

Critical Thinking and Clinical Decision Making Among Registered Nurses in Clinical Practice: A Systematic Review and Meta-Analysis

 ,
,  ,
,  ,
, 
Abstract
1. Introduction
2. Methods
2.1. Protocol and Registration
2.2. Search Strategy
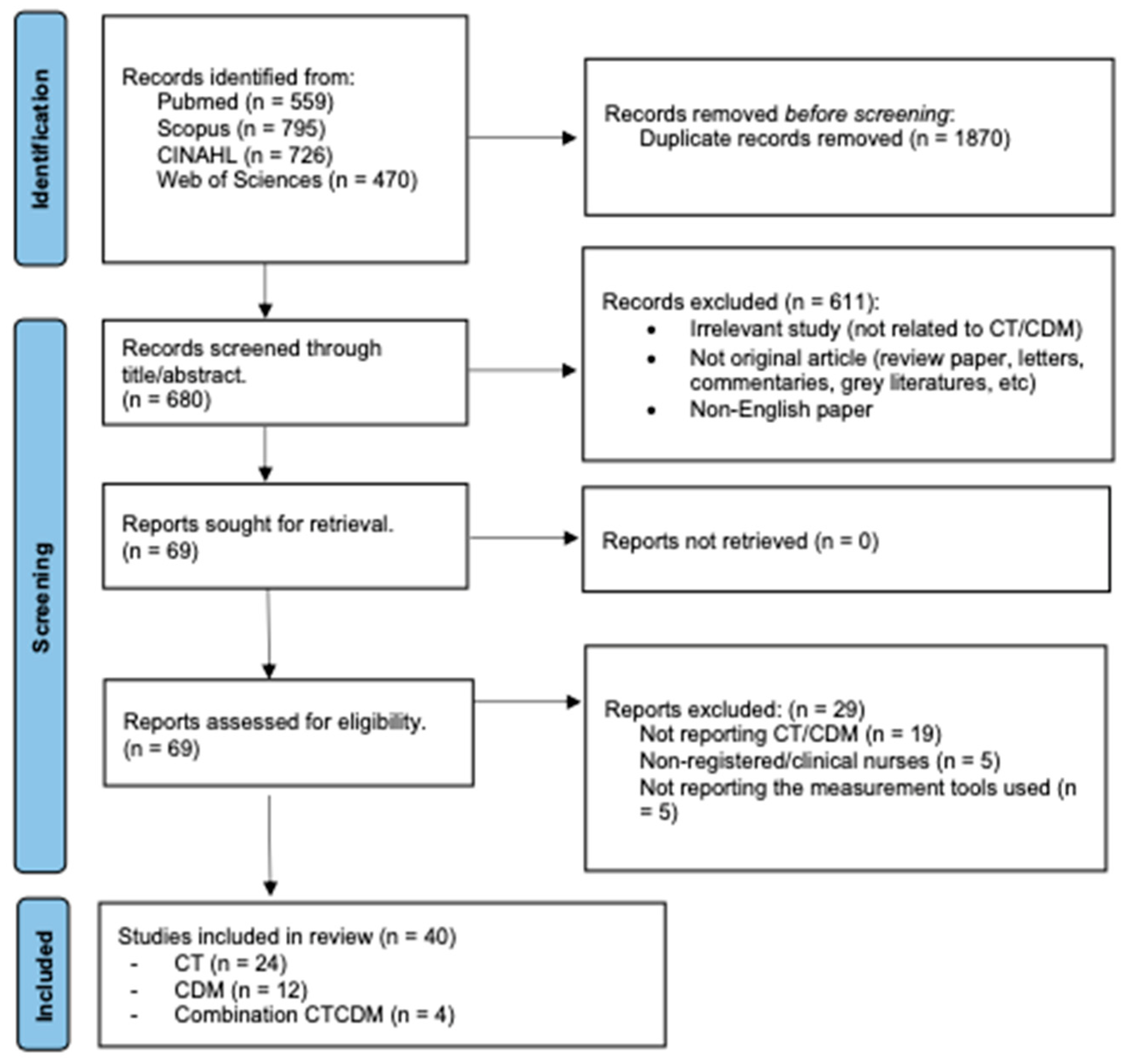
2.3. Study Selection
2.4. Data Extraction and Management
2.5. Quality Assessment
2.6. Statistical Analysis
3. Results
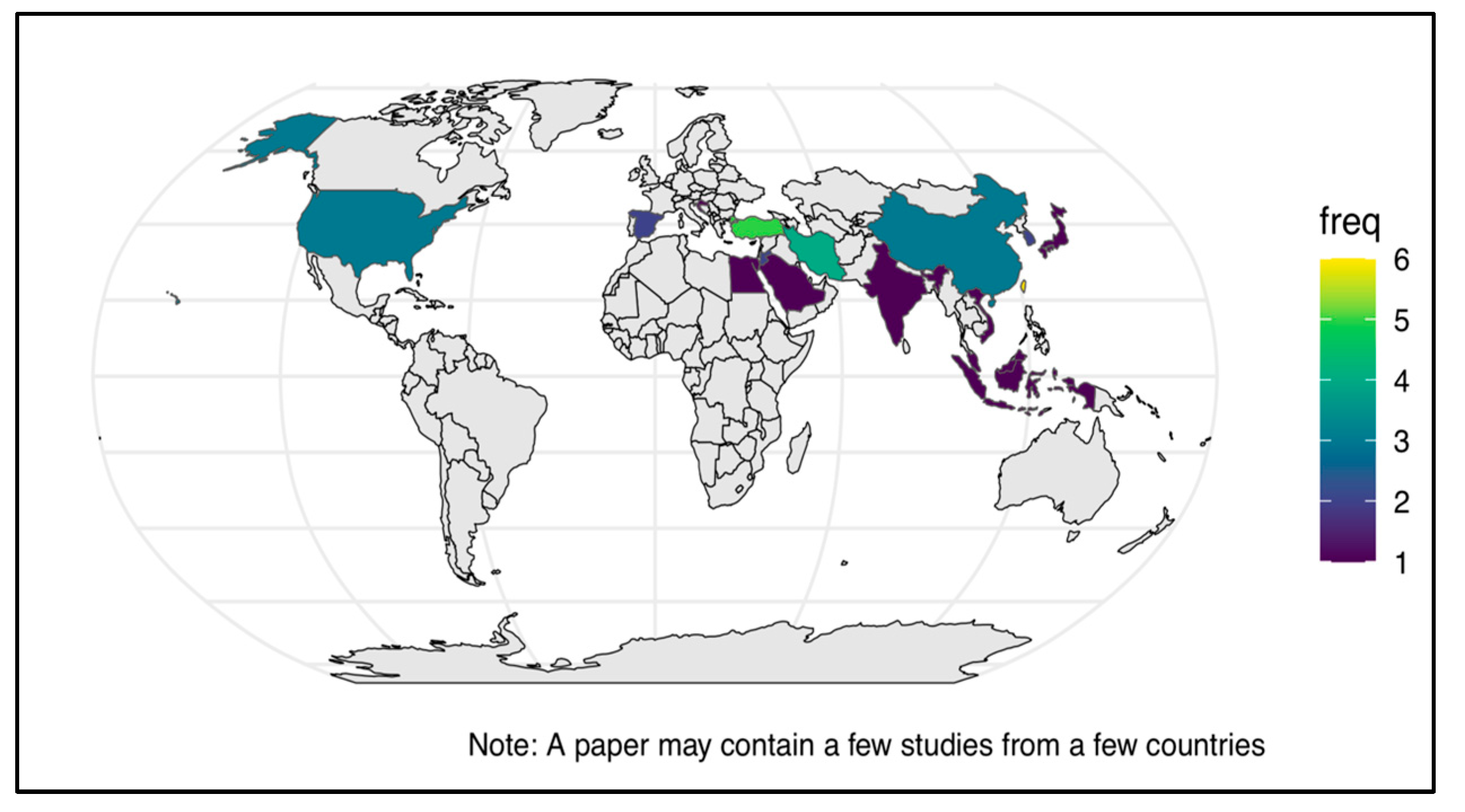
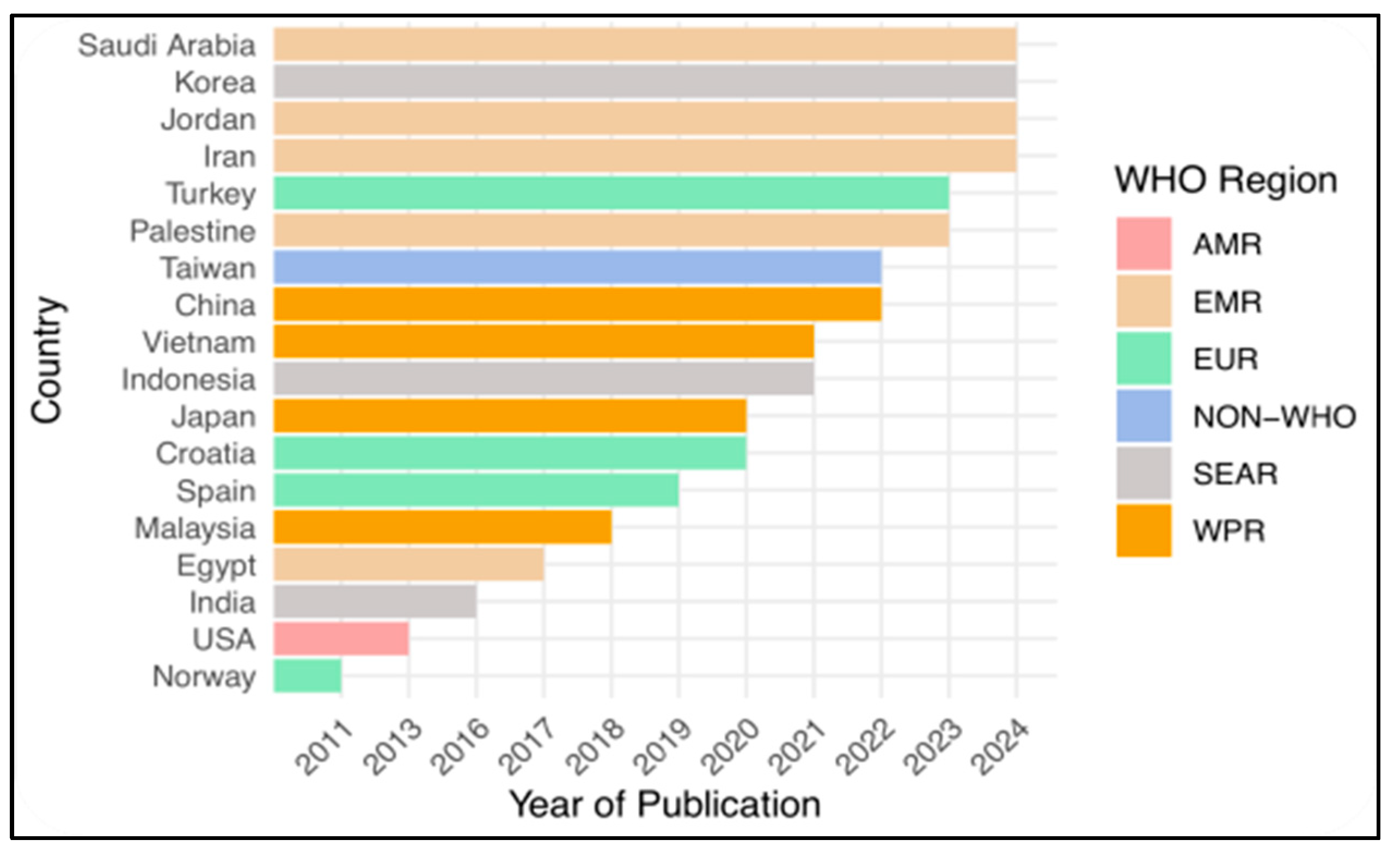
3.1. Characteristic of Included Studies
3.2. The Type of Observed Skills in the Selected Studies
3.3. The Results of the Observed Skills and Predictive Factors
3.4. The Measurement Tools Used in Selected Studies
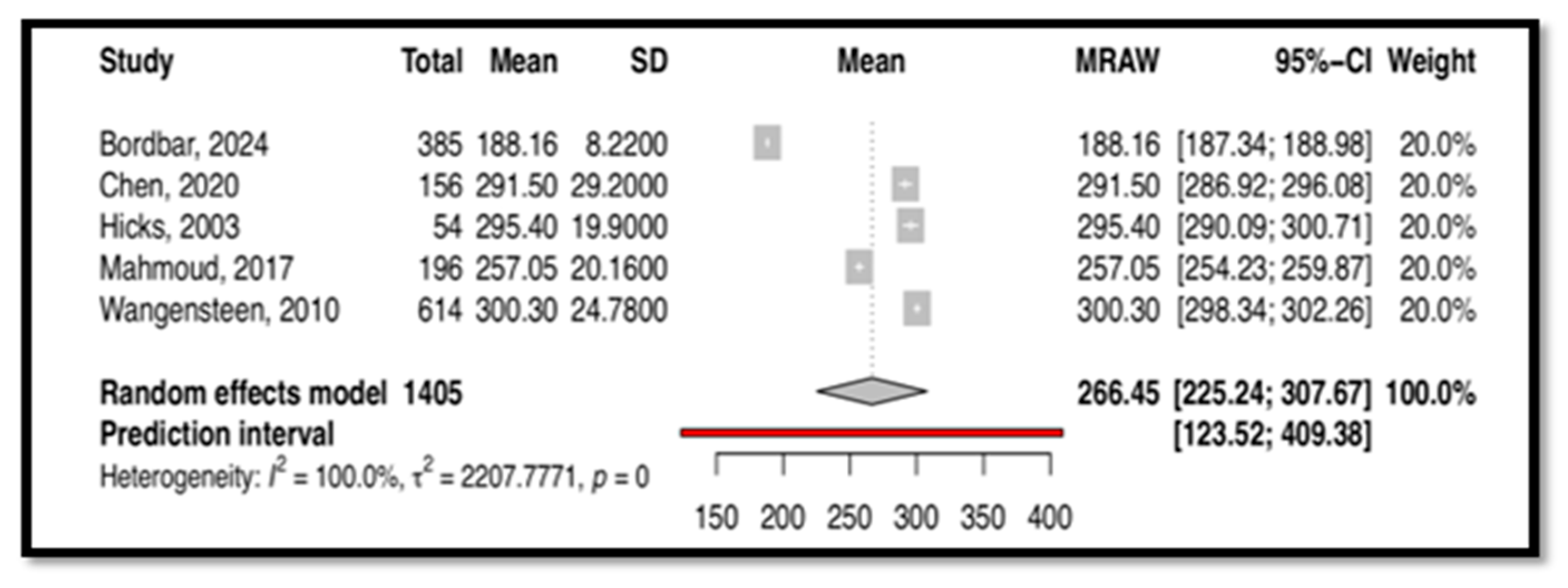
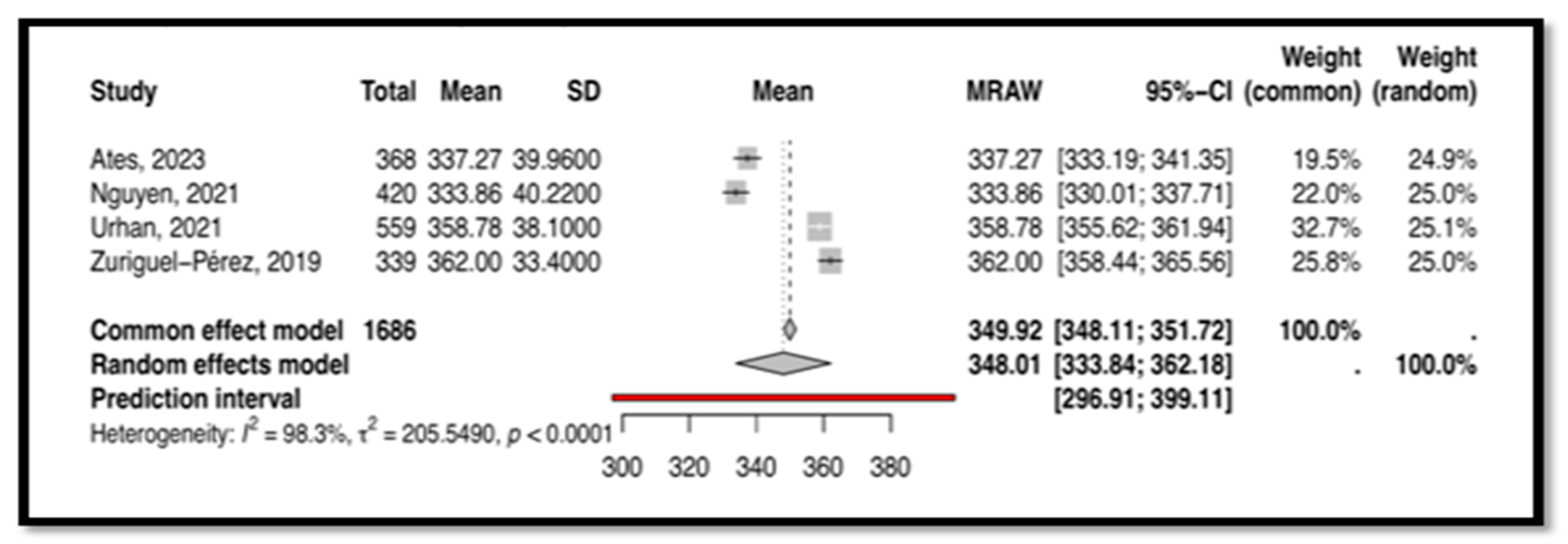
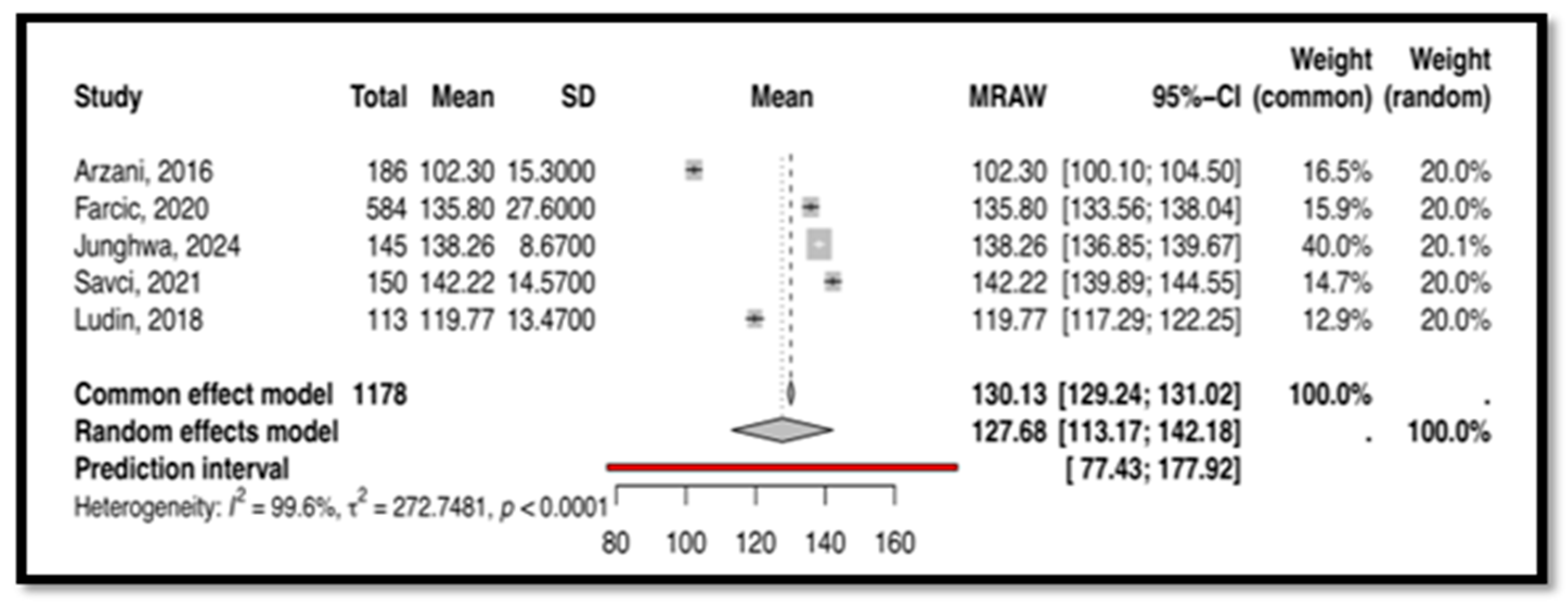
3.5. The Results of a Meta-Analysis
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Use of Artificial Intelligence
Conflicts of Interest
References
- Lee, D.S.; Abdullah, K.L.; Subramanian, P.; Bachmann, R.T.; Ong, S.L. An integrated review of the correlation between critical thinking ability and clinical decision-making in nursing. J. Clin. Nurs. 2017, 26, 4065–4079. [Google Scholar] [CrossRef]
