
Cognitive Stimulation and Its Effects on Well-Being, Executive Functions, and Brain-Derived Neurotrophic Factor in Older Adults from a Mexican Geriatric Center: A Quasi-Experimental Study

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Sample Size
2.3. Participants
- ○
- Adults (of any gender) over 60 years of age.
- ○
- Willingness to participate in all intervention and assessment sessions.
- ○
- Ability to communicate verbally.
- ○
- Ability to participate in simple games/activities.
- ○
- Impairments or behavioral problems that could prevent participation in activities.
- ○
- Have received psychological or psychiatric care in the last two months.
- ○
- Presenting any condition that requires immediate intervention (i.e., suicidal ideation) or that interferes with participation in the study (i.e., severe hearing loss).
- ○
- Inability to communicate that limits participation in the intervention, as determined by the researchers.
- ○
- Presence of any medical condition that endangered survival during the project.
- ○
- Change in residence.
- ○
- Participant or family member’s decision to withdraw from the study.
- ○
- Participating in less than 80% of the intervention sessions.
2.4. Blood Sample Collection and Measurement of BDNF Serum Levels
2.5. Cognitive Assessment
2.6. Measuring Well-Being Indicators
2.7. Cognitive Stimulation Intervention
2.8. Statistical Analysis
3. Results
3.1. Adherence to the Intervention
3.2. Cognitive Assessments
3.2.1. Intragroup Differences
3.2.2. Intergroup Differences
3.3. Well-Being Indicators
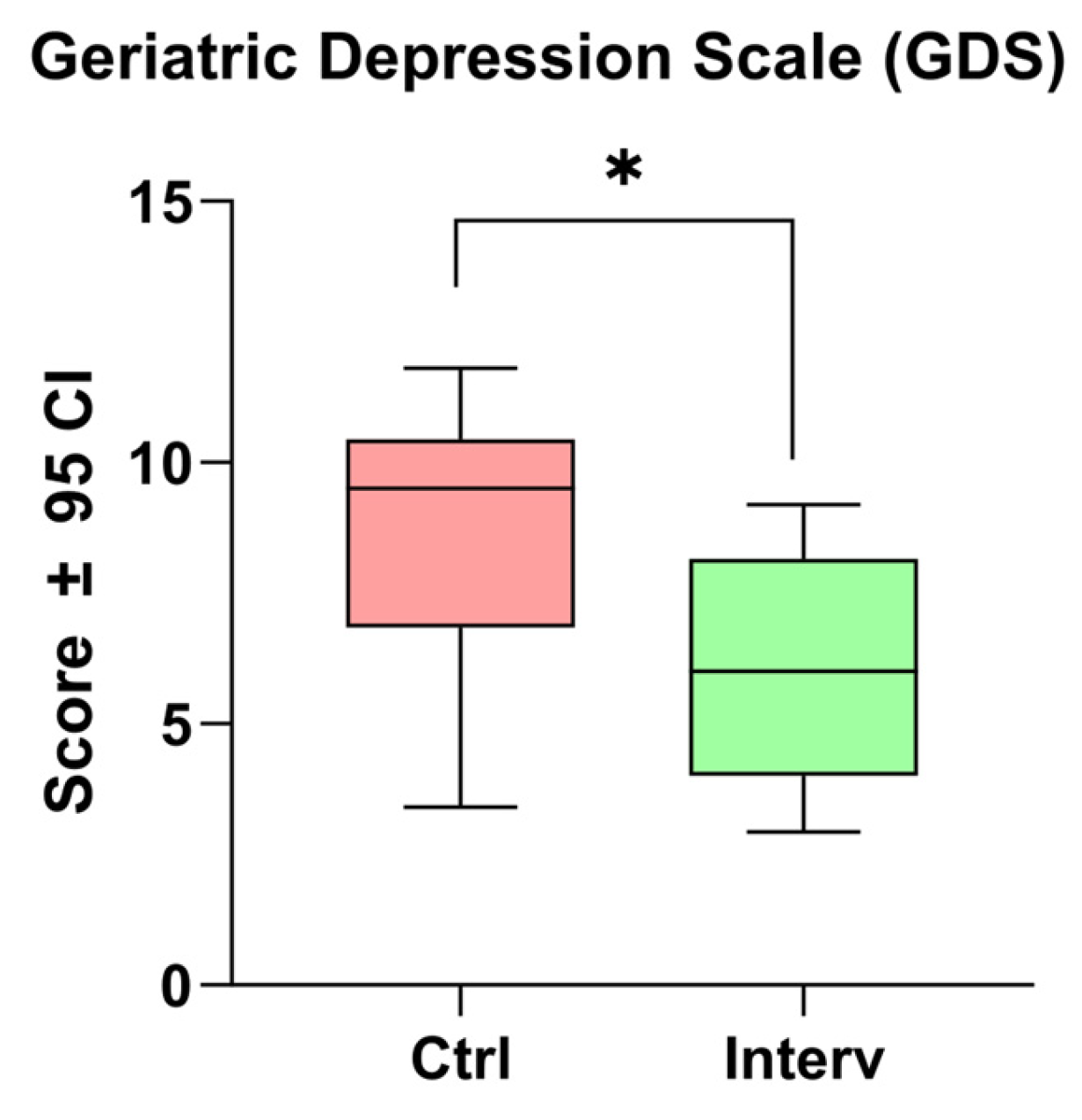
3.3.1. Depression
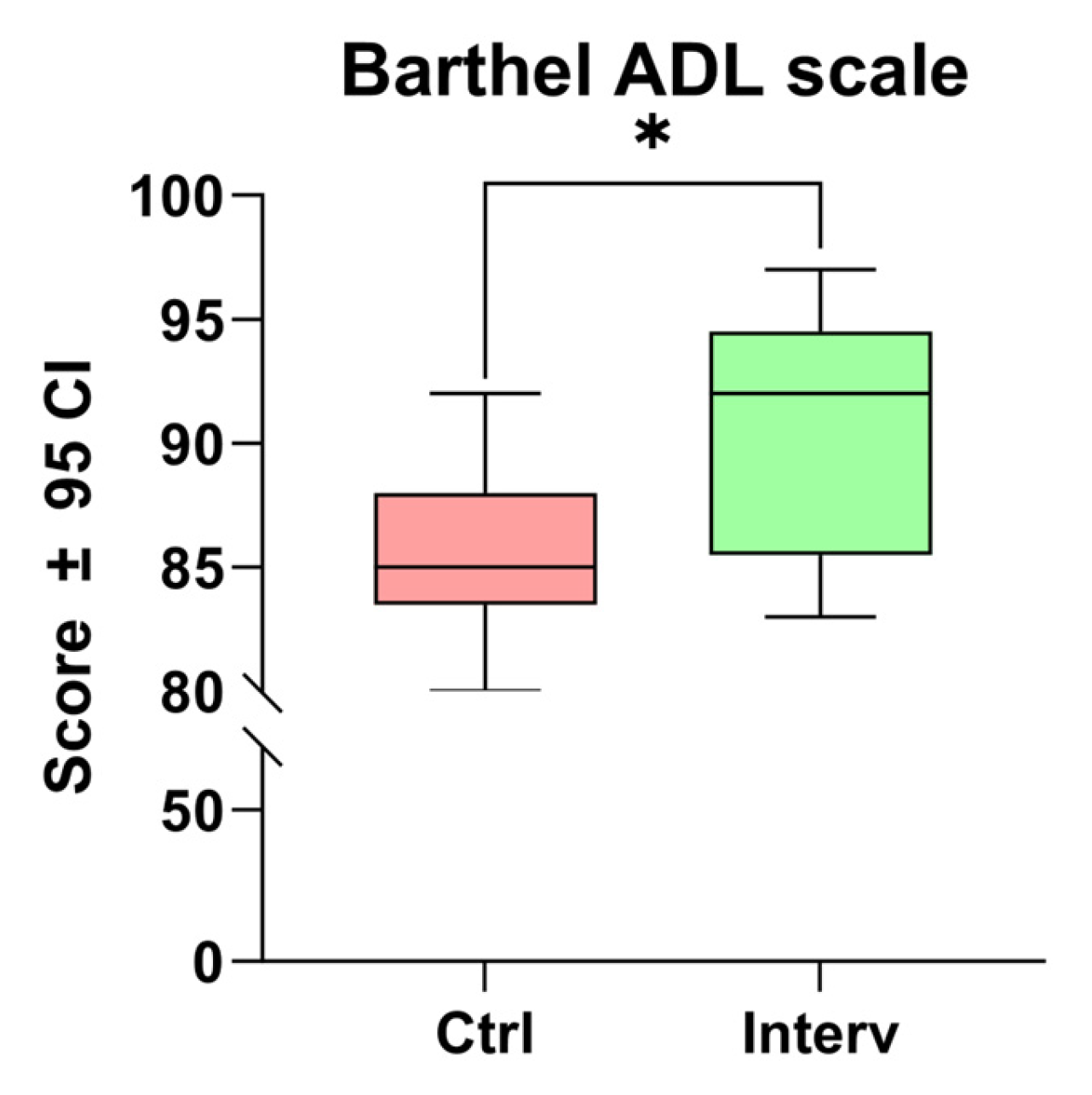
3.3.2. Autonomy in Activities of Daily Living (ADL)
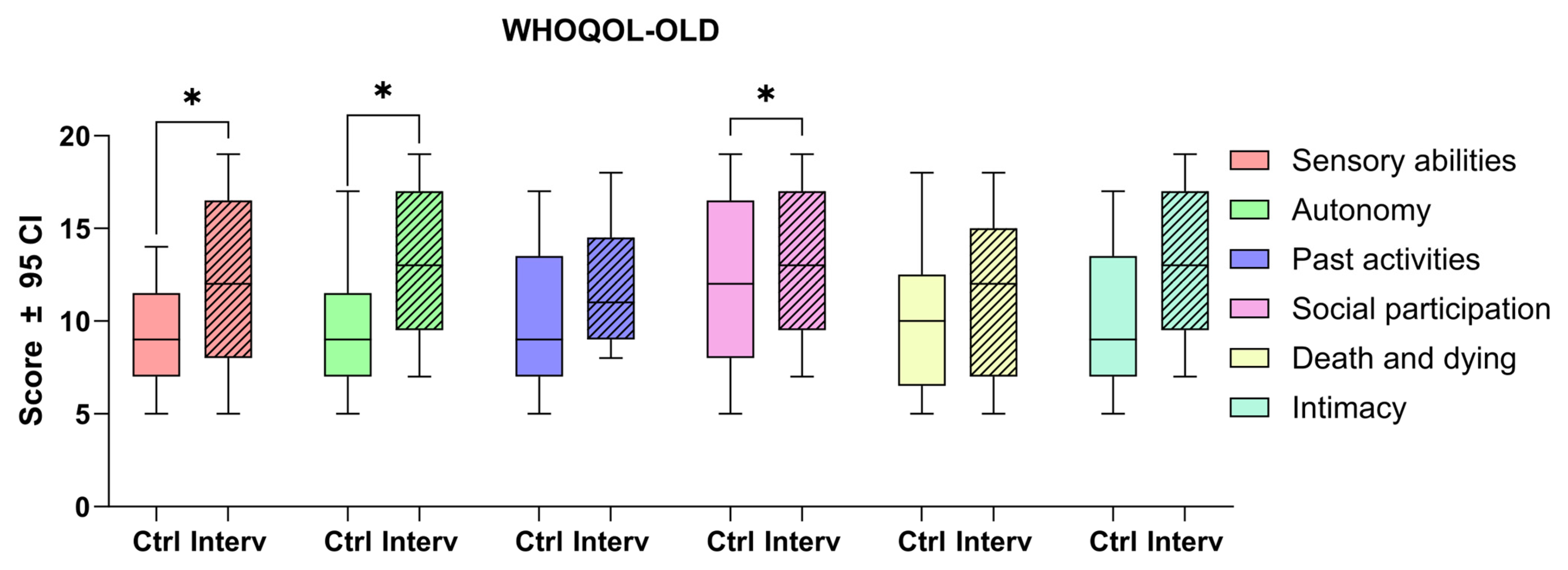
3.3.3. Quality of Life
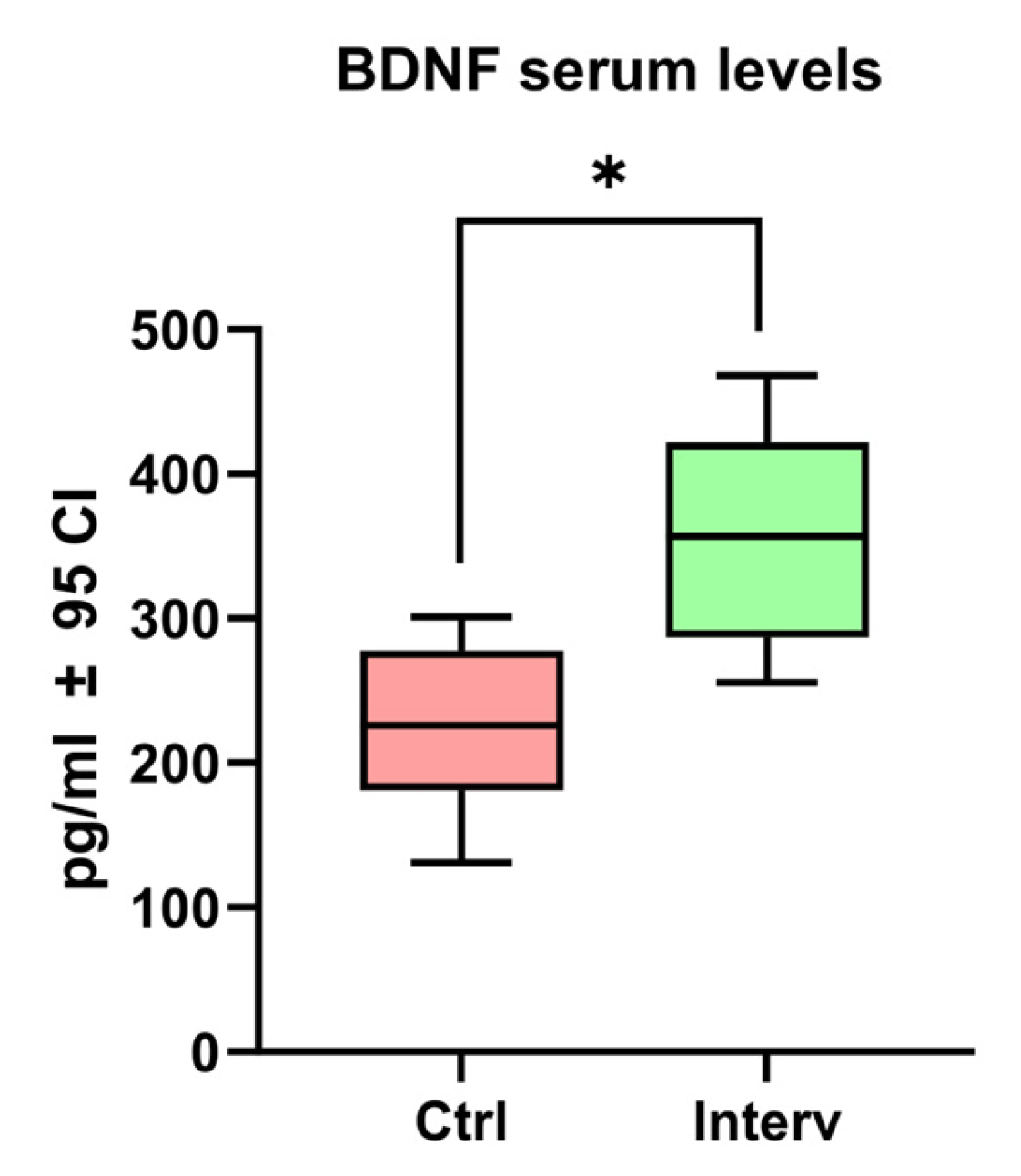
3.4. BDNF Serum Levels
4. Discussion
4.1. Perspectives for Clinical Practice
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Use of Artificial Intelligence
Acknowledgments
Conflicts of Interest
Abbreviations
| BDNF | Brain-Derived Neurotrophic Factor |
| BANFE-3 | Neuropsychological Executive Functions and Frontal Lobes battery-3 |
| GDS-15 | Yesavage Geriatric Depression Scale |
| ADL | Autonomy in activities of daily living |
| WHOQOL-OLD | World Health Organization Quality of Life-Old |
| WM | Working memory |
Appendix A. Exercise Schedule Used During the 120 Sessions

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1st Week | 2nd Week | 3rd Week | 4th Week | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Paper activities | S1 | S2 | S3 | S4 | S5 | S6 | S7 | S8 | S9 | S10 | S11 | S12 | S13 | S14 | S15 | S16 | S17 | S18 | S19 | S20 |
| 10.5 | 14.5 | 25.7 | 6.5 | 18.9 | 13.8 | 17.3 | 22.4 | 21.7 | 23.1 | 16.5 | 12.10 | 22.5 | 24.3 | 10.3 | 25.1 | 11.10 | 15.1 | 5.1 | 9.10 | |
| 3.1 | 11.3 | 8.5 | 5.4 | 6.1 | 14.10 | 3.2 | 2.3 | 26.7 | 9.5 | 23.7 | 11.6 | 12.5 | 16.7 | 1.4 | 7.6 | 21.1 | 19.7 | 9.8 | 28.3 | |
| 6.4 | 21.4 | 10.7 | 22.3 | 8.4 | 9.1 | 18.10 | 2.1 | 18.3 | 17.6 | 15.2 | 22.10 | 27.8 | 2.8 | 27.3 | 12.3 | 9.2 | 24.7 | 26.4 | 12.9 | |
| 19.3 | 20.8 | 27.1 | 10.2 | 19.8 | 22.2 | 19.10 | 8.10 | 23.10 | 12.6 | 26.8 | 5.2 | 10.8 | 16.4 | 4.7 | 3.5 | 18.7 | 21.3 | 3.10 | 5.3 | |
| 19.1 | 9.7 | 20.10 | 13.3 | 20.4 | 27.4 | 14.7 | 6.8 | 2.10 | 28.4 | 16.1 | 26.10 | 28.6 | 13.5 | 7.7 | 3.6 | 26.6 | 5.10 | 1.5 | 7.5 | |
| 21.10 | 23.6 | 26.9 | 27.6 | 20.3 | 26.2 | 17.2 | 22.6 | 7.1 | 7.3 | 8.9 | 24.6 | 24.8 | 9.9 | 3.9 | 4.2 | 28.5 | 21.6 | 24.10 | 15.6 | |
| 20.1 | 12.4 | 8.3 | 2.5 | 7.9 | 13.7 | 14.4 | 4.9 | 17.9 | 23.5 | 1.10 | 27.9 | 16.2 | 6.6 | 12.1 | 2.4 | 4.3 | 28.9 | 20.6 | 11.9 | |
| Board games | Dominoes | Take it all | Loteria | Snakes and ladders | Foosball | Bowling | Jenga® | Lottery | Golfito | Uno® | Jenga | Chinese chopsticks | Marbles | The game of the goose | Dominoes | Take it all | Loteria | Snakes and ladders | Foosball | Bowling |
| 5th Week | 6th Week | 7th Week | 8th Week | |||||||||||||||||
| Paper activities | S21 | S22 | S23 | S24 | S25 | S26 | S27 | S28 | S29 | S30 | S31 | S32 | S33 | S34 | S35 | S36 | S37 | S38 | S39 | S40 |
| 17.10 | 23.3 | 7.4 | 12.7 | 20.5 | 5.7 | 23.4 | 27.2 | 15.9 | 12.2 | 3.7 | 7.8 | 26.5 | 18.4 | 11.4 | 10.6 | 15.5 | 18.2 | 2.9 | 23.2 | |
| 25.9 | 5.8 | 8.6 | 3.3 | 9.6 | 22.9 | 17.1 | 1.3 | 20.7 | 19.6 | 4.6 | 26.3 | 23.8 | 11.8 | 15.4 | 1.8 | 8.8 | 27.5 | 19.9 | 25.3 | |
| 13.1 | 14.8 | 21.9 | 4.8 | 2.7 | 28.2 | 21.5 | 26.1 | 13.9 | 15.8 | 12.8 | 24.5 | 11.2 | 24.9 | 1.7 | 13.10 | 15.3 | 11.5 | 17.5 | 17.8 | |
