Developing Burdens in Caring for a Relative with a Cancer Diagnosis: A Qualitative Study of Lived Experiences of Family Caregivers in Saudi Arabia


Abstract
1. Introduction
2. Methods
2.1. Design
2.2. Setting
2.3. Sampling
2.4. Data-Collection Instrument and Procedure
2.5. Trustworthiness
2.6. Ethical Considerations
2.7. Data Analysis
3. Results
3.1. Personal Data of Family Caregivers of Patients with a Cancer Diagnosis
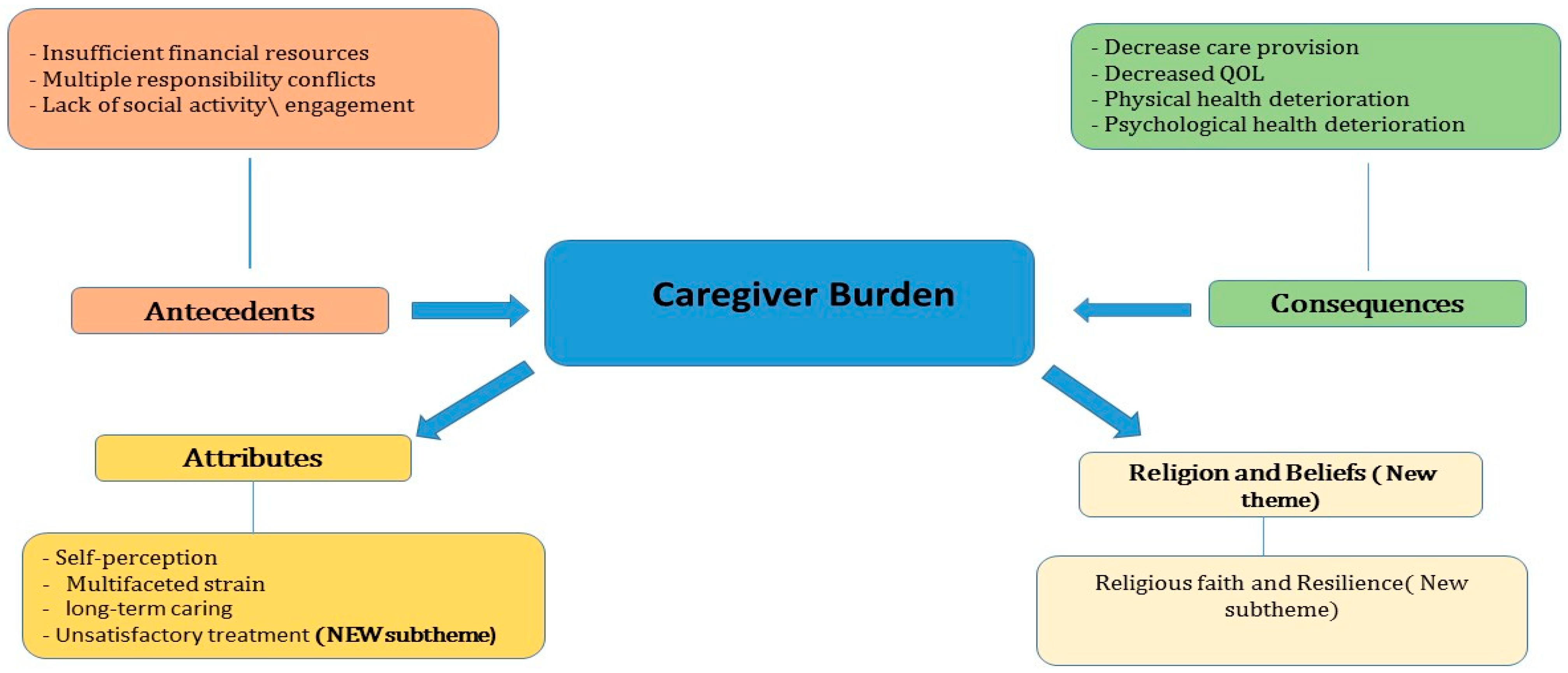
3.2. Theme 1: Antecedents to the Caregiving Burden
3.2.1. Insufficient Financial Resources
3.2.2. Multiple Responsibility Conflicts
3.2.3. Lack of Social Activity
3.3. Theme 2: Attributes of the Caregiving Burden
3.3.1. Self-Perception
3.3.2. Multifaceted Strain
3.3.3. Long-Term Care
3.3.4. Unsatisfactory Treatment (New Sub-Theme)
3.4. Theme 3: Consequences of the Caregiving Burden
3.4.1. Decreased Quality of Life
3.4.2. Decreased Care Provision
3.4.3. Physical Health Deterioration
3.4.4. Psychological Health Deterioration
3.5. Theme 4: Religion and Beliefs (New Theme)
Religious Faith and Resilience
4. Discussion
5. Limitations
Implications for Nurses
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Use of Artificial Intelligence
Conflicts of Interest
Abbreviations
| KSA | Kingdom of Saudi Arabia |
| FCGs | Family Caregivers |
References
- World Health Organization (WHO). Global Cancer Burden Growing, Amidst Mounting Need for Services. Available online: https://www.who.int/news/item/01-02-2024-global-cancer-burden-growing--amidst-mounting-need-for-services (accessed on 28 May 2025).