- Zainal, N.H.; Musa, K.I.; Rasudin, N.S.; Mamat, Z. Multilevel modeling of individual and group level influences on critical thinking and clinical decision-making skills among registered nurses: A study protocol. Healthcare 2023, 11, 1169. [Google Scholar] [CrossRef]
- Standing, M. Clinical Judgement and Decision Making in Nursing; Cunneen, M., Ed.; SAGE: Shozendoakes, CA, USA, 2023; pp. 10–15. Available online: https://www.torrossa.com/en/resources/an/5543022 (accessed on 3 December 2023).
- Agbedia, C.; Ogbe, J. Critical thinking; issues in nursing education and practice. Int. J. Adv. Nurs. Stud. 2014, 3, 13. [Google Scholar] [CrossRef]
- Falcó-Pegueroles, A.; Rodríguez-Martín, D.; Ramos-Pozón, S.; Zuriguel-Pérez, E. Critical thinking in nursing clinical practice, education and research: From attitudes to virtue. Nurs. Philos. 2021, 22, e12332. [Google Scholar] [CrossRef]
- Polat, Ş.; Kutlu, L.; Ay, F.; Purİsa, S.; Erkan, H.A. Decision-making styles, anxiety levels, and critical thinking levels of nurses. Jpn. J. Nurs. Sci. 2019, 16, 309–321. [Google Scholar] [CrossRef]