| 10.4 | 14.2 | 11.7 | 28.1 | 14.3 | 22.8 | 8.1 | 8.7 | 22.7 | 17.4 | 25.4 | 16.8 | 10.9 | 16.10 | 1.6 | 18.6 | 14.9 | 14.6 | 16.3 | 1.2 | |
| 20.2 | 23.9 | 10.1 | 5.6 | 25.10 | 24.1 | 13.4 | 18.1 | 6.7 | 21.8 | 5.9 | 4.4 | 13.2 | 25.5 | 1.9 | 6.9 | 25.8 | 3.4 | 6.10 | 25.2 | |
| 19.2 | 19.5 | 15.7 | 9.4 | 4.5 | 13.6 | 10.10 | 3.8 | 9.3 | 2.2 | 28.10 | 28.8 | 18.8 | 6.2 | 25.6 | 19.4 | 5.5 | 24.4 | 24.2 | 14.1 | |
| 11.1 | 7.2 | 27.10 | 15.10 | 1.1 | 4.1 | 4.10 | 27.7 | 17.7 | 2.6 | 16.6 | 16.9 | 6.3 | 20.9 | 8.2 | 18.5 | 7.10 | 28.7 | 21.2 | 22.1 | |
| Board games | Dominoes | Take it all | Loteria | Snakes and ladders | Foosball | Bowling | Jenga® | Lottery | Golfito | Uno® | Jenga | Chinese chopsticks | Marbles | The game of the goose | Dominoes | Take it all | Loteria | Snakes and ladders | Foosball | Bowling |
| 9th Week | 10th Week | 11th Week | 12th Week | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Paper activities | S1 | S2 | S3 | S4 | S5 | S6 | S7 | S8 | S9 | S10 | S11 | S12 | S13 | S14 | S15 | S16 | S17 | S18 | S19 | S20 |
| 10.12 | 21.11 | 6.16 | 1.18 | 15.13 | 26.18 | 19.12 | 10.14 | 21.15 | 18.14 | 18.20 | 3.14 | 25.12 | 16.18 | 28.12 | 15.18 | 8.12 | 9.19 | 16.11 | 22.17 | |
| 20.14 | 17.16 | 5.15 | 18.13 | 10.11 | 13.12 | 19.17 | 3.15 | 20.12 | 15.17 | 2.17 | 13.14 | 5.17 | 4.18 | 16.19 | 14.14 | 7.18 | 12.20 | 27.18 | 25.11 | |
| 21.12 | 17.15 | 17.14 | 2.14 | 27.14 | 5.11 | 18.12 | 14.16 | 12.18 | 27.19 | 17.12 | 4.19 | 22.15 | 21.19 | 1.12 | 14.20 | 1.17 | 9.13 | 20.13 | 28.20 | |
| 28.16 | 14.12 | 13.13 | 1.16 | 17.20 | 22.13 | 6.12 | 5.14 | 4.17 | 8.16 | 10.16 | 13.17 | 13.19 | 16.17 | 13.20 | 1.15 | 15.15 | 12.16 | 19.13 | 26.14 | |
| 10.19 | 7.13 | 15.16 | 6.20 | 15.11 | 10.18 | 23.18 | 24.18 | 14.18 | 19.18 | 25.14 | 3.12 | 12.15 | 19.16 | 24.14 | 4.11 | 8.17 | 1.20 | 14.13 | 24.20 | |
| 9.17 | 20.17 | 25.20 | 15.20 | 11.15 | 24.17 | 16.14 | 8.18 | 3.20 | 2.20 | 27.20 | 21.16 | 24.13 | 16.20 | 8.19 | 26.17 | 26.15 | 11.16 | 23.14 | 23.11 | |
| 23.17 | 27.13 | 28.18 | 8.14 | 27.11 | 14.11 | 28.14 | 27.16 | 4.13 | 19.19 | 17.19 | 26.19 | 23.13 | 4.16 | 16.13 | 19.11 | 5.20 | 21.17 | 23.16 | 28.17 | |
| Board games | UNO® | Dominoes | Loteria | Chinese chopsticks | Snakes and ladders | The game of the goose | Marbles | Bowling | Take it all | Foosball | Fenga® | Golfito | UNO® | Dominoes | Loteria | Chinese chopsticks | Snakes and ladders | The game of the goose | Marbles | Bowling |
| 13th Week | 14th Week | 15th Week | 16th Week | |||||||||||||||||
| Paper activities | S21 | S22 | S23 | S24 | S25 | S26 | S27 | S28 | S29 | S30 | S31 | S32 | S33 | S34 | S35 | S36 | S37 | S38 | S39 | S40 |
| 19.20 | 12.14 | 3.11 | 2.18 | 18.18 | 14.15 | 4.12 | 11.20 | 11.13 | 23.20 | 24.16 | 17.17 | 17.11 | 21.20 | 7.12 | 6.11 | 21.14 | 17.18 | 21.18 | 13.11 | |
| 16.15 | 16.16 | 28.15 | 12.19 | 22.11 | 26.12 | 7.16 | 6.14 | 4.20 | 2.12 | 6.15 | 7.19 | 12.11 | 20.16 | 16.12 | 10.15 | 10.13 | 12.17 | 18.15 | 12.13 | |
| 24.15 | 4.15 | 7.15 | 4.14 | 8.15 | 5.19 | 8.11 | 3.16 | 22.19 | 9.11 | 26.11 | 2.16 | 28.11 | 21.13 | 17.13 | 13.16 | 3.17 | 19.14 | 15.14 | 25.16 | |
| 9.15 | 7.14 | 20.15 | 9.12 | 9.20 | 1.19 | 3.13 | 19.15 | 9.16 | 11.11 | 8.13 | 1.11 | 28.19 | 26.13 | 6.17 | 5.18 | 14.19 | 22.16 | 11.19 | 11.14 | |
| 10.17 | 11.17 | 27.15 | 8.20 | 26.20 | 28.13 | 2.19 | 24.11 | 22.18 | 22.12 | 20.19 | 3.19 | 27.17 | 6.19 | 20.11 | 22.20 | 25.13 | 6.13 | 2.13 | 18.16 | |
| 2.11 | 5.12 | 7.11 | 13.18 | 27.12 | 20.20 | 18.19 | 14.17 | 23.19 | 11.18 | 26.16 | 24.19 | 5.13 | 11.12 | 3.18 | 5.16 | 2.15 | 9.14 | 6.18 | 7.17 | |
| 18.17 | 1.14 | 12.12 | 15.19 | 24.12 | 10.20 | 7.20 | 25.19 | 20.18 | 1.13 | 18.11 | 25.17 | 15.12 | 25.18 | 9.18 | 13.15 | 23.15 | 23.12 | 22.14 | 25.15 | |
| Board games | Take it all | Foosball | Jenga® | Golfito | UNO® | Dominoes | Loteria | Chinese chopsticks | Snakes and ladders | The game of the goose | Marbles | Bowling | Take it all | Foosball | Jenga® | Golfito | UNO® | Dominoes | Loteria | Chinese chopsticks |
| 17th Week | 18th Week | 19th Week | 20th Week | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Paper activities | S1 | S2 | S3 | S4 | S5 | S6 | S7 | S8 | S9 | S10 | S11 | S12 | S13 | S14 | S15 | S16 | S17 | S18 | S19 | S20 |
| 22.29 | 8.21 | 7.21 | 14.23 | 5.26 | 10.30 | 15.26 | 20.21 | 17.27 | 6.24 | 2.25 | 13.23 | 14.25 | 19.26 | 1.21 | 14.30 | 7.24 | 13.30 | 15.23 | 11.29 | |
| 10.28 | 24.28 | 3.27 | 13.26 | 11.23 | 10.29 | 23.25 | 2.30 | 16.29 | 20.29 | 24.21 | 15.22 | 15.29 | 14.21 | 8.24 | 2.26 | 4.25 | 15.27 | 21.23 | 28.22 | |
