

Evaluation of the Perceived Benefits of a Peer Support Group for People with Mental Health Problems


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Recruitment and Sampling
2.3. Data Collection
2.4. Data Analysis
- The facilitators familiarised themselves with the raw data from the interviews.
- Initial codes were identified from the data.
- Initial themes were generated from within the data.
- The themes identified were reviewed against the specific aims of the evaluation.
- The content and names of themes were reviewed for homogeneity and compatibility.
- Suitable participant quotes were identified to aid accurate and illustrative write-up of each theme in this report [40].
2.5. Ethics
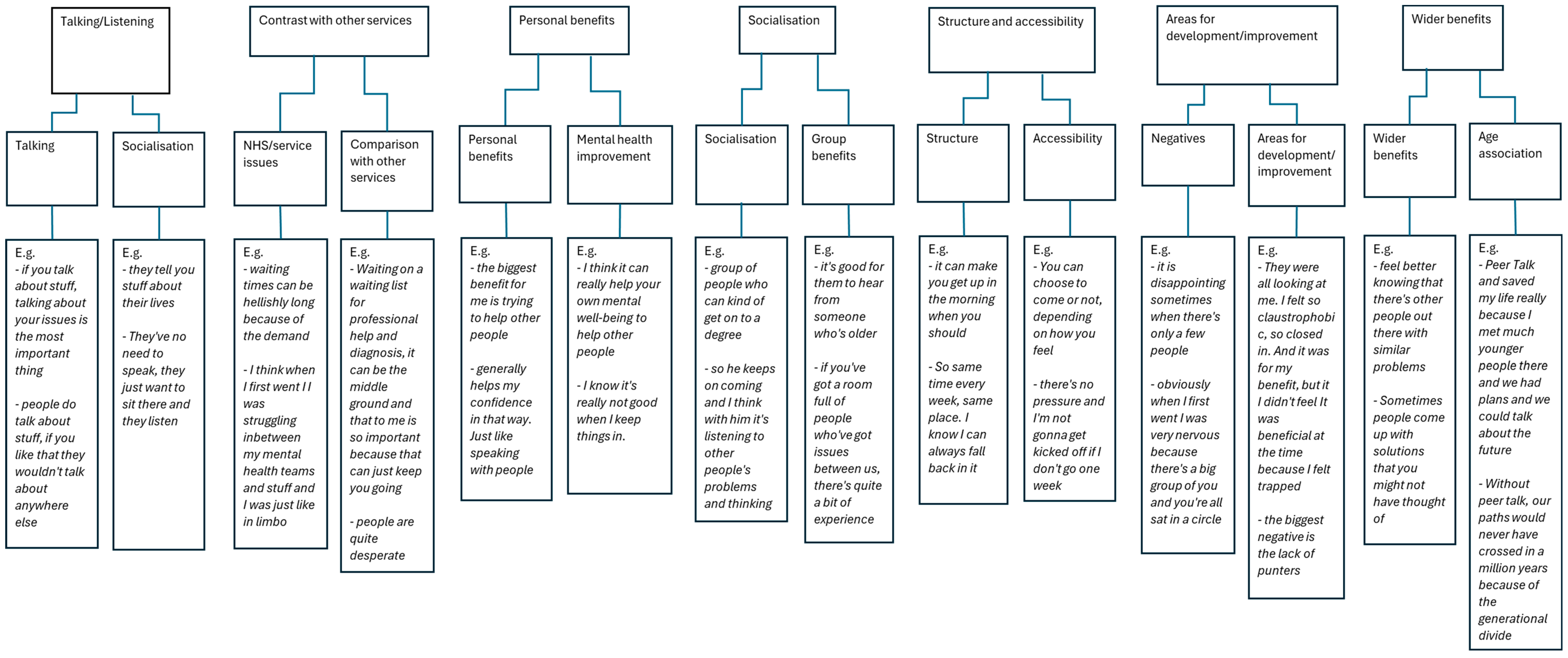
3. Results
3.1. Talking/Listening
“…some people come and they don’t say a word. They’ve no need to speak; they just want to sit there and listen”.(Participant 2)
“… it was quite relieving. Just being able to have a little space just to talk”.(Participant 3)
“I think these meetings allow people one, to voice what they think; and two, to reassure other people…”.(Participant 2)
“It is an opportunity to talk about things that make me emotionally upset”.(Participant 5)
“…helps you regulate it a bit, because once you’ve said it, it’s out in the world and it’s just like a problem halved”.(Participant 3)
“To have a genuine exchange of peer experiences…”.(Participant 2)
3.2. Socialising
“…meeting people from all walks of life, you would never ever meet in any other circumstance”.(Participant 2)
“The age group could be from 19 to, I think the group I go to, the oldest is 65”.(Participant 2)
“…there’s a diverse range of people come to these meetings…”.(Participant 2)
“…in PeerTalk, we’re totally neurodivergent when we totally just normally accept that, you know, that they’re, you know, the 16 others, as there often is, and in our group, there are 16 different versions of what’s going on…”.(Participant 5)
“I get the perspective of these different people, you know, the women, as opposed to men, the young ones, the older ones, the students as opposed to the bricklayers, the whatever, and they all had this different perspective”.(Participant 5)
“…get to know them as you come more regularly and I have made friends from it as well. It’s a friendly atmosphere”.(Participant 2)
“Everyone’s nervous the first time—I was, but once you get to know how friendly it is, your loneliness dissipates because you’ve got this to look forward to every week”.(Participant 6)
“And once you do it once [talk], it kind of breaks the barrier and then it’s easier and easier and easier”.(Participant 3)
3.3. Contrast with Other Services
“…waiting times can be hellishly long because of the demand…”.(Participant 2)
“…when you’re waiting for something on a list, you think it’s never going to happen”.(Participant 2)
“I’ve been to other groups where they give you two minutes or they give you a certain question to respond to. That’s not how mental health works. PeerTalk’s different”.(Participant 6)
“It’s vital while people are waiting desperately to be treated by NHS services”.(Participant 6)
“I think when I first went, I was struggling in between my mental health teams and stuff and I was just like in limbo”.(Participant 3)
“I get far more from PeerTalk groups than I ever did with CBT”.(Participant 2)
“…there’s not enough help with mental health services out of hours”.(Participant 2)