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2018, 144, 1941–1953. [Google Scholar] [CrossRef] [PubMed]
- Almatroudi, A. The incidence rate of colorectal cancer in Saudi Arabia: An observational descriptive epidemiological analysis. Int. J. Gen. Med. 2020, 13, 977–990. [Google Scholar] [CrossRef] [PubMed]
- Hsu, T.; Loscalzo, M.; Ramani, R.; Forman, S.; Popplewell, L.; Clark, K.; Katheria, V.; Feng, T.; Strowbridge, R.; Rinehart, R.; et al. Factors associated with high burden in caregivers of older adults with cancer. Cancer 2014, 120, 2927–2935. [Google Scholar] [CrossRef] [PubMed]
- Röing, M.; Hirsch, J.; Holmström, I. Living in a state of suspension—A phenomenological approach to the spouse’s experience of oral cancer. Scand. J. Caring Sci. 2008, 22, 40–47. [Google Scholar] [CrossRef]
- Girgis, A.; Lambert, S.; Johnson, C.; Waller, A.; Currow, D. Physical, Psychosocial, Relationship, and Economic Burden of Caring for People With Cancer: A Review. J. Oncol. Pract. 2013, 9, 197–202. [Google Scholar] [CrossRef]
- Tedla, J.S.; Asiri, F.; Sangadala, D.R.; Mukherjee, D.; Reddy, R.S.; Gular, K. Quality of Life Among Family Caregivers of Children with Disabilities in the Kingdom of Saudi Arabia. A Systematic Review; INPLASY—International Platform of Registered Systematic Review and Meta-Analysis Protocols: Middletown, DE, USA, 2023. [Google Scholar] [CrossRef]
- Sennfält, S.; Ullberg, T. Response to the Letter-to-the-Editor by Kajiwara et al. Int. J. Stroke 2019, 14, NP2. [Google Scholar] [CrossRef]
- Maimani, D.; Alhumedi, N.; Alghamdi, A. The Prevalence of Psychological Morbidities and the Determinant of care givers of children with intellectual disabilities, in specialized centers in Jeddah 2018. J. Prev. Med. Holist. Health 2019, 5, 27–31. [Google Scholar] [CrossRef]
- Haematology, T.L. Caregivers—An undervalued and underused essential. Lancet Haematol. 2022, 9, e707. [Google Scholar] [CrossRef]
- Al Saffer, Q.; Hariri, B.; Alhuseini, M.; Aljanoubi, H.; Bah, S.; Al Rais, S. Unsung Heroes: An Overview of the Informal Caregivers in the Gulf Cooperation Council—A Scoping Review and Thematic Analysis. Saudi J. Health Syst. Res. 2024, 4, 155–184. [Google Scholar] [CrossRef]
- Aloudiny, W.H.; Alsaran, F.F.; Alessa, F.M.; Almoayad, F.; Fiala, L. Examining Emotional and Physical Burden in Informal Saudi Caregivers: Links to Quality of Life and Social Support. Healthcare 2024, 12, 1851. [Google Scholar] [CrossRef]
- Jabeen, S.; Zakar, R.; Zakar, M.Z.; Fischer, F. Experiences of family caregivers in dealing with cases of advanced breast cancer: A qualitative study of the sociocultural context in Punjab, Pakistan. BMC Public Health 2024, 24, 1030. [Google Scholar] [CrossRef] [PubMed]
- Ho, H.T.; Jenkins, C.; Nghiem, H.L.P.; Hoang, M.V.; Santin, O. Understanding context: A qualitative analysis of the roles of family caregivers of people living with cancer in Vietnam and the implications for service development in low-income settings. Psychooncology 2021, 30, 1782–1788. [Google Scholar] [CrossRef] [PubMed]
- Hrar, Y.; Farhan, M. Working with Families, Infants, and Young Children from the Middle East. In Clinical Handbook of Transcultural Infant Mental Health; Springer: Cham, Switzerland, 2019; pp. 121–131. [Google Scholar] [CrossRef]
