
Mental Health Nursing Student’s Perception of Clinical Simulation about Patients at Risk of Suicide: A Qualitative Study

 ,
,  ,
,  ,
,  ,
,  , ,
, ,  , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Research Team and Reflexivity
2.3. Participants and Sampling
2.4. Data Collection
High Fidelity Simulation Procedure
2.5. Data Analysis
2.6. Ethical Considerations
2.7. Strictness Criteria
3. Results
3.1. Demographic Data
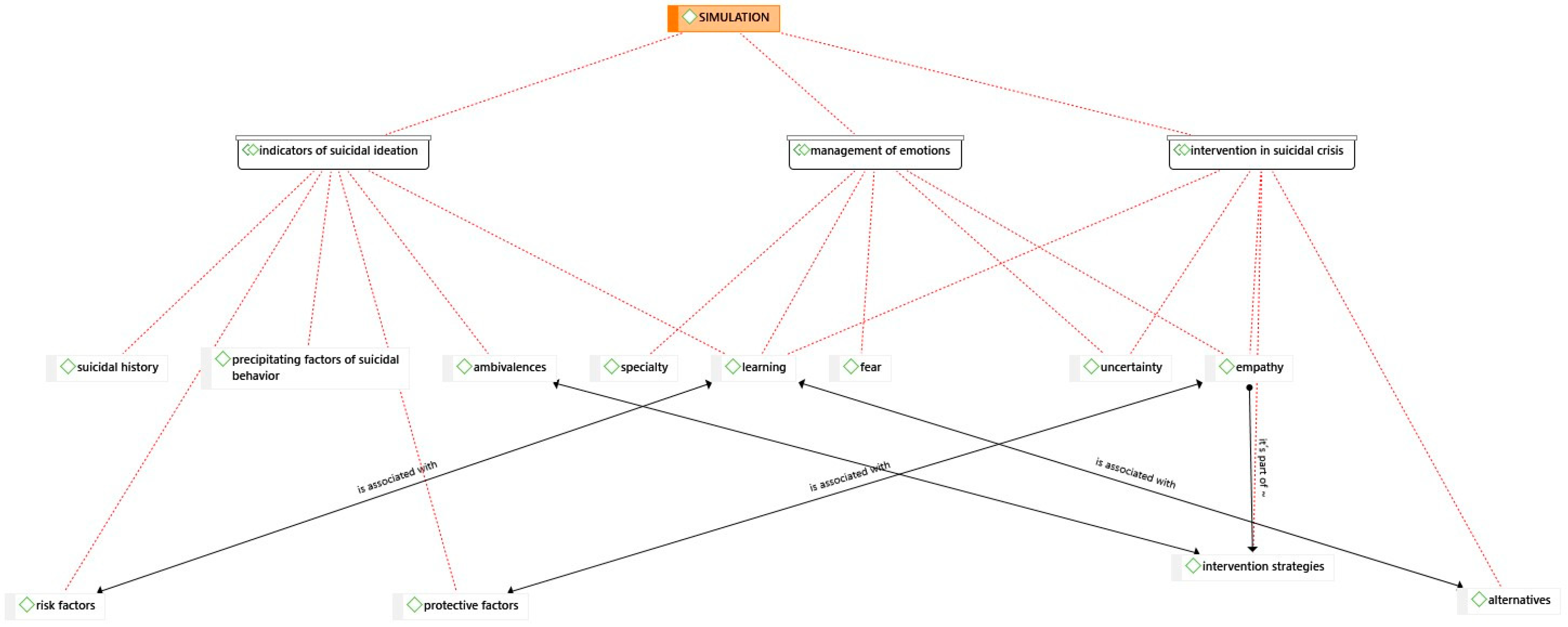
3.2. Themes
- Theme 1: Management and handling of emotions.