“If something happens with my mental health team, I can at least fall back on that [referring to PeerTalk] and I won’t have nothing”.(Participant 3)
“When I first came to a peer group, they were very careful to explain to me it is not a therapy”.(Participant 5)
“Ultimately we’re not medical professionals; we’re not there to diagnose issues”.(Participant 2)
3.4. Personal Benefits
“It’s helped me to quite significantly mature my self-perception and I’ve found some new insights”.(Participant 2)
“I’ve been very grateful for my people, for giving me vocabulary and some labels to discuss those things”.(Participant 5)
“It helps me to help others, to understand their feelings”.(Participant 6)
“I experienced that feeling of being helpful and knowledgeable and important, and not just old and ill, and that’s greatly helped my self-confidence”.(Participant 5)
“…because I’m involved in a group of people who’ve got future plans, they’re keeping up to date with themselves. I’m in the future and in the future, I have hope”.(Participant 5)
“You’re building these connections with people helping them; you’re also helping yourself”.(Participant 3)
“The biggest benefit for me is trying to help other people”.(Participant 2)
3.5. Structure and Accessibility
“…so same time every week, same place. I know I can always fall back on it”.(Participant 3)
“In terms of structure, PeerTalk meetings give me a reason to have structure in the rest of my week. So I can talk about it”.(Participant 6)
“But it’s so good to know my pattern is set one event after another. Yeah, 7:30 on a Thursday is very important”.(Participant 2)
“I relish going to these groups ever single week and I go every single week without fail”.(Participant 2)
3.6. Wider Benefits
“…we laugh quite a lot”.(Participant 3)
“…you sometimes feel that you’re the only one, when actually there’s lots of people out there who need similar support”.(Participant 2)
“…you can see a different perspective that someone in that situation can’t see”.(Participant 3)
“…if it’s not trivial to the individual, it’s so important they’re made aware of that”.(Participant 2)
4. Discussion
4.1. Limitations of the Study
4.2. Recommendations for PeerTalk
“…in a sense, the numbers need to be ramped up, to have a genuine exchange of peer experiences”.(Participant 2)
“…the biggest negative is the lack of punters”.(Participant 2)
4.3. Recommendations for Practice
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Use of Artificial Intelligence
Conflicts of Interest
Appendix A

{kind=link}
| Question No | Question |
|---|---|
| 1 | What is it about the sessions that provides benefit to you? |
| 2 | How have the PeerTalk sessions helped you relieve the pressure of your emotions? |
| 3 | Can you tell me how the PeerTalk sessions have helped with your confidence? |
| 4 | How have you been able to help support other group members? |
| 5 | How do the sessions help lift your mood? |
| 6 | How have the PeerTalk sessions helped you with loneliness? |
| 7 | In what way does the PeerTalk sessions provide structure to your life? |
| 8 | How has the PeerTalk sessions helped you understand your own feelings? |
| 9 | In what way do the sessions provide you with a new perspective on life? |
| 10 | What other support have you found through the PeerTalk sessions (e.g., other groups, services) |
Appendix B
References
- Torres, F. What Is Depression? American Psychiatric Association. Available online: https://www.psychiatry.org/patients-families/depression/what-is-depression (accessed on 26 March 2024).
