
Self-Care in Palliative Healthcare Professionals: A Qualitative Study
 ,
,
Abstract
1. Introduction
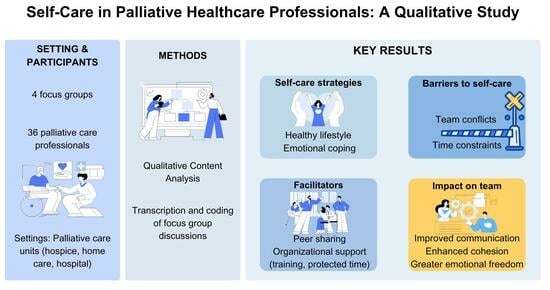
2. Materials and Methods
3. Results
3.1. Descriptive Analysis of the Sample
- focus group 1: eleven participants;
- focus group 2: eleven participants;
- focus group 3: six participants;
- focus group 4: eight participants.
3.2. Qualitative Content Analysis
3.2.1. First Question: “What Self-Care Strategies Do You Implement Most Frequently?”
- lifestyle strategies: taking care of physiological and physical aspects, such as maintaining a healthy lifestyle, ensuring restorative sleep and a balanced diet, taking care of oneself and one’s commitments, incorporating aromatherapy, and using essential oils;
- emotional coping strategies: physical isolation, finding moments of solitude to reconnect with oneself, maintaining a positive attitude, reflecting, crying, being able to disconnect from work at the end of the day;
- meaningful private life relationships: hanging out with loved ones, friends, relatives, and people who work in different professional settings and with whom you feel comfortable;
- taking care of others: volunteering, taking care of loved ones, patients, animals;
- psychological interventions: both individual (psychotherapy) and group and within the work context (supervision and psychodrama);
- discussion and sharing in teams: use of these strategies within the team;
- spiritual practices: meditation, yoga, prayer;
- physical activities: physical movement, walking, cycling;
- personal hobbies and passions: music, writing, reading and poetry, housework, cooking, handicrafts, shopping;
- contact with nature: trekking, taking care of plants.
3.2.2. Second Question: “Which Ones Do You Consider Most Effective? Why?”
- lifestyle strategies: maintaining regular sleep and eating habits to re-center oneself, while keeping a separation between work and personal life;
- emotional coping strategies: being aware of one’s emotions, isolating oneself and being silent, finding time for oneself;
- meaningful private life relationships: spending time with friends and family;
- discussion and sharing in teams: discussion, sharing, and mutual support;
- spiritual practices: individual and community prayer;
- physical activities: physical movement, sports, walking, cycling to feel free, achieve physical well-being, focus on the present moment, and as a challenge. Dance Movement Therapy is useful as an activity carried out in the company of a group;
- personal hobbies and passions: taking trips and new experiences to slow down and stop, listening to music, reading, doing housework, cooking;
- contact with nature: admiring nature, landscapes, plants, and the proximity of pets with the serenity and tranquility they convey.
3.2.3. Third Question: “What Does Taking Care of Yourself Mean to You?”
- self-awareness and self-knowledge: listening to oneself, knowing oneself, being self-aware, turning attention inward, accepting oneself and one’s limits, and forgiving oneself;
- connecting with one’s emotions: having deep contact with one’s emotions and feelings and knowing how to listen to them;
- seeking work-life balance: avoiding the transfer of personal problems and negative emotions into the workplace, and vice versa;
- taking time for oneself: taking care of oneself by attending to the physical and spiritual aspects, having a healthy lifestyle, making good use of time, stopping and momentarily freeing oneself from worries, practicing personal hobbies and spending time with loved ones and friends.