- Sibai, A.M.; Yamout, R. Family-Based Old-Age Care in Arab Countries: Between Tradition and Modernity. In Population Dynamics in Muslim Countries; Springer: Berlin/Heidelberg, Germany, 2012; pp. 63–76. [Google Scholar] [CrossRef]
- Kusi, G.; Boamah Mensah, A.B.; Boamah Mensah, K.; Dzomeku, V.M.; Apiribu, F.; Duodu, P.A.; Adamu, B.; Agbadi, P.; Bonsu, K.O. The experiences of family caregivers living with breast cancer patients in low-and middle-income countries: A systematic review. Syst. Rev. 2020, 9, 165. [Google Scholar] [CrossRef]
- Mlaba, P.C.; Ginindza, T.G.; Hlongwana, K.W. The social burden experienced by families caring for members living with cancer in KwaZulu-Natal, South Africa. Afr. J. Prim. Health Care Fam. Med. 2021, 13, a2955. [Google Scholar] [CrossRef]
- Najjuka, S.M.; Iradukunda, A.; Kaggwa, M.M.; Sebbowa, A.N.; Mirembe, J.; Ndyamuhaki, K.; Nakibuule, C.; Atuhaire, J.P.; Nabirye, E.; Namukwaya, E.; et al. The experience of caregivers living with cancer patients: A systematic review and meta-synthesis. PLoS ONE 2021, 13, 1–24. [Google Scholar] [CrossRef]
- Hassankhani, H.; Eghtedar, S.; Rahmani, A.; Ebrahimi, H.; Whitehead, B. A Qualitative Study on Cancer Care Burden: Experiences of Iranian Family Caregivers. Holist. Nurs. Pract. 2019, 33, 17–26. [Google Scholar] [CrossRef]
- Muliira, J.K.; Kizza, I.B.; Nakitende, G. Roles of family caregivers and perceived burden when caring for hospitalized adult cancer patients: Perspective from a low-income country. Cancer Nurs. 2019, 42, 208–217. [Google Scholar] [CrossRef]
- Northfield, S.; Nebauer, M. The caregiving journey for family members of relatives with cancer: How do they cope? Clin. J. Oncol. Nurs. 2010, 14, 567–577. [Google Scholar] [CrossRef]
- Williams, A.L.; Tisch, A.J.H.; Dixon, J.; McCorkle, R. Factors associated with depressive symptoms in cancer family caregivers of patients receiving chemotherapy. Support. Care Cancer 2013, 21, 2387–2394. [Google Scholar] [CrossRef]
- Thana, K.; Lehto, R.; Sikorskii, A.; Wyatt, G. Informal caregiver burden for solid tumour cancer patients: A review and future directions. Psychol. Health 2021, 36, 1514–1535. [Google Scholar] [CrossRef]
- Saimaldaher, Z.H.; Wazqar, D.Y. Relationships between caregiving stress, mental health and physical health in family caregivers of adult patients with cancer: Implications for nursing practice. Scand. J. Caring Sci. 2019, 34, 889–898. [Google Scholar] [CrossRef] [PubMed]
- Ghazwani, E.Y.; Al-Shehri, A.A.; Alghamdi, F.A. Assessment of Burden and Stress Among Caregivers of Terminally Ill Patients in a Saudi University Hospital: A Cross-Sectional Study. Cureus 2021, 13, e14215. [Google Scholar] [CrossRef]
- Mohamed Hussin, N.A.; Mohd Sabri, N.S. A qualitative exploration of the dynamics of guilt experience in family cancer caregivers. Support. Care Cancer 2023, 31, 659. [Google Scholar] [CrossRef] [PubMed]
- Giorgi, A. The Theory, Practice, and Evaluation of the Phenomenological Method as a Qualitative Research Procedure. J. Phenomenol. Psychol. 1997, 28, 235–260. [Google Scholar] [CrossRef]