| 25.21 | 7.25 | 12.28 | 26.28 | 11.21 | 11.22 | 9.29 | 5.30 | 28.27 | 11.27 | 22.24 | 7.26 | 15.30 | 11.28 | 26.21 | 17.21 | 28.23 | 24.30 | 5.21 | 28.21 | |
| 20.26 | 26.30 | 26.27 | 25.28 | 21.25 | 24.27 | 4.22 | 23.22 | 8.22 | 14.28 | 12.26 | 4.28 | 20.24 | 26.22 | 1.23 | 25.26 | 22.25 | 1.26 | 8.23 | 1.27 | |
| 26.24 | 23.21 | 17.22 | 13.28 | 10.26 | 8.29 | 2.21 | 16.21 | 19.28 | 13.21 | 17.23 | 10.21 | 8.27 | 9.25 | 18.28 | 5.27 | 3.29 | 8.30 | 14.26 | 9.23 | |
| 6.26 | 3.25 | 17.28 | 18.25 | 18.29 | 23.23 | 3.21 | 5.24 | 5.29 | 3.30 | 24.24 | 2.27 | 19.23 | 24.26 | 10.23 | 11.26 | 6.23 | 11.30 | 20.30 | 17.30 | |
| 25.27 | 9.21 | 21.24 | 26.29 | 16.24 | 24.25 | 21.30 | 1.30 | 12.24 | 2.28 | 23.30 | 13.29 | 12.30 | 21.28 | 10.25 | 19.25 | 23.27 | 12.21 | 27.24 | 6.27 | |
| Board games | Dominoes | Take it all | Loteria | Snakes and ladders | Foosball | Bowling | Jenga® | Lottery | Golfito | UNO® | Jenga | Chinese chopsticks | Marbles | The game of the goose | Dominoes | Take it all | Loteria | Snakes and ladders | Foosball | Bowling |
| 21th Week | 22th Week | 23th Week | 24th Week | |||||||||||||||||
| Paper activities | S21 | S22 | S23 | S24 | S25 | S26 | S27 | S28 | S29 | S30 | S31 | S32 | S33 | S34 | S35 | S36 | S37 | S38 | S39 | S40 |
| 1.24 | 18.30 | 20.23 | 23.26 | 1.22 | 6.25 | 2.24 | 9.27 | 27.29 | 5.23 | 12.23 | 9.24 | 27.28 | 6.22 | 12.29 | 19.27 | 19.29 | 24.29 | 27.30 | 11.24 | |
| 4.29 | 25.30 | 26.23 | 3.28 | 1.28 | 2.23 | 20.27 | 8.28 | 15.25 | 7.29 | 17.29 | 18.24 | 3.26 | 13.25 | 22.30 | 3.24 | 6.30 | 16.22 | 21.27 | 18.23 | |
| 28.24 | 17.25 | 7.22 | 14.22 | 13.27 | 26.26 | 22.22 | 12.22 | 22.27 | 7.23 | 19.30 | 15.28 | 16.25 | 20.22 | 16.23 | 6.28 | 10.22 | 19.22 | 25.22 | 27.26 | |
| 28.25 | 19.21 | 4.24 | 10.24 | 23.24 | 1.29 | 12.27 | 21.26 | 18.27 | 21.21 | 28.29 | 22.23 | 6.29 | 4.27 | 6.21 | 7.27 | 22.26 | 24.22 | 5.22 | 8.25 | |
| 15.24 | 16.30 | 25.23 | 3.22 | 25.29 | 15.21 | 14.24 | 20.28 | 8.26 | 13.24 | 24.23 | 22.21 | 27.25 | 4.21 | 16.26 | 21.29 | 27.22 | 7.30 | 28.26 | 28.28 | |
| 12.25 | 18.22 | 27.27 | 9.28 | 13.22 | 4.26 | 21.22 | 17.26 | 5.28 | 23.29 | 27.21 | 5.25 | 4.30 | 28.30 | 18.26 | 7.28 | 9.22 | 14.27 | 20.25 | 26.25 | |
| 16.27 | 25.24 | 19.24 | 16.28 | 4.23 | 23.28 | 22.28 | 2.22 | 1.25 | 9.26 | 10.27 | 2.29 | 17.24 | 18.21 | 9.30 | 27.23 | 14.29 | 3.23 | 11.25 | 25.25 | |
| Board games | Jenga® | Lottery | Golfito | UNO® | Jenga | Chinese chopsticks | Marbles | The game of the goose | Dominoes | Take it all | Toteria | Snakes and ladders | Foosball | Bowling | Jenga® | Lottery | Golfito | UNO® | Jenga | Chinese chopsticks |
References
- Rudnicka, E.; Napierała, P.; Podfigurna, A.; Męczekalski, B.; Smolarczyk, R.; Grymowicz, M. The World Health Organization (WHO) Approach to Healthy Ageing. Maturitas 2020, 139, 6–11. [Google Scholar] [CrossRef] [PubMed]
- PAHO. La Demencia en América Latina y el Caribe: Prevalencia, Incidencia, Repercusiones y Tendencias a lo Largo del Tiempo; PAHO: Washington, DC, USA, 2023. [Google Scholar]
- Friedman, N.P.; Robbins, T.W. The Role of Prefrontal Cortex in Cognitive Control and Executive Function. Neuropsychopharmacology 2022, 47, 72–89. [Google Scholar] [CrossRef]
- Idowu, M.I.; Szameitat, A.J. Executive Function Abilities in Cognitively Healthy Young and Older Adults-A Cross-Sectional Study. Front. Aging Neurosci. 2023, 15, 976915. [Google Scholar] [CrossRef]
- Raimo, S.; Maggi, G.; Ilardi, C.R.; Cavallo, N.D.; Torchia, V.; Pilgrom, M.A.; Cropano, M.; Roldán-Tapia, M.D.; Santangelo, G. The Relation between Cognitive Functioning and Activities of Daily Living in Normal Aging, Mild Cognitive Impairment, and Dementia: A Meta-Analysis. Neurol. Sci. 2024, 45, 2427–2443. [Google Scholar] [CrossRef]
- Feng, Z.; Chen, Q.; Li, Y.; Xue, Z.; Hao, X. The Association between Falls and Depressive Symptoms among Older Adults: Evidence from the China Health and Retirement Longitudinal Study. Front. Public Health 2023, 11, 1248551. [Google Scholar] [CrossRef]
- Choi, N.G.; Zhou, Y.; Marti, C.N.; Kunik, M.E. Associations between Changes in Depression/Anxiety Symptoms and Fall Worry among Community-Dwelling Older Adults. J. Appl. Gerontol. 2022, 41, 2520. [Google Scholar] [CrossRef]
- Carcelén-Fraile, M.D.C.; Llera-Delatorre, A.M.; Aibar-Almazán, A.; Afanador-Restrepo, D.F.; Baena-Marín, M.; Hita-Contreras, F.; Brandão-Loureiro, V.; García-Garro, P.A.; Castellote-Caballero, Y. Cognitive Stimulation as Alternative Treatment to Improve Psychological Disorders in Patients with Mild Cognitive Impairment. J. Clin. Med. 2022, 11, 3947. [Google Scholar] [CrossRef]