- World Health Organization. Depressive Disorder (Depression). Available online: https://www.who.int/news-room/fact-sheets/detail/depression (accessed on 6 March 2024).
- Rahman, A.; Malik, A.; Sikander, S.; Roberts, C.; Creed, F. Cognitive behaviour therapy-based intervention by community health workers for mothers with depression and their infants in rural Pakistan: A cluster-randomised controlled trial. Lancet 2008, 372, 902–909. [Google Scholar] [CrossRef]
- Lockhart, E.; Foreman, J.; Mase, R.; Heisler, M. Heart failure patients’ experiences of a self-management peer support program: A qualitative study. Heart Lung 2014, 43, 292–298. [Google Scholar] [CrossRef]
- Dale, J.R.; Williams, S.M.; Bowyer, V. What is the effect of peer support on diabetes outcomes in adults? A systematic review. Diabet. Med. 2012, 29, 1361–1377. [Google Scholar] [CrossRef]
- Lloyd-Evans, B.; Mayo-Wilson, E.; Harrison, B.; Istead, H.; Brown, E.; Pilling, S.; Johnson, S.; Kendall, T. A systematic review and meta-analysis of randomised controlled trials of peer support for people with severe mental illness. BMC Psychiatry 2014, 14, 39. [Google Scholar] [CrossRef]
- Schiller, V.F.; Dorstyn, D.S.; Taylor, A.M. The Protective Role of Social Support Sources and Types Against Depression in Caregivers: A Meta-Analysis. J. Autism Dev. Disord. 2021, 51, 1304–1315. [Google Scholar] [CrossRef]
- Crabtree, J.W.; Haslam, S.A.; Postmes, T.; Haslam, C. Mental Health Support Groups, Stigma, and Self-Esteem: Positive and Negative Implications of Group Identification: Mental Health and Stigma. J. Soc. Issues 2010, 66, 553–569. [Google Scholar] [CrossRef]
- Davidson, L.; Guy, K. Peer support among persons with severe mental illnesses: A review of evidence and experience. World Psychiatry 2012, 11, 123–128. [Google Scholar] [CrossRef]
- Kaltenboeck, A.; Harmer, C. The neuroscience of depressive disorders: A brief review of the past and some considerations about the future. Brain Neurosci. Adv. 2018, 2, 2398212818799269. [Google Scholar] [CrossRef]
- Cowen, P.J. Neuroendocrine and Neurochemical Processes in Depression. J. Exp. Psychopathol. 2016, a3, 3–15. [Google Scholar] [CrossRef]
- Lee, S.; Rhee, D. Effects of ginseng on stress-related depression, anxiety, and the hypothalamic-pituitary-adrenal axis. J. Ginseng Res. 2017, 41, 589–594. [Google Scholar] [CrossRef] [PubMed]
- Chekroud, A.M. Unifying treatments for depression: An application of the Free Energy Principle. Front. Psychol. 2015, 6, 153. [Google Scholar] [CrossRef]
- Nettle, D.; Bateson, M. The Evolutionary Origins of Mood and Its Disorders. Curr. Biol. 2012, 22, R712–R721. [Google Scholar] [CrossRef]
- Badcock, P.B. Evolutionary Systems Theory: A Unifying Meta-Theory of Psychological Science. Rev. Gen. Psychol. 2012, 16, 10–23. [Google Scholar] [CrossRef]