“The uncertainty, isn’t it? Because in the end, the situation doesn’t depend on you…”FG3
“I don’t know… as if he was always telling bad things, you empathized a lot with him… and you said fuck… and you wanted to find something good for him to get out of that… out of that loop from which he wants to commit suicide… I don’t know…” FG2: “I have felt the desperation they suffer, the inability to cope with situations.” FG1
“My fear of these situations has been removed, and I find myself much more prepared” E15 “I gained confidence by remembering the points explained earlier.” E4
“I have been very motivated thinking about possibly doing the mental health specialty.” E27 “I thought I didn’t like mental health, but since the simulation, it has caught my attention, and I am looking forward to it.” E31
“It has been challenging, helping us to reflect and having a link between theory and practice.”E20
“I have learned the keys to interventions for these patients.”E22
“It has been fundamental to have a real actor as a patient. It has made the simulation much more realistic.”E19
- Theme 2: Indicators of suicidal behavior
“It is important to identify why the person is in that situation.” E1. This statement is supported and enriched by the comments collected during the FGs. In one of the groups, various aspects that could contribute to the patient’s situation were explored:
“The economic issue, the family issue, the divorce issue, the relationship with the daughters, all these are risk factors.”FG1
“…it is an indicator, it is a protective factor of beliefs.”FG4
“The suicidal career can be very varied, but such events accumulate that I accumulate, and there comes a time when I can’t take it anymore, and that drop is predisposed.”FG3
“The wife… the daughters… have been a bit ambivalent, right? In the beginning, it seemed like… then it seemed like… with you, it seemed like.”FG1
“Creating ambivalence, yes it can be all and I at the end for them to decide and make that decision to take another path.”FG2
“Once the life hitch was identified, it has been easier to establish ambivalence.”E9
- Theme 3: Suicide crisis intervention
“We have learned how the approach to the simulation should be, following the steps.”E12
“The connection, what’s the first thing to do? Hook up with the person; otherwise, you won’t have anything.”FG4
“I introduced myself, tried to get him to talk to me, and got down to his level.”FG2
“I position myself as a safety measure to ensure that the person does not catch me at a given moment and throw me away, but I put myself at their level.”E12
“My partners and I did a pretty thorough approach…using relaxation techniques…looking for alternatives.”E4
“Sometimes I’ve felt like it was like what the two partners said a little bit, you’re left kind of thinking I don’t know if what I’m going to say now will be impactful enough for me to pay attention.”FG2
“I think the main thing is to accompany them, listen to them and make them feel supported…give alternatives that we can give him because he is not seeing them.”E5
“I told him that there were other alternatives to quitting that, even though he tried it once, it doesn’t mean it’s the only one, that he can try again.”FG3
4. Discussion
5. Strengths and Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Suicide Mortality Data. 2021. Available online: https://www.who.int/es/news-room/fact-sheets/detail/suicide (accessed on 11 March 2024).
- Sufrate-Sorzano, T. Suicide prevention from the classroom. In Nursing Interventions and Tools for Suicide Prevention; Activity book; Siníndice: Logroño, La Rioja, Spain, 2021. [Google Scholar]
- Harmer, B.; Lee, S.; Duong, T.V.H.; Saadabadi, A. Suicidal Ideation. Stat Pearls. In Treasure Island (FL); StatPearls: St. Petersburg, FL, USA, 2024. [Google Scholar]
- Echávarri-Gorricho, A. Concept and Classification of Suicidal Behavior. 2010. Available online: ftp.formainap.navarra.es/2014/2014-3E604-9971-SUICIDIO/TEMA%201.pdf (accessed on 11 March 2024).
- Hernández-Bello, L.; Hueso-Montoro, C.; Gómez-Urquiza, J.L.; Cogollo-Milanés, Z. Prevalence and associated factor for ideation and suicide attempt in adolescents: A systematic review. Rev. Esp. Public. Health 2020, 10, 94. [Google Scholar]
- National Institute of Statistics. Deaths from Causes, Gender, and Age Groups. 2020. Available online: https://www.ine.es/jaxiT3/Datos.htm?t=7947 (accessed on 15 November 2023).
- Spanish Foundation for Suicide Prevention. Suicide Observatory in Spain. 2022. Available online: https://www.fsme.es/observatorio-del-suicidio-2022-definitivo/ (accessed on 18 December 2023).
