morales-García, W. C. (2025). Spiritual Intelligence in Healthcare Practice and Servant Leadership as Predictors of Work Life Quality in Peruvian Nurses. Nursing Reports, 15(7), 249. https://doi.org/10.3390/nursrep15070249