- Penner, J.L.; McClement, S.E. Using Phenomenology to Examine the Experiences of Family Caregivers of Patients with Advanced Head and Neck Cancer: Reflections of a Novice Researcher. Int. J. Qual. Methods 2008, 7, 92–101. [Google Scholar] [CrossRef]
- Hafez, S.A.; Snethen, J.A.; Ngui, E.; Ellis, J.; Taani, M. Pediatric End of Life Care: Impact of Islamic Faith. West. J. Nurs. Res. 2021, 44, 773–779. [Google Scholar] [CrossRef]
- Malar, M.P.; Jain, A.; Holla, R.; Rao, R.; Rao, M.; Jose, J. IJCM_148A: Difference in unmet supportive care needs of patients and informal caregivers with advanced cancer, between developed and developing countries: A scoping review. Indian J. Community Med. 2024, 49, S43. [Google Scholar] [CrossRef]
- Ang, S.H.M.; Poon, W.H.E.; Best, O.; Graham, C. Exploring the lived experience of Chinese family caregivers caring for end-of-life cancer patients at home: A phenomenological study in Singapore. Support. Care Cancer 2025, 33, 111. [Google Scholar] [CrossRef]
- Kereszturi, A. Family caregivers’ lived experience of caring for hospitalised patients with cancer during the COVID-19 lockdown: A descriptive phenomenological study. J. Clin. Nurs. 2023, 32, 7509–7518. [Google Scholar] [CrossRef]
- Magnone, K.Q.; Yezierski, E.J. Beyond Convenience: A Case and Method for Purposive Sampling in Chemistry Teacher Professional Development Research. J. Chem. Educ. 2024, 101, 718–726. [Google Scholar] [CrossRef]
- Funder, D.C.; Ozer, D.J. Evaluating Effect Size in Psychological Research: Sense and Nonsense. Adv. Methods Pract. Psychol. Sci. 2019, 2, 156–168. [Google Scholar] [CrossRef]
- Mweshi, G.K.; Sakyi, K. Application of sampling methods for the research design. Arch. Bus. Res. 2020, 8, 180–193. [Google Scholar] [CrossRef]
- Fusch, P.; Ness, L. Are We There Yet? Data Saturation in Qualitative Research. Qual. Rep. 2015, 20, 1408–1416. [Google Scholar] [CrossRef]
- Morse, J.M. “Data Were Saturated…”. Qual. Health Res. 2015, 25, 587–588. [Google Scholar] [CrossRef] [PubMed]
- Mayer, M.; Sampayo, I.; Bell Dickson, R.; Citron, M.L.; Brufsky, A.M. Abstract P1-11-06: The experience of caregivers of women with metastatic breast cancer: Insights from the Make Your Dialogue Count survey. Cancer Res. 2016, 76 (Suppl. S4), P1-11-06. [Google Scholar] [CrossRef]
- Lkhoyaali, S.; Ait El Haj, M.; Raissouni, S.; Rais, G.; Mrabti, H.; Errihani, H. Family Caregiver Burden: Results of A Moroccan Prospective Study of Cancer in The Elderly and their Caregivers. Ann. Oncol. 2012, 23, ix476. [Google Scholar] [CrossRef]
- Paek, M.-S.; Nightingale, C.L.; Tooze, J.A.; Milliron, B.-J.; Weaver, K.E.; Sterba, K.R. Contextual and stress process factors associated with head and neck cancer caregivers’ physical and psychological well-being. Eur. J. Cancer Care 2018, 27, e12833. [Google Scholar] [CrossRef]
- Geiger, B.F.; O’Neal, M.R. Determining caregiver needs for respite, results of an Alabama survey. J. Nurs. Educ. Pract. 2013, 4, 1–11. [Google Scholar] [CrossRef]
- TalkadSukumar, P.; Metoyer, R. Replication and Transparency of Qualitative Research from a Constructivist Perspective. 2019. Available online: https://osf.io/preprints/6efvp/ (accessed on 26 September 2024).