- Ludin, S.M. Does good critical thinking equal effective decision-making among critical care nurses? A cross-sectional survey. Intensive Crit. Care Nurs. 2018, 44, 1–10. [Google Scholar] [CrossRef]
- Güven, Ş.D. Critical thinking in nursing. In Brain, Decision Making and Mental Health; Springer International Publishing: Cham, Switzerland, 2023; pp. 179–189. [Google Scholar] [CrossRef]
- Papathanasiou, I.V.; Kleisiaris, C.F.; Fradelos, E.C.; Kakou, K.; Kourkouta, L. Critical thinking: The development of an essential skill for nursing students. Acta Inform. Medica 2014, 22, 283. [Google Scholar] [CrossRef]
- Abu Arra, A.Y.; Ayed, A.; Toqan, D.; Albashtawy, M.; Salameh, B.; Sarhan, A.L.; Batran, A. The factors influencing nurses’ clinical decision-making in emergency department. Inq. J. Health Care Organ. Provis. Financ. 2023, 60, 00469580231152080. [Google Scholar] [CrossRef]
- Oh, S.; Gu, M.; Sok, S. A concept analysis of nurses’ clinical decision making: Implications for Korea. Int. J. Environ. Res. Public Health 2022, 19, 3596. [Google Scholar] [CrossRef]