3.2.4. Fourth Question: “In Your Opinion, What Is the Function of Strategies You Implement?”
- personal growth: inner and personal growth, finding oneself and one’s balance, and gaining deeper self-knowledge;
- working better: psychological serenity is reflected in the quality of work;
- improving relationships with oneself and others: establishing better connections with others, feeling a sense of belonging to a group, being in the right place, and feeling understood, non-judged, and supported by others;
- improving the quality of life: living better, feeling good, recalibrating priorities, achieving calm and tranquility, and relaxing. Self-care strategies have a liberating, regenerative, and nourishing function;
- managing and overcoming stress: controlling anxiety and stress, developing resilience, avoiding getting caught up in work, and centering oneself.
3.2.5. Fifth Question: “What Are the Factors (In Your Personal and Professional Life) That Facilitate Your Self-Care Practices?”
- individual factors: mental flexibility, reliance on oneself and one’s own strength, deriving gratification from one’s work;
- factors related to the work context: the organization facilitates the optimization of time at work;
- inter-individual factors related to private life: good social network that can motivate healthcare professionals;
- inter-individual factors of the team: support from the team, facing difficulties together, engaging in confrontation, and sharing.
3.2.6. Sixth Question: “Conversely, What Are the Factors That Hinder Your Self-Care Practices?”
- organizational factors related to the work context: excessive workload and demand for performance for the time available, busy work under pressure and consequent difficulties in doing the own job well, and unforeseen events such as changes in work shifts;
- time-related factors: inability to disconnect from work, lack of time to devote to oneself, abuse and lack of respect for other people’s time;
- factors related to the team’s climate: an uncomfortable working environment, misunderstandings, lack of affinity between colleagues, and lack of support from them;
- private life factors: problems, worries, unforeseen events, lack of serenity and stress, related to factors external to professional life, and difficulty in committing to and self-imposing the act of taking care of oneself.
3.2.7. Seventh Question: “Within Your Work Context, What Strategies, in Your Opinion, Can Improve Team Well-Being?”
- personal aspects: personality and personal resources of healthcare professionals, open, welcoming, and non-judgmental attitude, the ability, possibility, and willingness to undertake a personal path of knowledge, self-awareness within the team context;
- relational aspects: quality relationships between healthcare professionals, care for the group, communication, sharing and comparison and mutual collaboration, support, availability, and recognition among colleagues;
- working environment: positive working environment, availability of the institution in times of difficulties, training of healthcare professionals, supervision, formalized meetings, clarity in work, roles and meetings, common goals and the same enthusiasm in achieving them, as well as the idea of spreading palliative care as a culture.
3.2.8. Eighth Question: “Have You Ever Received Training in Self-Care Strategies During Your Professional Experience?”
3.2.9. Ninth Question: “In Your Opinion, Was It Useful to Take Part in This Project and Discuss Self-Care? In Which Way? If Not, Why?”
- improving work aspects and consolidating the group: discuss work aspects and problems, confront each other, make improvements, strengthen and bring the group closer together;