- Andrews, P.W.; Thomson, J.A. The Bright Side of Being Blue: Depression as an Adaptation for Analyzing Complex Problems. Psychol. Rev. 2009, 116, 620–654. [Google Scholar] [CrossRef]
- Hendrickx, G.; De Roeck, V.; Maras, A.; Dieleman, G.; Gerritsen, S.; Purper-Ouakil, D.; Russet, F.; Schepker, R.; Signorini, G.; Singh, S.P.; et al. Challenges during the Transition from Child and Adolescent Mental Health Services to Adult Mental Health Services. BJPsych Bull. 2020, 44, 163–168. [Google Scholar] [CrossRef]
- Embuldeniya, G.; Veinot, P.; Bell, E.; Bell, M.; Nyhof-Young, J.; Sale, J.E.M.; Britten, N. The experience and impact of chronic disease peer support interventions: A qualitative synthesis. Patient Educ. Couns. 2013, 92, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Dennis, C.; Dowswell, T.; Dennis, C. Psychosocial and psychological interventions for preventing postpartum depression. Cochrane Database Syst. Rev. 2013, 2013, CD001134. [Google Scholar] [CrossRef] [PubMed]
- Rush, B.; Urbanoski, K.; Bassani, D.; Castel, S.; Wild, T.C.; Strike, C.; Kimberley, D.; Somers, J. Prevalence of Co-Occurring Substance Use and other Mental Disorders in the Canadian Population. Can. J. Psychiatry 2008, 53, 800–809. [Google Scholar] [CrossRef]
- Cummings, J.R.; Zhang, X.; Gandré, C.; Morsella, A.; Shields-Zeeman, L.; Winkelmann, J.; Allin, S.; Augusto, G.F.; Cascini, F.; Cserháti, Z.; et al. Challenges facing mental health systems arising from the COVID-19 pandemic: Evidence from 14 European and North American countries. Health Policy 2023, 136, 104878. [Google Scholar] [CrossRef]
- Department of Health. No Decision about Me, without Me Liberating the NHS: Government Response; Department of Health: London, UK, 2012. [Google Scholar]
- Pfeiffer, P.N.; Heisler, M.; Piette, J.D.; Rogers, M.A.; Valenstein, M. Efficacy of peer support interventions for depression: A meta-analysis. Gen. Hosp. Psychiatry 2011, 33, 29–36. [Google Scholar] [CrossRef]
- Reynolds, K.A.; Helgeson, V.S. Children with Diabetes Compared to Peers: Depressed? Distressed? A Meta-Analytic Review. Ann. Behav. Med. 2011, 42, 29–41. [Google Scholar] [CrossRef]
- Williford, A.; Boulton, A.; Noland, B.; Little, T.D.; Kärnä, A.; Salmivalli, C. Effects of the KiVa Anti-bullying Program on Adolescents’ Depression, Anxiety, and Perception of Peers. J. Abnorm. Child. Psychol. 2012, 40, 289–300. [Google Scholar] [CrossRef]
- van Mol, M.M.; Kompanje, E.J.O.; Benoit, D.D.; Bakker, J.; Nijkamp, M.D. The Prevalence of Compassion Fatigue and Burnout among Healthcare Professionals in Intensive Care Units: A Systematic Review. PLoS ONE 2015, 10, e0136955. [Google Scholar] [CrossRef]
- Shilling, V.; Morris, C.; Thompson-Coon, J.; Ukoumunne, O.; Rogers, M.; Logan, S. Peer support for parents of children with chronic disabling conditions: A systematic review of quantitative and qualitative studies. Dev. Med. Child Neurol. 2013, 55, 602–609. [Google Scholar] [CrossRef]
