
Development and Validation of a Game for Older Adults on Lifestyles and Frailty

 ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
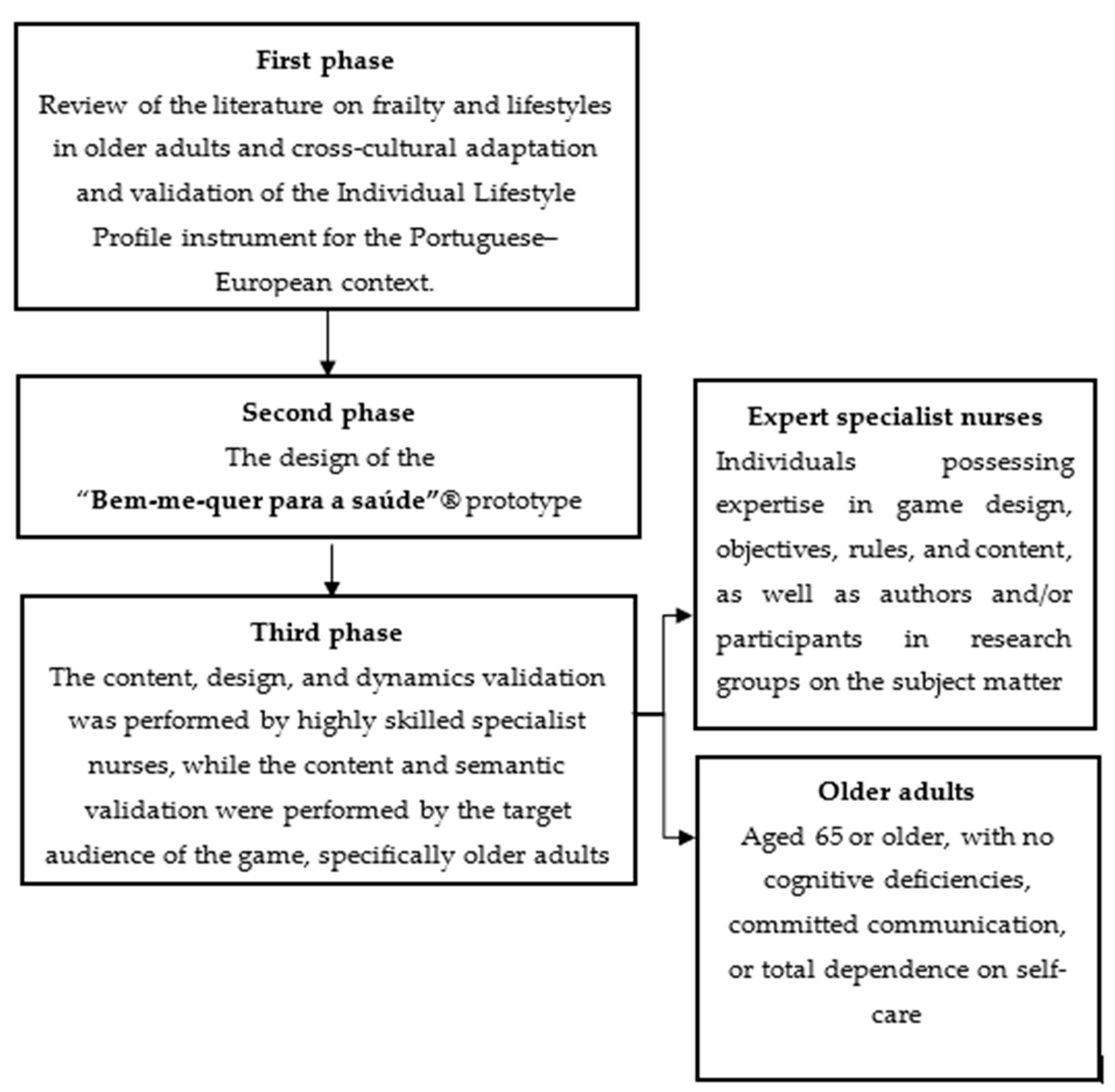
2.1. Study Design
2.2. Participants and Data Collection
2.3. Instruments
2.4. Data Analysis
2.5. Ethical Considerations
3. Results
3.1. Validation of the Game’s Content with the Experts
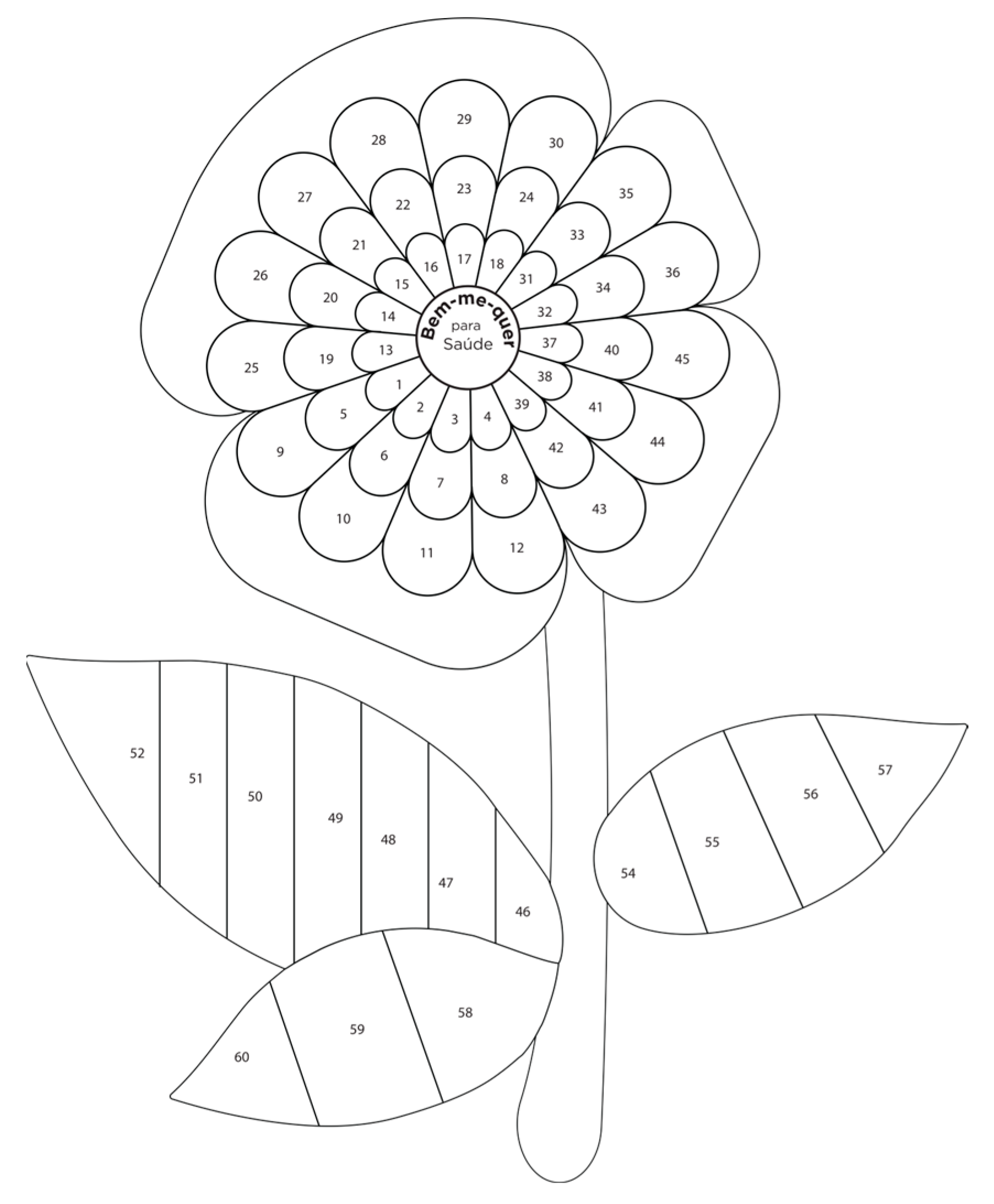
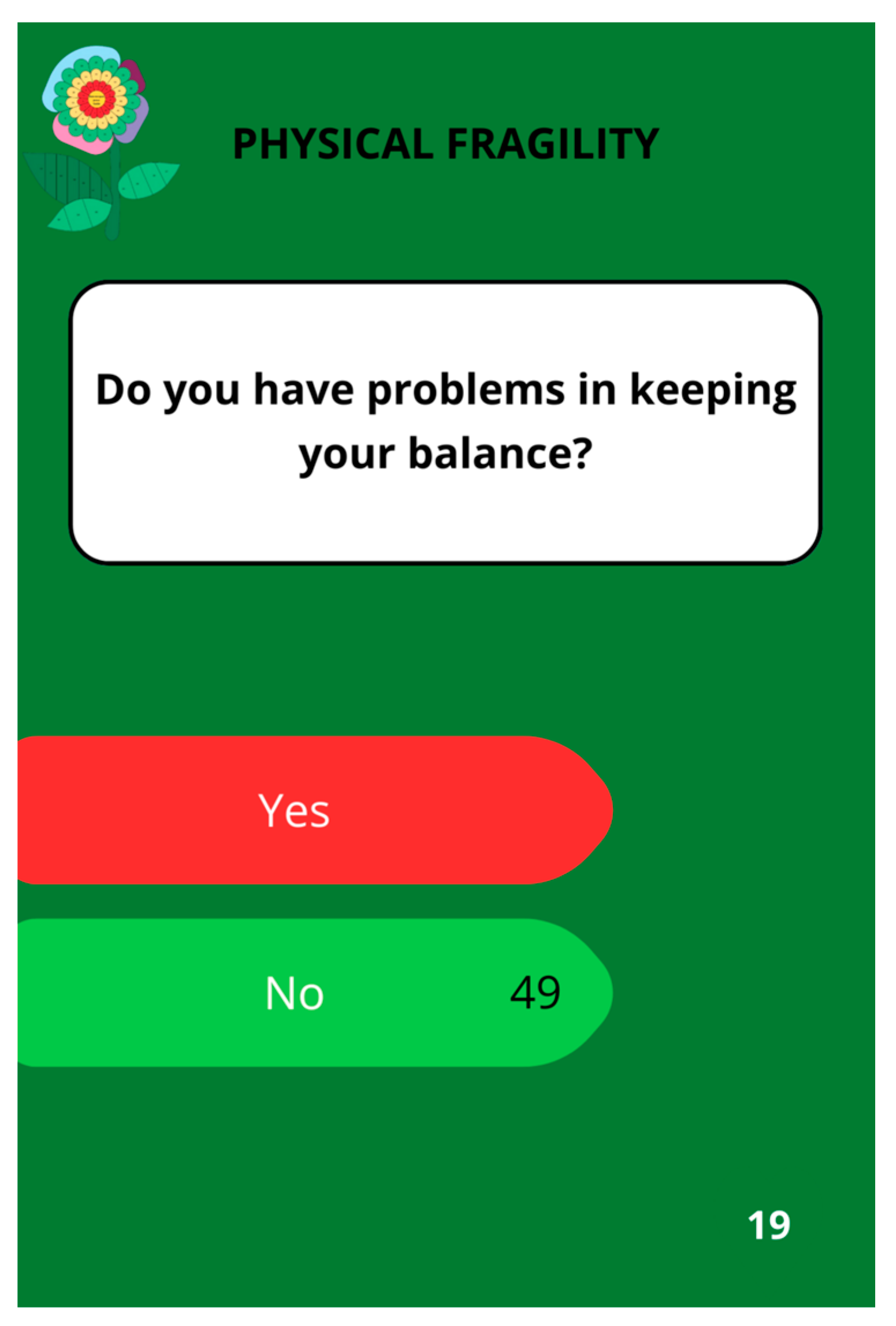
3.2. Game Prototype
3.3. Application and Validation of Game Content with Older Adults
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Use of Artificial Intelligence
Acknowledgments
Conflicts of Interest
References
- Keating, N. A research framework for the United Nations Decade of Healthy Aging (2021–2030). Eur. J. Aging 2022, 19, 775–787. [Google Scholar] [CrossRef] [PubMed]
- Torregrosa-Ruiz, M.; Gutiérrez, M.; Alberola, S.; Tomás, J.M. A Successful Aging Model Based on Personal Resources, Self-Care, and Life Satisfaction. J. Psychol. 2021, 155, 606–623. [Google Scholar] [CrossRef] [PubMed]
- Plácido, A.I.; Herdeiro, M.T.; Roque, F. Health and Wellbeing in Aging. Int. J. Environ. Res. Public Health 2022, 19, 8835. [Google Scholar] [CrossRef]
- Costa, A.; Henriques, J.; Alarcão, V.; Henriques, A.; Madeira, T.; Virgolino, A.; Sousa, J.; Feteira-Santos, R.; Arriaga, M.; Rocha, J.; et al. Active aging awareness and well-being among older adults in Portugal. Front. Public Health 2023, 11, 1149731. [Google Scholar] [CrossRef]
- Kwak, D.; Thompson, L.V. Frailty: Past, present, and future? Sports Med. Health Sci. 2021, 3, 5. [Google Scholar] [CrossRef]
- Gobbens, R.J.J.; van der Ploeg, T. The Prediction of Quality of Life by Frailty and Disability among Dutch Community-Dwelling People Aged 75 Years or Older. Healthcare 2024, 12, 874. [Google Scholar] [CrossRef]
- Gobbens, R.J.; Luijkx, K.G.; Wijnen-Sponselee, M.T.; Schols, J.M. Toward a conceptual definition of frail community dwelling older people. Nurs. Outlook 2010, 58, 76–86. [Google Scholar] [CrossRef]
- Gobbens, R.J.; Santiago, L.M.; Uchmanowicz, I.; van der Ploeg, T. Predicting Disability Using a Nomogram of the Tilburg Frailty Indicator (TFI). Healthcare 2023, 11, 1150. [Google Scholar] [CrossRef]
- Gobbens, R.J.; Vermeiren, S.; Van Hoof, A.; van der Ploeg, T. Nurses’ Opinions on Frailty. Healthcare 2022, 10, 1632. [Google Scholar] [CrossRef]