- Darnell, D.; Areán, P.A.; Dorsey, S.; Atkins, D.C.; Tanana, M.J.; Hirsch, T.; Mooney, S.D.; Boudreaux, E.D.; Comtois, K.A. Harnessing Innovative Technologies to Train Nurses in Suicide Safety Planning With Hospitalized Patients: Protocol for Formative and Pilot Feasibility Research. JMIR Res. Protoc. 2021, 15, 10. [Google Scholar] [CrossRef]
- World Health Organization. 72nd World Health Assembly. 2019. Available online: https://apps.who.int/gb/ebwha/pdf_files/WHA72/A72_11Rev1-sp.pdf (accessed on 11 March 2024).
- Heyman, I.; Webster, B.J.; Tee, S. Curriculum development through understanding the student nurse experience of suicide intervention education—A phenomenographic study. Nurse Educ. Pract. 2015, 15, 498–506. [Google Scholar] [CrossRef]
- Motillon-Toudic, C.; Walter, M.; Séguin, M.; Carrier, J.D.; Berrouiguet, S.; Lemey, C. Social isolation and suicide risk: Literature review and perspectives. Eur. Psychiatry 2022, 65, 1–22. [Google Scholar] [CrossRef]
- Oexle, N.; Rüsch, N. Stigma-risk factor and consequence of suicidal behavior: Implications for suicide prevention. Nervenarzt 2018, 89, 779–783. [Google Scholar] [CrossRef]
- Menon, V.; Vijayakumar, L. Interventions for attempted suicide. Curr. Opin. Psychiatry 2022, 35, 317–323. [Google Scholar] [CrossRef]
- Farmani, A.; Rahimianbougar, M.; Mohammadi, Y.; Faramarzi, H.; Khodarahimi, S.; Nahaboo, S. Psychological, Structural, Social and Economic Determinants of Suicide Attempt: Risk Assessment and Decision Making Strategies. Omega 2023, 86, 1144–1166. [Google Scholar] [CrossRef]
- Beghi, M.; Butera, E.; Cerri, C.G.; Cornaggia, C.M.; Febbo, F.; Mollica, A.; Berardino, G.; Piscitelli, D.; Resta, E.; Logroscino, G.; et al. Suicidal behaviour in older age: A systematic review of risk factors associated to suicide attempts and completed suicides. Neurosci. Biobehav. Rev. 2021, 127, 193–211. [Google Scholar] [CrossRef]
- Ferrara, P.; Terzoni, S.; Ruta, F.; Poggi, A.D.; Destrebecq, A.; Gambini, O.; D’agostino, A. Nursing students’ attitudes towards suicide and suicidal patients: A multicentre cross-sectional survey. Nurse Educ. Today 2022, 109, 105258. [Google Scholar] [CrossRef]
- Sufrate-Sorzano, T.; Juárez-Vela, R.; Ramírez-Torres, C.A.; Rivera-Sanz, F.; Garrote-Camara, M.E.; Roland, P.P.; Gea-Sánchez, M.; Del Pozo-Herce, P.; Gea-Caballero, V.; Angulo-Nalda, B.; et al. Nursing interventions of choice for the prevention and treatment of suicidal behaviour: The umbrella review protocol. Nurs. Open. 2022, 9, 845–850. [Google Scholar] [CrossRef] [PubMed]
- Richard, O.; Jollant, F.; Billon, G.; Attoe, C.; Vodovar, D.; Piot, M.A. Simulation training in suicide risk assessment and intervention: A systematic review and meta-analysis. Med. Educ. Online 2023, 28, 2199469. [Google Scholar] [CrossRef]
- Vannoy, S.D.; Fancher, T.; Meltvedt, C.; Unützer, J.; Duberstein, P.; Kravitz, R.L. Suicide inquiry in primary care: Creating context, inquiring, and following up. Ann. Fam. Med. 2010, 8, 33–39. [Google Scholar] [CrossRef]
- Hawgood, J.; Woodward, A.; Quinnett, P.; De Leo, D. Gatekeeper Training and Minimum Standards of Competency. Crisis 2022, 43, 516–522. [Google Scholar] [CrossRef]
- O’Brien, K.H.M.; Fuxman, S.; Humm, L.; Tirone, N.; Pires, W.J.; Cole, A.; Goldstein, G.J. Suicide risk assessment training using an online virtual patient simulation. mHealth 2019, 5, 31. [Google Scholar] [CrossRef]