- Carnot, M.L.; Bernardino, J.; Laranjeiro, N.; Oliveira, H.G. Applying text analytics for studying research trends in dependability. Entropy 2020, 22, 1303. [Google Scholar] [CrossRef]
- Rubin, M. Does preregistration improve the credibility of research findings? Quant. Methods Psychol. 2020, 16, 376–390. [Google Scholar] [CrossRef]
- McDonald, N.; Schoenebeck, S.; Forte, A. Reliability and inter-rater reliability in qualitative research: Norms and guidelines for CSCW and HCI practice. Proc. ACM Hum.-Comput. Interact. 2019, 3, 1–23. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Guest, G.; Namey, E.E.; Mitchell, M.L. Collecting Qualitative Data: A Field Manual for Applied Research; SAGE Publications, Ltd.: London, UK, 2013; ISBN 9781412986847. [Google Scholar]
- Guba, E. Research YLH of Qualitative, 1994 Undefined. Competing Paradigms in Qualitative Research. Available online: http://miguelangelmartinez.net/IMG/pdf/1994_Guba_Lincoln_Paradigms_Quali_Research_chapter.pdf (accessed on 28 September 2024).
- Temple, B.; Young, A. Qualitative Research and Translation Dilemmas. Qual. Res. 2004, 4, 161–178. [Google Scholar] [CrossRef]
- Shivji, N.A.; Meade, O.; Watts, K.; Lymn, J.S. Reflecting on ‘insider’ and ‘outsider’ positionality when undertaking culturally sensitive research with young Pakistani men: Insights from a female researcher. Nurse Res. 2022, 30, 24–29. [Google Scholar] [CrossRef]
- Liu, Z.; Heffernan, C.; Tan, J. Caregiver burden: A concept analysis. Int. J. Nurs. Sci. 2020, 7, 438–445. [Google Scholar] [CrossRef]
- Senden, C.; Vandecasteele, T.; Vandenberghe, E.; Versluys, K.; Piers, R.; Grypdonck, M.; Van Den Noortgate, N. The interaction between lived experiences of older patients and their family caregivers confronted with a cancer diagnosis and treatment: A qualitative study. Int. J. Nurs. Stud. 2015, 52, 197–206. [Google Scholar] [CrossRef]
- Lee, Y.; Zurlo, K.A. Spousal caregiving and financial strain among middle-aged and older adults. Int. J. Aging Hum. Dev. 2014, 79, 302–321. [Google Scholar] [CrossRef]
- Given, C.W. Family Caregiving for Cancer Patients: The State of the Literature and a Direction for Research to Link the Informal and Formal Care Systems to Improve Quality and Outcomes. Semin. Oncol. Nurs. 2019, 35, 389–394. [Google Scholar] [CrossRef]
- Gabriel, I.O. Caregiver Burden among Informal Caregivers of Women with Breast Cancer. Biomed. J. Sci. Tech. Res. 2019, 15, 11384–11392. [Google Scholar] [CrossRef]
- Moreno-González, M.M.; Galarza-Tejada, D.M.; Tejada-Tayabas, L.M. Experiencias del cuidado familiar durante el cáncer de mama: La perspectiva de los cuidadores. Rev. Esc. Enferm. USP 2019, 53, 1–9. [Google Scholar] [CrossRef]
- Gabriel, I.; Creedy, D.; Coyne, E. Quality of life and associated factors among adults living with cancer and their family caregivers. Nurs. Health Sci. 2021, 23, 419–429. [Google Scholar] [CrossRef]
- Hounsell, C.; Jed Johnson, W.; Seals Carol Levine, E.; Stein, R.; Vuckovic, N.; Donna Wagner, I.; Wolff, J.; Weber-Raley, L.; Smith, E.; Gibson Hunt, G.; et al. Caregiving in the U.S.—AARP 2019 Report; AARP: Washington, DC, USA, 2019; Volume 81. [Google Scholar]
- Stamataki, Z.; Ellis, J.E.; Costello, J.; Fielding, J.; Burns, M.; Molassiotis, A. Chronicles of informal caregiving in cancer: Using ‘The Cancer Family Caregiving Experience’ model as an explanatory framework. Support. Care Cancer 2013, 22, 435–444. [Google Scholar] [CrossRef]