- sharing and listening: sharing one’s opinions with other participants and listening to those of others;
- learning to listen: listening to team members is important and useful for understanding their points of view and difficulties at work;
- reciprocal exchange: enriching the reciprocal exchange of opinions and self-care strategies implemented;
- freedom of expression: having the opportunity to freely express thoughts and opinions.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Use of Artificial Intelligence
Conflicts of Interest
References
- Eche, I.J.; Phillips, C.S.; Alcindor, N.; Mazzola, E. A Systematic Review and Meta-analytic Evaluation of Moral Distress in Oncology Nursing. Cancer Nurs. 2023, 46, 128–142. [Google Scholar] [CrossRef]
- Corradi-Perini, C.; Beltrão, J.R.; Ribeiro, U.R.V.C.O. Circumstances Related to Moral Distress in Palliative Care: An Integrative Review. Am. J. Hosp. Palliat. Care 2021, 38, 1391–1397. [Google Scholar] [CrossRef]
- Kohli, D.; Padmakumari, P. Self-Care, Burnout, and Compassion Fatigue in Oncology Professionals. Indian J. Occup. Environ. Med. 2020, 24, 168–171. [Google Scholar] [CrossRef] [PubMed]
- Alkema, K.; Linton, J.M.; Davies, R. A Study of the Relationship Between Self-care, Compassion Satisfaction, Compassion Fatigue, and Burnout Among Hospice Professionals. J. Soc. Work End Life Palliat. Care 2008, 4, 101–119. [Google Scholar] [CrossRef]
- Slocum-Gori, S.; Hemsworth, D.; Chan, W.W.; Carson, A.; Kazanjian, A. Understanding Compassion Satisfaction, Compassion Fatigue, and Burnout: A Survey of the Hospice Palliative Care Workforce. Palliat. Med. 2013, 27, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Urquiza, J.L.; Albendín-García, L.; Velando-Soriano, A.; Ortega-Campos, E.; Ramírez-Baena, L.; Membrive-Jiménez, M.J.; Suleiman-Martos, N. Burnout in Palliative Care Nurses, Prevalence and Risk Factors: A Systematic Review with Meta-Analysis. Int. J. Environ. Res. Public Health 2020, 17, 7672. [Google Scholar] [CrossRef] [PubMed]
- Dijxhoorn, A.Q.; Brom, L.; van der Linden, Y.M.; Leget, C.; Raijmakers, N.J. Prevalence of Burnout in Healthcare Professionals Providing Palliative Care and the Effect of Interventions to Reduce Symptoms: A Systematic Literature Review. Palliat. Med. 2021, 35, 6–26. [Google Scholar] [CrossRef]
- Fattori, A.; Pedruzzi, M.; Cantarella, C.; Bonzini, M. The Burden in Palliative Care Assistance: A Comparison of Psychosocial Risks and Burnout Between Inpatient Hospice and Home Care Services Workers. Palliat. Support Care 2023, 21, 49–56. [Google Scholar] [CrossRef]
- Copur, M.S. Burnout in Oncology. Oncology 2019, 33, 522–687. [Google Scholar]
- Commissione Psicologi SICP. Gli Interventi Psicologici a Sostegno Dell’équipe di Cure Palliative; Società Italiana di Cure Palliative: Milano, Italy, 2016. [Google Scholar]
- Klimecki, O.M.; Singer, T. Empathic Distress Fatigue Rather Than Compassion Fatigue? Integrating Findings from Empathy Research in Psychology and Social Neuroscience. In Pathological Altruism; Oakley, B., Knafo, A., Madhavan, G., Eds.; Oxford University Press: New York, NY, USA, 2012; pp. 368–383. [Google Scholar]
- World Health Organization (WHO). National Cancer Control Programmes. In Policies and Managerial Guidelines, 2nd ed.; WHO: Geneva, Switzerland, 2002. [Google Scholar]
- Hussain, F.A. Psychological Challenges for Nurses Working in Palliative Care and Recommendations for Self-Care. Br. J. Nurs. 2021, 30, 484–489. [Google Scholar] [CrossRef]