- Santamaría-Ulloa, C.; Lehning, A.J.; Cortés-Ortiz, M.V.; Méndez-Chacón, E. Frailty as a predictor of mortality: A comparative cohort study of older adults in Costa Rica and the United States. BMC Public Health 2023, 23, 1960. [Google Scholar] [CrossRef]
- de Breij, S.; Rijnhart, J.J.M.; Schuster, N.A.; Rietman, M.L.; Peters, M.J.L.; Hoogendijk, E.O. Explaining the association between frailty and mortality in older adults: The mediating role of lifestyle, social, psychological, cognitive, and physical factors. Prev. Med. Rep. 2021, 24, 101589. [Google Scholar] [CrossRef] [PubMed]
- Gobbens, R.J.J.; van der Ploeg, T. The Development of Multidimensional Frailty Over Seven Years A longitudinal study among Dutch community-dwelling older people using the Tilburg Frailty Indicator. Arch. Gerontol. Geriatr. 2021, 95, 104393. [Google Scholar] [CrossRef] [PubMed]
- Travers, J.; Romero-Ortuno, R.; Langan, J.; MacNamara, F.; McCormack, D.; McDermott, C.; McEntire, J.; McKiernan, J.; Lacey, S.; Doran, P.; et al. Building resilience and reversing frailty: A randomised controlled trial of a primary care intervention for older adults. Age Aging 2023, 52, afad012. [Google Scholar] [CrossRef]
- Travers, J.; Romero-Ortuno, R.; Bailey, J.; Cooney, M.-T. Delaying and reversing frailty: A systematic review of primary care interventions. Br. J. Gen. Pract. J. R. Coll. Gen. Pract. 2019, 69, e61–e69. [Google Scholar] [CrossRef]
- Bailey, J.; Travers, J.; Romero-Ortuno, R.; Cooney, T. 138The Multiplicity of Frailty Screening Tools in Primary-Care: A Review and New Alternative. Age Aging 2018, 47 (Suppl. S5), v13–v60. [Google Scholar] [CrossRef]
- Archibald, M.M.; Lawless, M.T.; Ambagtsheer, R.C.; Kitson, A.L. Understanding consumer perceptions of frailty screening to inform knowledge translation and health service improvements. Age Aging 2001, 50, 227–232. [Google Scholar] [CrossRef]
- Schoenborn, N.L.; Van Pilsum Rasmussen, S.E.; Xue, Q.L.; Walston, J.D.; McAdams-Demarco, M.A.; Segev, D.L.; Boyd, C.M. Older adults’ perceptions and informational needs regarding frailty. BMC Geriatr. 2018, 18, 46. [Google Scholar] [CrossRef]
- Archibald, M.; Lawless, M.; Ambagtsheer, R.C.; Kitson, A. Older adults’ understandings and perspectives on frailty in community and residential aged care: An interpretive description. BMJ Open 2020, 10, e035339. [Google Scholar] [CrossRef]