- Shorey, S.; Chee, C.Y.I.; Ng, E.D.; Lau, Y.; Dennis, C.; Chan, Y.H. Evaluation of a Technology-Based Peer-Support Intervention Program for Preventing Postnatal Depression (Part 1): Randomized Controlled Trial. J. Med. Internet Res. 2019, 21, e12410. [Google Scholar] [CrossRef]
- Dukhovny, D.; Dennis, C.; Hodnett, E.; Weston, J.; Stewart, D.E.; Mao, W.; Zupancic, J.A.F. Prospective Economic Evaluation of a Peer Support Intervention for Prevention of Postpartum Depression among High-Risk Women in Ontario, Canada. Am. J. Perinatol. 2013, 30, 631–642. [Google Scholar] [CrossRef]
- Chinman, M.; George, P.; Dougherty, R.H.; Daniels, A.S.; Ghose, S.S.; Swift, A.; Delphin-Rittmon, M. Peer Support Services for Individuals with Serious Mental Illnesses: Assessing the Evidence. Psychiatr. Serv. 2014, 65, 429–441. [Google Scholar] [CrossRef]
- Heaslip, V.; Lindsay, B. Research and Evidence-Based Practice: For Nursing, Health and Social Care Students; Lantern: Banbury, UK, 2019. [Google Scholar]
- Evaluation Practice Handbook. Available online: https://cdn.who.int/media/docs/default-source/evaluation-office/who-evaluation-practice-handbook-2013.pdf?sfvrsn=2513394e_3&download=true (accessed on 6 March 2024).
- Szulc, J.; King, N. The Practice of Dyadic Interviewing: Strengths, Limitations and Key Decisions. FQS 2022, 23, 2. [Google Scholar]
- Green, J.; Thorogood, N. Qualitative Methods for Health Research; SAGE: Newcastle upon Tyne, UK, 2009. [Google Scholar]
- Morgan, D.L.; Eliot, S.; Lowe, R.A.; Gorman, P. Dyadic Interviews as a Tool for Qualitative Evaluation. Am. J. Eval. 2015, 37, 109–117. [Google Scholar] [CrossRef]
- Finch, A.; Ali, S.; Chang, D. Exploratory Conversations: Reflections on Developing a Triad Interview Method. Res. All 2023, 7, 1–8. [Google Scholar] [CrossRef]
- Zoom ©—Zoom Software; Version [6.1.1 (41705)]; Zoom Video Communications, Inc.: San Jose, CA, USA, 2023; Available online: https://zoom.com (accessed on 6 March 2024).
- Oliffe, J.L.; Kelly, M.T.; Gonzalez Montaner, G.; Yu Ko, W.F. Zoom Interviews: Benefits and Concessions. Int. J. Qual. Methods 2021, 20, 160940692110535. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Morse, J.M. Critical Analysis of Strategies for Determining Rigor in Qualitative Inquiry. Qual. Health Res. 2015, 25, 1212–1222. [Google Scholar] [CrossRef] [PubMed]
- Qualtrics XM: The Leading Experience Management Software; Version [July 2024]; Qualtrics: Provo, UT, USA, 2024; Available online: https://www.qualtrics.com (accessed on 26 March 2024).
- National Confidential Inquiry into Suicide and Safety in Mental Health. Available online: https://documents.manchester.ac.uk/display.aspx?DocID=71818 (accessed on 6 March 2024).