- Pennestrì, F.; Villa, G.; Giannetta, N.; Manara, F.D.; Sala, R.; Mordacci, R. Non C’è Cura Dei Pazienti Senza Cura Degli Operatori: Conoscere e Contrastare Moral Distress e Burnout Fra Prevenzione e Interventi Strutturali. Politiche Sanit. 2022, 23, 1–22. [Google Scholar]
- Fisher, S.; Gillanders, D.; Ferreira, N. The Experiences of Palliative Care Professionals and Their Responses to Work-related Stress: A Qualitative Study. Br. J. Health Psychol. 2022, 27, 605–622. [Google Scholar] [CrossRef]
- Mota Vargas, R.; Mahtani-Chugani, V.; Solano Pallero, M.; Rivero Jiménez, B.; Cabo Domínguez, R.; Robles Alonso, V. The Transformation Process for Palliative Care Professionals: The Metamorphosis, A Qualitative Research Study. Palliat. Med. 2016, 30, 161–170. [Google Scholar] [CrossRef] [PubMed]
- Orem, D.E. Nursing: Concepts of Practice, 3rd ed.; McGraw-Hill Book Company: New York, NY, USA, 1985. [Google Scholar]
- Butler, L.D.; Mercer, K.A.; McClain-Meeder, K.; Horne, D.M.; Dudley, M. Six Domains of Self-Care: Attending to the Whole Person. J. Hum. Behav. Soc. Environ. 2019, 29, 107–124. [Google Scholar] [CrossRef]
- Martínez, N.; Connelly, C.D.; Pérez, A.; Calero, P. Self-Care: A Concept Analysis. Int. J. Nurs. Sci. 2021, 8, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Bodenheimer, T.; Sinsky, C. From Triple to Quadruple Aim: Care of the Patient Requires Care of the Provider. Ann. Fam. Med. 2014, 12, 573–576. [Google Scholar] [CrossRef]
- Lluch-Sanz, C.; Galiana, L.; Tomás, J.M.; Oliver, A.; Vidal-Blanco, G.; Sansó, N. Using Latent Profile Analysis to Understand Palliative Care Professionals’ Quality of Life During the COVID-19 Pandemic. Curr. Psychol. 2023, 42, 28971–28983. [Google Scholar] [CrossRef]
- Cuartero-Castañer, M.E.; Hidalgo-Andrade, P.; Cañas-Lerma, A.J. Professional Quality of Life, Engagement, and Self-Care in Healthcare Professionals in Ecuador During the COVID-19 Pandemic. Healthcare 2021, 9, 515. [Google Scholar] [CrossRef]
- Mills, J.; Wand, T.; Fraser, J.A. Self-Care in Palliative Care Nursing and Medical Professionals: A Cross-Sectional Survey. J. Palliat. Med. 2017, 20, 625–630. [Google Scholar] [CrossRef]
- Mills, J.; Wand, T.; Fraser, J.A. Exploring the Meaning and Practice of Self-Care Among Palliative Care Nurses and Doctors: A Qualitative Study. BMC Palliat. Care 2018, 17, 63. [Google Scholar] [CrossRef]
- Galiana, L.; Oliver, A.; Sansó, N.; Benito, E. Validation of a New Instrument for Self-Care in Spanish Palliative Care Professionals Nationwide. Span. J. Psychol. 2015, 18, E67. [Google Scholar] [CrossRef] [PubMed]
- Sansó, N.; Galiana, L.; Oliver, A.; Pascual, A.; Sinclair, S.; Benito, E. Palliative Care Professionals’ Inner Life: Exploring the Relationships Among Awareness, Self-Care, and Compassion Satisfaction and Fatigue, Burnout, and Coping With Death. J. Pain Symptom Manage. 2015, 50, 200–207. [Google Scholar] [CrossRef]
- Mehrotra, S.; Tripathi, R.; Banu, H. Psychological Well-Being: Reflections on an Elusive Construct and Its Assessment. J. Indian Acad. Appl. Psychol. 2013, 39, 189–195. [Google Scholar]
- Kaur, A.; Sharma, M.P.; Chaturvedi, S.K. Psychological Well-Being Amongst Cancer Palliative Care Professionals Working in Bengaluru, India. Indian J. Palliat. Care 2022, 28, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Krueger, R.A.; Casey, M.A. Focus Groups: A Practical Guide for Applied Research, 3rd ed.; Sage Publications, Inc.: Thousand Oaks, CA, USA, 2000. [Google Scholar]
- Krueger, R.A.; Casey, M.A. Focus Group Interviewing. In Handbook of Practical Program Evaluation, 4th ed.; Newcomer, K.E., Hatry, H.P., Wholey, J.S., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2015; pp. 506–534. [Google Scholar]