- Goldstein, N.E.; Johnson, R.W. Factors Associated with Caregiver Burden Among Caregivers of Tenninally TIl Patients With Cancer. J. Palliat Care 2004, 20, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Noble, H.; Kelly, D.; Hudson, P. Experiences of carers supporting dying renal patients managed without dialysis. J. Adv. Nurs. 2012, 69, 1829–1839. [Google Scholar] [CrossRef] [PubMed]
- Sajjadi, M.; Rassouli, M.; Abbaszadeh, A.; Brant, J.; Majd, H.A. Lived Experiences of “Illness Uncertainty” of Iranian Cancer Patients. Cancer Nurs. 2016, 39, E1–E9. [Google Scholar] [CrossRef] [PubMed]
- Hodge, D.R.; Sun, F. Positive feelings of caregiving among Latino Alzheimer’s family caregivers: Understanding the role of spirituality. Aging Ment. Health 2012, 16, 689–698. [Google Scholar] [CrossRef]
- Nemati, S.; Rassouli, M.; Ilkhani, M.; Baghestani, A.R. Perceptions of family caregivers of cancer patients about the challenges of caregiving: A qualitative study. Scand. J. Caring Sci. 2018, 32, 309–316. [Google Scholar] [CrossRef]
- Nakken, N.; Spruit, M.A.; Wouters, E.F.M.; Schols, J.M.G.A.; Janssen, D.J.A. Family caregiving during 1-year follow-up in individuals with advanced chronic organ failure. Scand. J. Caring Sci. 2015, 29, 734–744. [Google Scholar] [CrossRef]
- De Korte-Verhoef, M.C.; Pasman, H.R.W.; Schweitzer, B.P.M.; Francke, A.L.; Onwuteaka-Philipsen, B.D.; Deliens, L. Burden for family carers at the end of life; a mixed-method study of the perspectives of family carers and GPs. BMC Palliat. Care 2014, 13, 16. [Google Scholar] [CrossRef]
- Yoon, S.-J.; Kim, J.-S.; Jung, J.-G.; Kim, S.-S.; Kim, S. Modifiable factors associated with caregiver burden among family caregivers of terminally ill Korean cancer patients. Support. Care Cancer 2014, 22, 1243–1250. [Google Scholar] [CrossRef]
- Ateş, G.; Ebenau, A.F.; Busa, C.; Csikos, Á.; Hasselaar, J.; Jaspers, B.; Menten, J.; Payne, S.; Van Beek, K.; Varey, S.; et al. “Never at ease”—Family carers within integrated palliative care: A multinational, mixed method study. BMC Palliat. Care 2018, 17, 39. [Google Scholar] [CrossRef] [PubMed]
- Arian, M.; Younesi, S.J.; Khanjani, M.S. Explaining the Experiences and Consequences of Care Among Family Caregivers of Patients with Cancer in the Terminal Phase: A Qualitative Research. Int. J. Cancer Manag. 2017, 10, e10753. [Google Scholar] [CrossRef]
- Lee, Y.; Liao, Y.; Shun, S.; Lin, K.; Liao, W.; Chang, P.; Jhang, S.; Yu, C.; Yang, P.; Hsieh, P.; et al. Trajectories of caregiver burden and related factors in family caregivers of patients with lung cancer. Psychooncology 2018, 27, 1493–1500. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Dolansky, M.A.; Hu, X.; Zhang, F.; Qu, M. Factors associated with the caregiver burden among family caregivers of patients with heart failure in southwest China. Nurs. Health Sci. 2016, 18, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Unsar, S.; Erol, O.; Ozdemir, O. Caregiving burden, depression, and anxiety in family caregivers of patients with cancer. Eur. J. Oncol. Nurs. 2021, 50, 101882. [Google Scholar] [CrossRef]
- Naoki, Y.; Matsuda, Y.; Maeda, I.; Kamino, H.; Kozaki, Y.; Tokoro, A.; Maki, N.; Takada, M. Association between family satisfaction and caregiver burden in cancer patients receiving outreach palliative care at home. Palliat. Support. Care 2017, 16, 260–268. [Google Scholar] [CrossRef]