- Xiao, Y.; Watson, M. Guidance on conducting a systematic literature review. J. Plan. Educ. Res. 2019, 39, 93–112. [Google Scholar] [CrossRef]
- Chan, Z.C. A systematic review of critical thinking in nursing education. Nurse Educ. Today 2013, 33, 236–240. [Google Scholar] [CrossRef]
- Zuriguel Perez, E.; Lluch Canut, M.T.; Falco Pegueroles, A.; Puig Llobet, M.; Moreno Arroyo, C.; Roldan Merino, J. Critical thinking in nursing: Scoping review of the literature. Int. J. Nurs. Pract. 2015, 21, 820–830. [Google Scholar] [CrossRef]
- Nibbelink, C.W.; Brewer, B.B. Decision-making in nursing practice: An integrative literature review. J. Clin. Nurs. 2018, 27, 917–928. [Google Scholar] [CrossRef]
- Sholehah, B.; Astari, A.M.; Kapti, R.E. Factors influencing in clinical decision making of nurse: A systematic review. Int. J. Sci. Soc. 2020, 2, 135–145. [Google Scholar] [CrossRef]
- Yue, M.; Zhang, M.; Zhang, C.; Jin, C. The effectiveness of concept mapping on development of critical thinking in nursing education: A systematic review and meta-analysis. Nurse Educ. Today 2017, 52, 87–94. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 5 January 2024).