- van Assen, M.A.L.M.; Helmink, J.H.M.; Gobbens, R.J.J. Associations between lifestyle factors and multidimensional frailty: A cross-sectional study among community-dwelling older people. BMC Geriatr. 2022, 22, 7. [Google Scholar] [CrossRef]
- Haapanen, M.J.; Mikkola, T.M.; Jylhävä, J.; Wasenius, N.S.; Kajantie, E.; Eriksson, J.G.; von Bonsdorff, M.B. Lifestyle-related factors in late midlife as predictors of frailty from late midlife into old age: A longitudinal birth cohort study. Age and Aging. 2024, 53, afae066. [Google Scholar] [CrossRef]
- Rodrigues, A.M.; Gregório, M.J.; Sousa, R.D.; Dias, S.S.; Santos, M.J.; Mendes, J.M.; Coelho, P.S.; Branco, J.C.; Canhão, H. Challenges of Ageing in Portugal: Data from the EpiDoC Cohort. Acta Médica Port. 2018, 31, 80–93. [Google Scholar] [CrossRef] [PubMed]
- Spiteri, K.; Broom, D.; Bekhet, A.H.; de Caro, J.X.; Laventure, B.; Grafton, K. Barriers and Motivators of Physical Activity Participation in Middle-aged and Older-adults—A Systematic Review. J. Aging Phys. Act. 2019, 27, 929–944. [Google Scholar] [CrossRef] [PubMed]
- Faria, A.D.C.A.; Martins, M.M.F.P.S.; Ribeiro, O.M.P.L.; Ventura-Silva, J.M.A.; Fonseca, E.F.; Ferreira, L.J.M.; Teles, P.J.F.C.; Laredo-Aguilera, J.A. Multidimensional Frailty and Lifestyles of Community-Dwelling Older Portuguese Adults. Int. J. Environ. Res. Public Health 2022, 19, 14723. [Google Scholar] [CrossRef]
- Robinson, S.M.; Jameson, K.A.; Syddall, H.E.; Dennison, E.M.; Cooper, C.; Aihie Sayer, A. Hertfordshire Cohort Study Group. Clustering of lifestyle risk factors and poor physical function in older adults: The Hertfordshire cohort study. J. Am. Geriatr. Soc. 2013, 61, 1684–1691. [Google Scholar] [CrossRef]
- Schwarzer, R. Health Action Process Approach (HAPA) as a Theoretical Framework to Understand Behavior Change. Actual. En. Psicol. 2016, 30, 119–130. [Google Scholar] [CrossRef]
- Pender, N.; Murdaugh, C.; Parsons, M. Health Promotion in Nursing Practice, 8th ed.; Pearson: London, UK; Prentice-Hall: Upper Saddle River, NJ, USA, 2019. [Google Scholar]
- Koivisto, J.; Malik, A. Gamification for Older Adults: A Systematic Literature Review. Gerontol. 2021, 61, e360–e372. [Google Scholar] [CrossRef]