- Alvares-Pereira, G.; Silva-Nunes, M.V.; Spector, A. Validation of the Cognitive Stimulation Therapy (CST) Program for People with Dementia in Portugal. Aging Ment. Health 2021, 25, 1019–1028. [Google Scholar] [CrossRef]
- Da Silva, T.B.L.; Dos Santos, G.; Moreira, A.P.B.; Ishibashi, G.A.; Verga, C.E.R.; De Moraes, L.C.; Lessa, P.P.; Cardoso, N.P.; Ordonez, T.N.; Brucki, S.M.D. Cognitive Interventions in Mature and Older Adults, Benefits for Psychological Well-Being and Quality of Life: A Systematic Review Study. Dement. Neuropsychol. 2021, 15, 428–439. [Google Scholar] [CrossRef]
- Srisuwan, P.; Nakawiro, D.; Chansirikarnjana, S.; Kuha, O.; Chaikongthong, P.; Suwannagoot, T. Effects of a Group-Based 8-Week Multicomponent Cognitive Training on Cognition, Mood and Activities of Daily Living among Healthy Older Adults: A One-Year Follow-Up of a Randomized Controlled Trial. J. Prev. Alzheimers Dis. 2020, 7, 112–121. [Google Scholar] [CrossRef]
- Sanjuán, M.; Navarro, E.; Dolores Calero, M. Effectiveness of Cognitive Interventions in Older Adults: A Review. Eur. J. Investig. Health Psychol. Educ. 2020, 10, 876. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Soria, I.; Peralta-Marrupe, P.; Plo, F. Cognitive Stimulation Program in Mild Cognitive Impairment A Randomized Controlled Trial. Dement. Neuropsychol. 2020, 14, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Woods, B.; Rai, H.K.; Elliott, E.; Aguirre, E.; Orrell, M.; Spector, A. Cognitive Stimulation to Improve Cognitive Functioning in People with Dementia. Cochrane Database Syst. Rev. 2023, 2023, CD005562. [Google Scholar]
- Gray, M.; Gills, J.L.; Glenn, J.M.; Vincenzo, J.L.; Walter, C.S.; Madero, E.N.; Hall, A.; Fuseya, N.; Bott, N.T. Cognitive Decline Negatively Impacts Physical Function. Exp. Gerontol. 2020, 143, 111164. [Google Scholar] [CrossRef]
- Sokołowski, D.R.; Hansen, T.I.; Rise, H.H.; Reitlo, L.S.; Wisløff, U.; Stensvold, D.; Håberg, A.K. 5 Years of Exercise Intervention Did Not Benefit Cognition Compared to the Physical Activity Guidelines in Older Adults, but Higher Cardiorespiratory Fitness Did. A Generation 100 Substudy. Front. Aging Neurosci. 2021, 13, 742587. [Google Scholar] [CrossRef] [PubMed]
- Sandison, H.; Callan, N.G.L.; Rao, R.V.; Phipps, J.; Bradley, R. Observed Improvement in Cognition During a Personalized Lifestyle Intervention in People with Cognitive Decline. J. Alzheimer’s Dis. 2023, 94, 993. [Google Scholar] [CrossRef]
- Dinius, C.J.; Pocknell, C.E.; Caffrey, M.P.; Roche, R.A.P. Cognitive Interventions for Memory and Psychological Well-Being in Aging and Dementias. Front. Psychol. 2023, 14, 1070012. [Google Scholar] [CrossRef]
- Justo-Henriques, S.I.; Marques-Castro, A.E.; Otero, P.; Vázquez, F.L.; Torres, Á.J. Long-Term Individual Cognitive Stimulation Program in Patients with Mild Neurocognitive Disorder: A Pilot Study. Rev. Neurol. 2019, 68, 281–289. [Google Scholar]
- Chiu, H.L.; Chu, H.; Tsai, J.C.; Liu, D.; Chen, Y.R.; Yang, H.L.; Chou, K.R. The Effect of Cognitive-Based Training for the Healthy Older People: A Meta-Analysis of Randomized Controlled Trials. PLoS ONE 2017, 12, e0176742. [Google Scholar] [CrossRef]
- Justo-Henriques, S.I.; Otero, P.; Torres, Á.J.; Vázquez, F.L. Effect of Long-Term Individual Cognitive Stimulation Intervention for People with Mild Neurocognitive Disorder. Rev. Neurol. 2021, 73, 121–129. [Google Scholar]
- Cheng, C.; Ebrahimi, O.V. Gamification: A Novel Approach to Mental Health Promotion. Curr. Psychiatry Rep. 2023, 25, 577. [Google Scholar] [CrossRef]
- Pisani, A.; Paciello, F.; Del Vecchio, V.; Malesci, R.; De Corso, E.; Cantone, E.; Fetoni, A.R. The Role of BDNF as a Biomarker in Cognitive and Sensory Neurodegeneration. J. Pers. Med. 2023, 13, 652. [Google Scholar] [CrossRef]
- Nicastri, C.M.; McFeeley, B.M.; Simon, S.S.; Ledreux, A.; Håkansson, K.; Granholm, A.C.; Mohammed, A.H.; Daffner, K.R. BDNF Mediates Improvement in Cognitive Performance after Computerized Cognitive Training in Healthy Older Adults. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2022, 8, e12337. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef]
- Acosta, C.O.; Palacio, R.R.; Cortez, J.; Echeverría, S.B.; Rodríguez-Fórtiz, M.J. Effects of a Cognitive Stimulation Software on Attention, Memory, and Activities of Daily Living in Mexican Older Adults. Univers. Access Inf. Soc. 2022, 21, 21–31. [Google Scholar] [CrossRef]