- Herzog, R.; Álvarez-Pasquin, M.J.; Díaz, C.; Del Barrio, J.L.; Estrada, J.M.; Gil, Á. Are healthcare workers’ intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health 2013, 13, 154. [Google Scholar] [CrossRef]
- Schwarzer, G. meta: An R package for meta-analysis. R News 2007, 7, 40–45. [Google Scholar]
- Hasani, W.S.; Muhamad, N.A.; Hanis, T.M.; Maamor, N.H.; Chen, X.W.; Omar, M.A.; Cheng Kueh, Y.; Abd Karim, Z.; Hassan, M.R.; Musa, K.I. The global estimate of premature cardiovascular mortality: A systematic review and meta-analysis of age-standardized mortality rate. BMC Public Health 2023, 23, 1561. [Google Scholar] [CrossRef]
- Cai, S.; Zhou, J.; Pan, J. Estimating the sample mean and standard deviation from order statistics and sample size in meta-analysis. Stat. Methods Med. Res. 2021, 30, 2701–2719. [Google Scholar] [CrossRef] [PubMed]
- Ali-Abadi, T.; Babamohamadi, H.; Nobahar, M. Critical thinking skills in intensive care and medical-surgical nurses and their explaining factors. Nurse Educ. Pract. 2020, 45, 102783. [Google Scholar] [CrossRef]
- Ateş, N.; Erdal, N.; Harmancı Seren, A.K. The relationship between critical thinking and job performance among nurses: A descriptive survey study. Int. J. Nurs. Pract. 2023, 29, e13173. [Google Scholar] [CrossRef] [PubMed]
- Bordbar, S.; Bahmaei, J.; Rad, H.F.; Yusefi, A.R. Investigate the state of critical thinking and its impact on moral courage and moral sensitivity: Evidence from nurses’ perspective. BMC Nurs. 2024, 23, 825. [Google Scholar] [CrossRef]
- Chang, M.J.; Chang, Y.J.; Kuo, S.H.; Yang, Y.H.; Chou, F.H. Relationships between critical thinking ability and nursing competence in clinical nurses. J. Clin. Nurs. 2011, 20, 3224–3232. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.F.; Chen, S.Y.; Pai, H.C. Self-reflection and critical thinking: The influence of professional qualifications on registered nurses. Contemp. Nurse 2019, 55, 59–70. [Google Scholar] [CrossRef]
- Chen, Q.; Liu, D.; Zhou, C.; Tang, S. Relationship between critical thinking disposition and research competence among clinical nurses: A cross-sectional study. J. Clin. Nurs. 2020, 29, 1332–1340. [Google Scholar] [CrossRef]
- Feng, R.C.; Chen, M.J.; Chen, M.C.; Pai, Y.C. Critical thinking competence and disposition of clinical nurses in a medical center. J. Nurs. Res. 2010, 18, 77–87. [Google Scholar] [CrossRef]
- Futami, A.; Noguchi-Watanabe, M.; Mikoshiba, N.; Yamamoto-Mitani, N. Critical thinking disposition among hospital nurses in Japan: Impact of organizational versus personal factors. Jpn. J. Nurs. Sci. 2020, 17, e12298. [Google Scholar] [CrossRef] [PubMed]
- Hicks, F.D.; Merritt, S.L.; Elstein, A.S. Critical thinking and clinical decision making in critical care nursing: A pilot study. Heart Lung 2003, 32, 169–180. [Google Scholar] [CrossRef]
- Hsu, H.Y.; Chang, S.C.; Chang, A.L.; Chen, S.L. Critical thinking disposition of nurse practitioners in Taiwan. J. Contin. Educ. Nurs. 2017, 48, 425–430. [Google Scholar] [CrossRef]
- Kaya, H.; Yalniz, N. Critical thinking dispositions of emergency nurses in Turkey: A cross-sectional study. Hong Kong J. Emerg. Med. 2012, 19, 198–203. [Google Scholar] [CrossRef]
- Lang, G.M.; Beach, N.L.; Patrician, P.A.; Martin, C. A cross-sectional study examining factors related to critical thinking in nursing. J. Nurses Prof. Dev. 2013, 29, 8–15. [Google Scholar] [CrossRef]
- Lee, S.Y.; Chang, C.Y. Nursing management of the critical thinking and care quality of ICU nurses: A cross-sectional study. J. Nurs. Manag. 2022, 30, 2889–2896. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, A.S.; Mohamed, H.A. Critical thinking disposition among nurses working in puplic hospitals at port-said governorate. Int. J. Nurs. Sci. 2017, 4, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Van Nguyen, T.; Liu, H.E. Factors associated with the critical thinking ability of professional nurses: A cross-sectional study. Nursing Open. 2021, 8, 1970–1980. [Google Scholar] [CrossRef]
- Park, S.K.; Jeong, Y.W. Relationship between hospital ethical climate, critical thinking disposition, and nursing task performance. BMC Nurs. 2024, 23, 696. [Google Scholar] [CrossRef]
- Schubert, C.R. Effect of simulation on nursing knowledge and critical thinking in failure to rescue events. J. Contin. Educ. Nurs. 2012, 43, 467–471. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Yin, Y.; Wang, J.; Ding, Z.; Wang, D.; Zhang, Y.; Zhang, J.; Wang, Y. Critical thinking abilities among newly graduated nurses: A cross-sectional survey study in China. Nurs. Open 2023, 10, 1383–1392. [Google Scholar] [CrossRef]
- Urhan, E.; Zuriguel-Perez, E.; Harmancı Seren, A.K. Critical thinking among clinical nurses and related factors: A survey study in public hospitals. J. Clin. Nurs. 2022, 31, 3155–3164. [Google Scholar] [CrossRef]