- Gauthier, A.; Kato, P.M.; Bul, K.C.M.; Dunwell, I.; Walker-Clarke, A.; Lameras, P. Board Games for Health: A Systematic Literature Review and Meta-Analysis. Games Health J. 2019, 8, 85–100. [Google Scholar] [CrossRef]
- Deater-Deckard, K.; Chang, M.; Evans, M.E. Engagement states and learning from educational games. New Dir. Child. Adolesc. Dev. 2013, 2013, 21–30. [Google Scholar] [CrossRef]
- Dichev, C.; Dicheva, D. Gamifying education: What is known, what is believed and what remains uncertain: A critical review. Int. J. Educ. Technol. High. Educ. 2017, 14, 9. [Google Scholar] [CrossRef]
- Salazar-Cardona, J.; Gutiérrez Vela, F.L.; Arango-Lopez, J.; Moreira, F. Older adults’ motivations in game based systems: Heuristic definition and its connection with fun. Comput. Hum. Behav. Rep. 2023, 11, 100304. [Google Scholar] [CrossRef]
- Gordo, S.; Pocinho, R.; Marinho, R.; Rosa, M. Board game for the upper limbs rehabilitation in institutionalised elderly from Portugal: A quasi- experimental pilot study. J. Physiother. Res. 2021, 11, 657–670. [Google Scholar] [CrossRef]
- Sardone, N.B.; Devlin-Scherer, R. Let the (Board) Games Begin: Creative Ways to Enhance Teaching and Learning. Clear. House A J. Educ. Strateg. Issues Ideas 2016, 89, 215–222. [Google Scholar] [CrossRef]
- DeSmet, A.; Van Ryckeghem, D.; Compernolle, S.; Baranowski, T.; Thompson, D.; Crombez, G.; Poels, K.; Van Lippevelde, W.; Bastiaensens, S.; Van Cleemput, K.; et al. A meta-analysis of serious digital games for healthy lifestyle promotion. Prev. Med. 2014, 69, 95–107. [Google Scholar] [CrossRef] [PubMed]
- Buckinx, F.; Bruyère, O.; Lengelé, L.; Reginster, J.-Y.; Marchal, Q.; Hurtrez, P.; Mouton, A. The effects of GAMotion (a giant exercising board game) on physical capacity, motivation and quality of life among nursing home residents: A pilot interventional study. Exp. Gerontol. 2020, 138, 110983. [Google Scholar] [CrossRef]
- Nakao, M. Special series on “effects of board games on health education and promotion” board games as a promising tool for health promotion: A review of recent literature. Biopsychosoc. Med. 2019, 13, 5. [Google Scholar] [CrossRef]
- Ching-Teng, Y. Effect of board game activities on cognitive function improvement among older adults in adult day care centers. Soc. Work. Health Care 2019, 58, 825–838. [Google Scholar] [CrossRef]