- Andrews, H.; Tierney, S.; Seers, K. Needing permission: The experience of self-care and self-compassion in nursing: A constructivist grounded theory study. Int. J. Nurs. Stud. 2020, 101, 103436. [Google Scholar] [CrossRef] [PubMed]
- Graneheim, U.H.; Lindgren, B.M.; Lundman, B. Methodological challenges in qualitative content analysis: A discussion paper. Nurse Educ. Today 2017, 56, 29–34. [Google Scholar] [CrossRef]
- Gruppo Psicologi SICP. Documento di Consenso e Compendio: Appropriatezza dei Termini Psicologici e Relazionali in Cure Palliative; Società Italiana di Cure Palliative: Milano, Italy, 2016. [Google Scholar]
- Di Leo, S.; Serpentini, S. Supervisione. In Documento di Consenso e Compendio: Appropriatezza dei Termini Psicologici e Relazionali in Cure Palliative; Gruppo Psicologi SICP, Ed.; Società Italiana di Cure Palliative: Milano, Italy, 2016; pp. 28–30. [Google Scholar]
- Buonaccorso, L.; Tanzi, S.; Sacchi, S.; Alquati, S.; Bertocchi, E.; Autelitano, C.; Taberna, E.; Martucci, G. Self-Care as a Method to Cope With Suffering and Death: A Participatory Action-Research Aimed at Quality Improvement. Front. Psychol. 2022, 13, 769702. [Google Scholar] [CrossRef]
- Heeter, C.; Day, T.; Lehto, R.; Allbritton, M.; Wiseman, M. Effects of a Technology-Assisted Meditation Program on Healthcare Providers’ Interoceptive Awareness, Compassion Fatigue, and Burnout. J. Hosp. Palliat. Nurs. 2017, 19, 314–322. [Google Scholar] [CrossRef]
- Lehto, R.H.; Heeter, C.; Allbritton, M.; Wiseman, M. Hospice and Palliative Care Provider Experiences With Meditation Using Mobile Applications. Oncol. Nurs. Forum 2018, 45, 380–388. [Google Scholar] [CrossRef]
- Sansó, N.; Galiana, L.; Oliver, A.; Cuesta, P.; Sánchez, C.; Benito, E. Evaluación de una Intervención Mindfulness en Equipos de Cuidados Paliativos. Psychosoc. Interv. 2018, 27, 81–88. [Google Scholar] [CrossRef]
- Gerhart, J.; O’Mahony, S.; Abrams, I.; Grosse, J.; Greene, M.; Levy, M. A Pilot Test of a Mindfulness-Based Communication Training to Enhance Resilience in Palliative Care Professionals. J. Context. Behav. Sci. 2016, 5, 89–96. [Google Scholar] [CrossRef]
- Orellana-Rios, C.L.; Radbruch, L.; Kern, M.; Regel, Y.U.; Anton, A.; Sinclair, S.; Schmidt, S. Mindfulness and Compassion-Oriented Practices at Work Reduce Distress and Enhance Self-Care of Palliative Care Teams: A Mixed-Method Evaluation of an “On the Job” Program. BMC Palliat. Care 2018, 17, 3, Erratum in: BMC Palliat. Care 2017, 16, 51. [Google Scholar] [CrossRef]
- Lautwein, F.; Schallenburger, M.; Scherg, A.; Schlieper, D.; Karger, A.; Regel, Y.U.; Schwartz, J.; Neukirchen, M. Mindfulness and Compassion Training on Daily Work with Patients and within the Multiprofessional Palliative Care Team: A Retrospective Self-Assessment Study. BMC Palliat. Care 2023, 22, 37. [Google Scholar] [CrossRef]
- Ho, A.H.Y.; Tan-Ho, G.; Ngo, T.A.; Ong, G.; Chong, P.H.; Dignadice, D.; Potash, J. A Novel Mindful-Compassion Art-Based Therapy for Reducing Burnout and Promoting Resilience Among Healthcare Workers: Findings From a Waitlist Randomized Control Trial. Front. Psychol. 2021, 12, 744443. [Google Scholar] [CrossRef] [PubMed]
- Arantzamendi, M.; Sapeta, P.; Collette, N.; Sesma, A.B.; Pérez-Solero, M.T.T.; Echarri, F.I.; Centeno, C. Insight and Inner Peace in Palliative Care Professionals after an Art Therapy Workshop Focused on Personal Self-Care: A Preliminary Experience. Palliat. Med. Rep. 2021, 2, 34–39. [Google Scholar] [CrossRef]
- Essary, A.C.; Lussier, M.; Stone, N.; Volk-Craft, B.; Hamilton, G. Reflections on the Integration of a Narrative Medicine and Mindfulness Program in Hospice and Palliative Care. Prog. Palliat. Care 2020, 28, 260–266. [Google Scholar] [CrossRef]