- Mondragón-Maya, A.; Flores-Medina, Y.; López-Arreaga, G.; López-Ramírez, S.; Paz-Rodríguez, F. Funciones Ejecutivas En Estudiantes Universitarios Con Patrón de Consumo Excesivo de Alcohol. Psicol. Salud 2021, 31, 295–306. [Google Scholar] [CrossRef]
- Valenzuela, M.J.; Sachdev, P. Brain Reserve and Dementia: A Systematic Review. Psychol. Med. 2006, 36, 441–454. [Google Scholar] [CrossRef]
- Miranda de Jesus, Y.; Álvarez Orozco, M.E.; Álvarez Hernández, H.J.; Jaimes Cortés, D.; Alvarado Reyes, E.R. Factores Que Desencadenan Depresión En El Adulto Mayor de La Comunidad de Santiaguito Maxda, Estado de México. Dilemas Contemp. Educ. Política Valores 2020, 2020, 8. [Google Scholar] [CrossRef]
- Krystal Salgado Cedano, Y.; Andrade Palos, P.; Hernández Galván, A.; Ivonne González-Arriata López-Fuentes, N.; en Psicología, D.; Eduardo Velasco Rojano, Á. Validación de La Escala de Depresión Geriátrica de Yesavage En Adultos Mayores Mexicanos. Inf. Psicol. 2024, 24, 123–135. [Google Scholar] [CrossRef]
- Alonso, M.A.M.; Barajas, M.E.S.; Ordóñez, J.A.G.; Alpirez, H.Á.; Fhon, J.R.S.; Duran-Badillo, T. Quality of Life Related to Functional Dependence, Family Functioning and Social Support in Older Adults*. Rev. Esc. Enferm. 2022, 56, e20210482. [Google Scholar] [CrossRef]
- Dos Reis, N.F.; Figueiredo, F.C.X.S.; Biscaro, R.R.M.; Lunardelli, E.B.; Maurici, R. Psychometric Properties of the Barthel Index Used at Intensive Care Unit Discharge. Am. J. Crit. Care 2022, 31, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Elizabeth Duarte-Ayala, R.; Ángel Eduardo Velasco-Rojano, D.; Elizabeth Duarte Ayala Dirección postal, R.; de Las Aves, P.; Mateo Nopala, S.; de Juárez, N.; de México, C.; Mayor, A. Validación Psicométrica Del Índice de Barthel En Adultos Mayores Mexicanos. Horiz. Sanit. 2022, 21, 113–120. [Google Scholar]
- Pekçetin, E.; Pekçetin, S.; Sağlamoğlu, E.; Ekici, G. Urban versus Rural Older Adults: Occupational Balance and Quality of Life Comparison. BMC Geriatr. 2025, 25, 49. [Google Scholar] [CrossRef]
- Díaz de León Castañeda, C.; Anguiano-Morán, A.C.; Valtierra-Oba, E.R.; Lemus-Loeza, B.M.; Galván-Villalobos, G.; Rodríguez-Orozco, A.R. Psychometric Properties of the World Health Organization Quality of Life Scale for Older Adults (WHO-QoL-Old) in a Mexican Population. Geriatrics 2024, 9, 134. [Google Scholar] [CrossRef]
- Yates, L.A. Individual Cognitive Stimulation Therapy (ICST). In Cognitive Stimulation Therapy for Dementia; Routledge: New York, NY, USA, 2018; pp. 69–88. [Google Scholar]
- Stern, Y. What Is Cognitive Reserve? Theory and Research Application of the Reserve Concept. J. Int. Neuropsychol. Soc. 2002, 8, 448–460. [Google Scholar] [CrossRef]
- Van Loenhoud, A.C.; Van Der Flier, W.M.; Wink, A.M.; Dicks, E.; Groot, C.; Twisk, J.; Barkhof, F.; Scheltens, P.; Ossenkoppele, R. Cognitive Reserve and Clinical Progression in Alzheimer Disease: A Paradoxical Relationship. Neurology 2019, 93, e334–e346. [Google Scholar] [CrossRef]
- Koch, G.; Spampinato, D. Alzheimer Disease and Neuroplasticity. Handb. Clin. Neurol. 2022, 184, 473–479. [Google Scholar]
- Dreer, L.E.; Copeland, J.N.; Cheavens, J.S. Integrating Neuropsychological Functioning into Cognitive Behavioral Therapy: Implications for Older Adults. In Cognitive Behavior Therapy with Older Adults: Innovations Across Care Settings; Springer Publishing Company: New York, NY, USA, 2011; pp. 317–365. [Google Scholar]
- Justo-Henriques, S.I. Individual Intervention Protocol Based on Cognitive Stimulation Therapy for Older Adults with Mild Neurocognitive Disorder. Rev. Enferm. Ref. 2021, 2021, 5. [Google Scholar]
- Gómez-Soria, I.; Iguacel, I.; Aguilar-Latorre, A.; Peralta-Marrupe, P.; Latorre, E.; Zaldívar, J.N.C.; Calatayud, E. Cognitive Stimulation and Cognitive Results in Older Adults: A Systematic Review and Meta-Analysis. Arch. Gerontol. Geriatr. 2023, 104, 104807. [Google Scholar] [CrossRef]
- Yun, S.; Ryu, S. The Effects of Cognitive-Based Interventions in Older Adults: A Systematic Review and Meta-Analysis. Iran. J. Public Health 2022, 51, 1–11. [Google Scholar] [CrossRef]
- Ledreux, A.; Håkansson, K.; Carlsson, R.; Kidane, M.; Columbo, L.; Terjestam, Y.; Ryan, E.; Tusch, E.; Winblad, B.; Daffner, K.; et al. Differential Effects of Physical Exercise, Cognitive Training, and Mindfulness Practice on Serum BDNF Levels in Healthy Older Adults: A Randomized Controlled Intervention Study. J. Alzheimer’s Dis. 2019, 71, 1245–1261. [Google Scholar] [CrossRef]