- Ammar, M.; Amjad, I.; Nisar, M.; Ghoneim, O.S. Effects of board games on balance in association with cognition in communi-ty-dwelling older adults. J. Musculoskelet. Surg. Res. 2024, 8, 256–263. [Google Scholar] [CrossRef]
- Noda, S.; Shirotsuki, K.; Nakao, M. The effectiveness of intervention with board games: A systematic review. Biopsychosoc. Med. 2019, 13, 22. [Google Scholar] [CrossRef]
- Kuo, C.-Y.; Huang, Y.-M.; Yeh, Y.-Y. Let’s Play Cards: Multi-Component Cognitive Training with Social Engagement Enhances Executive Control in Older Adults. Front. Psychol. 2018, 9, 2482. [Google Scholar] [CrossRef]
- Rosa, M.; Lopes, S.; Silva, E.; Martins, N. El juego analógico como sistema de optimización en la evaluación de tareas duales en personas equilibradas—Un estudio exploratorio (The Analog Game as an Optimization System in the Evaluation of Dual Task Performance in Elderly People—An Exploratory Study). Retos 2024, 51, 856–863. [Google Scholar] [CrossRef]
- Epstein, D.S.; Zemski, A.; Enticott, J.; Barton, C. Tabletop Board Game Elements and Gamification Interventions for Health Behavior Change: Realist Review and Proposal of a Game Design Framework. JMIR Serious Games 2021, 9, e23302. [Google Scholar] [CrossRef]
- Medeiros, R.K.S.; Ferreira, M.A.; Júnior, M.A.F.; Pinto, D.P.S.R.; Vitor, A.F.; Santos, V.E.P.; Barichello, E. Pasquali’s model of content validation in Nursing research. Rev. Enf. Ref. 2015, IV, 127–135. [Google Scholar] [CrossRef]
- Alves Faria, A.D.; Martins, M.M.; Ribeiro, O.M.; Ventura-Silva, J.M.; Teles, P.J.; Laredo-Aguilera, J.A. Adaptation and Validation of the Individual Lifestyle Profile Scale of Portuguese Older Adults Living at Home. Int. J. Environ. Res. Public Health 2022, 19, 5435. [Google Scholar] [CrossRef] [PubMed]
- Coelho, T.; Santos, R.; Paúl, C.; Gobbens, R.J.; Fernandes, L. Portuguese version of the Tilburg Frailty Indicator: Transcultural adaptation and psychometric validation. Geriatr. Gerontol. Int. 2015, 15, 951–960. [Google Scholar] [CrossRef]
- Niederberger, M.; Spranger, J. Delphi Technique in Health Sciences: A Map. Front. Public Health 2020, 8, 457. [Google Scholar] [CrossRef]
- Fernandes, C.S.; Magalhães, B.M.B.d.S. A reflection on the use of the delphi technique in nursing. Texto Contexto Enferm. 2024, 33, e20230227. [Google Scholar] [CrossRef]