- Silva, C.; Smith, A.R.; Dodd, D.R.; Covington, D.W.; Joiner, T.E. Suicide-Related Knowledge and Confidence Among Behavioral Health Care Staff in Seven States. Psychiatr. Serv. 2016, 67, 1240–1245. [Google Scholar] [CrossRef]
- Silverman, M.M.; Berman, A.L. Suicide risk assessment and risk formulation part I: A focus on suicide ideation in assessing suicide risk. Suicide Life Threat. Behav. 2014, 44, 420–431. [Google Scholar] [CrossRef] [PubMed]
- Goh, Y.S.; Selvarajan, S.; Chng, M.L.; Tan, C.S.; Yobas, P. Using standardized patients in enhancing undergraduate students’ learning experience in mental health nursing. Nurse Educ. Today 2016, 45, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Lilly, M.L.; Hermans, M.; Crawley, B. Psychiatric nursing emergency: A simulated experience of wrist-cutting suicide attempt. J. Psychosoc. Nurs. Ment. Health Serv. 2012, 50, 35–42. [Google Scholar] [CrossRef]
- Keltner, N.L.; Grant, J.S.; McLernon, D. Use of actors as standardized psychiatric patients. J. Psychosoc. Nurs. Ment. Health Serv. 2011, 49, 34–40. [Google Scholar] [CrossRef]
- Piot, M.A.; Attoe, C.; Billon, G.; Cross, S.; Rethans, J.J.; Falissard, B. Simulation Training in Psychiatry for Medical Education: A Review. Front. Psychiatry 2021, 12, 658967. [Google Scholar] [CrossRef] [PubMed]
- Vallance, A.K.; Hemani, A.; Fernandez, V.; Livingstone, D.; McCusker, K.; Toro-Troconis, M. Using virtual worlds for role 613 play simulation in child and adolescent psychiatry: An evaluation study. Psychiatr. Bull. 2014, 38, 204–210. [Google Scholar] [CrossRef]
- O’Brien, K.H.M.; Quinlan, K.; Humm, L.; Cole, A.; Pires, W.J.; Jacobs, A.; Goldstein-Grumet, J. A qualitative study of 616 provider feedback on the feasibility and acceptability of virtual patient simulations for suicide prevention training. mHealth 2022, 8, 31. [Google Scholar]
- Phillips, E.C.; Neagle, G.; Cameron, B.; Moneypenny, M. It’s okay to talk: Suicide awareness simulation. Clin. Teach. 2019, 16, 373–377. [Google Scholar] [CrossRef]
- Korstjens, I.; Moser, A. Series: Practical guidance to qualitative research. Part 2: Context, research questions and designs. Eur. J. Gen. Pract. 2017, 23, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.W.; Poth, C.N. Qualitative inquiry and research design. In Choosing among FIVE Approaches, 4th ed.; Sage: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Paley, J. Husserl, phenomenology and nursing. J. Adv. Nurs. 1997, 26, 187–193. [Google Scholar] [CrossRef]
- Al-Sheikh, M. The use of Husserl’s phenomenology in nursing research: A discussion paper. J. Adv. Nurs. 2023, 79, 3160–3169. [Google Scholar] [CrossRef]
- Moser, A.; Korstjens, I. Series: Practical guidance to qualitative research. Part 3: Sampling, data collection and analysis. Eur. J. Gen. Pract. 2018, 24, 9–18. [Google Scholar] [CrossRef]
- NANDA International. Nursing Diagnoses: Definitions and Classification 2018–2020; Elsevier: New York, NY, USA, 2019. [Google Scholar]
- Butcher, H.K.; Bulechek, G.M.; Dochterman, J.M.; Wagner, C.M. Nursing Interventions Classification (NIC); Elsevier: St. Louis, MO, USA, 2018. [Google Scholar]
- Sittner, B.J.; Aebersold, M.L.; Paige, J.B.; Graham, L.L.; Schram, A.P.; Decker, S.I.; Lioce, L. INACSL Standards of Best Practice for Simulation: Past, Present, and Future. Nur. Educ. Perspect. 2015, 36, 294–298. [Google Scholar] [CrossRef]