- Wangensteen, S.; Johansson, I.S.; Bjørkstrøm, M.E.; Nordström, G. Critical thinking dispositions among newly graduated nurses. J. Adv. Nurs. 2010, 66, 2170–2181. [Google Scholar] [CrossRef]
- Wangensteen, S.; Johansson, I.S.; Björkström, M.E.; Nordström, G. Research utilisation and critical thinking among newly graduated nurses: Predictors for research use. A quantitative cross-sectional study. J. Clin. Nurs. 2011, 20, 2436–2447. [Google Scholar] [CrossRef] [PubMed]
- Zuriguel-Pérez, E.; Falcó-Pegueroles, A.; Agustino-Rodríguez, S.; del Carmen Gómez-Martín, M.; Roldán-Merino, J.; Lluch-Canut, M.T. Clinical nurses’s critical thinking level according to sociodemographic and professional variables (phase II): A correlational study. Nurse Educ. Pract. 2019, 41, 102649. [Google Scholar] [CrossRef] [PubMed]
- Zuriguel-Pérez, E.; Lluch-Canut, M.T.; Agustino-Rodríguez, S.; Gómez-Martín, M.D.; Roldán-Merino, J.; Falcó-Pegueroles, A. Critical thinking: A comparative analysis between nurse managers and registered nurses. J. Nurs. Manag. 2018, 26, 1083–1090. [Google Scholar] [CrossRef] [PubMed]
- Al-Shomrani, A.Z.; Hamouda, G.M.; Abdullah, N. The Relationship Between Psychological Empowerment and Clinical Decision-Making Among Staff Nurses in Governmental Hospital in Al-Baha, Saudi Arabia. Cureus 2024, 16, e56871. [Google Scholar] [CrossRef]
- Arash, A.; Mahmoodi-Shan, G.; Mehravar, F.; Sabzi, Z.; Mancheri, H. Clinical decision making and moral distress among intensive care units nurses in Iran. BMC Psychol. 2024, 12, 692. [Google Scholar] [CrossRef]
- Arzani, A.; Lotfi, M.; Abedi, A.R. Experiences and clinical decision-making of operating room nurses based on benner’s theory. J. Babol Univ. Med. Sci. 2016, 18, 35–40. [Google Scholar] [CrossRef]
- Batran, A.; Al-Humran, S.M.; Malak, M.Z.; Ayed, A. The relationship between nursing informatics competency and clinical decision-making among nurses in West Bank, Palestine. CIN Comput. Inform. Nurs. 2022, 40, 547–553. [Google Scholar] [CrossRef]
- Bjørk, I.T.; Hamilton, G.A. Clinical decision making of nurses working in hospital settings. Nurs. Res. Pract. 2011, 2011, 524918. [Google Scholar] [CrossRef]
- Farčić, N.; Barać, I.; Plužarić, J.; Ilakovac, V.; Pačarić, S.; Gvozdanović, Z.; Lovrić, R. Personality traits of core self-evaluation as predictors on clinical decision-making in nursing profession. PLoS ONE 2020, 15, e0233435. [Google Scholar] [CrossRef]
- Yun, J.; Seong, M.; Cho, Y.; Sok, S. Influences of Nursing Professionalism, Empathy, and Clinical Decision-Making Ability on Shared Decision-Making Awareness among Hemodialysis Nurses. J. Nurs. Manag. 2024, 2024, 2518065. [Google Scholar] [CrossRef]
- Nageshwar, V.; Noronha, J.A.; Nileshwar, A.; George, A.; Nayak, B.S.; Jose, T.T.; Valsaraj, B.P. Nurses perception of factors influencing clinical decision making. Indian J. Public Health Res. Dev. 2016, 7, 54–58. [Google Scholar] [CrossRef]
- Rababah, J.A.; Al-Hammouri, M.M. Predictors of Jordanian Registered Nurses’ Clinical Decision-Making: The Role of Self-Directed Learning and Personal Characteristics. Nurs. Forum 2024, 2024, 5558520. [Google Scholar] [CrossRef]
- Savci, C.; Akinci, A.C.; Keles, F. Anxiety levels and clinical decision-making skills of nurses providing care for patients diagnosed with COVID-19. Electron. J. Gen. Med. 2021, 18, em322. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Yang, J.; Liu, L.; Ye, B. An investigation of factors influencing nurses’ clinical decision-making skills. West. J. Nurs. Res. 2016, 38, 974–991. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.L.; Hsu, H.Y.; Chang, C.F.; Lin, E.C. An exploration of the correlates of nurse practitioners’ clinical decision-making abilities. J. Clin. Nurs. 2016, 25, 1016–1024. [Google Scholar] [CrossRef]
- Dewi, N.A.; Yetti, K.; Nuraini, T. Nurses’ critical thinking and clinical decision-making abilities are correlated with the quality of nursing handover. Enferm. Clin. 2021, 31, S271–S275. [Google Scholar] [CrossRef]
- Rababa, M.; Al-Rawashdeh, S. Critical care nurses’ critical thinking and decision making related to pain management. Intensive Crit. Care Nurs. 2021, 63, 103000. [Google Scholar] [CrossRef]
- Yin, J.D. WHO, COVID-19, and Taiwan as the Ghost Island. Glob. Public Health 2021, 16, 1267–1282. [Google Scholar] [CrossRef]
- Chen, Y.F. Taiwan and the World Health Assembly/World Health Organization: Perspectives from health services and research. Int. J. Taiwan Stud. 2020, 3, 10–27. [Google Scholar] [CrossRef]
- Taherdoost, H. Determining sample size; how to calculate survey sample size. Int. J. Econ. Manag. Syst. 2017, 2. Available online: https://ssrn.com/abstract=3224205 (accessed on 7 December 2024).