- Jünger, S.; Payne, S.A.; Brine, J.; Radbruch, L.; Brearley, S.G. Guidance on Conducting and REporting DElphi Studies (CREDES) in Palliative Care: Recommendations Based on a Methodological Systematic Review. Palliat. Med. 2017, 31, 684–706. [Google Scholar] [CrossRef]
- Yusoff, M.S. ABC of content validation and content validity index calculation. Educ. Med. J. 2019, 11, 49–54. [Google Scholar] [CrossRef]
- Martins, A.I.; Rosa, A.F.; Queirós, A.; Silva, A.; Rocha, N.P. European Portuguese validation of the System Usability Scale (SUS). Procedia Comput. Sci. 2015, 67, 293–300. [Google Scholar] [CrossRef]
- Brooke, J. SUS: A ‘Quick and Dirty’ Usability Scale. In Usability Evaluation in Industry; Jordan Patrick, W., Thomas, B., Weerdmeester, B.A., McClelland, I.L., Eds.; Taylor & Francis: London, UK, 1996; pp. 189–194. [Google Scholar]
- Lewis, J.R.; Sauro, J. Item benchmarks for the system usability scale. J. Usabil. Stud. 2018, 13, 158–167. Available online: https://dl.acm.org/doi/10.5555/3294033.3294037#core-cited-by (accessed on 10 July 2024).
- Bardin, L. Content Analysis; Edições 70: São Paulo, Brazil, 2011. [Google Scholar]
- World Health Organization. Tackling Abuse of Older People: Five Priorities for the United Nations Decade of Healthy Aging (2021–2030). Available online: https://iris.who.int/bitstream/handle/10665/356151/9789240052550-eng.pdf?sequence=1 (accessed on 2 June 2024).
- Cano, A.; Dargent, G.; Carriazo, A.; López-Samaniego, L.; Apostolo, J.; Campos, E.; Holland, C.; Varela-Nieto, I.; Luz Sánchez-Sánchez, M.; Illario, M.; et al. Tackling frailty and functional decline: Background of the action group A3 of the European innovation partnership for active and healthy aging. Maturitas 2018, 115, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Shell, J. The Art of Game Design: A Book of Lenses; Morgan Kaufmann: Burlington, MA, USA, 2008; ISBN 978-0-12-369496. [Google Scholar]
- Romero Naranjo, F.J.; Andreu-Cabrera, E. Neuromotricidad como recurso interdisciplinar. Justificación teórico-práctica a través del método BAPNE (Neuromotricity As an Interdisciplinary Resource. Theoretical-Practical Justification through the BAPNE Method). Retos 2023, 49, 350–364. [Google Scholar] [CrossRef]
- Cassiano, A.d.N.; Silva, C.J.D.A.; Nogueira, I.L.A.; Elias, T.M.N.; Teixeira, E.; Menezes, R.M.P.D. Validation of educational technologies: Bibliometric study in nursing theses and dissertations. Rev. de Enferm. do Centro-Oeste Min. 2020, 10, 3900. [Google Scholar] [CrossRef]