- Romero Garavito, A.; Díaz Martínez, V.; Juárez Cortés, E.; Negrete Díaz, J.V.; Montilla Rodríguez, L.M. Impact of Physical Exercise on the Regulation of Brain-Derived Neurotrophic Factor in People with Neurodegenerative Diseases. Front. Neurol. 2025, 15, 1505879. [Google Scholar] [CrossRef]
- Lukkahatai, N.; Ong, I.L.; Benjasirisan, C.; Saligan, L.N. Brain-Derived Neurotrophic Factor (BDNF) as a Marker of Physical Exercise or Activity Effectiveness in Fatigue, Pain, Depression, and Sleep Disturbances: A Scoping Review. Biomedicines 2025, 13, 332. [Google Scholar] [CrossRef]
- Gholami, F.; Mesrabadi, J.; Iranpour, M.; Donyaei, A. Exercise Training Alters Resting Brain-Derived Neurotrophic Factor Concentration in Older Adults: A Systematic Review with Meta-Analysis of Randomized-Controlled Trials. Exp. Gerontol. 2025, 199, 112658. [Google Scholar] [CrossRef]
- Gan, J.; He, J.; Zhou, K.; Shang, Z.; Dong, G.; Bao, D.; Zhou, J. Effects of Traditional Chinese Exercises on Brain-Derived Neurotrophic Factor in Middle-Aged and Older Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Exerc. Sci. Fit. 2025, 23, 32–41. [Google Scholar] [CrossRef]
- Grossberg, A.N.; Bettcher, B.M.; Gorgens, K.A.; Ledreux, A. Curiosity-Based Interventions Increase Everyday Functioning Score But Not Serum BDNF Levels in a Cohort of Healthy Older Adults. Front. Aging 2021, 2, 700838. [Google Scholar] [CrossRef]
- Sanaeifar, F.; Pourranjbar, S.; Pourranjbar, M.; Ramezani, S.; Mehr, S.R.; Wadan, A.H.S.; Khazeifard, F. Beneficial Effects of Physical Exercise on Cognitive-Behavioral Impairments and Brain-Derived Neurotrophic Factor Alteration in the Limbic System Induced by Neurodegeneration. Exp. Gerontol. 2024, 195, 112539. [Google Scholar] [CrossRef]
- Krivanek, T.J.; Gale, S.A.; McFeeley, B.M.; Nicastri, C.M.; Daffner, K.R. Promoting Successful Cognitive Aging: A Ten-Year Update. J. Alzheimer’s Dis. 2021, 81, 871–920. [Google Scholar] [CrossRef]
- Ayoubi-Mahani, S.; Eghbali-Babadi, M.; Farajzadegan, Z.; Keshvari, M.; Farokhzadian, J. Active Aging Needs from the Perspectives of Older Adults and Geriatric Experts: A Qualitative Study. Front. Public Health 2023, 11, 1121761. [Google Scholar] [CrossRef]
- Hanifa, A.L.B.; Alrø, A.B.; Holm, A.; Dreyer, P. Nurses’ Experiences of Managing Cognitive Problems in Intensive Care Unit Patients: A Qualitative Study. Intensive Crit. Care Nurs. 2023, 79, 103508. [Google Scholar] [CrossRef]
- Cangelosi, G.; Mancin, S.; Pantanetti, P.; Thi, C.; Nguyen, T.; Palomares, S.M.; Biondini, F.; Sguanci, M.; Petrelli, F. Lifestyle Medicine Case Manager Nurses for Type Two Diabetes Patients: An Overview of a Job Description Framework—A Narrative Review. Diabetology 2024, 5, 375–388. [Google Scholar] [CrossRef]
- Mishra, B.; Pradhan, J. Impact of Social Isolation and Leisure Activities on Cognition and Depression: A Study on Middle-Aged and Older Adults in India. Int. J. Geriatr. Psychiatry 2023, 38, e5946. [Google Scholar] [CrossRef]
| Content | Duration | Activities |
|---|---|---|
| Session introduction | 5 min | Greetings/welcome. Mood check. Communicate the aim of the session. |
| Reality orientation | 10 min | Identify time elements and address spatial elements (day of the week, month, day of the month, year, season of the year and weather conditions), using a time orientation chart. |
| Stimulation of cognitive domains | 40 min | Explore cognitive stimulation material regarding domains as cognitive flexibility, inhibitory control, working memory, planning, reasoning, attention, concentration and processing speed. |
| Session closure | 5 min | Analyze the difficulties, interests and benefits of the session. Goodbye. |
| Name of the Activity | Mainly Stimulated Cognitive Function | Level 1 | Level 2 | Level 3 |
|---|---|---|---|---|
| Reasoning, WM | Exercise 1.1 to 1.10 | Exercise 1.11 to 1.20 | Exercise 1.21 to 1.30. |
| WM, Attention, Reasoning | Exercise 2.1 to 2.10 | Exercise 2.11 to 2.20 | Exercise 2.21 to 2.30. |
| Cognitive flexibility, Attention, Reasoning | Exercise 3.1 to 3.10 | Exercise 3.11 to 3.20 | Exercise 3.21 to 3.30. |
| Reasoning, WM, Reasoning | Exercise 4.1 to 4.10 | Exercise 4.11 to 4.20 | Exercise 4.21 to 4.30 |
| Attention, Processing speed, Reasoning | Exercise 5.1 to 5.10 | Exercise 5.11 to 5.20 | Exercise 5.21 to 5.30 |
| Reasoning, WM, Reasoning | Exercise 6.1 to 6.10 | Exercise 6.11 to 6.20 | Exercise 6.21 to 6.30 |
| Reasoning, Planning, Reasoning | Exercise 7.1 to 7.10 | Exercise 7.11 to 7.20 | Exercise 7.21 to 7.30 |