- Rudolph, J.W.; Raemer, D.B.; Simon, R. Establishing a safe container for learning in simulation: The role of the presimulation briefing. Simul. Healthc. 2014, 9, 339–349. [Google Scholar] [CrossRef]
- Maestre, J.M.; Rudolph, J.W. Theories and styles of debriefing: The good judgment method as a tool for formative assessment in healthcare. Rev. Esp. Cardiol. 2015, 68, 282–285. [Google Scholar] [CrossRef]
- Kirkbakk-Fjær, K.; Hedelin, B.; Moen, Ø.L. Undergraduate Nursing Students’ Evaluation of the Debriefing Phase in Mental Health Nursing Simulation. Issues Ment. Health Nurs. 2016, 37, 360–366. [Google Scholar] [CrossRef] [PubMed]
- Ng, R.; O’Reilly, C.L.; Collins, J.C.; Roennfeldt, H.; McMillan, S.S.; Wheeler, A.J.; El-Den, S. Mental Health First Aid crisis 649 role-plays between pharmacists and simulated patients with lived experience: A thematic analysis of debriefing. Soc. Psychiatry Psychiatr. Epidemiol. 2023, 58, 1365–1373. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. What can “thematic analysis” offer health and wellbeing researchers? Int. J. Qualitative Stud. Health Well-Being 2014, 9, 26153. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef]
- Morse, J.M. Critical Analysis of Strategies for Determining Rigor in Qualitative Inquiry. Qual. Health Res. 2015, 25, 1212–1222. [Google Scholar] [CrossRef]
- Soccio, D.A. Effectiveness of Mental Health Simulation in Replacing Traditional Clinical Hours in Baccalaureate Nursing Education. J. Psychosoc. Nurs. Ment. Health Serv. 2017, 55, 36–43. [Google Scholar] [CrossRef] [PubMed]
- McGough, S.; Heslop, K. Developing Mental Health-Related Simulation Activities for an Australian Undergraduate Nursing Curriculum. J. Nurs. Educ. 2021, 60, 356–361. [Google Scholar] [CrossRef]
- Simonelli-Muñoz, A.J.; Jiménez-Rodríguez, D.; Arrogante, O.; Plaza Del Pino, F.J.; Gallego-Gómez, J.I. Breaking the Stigma 668 in Mental Health Nursing through High-Fidelity Simulation Training. Nurs. Rep. 2023, 13, 1593–1606. [Google Scholar] [CrossRef]
- Lilly, M.L.; Hermanns, M.; Crawley, B. Clinical Simulation in Psychiatric-Mental Health Nursing: Post-Graduation Follow Up. J. Psychosoc. Nurs. Ment. Health Serv. 2016, 54, 40–46. [Google Scholar] [CrossRef]
- Koch, C.; Meier, S.; Fischer, C.; Brich, J. Simulated patients to demonstrate common stroke syndromes: Accurate and convincing. Cerebrovasc. Dis. 2023. [Google Scholar] [CrossRef]
- Lawton, A.J.; Greco, L.; Airaldi, R.; Tulsky, J.A. Development of an Actor Rehearsal Guide for Communication Skills Courses. BMJ Palliat. Care 2024. [Google Scholar] [CrossRef] [PubMed]
- Godzik, C.M.; Solomon, J.; Yacinthus, B. Using standardized mental health patient simulations to increase critical thinking and confidence in undergraduate nursing students. Arch. Psychiatr. 2023, 43, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Öz, F.; Turgut, A.N.; Meriç, M. Nursing student’s attitudes toward death and stigma toward individuals who attempt suicide. Perspect. Psychiatr. Care 2022, 58, 1728–1735. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Post-Clinical simulation phase |
|
| Simulated Scenario 1 | NANDA Diagnose | NIC Intervention | NOC Outcomes | Nursing Activities |