- Faber, J.; Fonseca, L.M. How sample size influences research outcomes. Dent. Press J. Orthod. 2014, 19, 27–29. [Google Scholar] [CrossRef] [PubMed]
- Thompson, C.; Stapley, S. Do educational interventions improve nurses’ clinical decision making and judgement? A systematic review. Int. J. Nurs. Stud. 2011, 48, 881–893. [Google Scholar] [CrossRef]
- Clemett, V.J.; Raleigh, M. The validity and reliability of clinical judgement and decision-making skills assessment in nursing: A systematic literature review. Nurse Educ. Today 2021, 102, 104885. [Google Scholar] [CrossRef]
- Carter, A.G.; Creedy, D.K.; Sidebotham, M. Evaluation of tools used to measure critical thinking development in nursing and midwifery undergraduate students: A systematic review. Nurse Educ. Today 2015, 35, 864–874. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.E.; Dahinten, V.S. The enabling, enacting, and elaborating factors of safety culture associated with patient safety: A multilevel analysis. J. Nurs. Scholarsh. 2020, 52, 544–552. [Google Scholar] [CrossRef]
- Hox, J.J.; Moerbeek, M.; Van de Schoot, R. Multilevel Analysis: Techniques and Applications; Routledge: London, UK, 2017. [Google Scholar]
- Maas, C.J.; Hox, J.J. Sufficient sample sizes for multilevel modeling. Methodology 2005, 1, 86–92. [Google Scholar] [CrossRef]
- Zuriguel-Pérez, E.; Falcó-Pegueroles, A.; Roldán-Merino, J.; Agustino-Rodriguez, S.; Gómez-Martín, M.D.; Lluch-Canut, M.T. Development and psychometric properties of the nursing critical thinking in clinical practice questionnaire. Worldviews Evid.-Based Nurs. 2017, 14, 257–264. [Google Scholar] [CrossRef]
- Lauri, S.; Salanterä, S. Developing an instrument to measure and describe clinical decision making in different nursing fields. J. Prof. Nurs. 2002, 18, 93–100. [Google Scholar] [CrossRef]
- Souza, A.C.; Alexandre, N.M.; Guirardello, E.D. Psychometric properties in instruments evaluation of reliability and validity. Epidemiol. E Serv. De Saude 2017, 26, 649–659. [Google Scholar] [CrossRef] [PubMed]
- Swan, K.; Speyer, R.; Scharitzer, M.; Farneti, D.; Brown, T.; Woisard, V.; Cordier, R. Measuring what matters in healthcare: A practical guide to psychometric principles and instrument development. Front. Psychol. 2023, 14, 1225850. [Google Scholar] [CrossRef]
- Sahoo, M. Structural equation modeling: Threshold criteria for assessing model fit. In Methodological Issues in Management Research: Advances, Challenges, and the Way Ahead; Emerald Publishing Limited: Bradford, UK, 2019; pp. 269–276. [Google Scholar] [CrossRef]
- Awang, Z. SEM Made Simple: A Gentle Approach to Learning Structural Equation Modeling; MPWS Rich Publication: Bandar Baru Bangi, Malaysia, 2015; Available online: http://eprints.unisza.edu.my/id/eprint/3180 (accessed on 9 December 2024).
- Haidich, A.B. Meta-analysis in medical research. Hippokratia 2010, 14 (Suppl. S1), 29. [Google Scholar] [PubMed]
- Metelli, S.; Chaimani, A. Challenges in meta-analyses with observational studies. BMJ Ment Health 2020, 23, 83–87. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Schroll, J.B.; Moustgaard, R.; Gøtzsche, P.C. Dealing with substantial heterogeneity in Cochrane reviews. Cross-sectional study. BMC Med. Res. Methodol. 2011, 11, 22. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study ID | Measurement Tools Used | Findings | Quality Assessment (NOS) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Score Indicators | Predictive Factors Influenced the Study | S | C | O | Total Score | |||||
| Instrument | Reliability Test | Psychometric Test | Individual | Group | ||||||
| Ali-Abadi, 2020 [24] | CCTST-FB | Available | N/A | CT level | Available | N/A | *** | ** | ** | 7 (Good studies) |
| Ates, 2023 [25] | CTSiCPfN | Available | N/A | CT skill | Available | N/A | **** | * | ** | 7 (Good studies) |
| Bordbar, 2024 [26] | CCTDI | Available | N/A | CT disposition | Available | N/A | **** | ** | *** | 9 (Very good studies) |
| Chang, 2011 [27] | WGCTA-CV | Available | N/A | CT ability | Available | N/A | *** | ** | ** | 7 (Good studies) |
| Chen, 2019 [28] | TCTDI | Available | N/A | CT disposition | Available | N/A | **** | * | ** | 7 (Good studies) |
| Chen, 2020 [29] | CTDI-CV | N/A | N/A | CT disposition | N/A | N/A | **** | * | ** | 7 (Good studies) |
| Feng, 2010 [30] | Tw-WGCT; TCTDI | Available | N/A | CT competence, CT disposition | Available | N/A | **** | ** | ** | 8 (Good studies) |
| Futami, 2020 [31] | JCTDS | Available | N/A | CT disposition | Available | Available | *** | ** | ** | 7 (Good studies) |
| Hicks, 2003 [32] | CCTDI, CCTST, DAQ | N/A | N/A | CT disposition, CT skill, CDM consistency | N/A | N/A | ** | * | ** | 5 (Satisfactory studies) |
| Hsu, 2017 [33] | CTD | Available | N/A | CT disposition | Available | N/A | *** | ** | ** | 7 (Good studies) |
| Kaya, 2012 [34] | CCTDI | Available | N/A | CT disposition | Available | N/A | *** | ** | ** | 7 (Good studies) |