| WM, Attention | Exercise 8.1 to 8.10 | Exercise 8.11 to 8.20 | Exercise 8.21 to 8.30 |
| Visual perception, Attention | Exercise 9.1 to 9.10 | Exercise 9.11 to 9.20 | Exercise 9.21 to 9.30 |
| Planning, Cognitive flexibility | Exercise 10.1 to 10.10 | Exercise 10.11 to 10.20 | Exercise 10.21 to 10.30 |
| Reasoning, Attention | Exercise 11.1 to 11.10 | Exercise 11.11 to 11.20 | Exercise 11.21 to 11.30 |
| Visual perception, Attention | Exercise 12.1 to 12.10 | Exercise 12.11 to 12.20 | Exercise 12.21 to 12.30 |
| Attention, WM | Exercise 13.1 to 13.10 | Exercise 13.11 to 13.20 | Exercise 13.21 to 13.30 |
| Attention, Spatial reasoning | Exercise 14.1 to 14.10 | Exercise 14.11 to 14.20 | Exercise 14.21 to 14.30 |
| WM, Visual perception | Exercise 15.1 to 15.10 | Exercise 15.11 to 15.20 | Exercise 15.21 to 15.30 |
| WM, Attention | Exercise 16.1 to 16.10 | Exercise 16.11 to 16.20 | Exercise 16.21 to 16.30 |
| WM, Processing speed | Exercise 17.1 to 17.10 | Exercise 17.11 to 17.20 | Exercise 17.21 to 17.30 |
| WM, Processing speed | Exercise 18.1 to 18.10 | Exercise 18.11 to 18.20 | Exercise 18.21 to 18.30 |
| WM, Processing speed | Exercise 19.1 to 19.10 | Exercise 19.11 to 19.20 | Exercise 19.21 to 19.30 |
| WM, Spatial reasoning | Exercise 20.1 to 20.10 | Exercise 20.11 to 20.20 | Exercise 20.21 to 20.30 |
| WM, Attention | Exercise 21.1 to 21.10 | Exercise 21.11 to 21.20 | Exercise 21.21 to 21.30 |
| Attention, Visual perception | Exercise 22.1 to 22.10 | Exercise 22.11 to 22.20 | Exercise 22.21 to 22.30 |
| Cognitive flexibility, Planning, Reasoning | Exercise 23.1 to 23.10 | Exercise 23.11 to 23.20 | Exercise 23.21 to 23.30 |
| Reasoning, WM | Exercise 24.1 to 24.10 | Exercise 24.11 to 24.20 | Exercise 24.21 to 24.30 |
| Attention, WM | Exercise 25.1 to 25.10 | Exercise 25.11 to 25.20 | Exercise 25.21 to 25.30 |
| Attention, Processing speed, WM | Exercise 26.1 to 26.10 | Exercise 26.11 to 26.20 | Exercise 26.21 to 26.30 |
| Reasoning, WM | Exercise 27.1 to 27.10 | Exercise 27.11 to 27.20 | Exercise 27.21 to 27.30 |
| Attention, Visual perception | Exercise 28.1 to 28.10 | Exercise 28.11 to 28.20 | Exercise 28.21 to 28.30 |
| Stimulated Cognitive Function | Board Game |
|---|---|
| Cognitive flexibility | UNO®, dominoes, loteria, Chinese chopsticks, snakes and ladders, the game of the goose, marbles, bowling and take it all. |
| Inhibitory control | UNO®, dominoes, loteria, Chinese chopsticks, snakes and ladders, the game of the goose, foosball, marbles, jenga® and take it all, |
| Working memory | UNO®, dominoes, lottery, Chinese chopsticks, snakes and ladders and the game of the goose |
| Planning | UNO®, dominoes, snakes and ladders and bowling. |
| Reasoning | UNO®, dominoes, loteria, Chinese chopsticks, snakes and ladders, the game of the goose, foosball, marbles, jenga, take it all and golfito. |
| Attention | UNO®, dominoes, loteria, Chinese chopsticks, snakes and ladders, the game of the goose, foosball, marbles, bowling, jenga®, take it all and golfito |
| Concentration and processing speed | UNO®, dominoes, loteria, Chinese chopsticks, snakes and ladders, the game of the goose, foosball, marbles, bowling, jenga®, take it all and golfito. |
| Variable | Control Group (n = 12) | Intervention Group (n = 24) | p | |
|---|---|---|---|---|
| Age (years) a | 66.17 ± 2.93 | 67.75 ± 4.75 | 0.732 d | |
| Gender b | Women | 6 (50) | 12 (50) | 0.982 c |
| Men | 6 (50) | 12 (50) | 0.973 c | |
| Level education c | Primary School | 2 (16.67) | 4 (16.67) | 0.181 c |
| Secondary School | 2 (16.67) | 4 (16.67) | 0.985 c | |
| High School | 2 (16.67) | 2 (8.33) | 0.075 c | |
| Technical School | 0 (0) | 2 (8.33) | 0.053 c | |
| High School | 4 (33.33) | 10 (41.67) | 0.184 c | |
| Postgraduate | 2 (16.67) | 2 (8.33) | 0.089 c | |
| Initial cognitive assessment score d | Total executive functions | 73.83 ± 20.63 | 80.75 ± 44.86 | 0.461 d |
| Orbitofrontal cortex | 75.50 ± 25.22 | 73.82 ± 24.77 | 0.775 d | |
| Anterior prefrontal cortex | 83.67 ± 28.97 | 82.64 ± 25.33 | 0.311 d | |
| Dorsolateral cortex | 82.17 ± 15.48 | 90.18 ± 14.84 | 0.285 d | |
| BANFE-3 | Control Group (n = 12) | Intervention Group (n = 24) | |||||
|---|---|---|---|---|---|---|---|
| Zone | Classification | Pre Evaluation | Post Evaluation | p | Pre Evaluation | Post Evaluation | p |
| Orbitofrontal | Score a | 75.50 ± 25.22 | 71.50 ± 14.77 | 0.832 d | 73.82 ± 24.77 | 85.17 ± 26.75 | 0.002 d |
| High normal b | 0 (0) | 0 (0) | - | 0 (0) | 0 (0) | - | |