- Lewandowska, A.; Rudzki, G.; Lewandowski, T.; Rudzki, S. The problems and needs of patients diagnosed with cancer and their caregivers. Int. J. Environ. Res. Public Health 2021, 18, 87. [Google Scholar] [CrossRef]
- Cengiz, Z.; Turan, M.; Olmaz, D.; Erce, Ç. Care Burden and Quality of Life in Family Caregivers of Palliative Care Patients. J. Soc. Work End-of-Life Palliat. Care 2021, 17, 50–63. [Google Scholar] [CrossRef]
- Ochoa, C.Y.; Buchanan Lunsford, N.; Lee Smith, J. Impact of informal cancer caregiving across the cancer experience: A systematic literature review of quality of life. Palliat. Support. Care 2019, 18, 220–240. [Google Scholar] [CrossRef]
- Leiknes, I.; Lien, U.-T.; Severinsson, E. The Relationship among Caregiver Burden, Demographic Variables, and the Clinical Characteristics of Patients with Parkinson’s Disease—A Systematic Review of Studies Using Various Caregiver Burden Instruments. Open J. Nurs. 2015, 05, 855–877. [Google Scholar] [CrossRef]
- Choi, S.; Seo, J.Y. Analysis of caregiver burden in palliative care: An integrated review. Nurs. Forum 2019, 54, 280–290. [Google Scholar] [CrossRef] [PubMed]
- Adelman, R.D.; Tmanova, L.L.; Delgado, D.; Dion, S.; Lachs, M.S. Caregiver Burden: A Clinical Review. JAMA 2014, 311, 1052. [Google Scholar] [CrossRef] [PubMed]
- Song, J.I.; Shin, D.W.; Choi, J.Y.; Kang, J.; Baik, Y.J.; Mo, H.; Park, M.H.; Choi, S.E.; Kwak, J.H.; Kim, E.J. Quality of life and mental health in family caregivers of patients with terminal cancer. Support. Care Cancer 2011, 19, 1519–1526. [Google Scholar] [CrossRef] [PubMed]
- Gallego-Alberto, L.; Losada, A.; Cabrera, I.; Romero-Moreno, R.; Pérez-Miguel, A.; Pedroso-Chaparro, M.D.S.; Márquez-González, M. “I Feel Guilty”. Exploring Guilt-Related Dynamics in Family Caregivers of People with Dementia. Clin. Gerontol. 2022, 45, 1294–1303. [Google Scholar] [CrossRef]
- King, J.J.; Badger, T.A.; Segrin, C.; Thomson, C.A. Loneliness, Spirituality, and Health-Related Quality of Life in Hispanic English-Speaking Cancer Caregivers: A Qualitative Approach. J. Relig. Health 2023, 63, 1433–1456. [Google Scholar] [CrossRef]

{kind=link}
|
|
|
|
| Themes | Sub-themes |
|---|---|
| Antecedents to caregiving burden |
|
| Attributes of caregiving burden |
|
| Consequences of caregiving burden |
|
| Religion and beliefs (new theme). |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Enazy, E.H.; Alyousef, S.M. Developing Burdens in Caring for a Relative with a Cancer Diagnosis: A Qualitative Study of Lived Experiences of Family Caregivers in Saudi Arabia. Nurs. Rep. 2025, 15, 233. https://doi.org/10.3390/nursrep15070233
Al Enazy EH, Alyousef SM. Developing Burdens in Caring for a Relative with a Cancer Diagnosis: A Qualitative Study of Lived Experiences of Family Caregivers in Saudi Arabia. Nursing Reports. 2025; 15(7):233. https://doi.org/10.3390/nursrep15070233
Chicago/Turabian StyleAl Enazy, Eman Halil, and Seham Mansour Alyousef. 2025. "Developing Burdens in Caring for a Relative with a Cancer Diagnosis: A Qualitative Study of Lived Experiences of Family Caregivers in Saudi Arabia" Nursing Reports 15, no. 7: 233. https://doi.org/10.3390/nursrep15070233
APA StyleAl Enazy, E. H., & Alyousef, S. M. (2025). Developing Burdens in Caring for a Relative with a Cancer Diagnosis: A Qualitative Study of Lived Experiences of Family Caregivers in Saudi Arabia. Nursing Reports, 15(7), 233. https://doi.org/10.3390/nursrep15070233