- Seebohm, P.; Chaudhary, S.; Boyce, M.; Elkan, R.; Avis, M.; Munn-Giddings, C. The contribution of self-help/mutual aid groups to mental well-being. Health Soc. Care Community 2013, 21, 391–401. [Google Scholar] [CrossRef] [PubMed]
- Strand, M.; Eng, L.S.; Gammon, D. Combining online and offline peer support groups in community mental health care settings: A qualitative study of service users’ experiences. Int. J. Ment. Health Syst. 2020, 14, 39. [Google Scholar] [CrossRef] [PubMed]
- McMahon, G.; Douglas, A.; Casey, K.; Ahern, E. Disruption to well-being activities and depressive symptoms during the COVID-19 pandemic: The mediational role of social connectedness and rumination. J. Affect. Disord. 2022, 309, 274–281. [Google Scholar] [CrossRef]
- Vickery, A. ‘It’s made me feel less isolated because there are other people who are experiencing the same or very similar to you’: Men’s experiences of using mental health support groups. Health Soc. Care Community 2022, 30, 2383–2391. [Google Scholar] [CrossRef] [PubMed]
- Satinsky, E.; Crepaz-Keay, D.; Kousoulis, A. Making peer-focused self-management programmes work in public mental health. J. Ment. Health Train. Educ. Pract. 2018, 13, 257–263. [Google Scholar] [CrossRef]
- Henriksen, I.O.; Ranøyen, I.; Indredavik, M.S.; Stenseng, F. The role of self-esteem in the development of psychiatric problems: A three-year prospective study in a clinical sample of adolescents. Child. Adolesc. Psychiatry Ment. Health 2017, 11, 68. [Google Scholar] [CrossRef]
- Barbalat, G.; Plasse, J.; Gauthier, E.; Verdoux, H.; Quiles, C.; Dubreucq, J.; Legros-Lafarge, E.; Jaafari, N.; Massoubre, C.; Guillard-Bouhet, N.; et al. The central role of self-esteem in the quality of life of patients with mental disorders. Sci. Rep. 2022, 12, 7852. [Google Scholar] [CrossRef]
- Haim-Litevsky, D.; Komemi, R.; Lipskaya-Velikovsky, L. Sense of Belonging, Meaningful Daily Life Participation, and Well-Being: Integrated Investigation. Int. J. Environ. Res. Public Health 2023, 20, 4121. [Google Scholar] [CrossRef] [PubMed]
- National Health Service. NHS Talking Therapies, for Anxiety and Depression, Annual Reports, 2022–2023. 2024. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/nhs-talking-therapies-for-anxiety-and-depression-annual-reports/2022-23Digital (accessed on 26 March 2024).
- Kelly, J.F.; Hoffman, L.; Vilsaint, C.; Weiss, R.; Nierenberg, A.; Hoeppner, B. Peer support for mood disorder: Characteristics and benefits from attending the Depression and Bipolar Support Alliance mutual-help organization. J. Affect. Disord. 2019, 255, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Hennink, M.M.; Kaiser, B.N.; Weber, M.B. What Influences Saturation? Estimating Sample Sizes in Focus Group Research. Qual. Health Res. 2019, 29, 1483–1496. [Google Scholar] [CrossRef] [PubMed]
- Equality Act 2010; HMSO: London, UK, 2010; Available online: https://www.legislation.gov.uk/ukpga/2010/15/contents (accessed on 4 July 2024).
- Connell, C.; Jones, E.; Haslam, M.; Firestone, J.; Pope, G.; Thompson, C. Mental health nursing identity: A critical analysis of the UK’s Nursing and Midwifery Council’s pre-registration syllabus change and subsequent move towards genericism. Ment. Health Rev. J. 2022, 27, 472–483. [Google Scholar] [CrossRef]
- Cooper, M.; Flynn, D.; Avery, L.; Ashley, K.; Jordan, C.; Errington, L.; Scott, J. Service user perspectives on social prescribing services for mental health in the UK: A systematic review. Perspect. Public Health 2023, 143, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Walker, G.; Bryant, W. Peer Support in Adult Mental Health Services: A Metasynthesis of Qualitative Findings. Psychiatr. Rehabil. J. 2013, 36, 28–34. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beard, D.; Cottam, C.; Painter, J. Evaluation of the Perceived Benefits of a Peer Support Group for People with Mental Health Problems. Nurs. Rep. 2024, 14, 1661-1675. https://doi.org/10.3390/nursrep14030124
Beard D, Cottam C, Painter J. Evaluation of the Perceived Benefits of a Peer Support Group for People with Mental Health Problems. Nursing Reports. 2024; 14(3):1661-1675. https://doi.org/10.3390/nursrep14030124
Chicago/Turabian StyleBeard, David, Charlie Cottam, and Jon Painter. 2024. "Evaluation of the Perceived Benefits of a Peer Support Group for People with Mental Health Problems" Nursing Reports 14, no. 3: 1661-1675. https://doi.org/10.3390/nursrep14030124
APA StyleBeard, D., Cottam, C., & Painter, J. (2024). Evaluation of the Perceived Benefits of a Peer Support Group for People with Mental Health Problems. Nursing Reports, 14(3), 1661-1675. https://doi.org/10.3390/nursrep14030124