| Normal b | 6 (50) | 6 (50) | 0.932 c | 2 (8.34) | 12 (50) | 0.009 c | |
| Mild–Mod impairment b | 2 (16.67) | 2 (16.67) | 0.948 c | 6 (25) | 10 (41.66) | 0.921 c | |
| Severe impairment b | 4 (33.33) | 4 (33.33) | 0.931 c | 16 (66.66) | 2 (8.34) | 0.012 c | |
| Anterior prefrontal | Score a | 83.67 ± 28.97 | 82.64 ± 25.33 | 0.124 d | 81.14 ± 26.22 | 100.28 ± 28.13 | 0.001 d |
| High normal b | 2 (16.67) | 2 (16.67) | 0.913 c | 2 (8.33) | 8 (33.33) | 0.018 c | |
| Normal b | 2 (16.67) | 2 (16.67) | 0.974 c | 14 (58.33) | 10 (41.67) | 0.045 c | |
| Mild–Mod impairment b | 4 (33.33) | 6 (50) | 0.113 c | 2 (8.33) | 4 (16.67) | 0.948 c | |
| Severe impairment b | 4 (33.33) | 2 (16.67) | 0.081 c | 6 (25) | 2 (8.33) | 0.214 c | |
| Dorsolateral | Score a | 82.17 ± 15.48 | 90.18 ± 14.84 | 0.372 d | 80.28 ± 18.54 | 112.67 ± 28.17 | 0.031 d |
| High normal b | 2 (16.67) | 2 (16.67) | 0.948 c | 2 (8.33) | 2 (8.33) | 0.965 c | |
| Normal b | 4 (66.67) | 6 (50) | 0.642 c | 16 (66.67) | 16 (66.67) | 0.924 c | |
| Mild–Mod impairment b | 2 (16.67) | 2 (16.67) | 0.985 c | 2 (8.33) | 6 (25) | 0.017 c | |
| Severe impairment b | 4 (33.33) | 2 (16.67) | 0.271 | 4 (16.67) | 0 (0) | 0.003 c | |
| Total executive functions | Score a | 73.83 ± 20.63 | 76.83 ± 11.89 | 0.823 d | 80.75 ± 44.86 | 93.17 ± 19.66 | 0.001 d |
| High normal b | 0 (0) | 0 (0) | - | 2 (8.33) | 2 (8.33) | 0.924 c | |
| Normal b | 6 (50) | 6 (50) | 0.924 c | 6 (25) | 12 (50) | 0.001 c | |
| Mild–Mod impairment b | 2 (16.67) | 4 (33.33) | 0.073 c | 12 (50) | 6 (33.34) | 0.438 c | |
| Severe impairment b | 4 (33.33) | 2 (16.67) | 0.091 c | 4 (16.67) | 2 (8.33) | 0.137 c | |
| BANFE-3 | Post Evaluation | p | ||
|---|---|---|---|---|
| Zone | Classification | Control Group (n = 12) | Intervention Group (n = 24) | |
| Orbitofrontal | Score a | 71.50 ± 14.77 | 85.17 ± 26.75 | 0.001 d |
| High normal b | 0 (0) | 0 (0) | - | |
| Normal b | 6 (50) | 12 (50) | 0.023 c | |
| Mild–Mod impairment b | 2 (16.67) | 10 (41.66) | 0.014 c | |
| Severe impairment b | 4 (33.33) | 2 (8.34) | 0.128 c | |
| Anterior prefrontal | Score a | 82.64 ± 25.33 | 100.28 ± 28.13 | 0.031 d |
| High normal b | 2 (16.67) | 8 (33.33) | 0.041 c | |
| Normal b | 2 (16.67) | 10 (41.67) | 0.017 c | |
| Mild–Mod impairment b | 6 (50) | 4 (16.67) | 0.016 c | |
| Severe impairment b | 2 (16.67) | 2 (8.33) | 0.928 c | |
| Dorsolateral | Score a | 90.18 ± 14.84 | 112.67 ± 28.17 | 0.009 d |
| High normal b | 2 (16.67) | 2 (8.33) | 0.352 c | |
| Normal b | 6 (50) | 16 (66.67) | 0.184 c | |
| Mild–Mod impairment b | 2 (16.67) | 6 (25) | 0.017 c | |
| Severe impairment b | 2 (16.67) | 0 (0) | 0.008 c | |
| Total executive functions | Score a | 76.83 ± 11.89 | 93.17 ± 19.66 | 0.028 d |
| High normal b | 0 (0) | 2 (8.33) | 0.031 c | |
| Normal b | 6 (50) | 12 (50) | 0.004 c | |
| Mild–Mod impairment b | 4 (33.33) | 8 (33.34) | 0.040 c | |
| Severe impairment b | 2 (16.67) | 2 (8.33) | 0.005 c | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cortés-Álvarez, N.Y.; Vuelvas-Olmos, C.R.; Marmolejo-Murillo, L.G.; Sánchez-Duarte, E.; Lara-Morales, A. Cognitive Stimulation and Its Effects on Well-Being, Executive Functions, and Brain-Derived Neurotrophic Factor in Older Adults from a Mexican Geriatric Center: A Quasi-Experimental Study. Nurs. Rep. 2025, 15, 151. https://doi.org/10.3390/nursrep15050151
Cortés-Álvarez NY, Vuelvas-Olmos CR, Marmolejo-Murillo LG, Sánchez-Duarte E, Lara-Morales A. Cognitive Stimulation and Its Effects on Well-Being, Executive Functions, and Brain-Derived Neurotrophic Factor in Older Adults from a Mexican Geriatric Center: A Quasi-Experimental Study. Nursing Reports. 2025; 15(5):151. https://doi.org/10.3390/nursrep15050151
Chicago/Turabian StyleCortés-Álvarez, Nadia Yanet, César Rubén Vuelvas-Olmos, Leticia Gabriela Marmolejo-Murillo, Elizabeth Sánchez-Duarte, and Alfredo Lara-Morales. 2025. "Cognitive Stimulation and Its Effects on Well-Being, Executive Functions, and Brain-Derived Neurotrophic Factor in Older Adults from a Mexican Geriatric Center: A Quasi-Experimental Study" Nursing Reports 15, no. 5: 151. https://doi.org/10.3390/nursrep15050151
APA StyleCortés-Álvarez, N. Y., Vuelvas-Olmos, C. R., Marmolejo-Murillo, L. G., Sánchez-Duarte, E., & Lara-Morales, A. (2025). Cognitive Stimulation and Its Effects on Well-Being, Executive Functions, and Brain-Derived Neurotrophic Factor in Older Adults from a Mexican Geriatric Center: A Quasi-Experimental Study. Nursing Reports, 15(5), 151. https://doi.org/10.3390/nursrep15050151