- Cosentino, C.; D’apice, C.; Del Gaudio, M.; Bertoletti, C.; Bini, M.; Liotti, M.C.; Melli, E.; Tesa, F.; Sarli, L.; Artioli, G. Effectiveness of Expressive Writing Protocol in Palliative Care Healthworkers: A Quantitative Study. Acta Biomed. 2021, 92, e2021010. [Google Scholar]
- Popa-Velea, O.; Trutescu, C.I.; Diaconescu, L.V. The Impact of Balint Work on Alexithymia, Perceived Stress, Perceived Social Support, and Burnout Among Physicians Working in Palliative Care: A Longitudinal Study. Int. J. Occup. Med. Environ. Health 2019, 32, 53–63. [Google Scholar] [CrossRef]

{kind=link}
| What self-care strategies do you implement most frequently? |
| Which ones do you consider most effective? Why? |
| What does taking care of yourself mean to you? |
| In your opinion, what is the function of strategies you implement? |
| What are the factors (in your personal and professional life) that facilitate your self-care practices? |
| Conversely, what are the factors that hinder your self-care practices? |
| Within your work context, what strategies, in your opinion, can improve team well-being? |
| Have you ever received training in self-care strategies during your professional experience? |
| In your opinion, was it useful to take part in this project and discuss self-care? In which way? If not, why? |
| Categories | Frequency | Percentage (%) | Mean | SD | |
|---|---|---|---|---|---|
| Sex | Male | 9 | 25 | ||
| Female | 27 | 75 | |||
| Age | 20–29 | 5 | 13.87 | 47.08 | 12.08 |
| 30–39 | 4 | 11.11 | |||
| 40–49 | 10 | 27.78 | |||
| 50–59 | 11 | 30.56 | |||
| 60–69 | 6 | 16.67 | |||
| Workplace | Hospital | 11 | 30.56 | ||
| Hospice | 25 | 69.44 | |||
| Profession | Nursing assistant | 10 | 27.78 | ||
| Nurse | 13 | 36.11 | |||
| Coordinator nurse | 2 | 5.56 | |||
| University nursing student | 1 | 2.78 | |||
| Physician | 6 | 16.67 | |||
| Psychologist | 3 | 8.33 | |||
| Spiritual assistant | 1 | 2.78 | |||
| Working experience in palliative care (years) | 0–2 | 14 | 38.89 | 8.98 | 8.02 |
| 3–5 | 10 | 27.78 | |||
| 6–10 | 1 | 2.78 | |||
| 11–15 | 5 | 13.89 | |||
| 16–20 | 3 | 8.33 | |||
| 21–25 | 2 | 5.56 | |||
| >26 | 1 | 2.78 |
| Questions | Emerging Themes | Examples |
|---|---|---|
| Most frequently implemented self-care strategies | Lifestyle strategies | “[…] care of the organic and physical aspects.”—P1 |
| Emotional coping strategies | “[…] even just being with yourself in silence. […] it helps me to be alone with myself, in silence.”—P2 | |
| Meaningful private life relationships | “[…] being with the people who make me feel good […]”—P3 | |
| Taking care of others | “[…] I like to take care of the people I care about.”—P4 | |
| Psychological interventions (individual, group, work) | “[…] the contribution of the psychotherapist with whom I have had a connection for years.”—P5 “[Regarding the psychodrama supervision meetings] […] they represented […] a port where one landed and then departed […]”—P6 | |
| Discussion and sharing in teams | “[…] be able to talk to your colleague about how you’ve felt. […] it happens here a lot […]”—P7 | |
| Spiritual practices | “[…] prayer […] and the care of spirituality […] helps me to be more centered and balanced.”—P8 | |
| Physical activity | “[…] moving my body […] to take care also of the emotional aspects, […] psyche and body are a unity”—P1 | |
| Personal hobbies and passions | “I like to read poetry, […] cropping photos, […] doing handicrafts […] my little space that I take for myself.”—P4 | |