| A 34-year-old male, on our arrival, was on the M-40 bridge. He presented suicidal ideation and the intention to jump. As background, he refers to an argument with his wife. He has two daughters that he has not seen for some time, cocaine consumption, and his van broke down just today when he was going to deliver an order. No one else is on the bridge, only you (nursing students). You are the first to intervene and establish the first contact with the person. | (00150) Suicide risk | (6486) Environmental management: Safety (4500) Prevention of substance abuse (6340) Suicide prevention | (1408) Self-control of suicidal impulses (1904) Risk management: drug use |
|
| Simulated Scenario 2 | NANDA Diagnose | NIC Intervention | NOC Outcomes | Nursing Activities |
| Middle-aged man threatening to take his own life on the viaduct in Segovia (Madrid). No further information is available at the Emergency Service Center. You arrive as the first unit to intervene. When you come, the person is at high risk of suicide, as he is attached to a railing on the outside of the bridge. It is you (nursing students) who make the first contact. | (00124) Despair (00150) Suicide risk | (5230) Increasing coping (5270) Emotional support (4920) Active Listening (6654) Surveillance: security | (1302) Coping with problems (1305) Psychosocial modification: life change |
|
| Variables | N (%) |
|---|---|
| Age (Mean, SD) | 21.36 (2.29) |
| Gender | |
| Female | 41 (91.1%) |
| Male | 4 (8.9%) |
| Themes (T) | Categories | |
|---|---|---|
| T 1 | Management and handling of emotions | Fear, uncertainty, empathy, trust, learning, specialty. |
| T 2 | Indicators of suicidal behavior | Risk factors and protective factors, precipitating factors of suicidal behavior, suicidal history, and ambivalence. |
| T 3 | Suicidal crisis intervention | Establishment of the relationship, intervention strategies and alternatives. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Del Pozo-Herce, P.; Tovar-Reinoso, A.; Martínez-Sabater, A.; Chover-Sierra, E.; Pacheco-Tabuenca, T.; Carrasco-Yubero, J.; Sánchez-González, J.L.; González-Fernández, S.; Santolalla-Arnedo, I.; Sufrate-Sorzano, T.; et al. Mental Health Nursing Student’s Perception of Clinical Simulation about Patients at Risk of Suicide: A Qualitative Study. Nurs. Rep. 2024, 14, 641-654. https://doi.org/10.3390/nursrep14010049
Del Pozo-Herce P, Tovar-Reinoso A, Martínez-Sabater A, Chover-Sierra E, Pacheco-Tabuenca T, Carrasco-Yubero J, Sánchez-González JL, González-Fernández S, Santolalla-Arnedo I, Sufrate-Sorzano T, et al. Mental Health Nursing Student’s Perception of Clinical Simulation about Patients at Risk of Suicide: A Qualitative Study. Nursing Reports. 2024; 14(1):641-654. https://doi.org/10.3390/nursrep14010049
Chicago/Turabian StyleDel Pozo-Herce, Pablo, Alberto Tovar-Reinoso, Antonio Martínez-Sabater, Elena Chover-Sierra, Teresa Pacheco-Tabuenca, Jorge Carrasco-Yubero, Juan Luis Sánchez-González, Silvia González-Fernández, Iván Santolalla-Arnedo, Teresa Sufrate-Sorzano, and et al. 2024. "Mental Health Nursing Student’s Perception of Clinical Simulation about Patients at Risk of Suicide: A Qualitative Study" Nursing Reports 14, no. 1: 641-654. https://doi.org/10.3390/nursrep14010049
APA StyleDel Pozo-Herce, P., Tovar-Reinoso, A., Martínez-Sabater, A., Chover-Sierra, E., Pacheco-Tabuenca, T., Carrasco-Yubero, J., Sánchez-González, J. L., González-Fernández, S., Santolalla-Arnedo, I., Sufrate-Sorzano, T., Juárez-Vela, R., & García-Carpintero Blas, E. (2024). Mental Health Nursing Student’s Perception of Clinical Simulation about Patients at Risk of Suicide: A Qualitative Study. Nursing Reports, 14(1), 641-654. https://doi.org/10.3390/nursrep14010049