- de Sant’anna, R.M.; Camacho, A.C.L.F.; de Souza, V.M.F.; de Menezes, H.F.; Silva, R.P. Tecnologias educacionais no cuidado à pacientes com doenças cardiovasculares. Rev. Recien Rev. Científica De. Enferm. 2022, 12, 163–175. [Google Scholar] [CrossRef]
- White, B.K.; Martin, A.; White, J. Gamification and older adults: Opportunities for gamification to support health promotion initiatives for older adults in the context of COVID-19. Lancet Reg. Health West. Pac. 2023, 35, 100528. [Google Scholar] [CrossRef]
- Silva, C.R.D.T.; Felipe, S.G.B.; Carvalho, K.M.; Gouveia, M.T.O.; Silva, F.L., Jr.; Figueiredo, M.L.F. Construction and validation of an educational gerontotechnology on frailty in elderly people. Rev. Bras. Enferm. 2020, 73 (Suppl. S3), e20200800. [Google Scholar] [CrossRef]
- Orfanou, K.; Tselios, N.; Katsanos, C. Perceived usability evaluation of learning management systems: Empirical evaluation of the System Usability Scale. Int. Rev. Res. Open Distrib. Learn. 2015, 16, 227–246. [Google Scholar] [CrossRef]
- Vlachogianni, P.; Tselios, N. The relationship between perceived usability, personality traits and learning gain in an e-learning context. Int. J. Inf. Learn. Technol. 2022, 39, 70–81. [Google Scholar] [CrossRef]
- Vlachogianni, P.; Tselios, N. Perceived usability evaluation of educational technology using the System Usability Scale (SUS): A systematic review. J. Res. Technol. Educ. 2021, 54, 392–409. [Google Scholar] [CrossRef]
- Aiyegbusi, O.L. Key methodological considerations for usability testing of electronic patient-reported outcome (ePRO) systems. Qual. Life Res. 2020, 29, 325–333. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T. Generalization in quantitative and qualitative research: Myths and strategies. Int. J. Nurs. Stud. 2010, 47, 1451–1458. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Description | CVI |
|---|---|
| Purposes, goals, or ends to be reached with the game | 1 |
| Theoretical significance | 1 |
| Practical relevance | 1 |
| Design (attractiveness, choice of colors for the board game with a puzzle board and cards) | 0.93 |
| Clarity of information (general organization, structure, coherence, presentation, formatting, and size of game pieces) | 0.93 |