| Contact with nature | “[…] going to the mountains […] to […] switch off and look at things from another point of view.”—P9 | |
| Self-care strategies considered most effective | Lifestyle strategies | “[…] regularity […] in both nutrition and sleep […]”—P3 |
| Emotional coping strategies | “[…] find a time of isolation in which I stay at home […] and I create an environment… a nest […] this thing […] isolates me from everything else and allows me to decant.”—P10 | |
| Meaningful private life relationships | “[…] spending also time with family and friends.”—P2 | |
| Discussion and sharing in teams | “[…] the beautiful thing […] that I observe in this group, is that there is a taking care of each other.”—P11 | |
| Spiritual practices | “[…] what helps me the most […] is definitely prayer. […] without that I would have a much harder time finding a personal balance […]”—P8 | |
| Physical activities | “[…] I cycle without noticing where I am, […] it helps me a lot. It frees me.”—P12 | |
| Personal hobbies and passions | “[Regarding traveling and new experiences] […] it helps me to detach myself and […] to distance myself […] to rework and see things from another perspective, but above all, to slow down and stop.”—P3 | |
| Contact with nature | “[…] I try […] to go to my little garden, […] where I have planted all my plants […] I am content with that time that I take. […] in front of you there is the mountain, there is the meadow […] for the way I am, that is the best […]”—P4 | |
| Meaning of self-care | Self-awareness and self-knowledge | “[…] to enter deeper into oneself, to learn to know oneself deeply for what one is […] [know] just a little more […] of one’s soul […] of one’s heart, of one’s mind […]”—P8 |
| Connecting with one’s emotions | “Listen to my gut and make it say, because that’s the way it is, that it’s fine at that moment, regardless of what rationality would say […]”—P10 | |
| Seeking work–life balance | “[…] we always try not to bring the work home and not to bring the home to the work […]”—P13 | |
| Taking time for oneself | “In my opinion, caring is being able to stop, for a moment, to make a moment of emptiness and to get rid of all the thoughts that are circulating. […] be able to stop.”—P14 | |
| Function of self-care strategies implemented | Personal growth | “[…] as a term […] of knowledge, of personal deepening and certainly of growth […]”—P8 |
| Working better | “If you can take care of yourself, you can, of course, be calm and work better and better. That is, if we are mentally calm, surely we do our job better.”—P15 | |
| Improving relationship with oneself and others | “It’s making me feel like I’m in the right place at the right time.”—P16 “[…] being able to relate better to people. It is not only a personal, intimate thing, which is certainly there, but this is a reflection and allows you to feel better with others as well.”—P8 | |
| Improving the quality of life | “[Self-care strategies] […] are liberating […] regenerative, nourishing […]”—P5 | |
| Managing and overcoming stress | “[…] calm anxiety and stress […]”—P4 “[…] enhance your private life, not get absorbed in a very demanding job […]”—P17 | |
| Factors facilitating self-care | Individual factors | “The flexibility training you have in doing this job helps you a lot in your private life as well.”—P17 |
| Factors related to the work context | “[The organization] […] allows you to […] move from one thing to another with a bit of logic without wasting time and managing to work with adequate time […]”—P8 | |
| Inter-individual factors related to private life | “[…] also a good […] social network around. Something that pushes you to do […]”—P18 | |