| Lang, 2013 [35] | HSRT | N/A | N/A | CT skills | Available | N/A | **** | ** | ** | 8 (Good studies) |
| Lee, 2022 [36] | CTQ | Available | N/A | CT ability | Available | N/A | *** | ** | ** | 7 (Good studies) |
| Mahmoud, 2017 [37] | CCTDI | Available | N/A | CT disposition | N/A | N/A | **** | * | ** | 7 (Good studies) |
| Nguyen, 2021 [38] | N-CT-4 P | Available | Available | CT ability | Available | N/A | ***** | ** | ** | 9 (Very good studies) |
| Park, 2024 [39] | CTDS | Available | N/A | CT disposition | N/A | N/A | **** | * | *** | 8 (Good studies) |
| Polat, 2019 [6] | Turkish CCTDI | Available | Available | CT disposition | Available | N/A | ***** | * | ** | 8 (Good studies) |
| Schubert, 2012 [40] | LTT | N/A | N/A | CT skill | N/A | N/A | ** | ** | 4 (Unsatis-factory studies | |
| Sun, 2022 [41] | CTDI-CV | Available | N/A | CT disposition | Available | N/A | *** | * | ** | 6 (Satisfactory studies) |
| Urhan, 2021 [42] | N-CT-4 P-Tv | Available | N/A | CT skill | Available | Available | *** | ** | ** | 7 (Good studies) |
| Wangen-steen, 2010 [43] | CCTDI | Available | N/A | CT disposition | Available | N/A | *** | ** | ** | 7 (Good studies) |
| Wangen-steen, 2011 [44] | CCTDI | Available | N/A | CT disposition | N/A | N/A | *** | ** | 5 (Satisfactory studies) | |
| Zuriguel-Pérez, 2019 [45] | N-CT-4 P | Available | Available | CT level | Available | N/A | **** | ** | ** | 8 (Good studies) |
| Zuriguel-Pérez, 2018 [46] | N-CT-4 P | Available | Available | CT level | Available | N/A | **** | ** | ** | 8 (Good studies) |
| Abu Arra, 2023 [10] | CDMNS | Available | N/A | CDM level | Available | N/A | **** | ** | ** | 8 (Good studies) |
| Alshomrani, 2024 [47] | NDMI | Available | N/A | Decision-making style | Available | N/A | **** | ** | ** | 8 (Good studies) |
| Arash, 2024 [48] | NDMI | Available | N/A | Decision-making style | Available | N/A | **** | ** | ** | 8 (Good studies) |
| Arzani, 2016 [49] | CDMNS | Available | N/A | CDM level | Available | N/A | *** | ** | ** | 7 (Good studies) |
| Batran, 2022 [50] | CDMNS | Available | N/A | CDM level | N/A | N/A | **** | * | ** | 7 (Good studies) |
| Bjørk, 2011 [51] | NDMI | Available | N/A | Decision-making style | Available | Available | ** | ** | ** | 6 (Satisfactory studies) |
| Farčić, 2020 [52] | CDMNS | Available | N/A | CDM level | Available | N/A | ** | ** | ** | 6 (Satisfactory studies) |
| Junghwa Yun, 2024 [53] | CDMNS | Available | N/A | CDM level | N/A | N/A | **** | * | *** | 8 (Good studies) |
| Nageshwar, 2016 [54] | 36-item Q | Available | N/A | N/A | Available | N/A | *** | * | ** | 6 (Satisfactory studies) |
| Rababah, 2024 [55] | NDMI | Available | N/A | Decision-making style | Available | N/A | **** | ** | *** | 9 (Very good studies) |
| Savci, 2021 [56] | CDMNS | Available | N/A | CDM level | Available | N/A | *** | ** | ** | 7 (Good studies) |
| Wu, 2016 [57] | PKIN | Available | N/A | Nurses’ ability levels | Available | N/A | *** | ** | ** | 7 (Good studies) |
| Chen, 2016 [58] | CCTDI, CDMI | Available | N/A | CT disposition, CDM abilities | Available | Available | *** | ** | ** | 7 (Good studies) |
| Dewi, 2021 [59] | CTQ, CDMQ | Available | N/A | CT ability, CDM ability | N/A | N/A | **** | * | ** | 7 (Good studies) |
| Ludin, 2018 [7] | SF-CTDI-CV, CDMNS | Available | N/A | CT disposition, CDM level | Available | N/A | **** | ** | ** | 8 (Good studies) |
| Rababa, 2021 [60] | CTSAS, NDMI | Available | N/A | CT skills, CDM modes | Available | N/A | **** | ** | ** | 8 (Good studies) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zainal, N.H.; Islam, M.A.; Rasudin, N.S.; Mamat, Z.; Hanis, T.M.; Rodzlan Hasani, W.S.; Musa, K.I. Critical Thinking and Clinical Decision Making Among Registered Nurses in Clinical Practice: A Systematic Review and Meta-Analysis. Nurs. Rep. 2025, 15, 175. https://doi.org/10.3390/nursrep15050175
Zainal NH, Islam MA, Rasudin NS, Mamat Z, Hanis TM, Rodzlan Hasani WS, Musa KI. Critical Thinking and Clinical Decision Making Among Registered Nurses in Clinical Practice: A Systematic Review and Meta-Analysis. Nursing Reports. 2025; 15(5):175. https://doi.org/10.3390/nursrep15050175
Chicago/Turabian StyleZainal, Nur Hidayah, Md Asiful Islam, Nur Syahmina Rasudin, Zakira Mamat, Tengku Muhammad Hanis, Wan Shakira Rodzlan Hasani, and Kamarul Imran Musa. 2025. "Critical Thinking and Clinical Decision Making Among Registered Nurses in Clinical Practice: A Systematic Review and Meta-Analysis" Nursing Reports 15, no. 5: 175. https://doi.org/10.3390/nursrep15050175
APA StyleZainal, N. H., Islam, M. A., Rasudin, N. S., Mamat, Z., Hanis, T. M., Rodzlan Hasani, W. S., & Musa, K. I. (2025). Critical Thinking and Clinical Decision Making Among Registered Nurses in Clinical Practice: A Systematic Review and Meta-Analysis. Nursing Reports, 15(5), 175. https://doi.org/10.3390/nursrep15050175