| Clarity (linguistic characteristics, understanding and style of the game’s writing, and its scientific accuracy) | 0.857 |
| Easy for community nurses to use for older adult health education | 1 |
| Promoting awareness and behavior change | 1 |
| TOTAL GAME CVI | 0.964 |
| Dimensions | Items | Minimum | Maximum | Mean | Standard Deviation |
|---|---|---|---|---|---|
| Usability | Q1. I would like to use this game often | 2 | 5 | 3.54 | 0.65 |
| Q2. I found the game more complex than necessary | 1 | 4 | 1.81 | 0.76 | |
| Q3. The game was easy to use | 2 | 5 | 4.21 | 0.72 | |
| Q5. I felt that the various functionalities of this game were well integrated | 2 | 5 | 3.88 | 0.81 | |
| Q6. I thought this game had a lot of inconsistencies | 1 | 3 | 1.64 | 0.58 | |
| Q7. I suppose most people would learn to use this game quickly | 4 | 5 | 4.50 | 0.54 | |
| Q8. I found the game very complicated to use | 1 | 3 | 1.56 | 0.65 | |
| Q9. I felt very confident when using the game | 3 | 5 | 4.25 | 0.62 | |
| Learning | Q4. I think I would need the help of a professional to be able to use this game | 1 | 4 | 1.19 | 0.92 |
| Q10. I had to learn a lot before I could handle this game | 1 | 4 | 1.14 | 0.93 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faria, A.d.C.A.; Martins, M.M.; Laredo-Aguilera, J.A.; Ventura-Silva, J.M.A.; Ribeiro, O.M.P.L. Development and Validation of a Game for Older Adults on Lifestyles and Frailty. Nurs. Rep. 2024, 14, 2499-2512. https://doi.org/10.3390/nursrep14030184
Faria AdCA, Martins MM, Laredo-Aguilera JA, Ventura-Silva JMA, Ribeiro OMPL. Development and Validation of a Game for Older Adults on Lifestyles and Frailty. Nursing Reports. 2024; 14(3):2499-2512. https://doi.org/10.3390/nursrep14030184
Chicago/Turabian StyleFaria, Ana da Conceição Alves, Maria Manuela Martins, José Alberto Laredo-Aguilera, João Miguel Almeida Ventura-Silva, and Olga Maria Pimenta Lopes Ribeiro. 2024. "Development and Validation of a Game for Older Adults on Lifestyles and Frailty" Nursing Reports 14, no. 3: 2499-2512. https://doi.org/10.3390/nursrep14030184
APA StyleFaria, A. d. C. A., Martins, M. M., Laredo-Aguilera, J. A., Ventura-Silva, J. M. A., & Ribeiro, O. M. P. L. (2024). Development and Validation of a Game for Older Adults on Lifestyles and Frailty. Nursing Reports, 14(3), 2499-2512. https://doi.org/10.3390/nursrep14030184