| Inter-individual factors of the team | “If there are difficulties, we face them together […]”—P19 | |
| Factors hindering self-care | Organizational factors related to the work context | “[…] the list of things to do quickly, the demand for performance […]”—P6 |
| Time-related factors | “[…] the whole day is so busy with work […] and sometimes you have little time to implement strategies […]”—P1 | |
| Factors related to the team’s climate | “Not being able to understand each other, not being able to work together at that moment there.”—P13 | |
| Private life factors | “[…] when I’m so […] polluted by external problems […] I’m drained, and I can’t take care of my patients.”—P7 “[…] it’s a much harder task than it sounds: the difficulty of self-obliging yourself to take care of yourself.”—P20 | |
| Self-care strategies for the well-being of the team | Personal aspects | “[…] the awareness of the person within a context and how this awareness can guide the person in his or her own self-care practices […]”—P5 “[…] an attitude of openness and, if possible, non-judgment.”—P11 |
| Relational aspects | “[…] we try to meet each other, […] there is a lot of attention among us operators.”—P4 “[…] make me available […] and know that this availability, in some way, is accepted and valued […]”—P21 | |
| Working environment | “[…] clarity in work, […] in the roles, […] in the order of the meeting […]”—P5 “[…] supervision, meetings between operators, meetings.”—P22 “[…] having a common, shared goal and the same enthusiasm in wanting to achieve it […]”—P10 | |
| Professional training on self-care | No | |
| Yes | “At the university there is a course called “Helping Relationship” […] we talk to the psychologist […] about what we experienced during the training, […] how to deal with certain situations.”—P23 | |
| Perception of usefulness of participation in the project | Improving the work aspects and consolidating the group | “[…] it also brings the operators very close […]”—P24 “This is the only way […] to confront and continue to cement the group […] there is always a need for small precautions […]”—P9 |
| Sharing and listening | “[…] sharing is very important […]”—P7 | |
| Learning to listen | “It also makes us understand […] the difficulties that [the colleague] experiences in the workplace […]”—P24 | |
| Reciprocal exchange | “[…] it also makes us understand what kind of strategies he [regarding the other healthcare professionals] uses and… strategies that maybe […] then we could also make our own.”—P24 | |
| Freedom of expression | “[…] each of us was free to say what we wanted […]”—P17 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bovero, A.; Spada, M.F.; Cito, A.L.; Pidinchedda, A.V.; Tosi, C.; Carletto, S. Self-Care in Palliative Healthcare Professionals: A Qualitative Study. Nurs. Rep. 2025, 15, 139. https://doi.org/10.3390/nursrep15050139
Bovero A, Spada MF, Cito AL, Pidinchedda AV, Tosi C, Carletto S. Self-Care in Palliative Healthcare Professionals: A Qualitative Study. Nursing Reports. 2025; 15(5):139. https://doi.org/10.3390/nursrep15050139
Chicago/Turabian StyleBovero, Andrea, Maria Federica Spada, Alessandra Loreta Cito, Alexa Victoria Pidinchedda, Chiara Tosi, and Sara Carletto. 2025. "Self-Care in Palliative Healthcare Professionals: A Qualitative Study" Nursing Reports 15, no. 5: 139. https://doi.org/10.3390/nursrep15050139
APA StyleBovero, A., Spada, M. F., Cito, A. L., Pidinchedda, A. V., Tosi, C., & Carletto, S. (2025). Self-Care in Palliative Healthcare Professionals: A Qualitative Study. Nursing Reports, 15(5), 139. https://doi.org/10.3390/nursrep15050139