


Community-Based Action Research Intervention to Promote Occupational Health Nursing of Portuguese Quarry Workers

 ,
, {kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Phase 1: Social Assessment
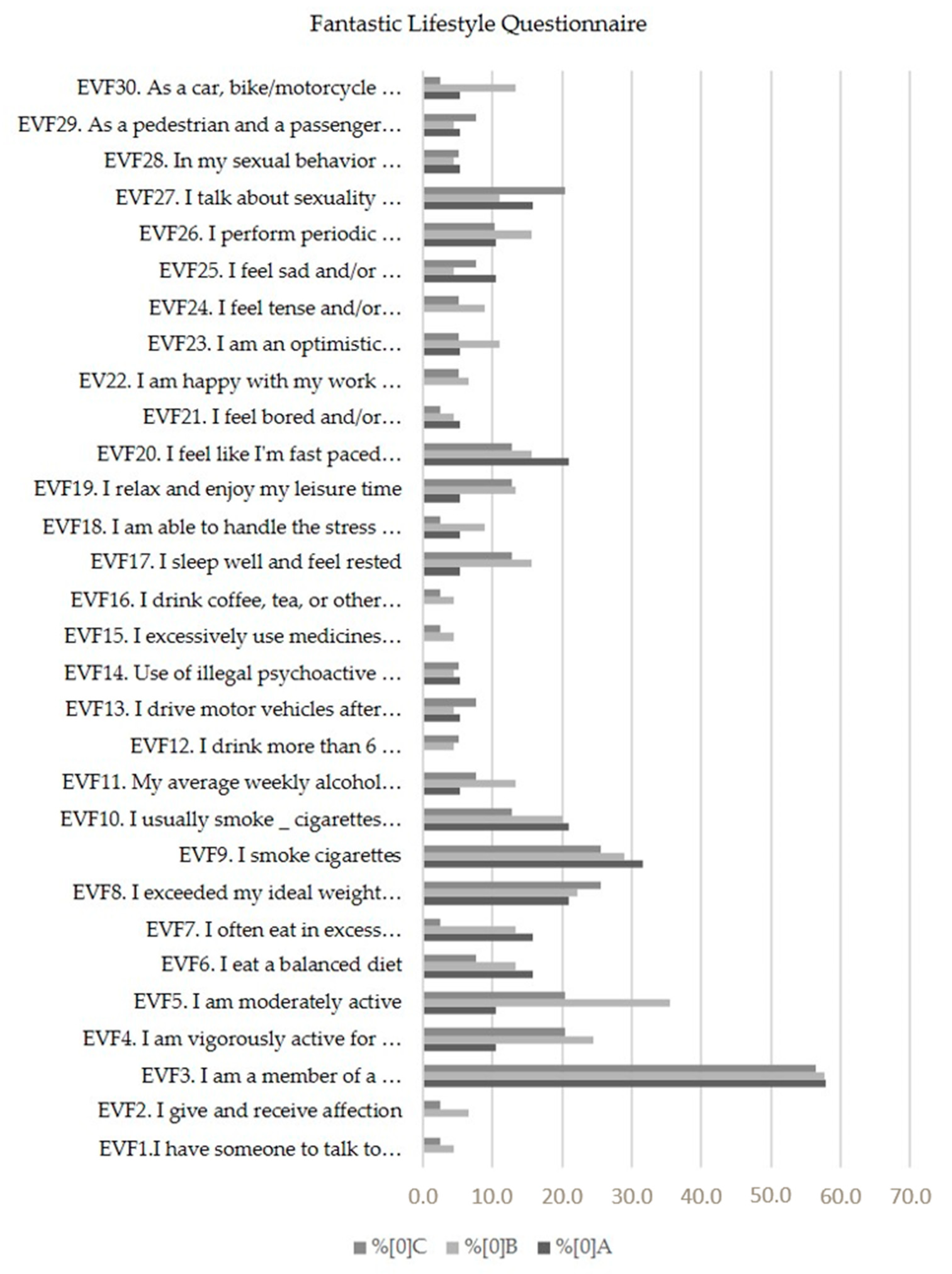
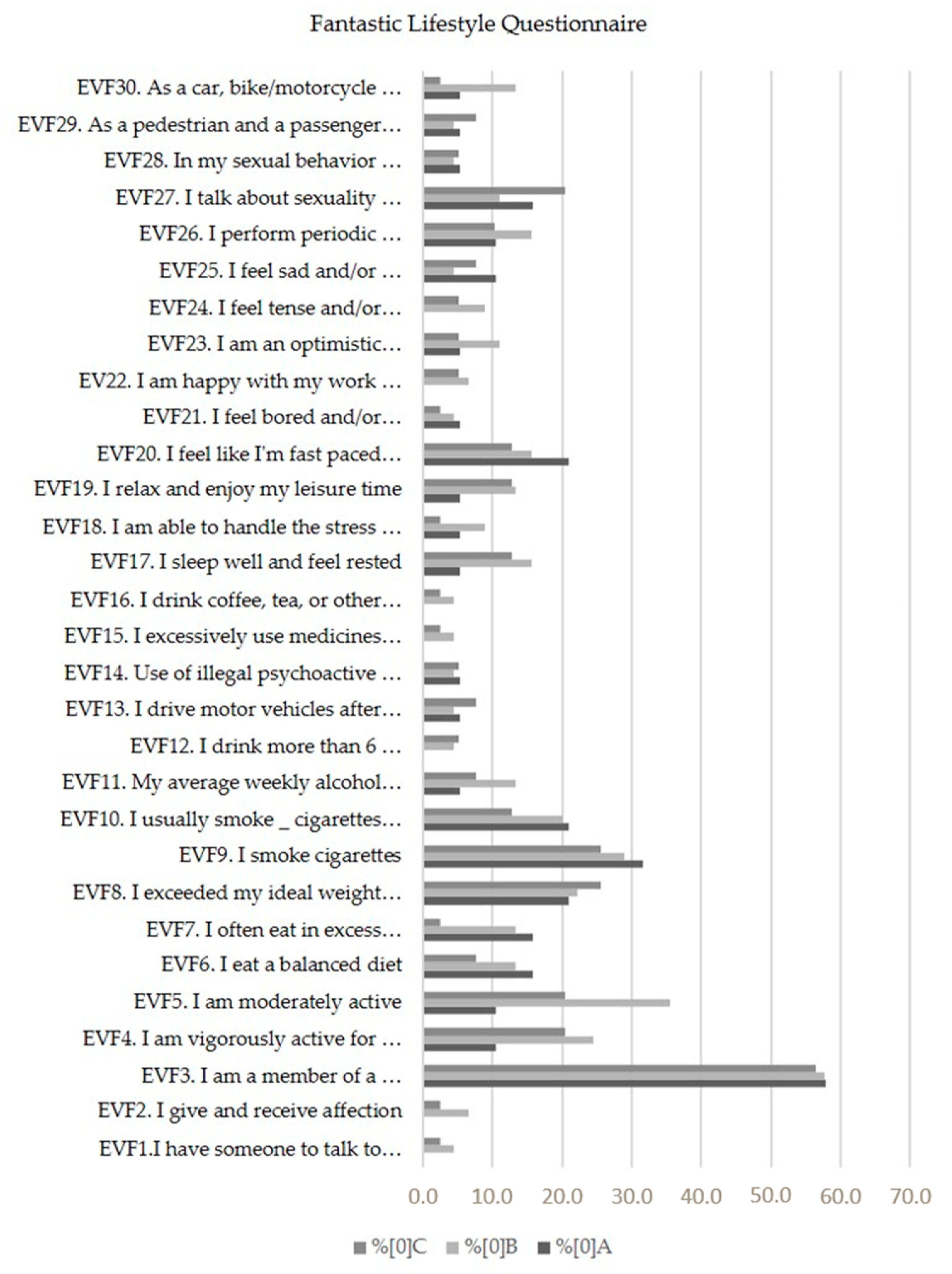
3.2. Phase 2: Epidemiological Assessment
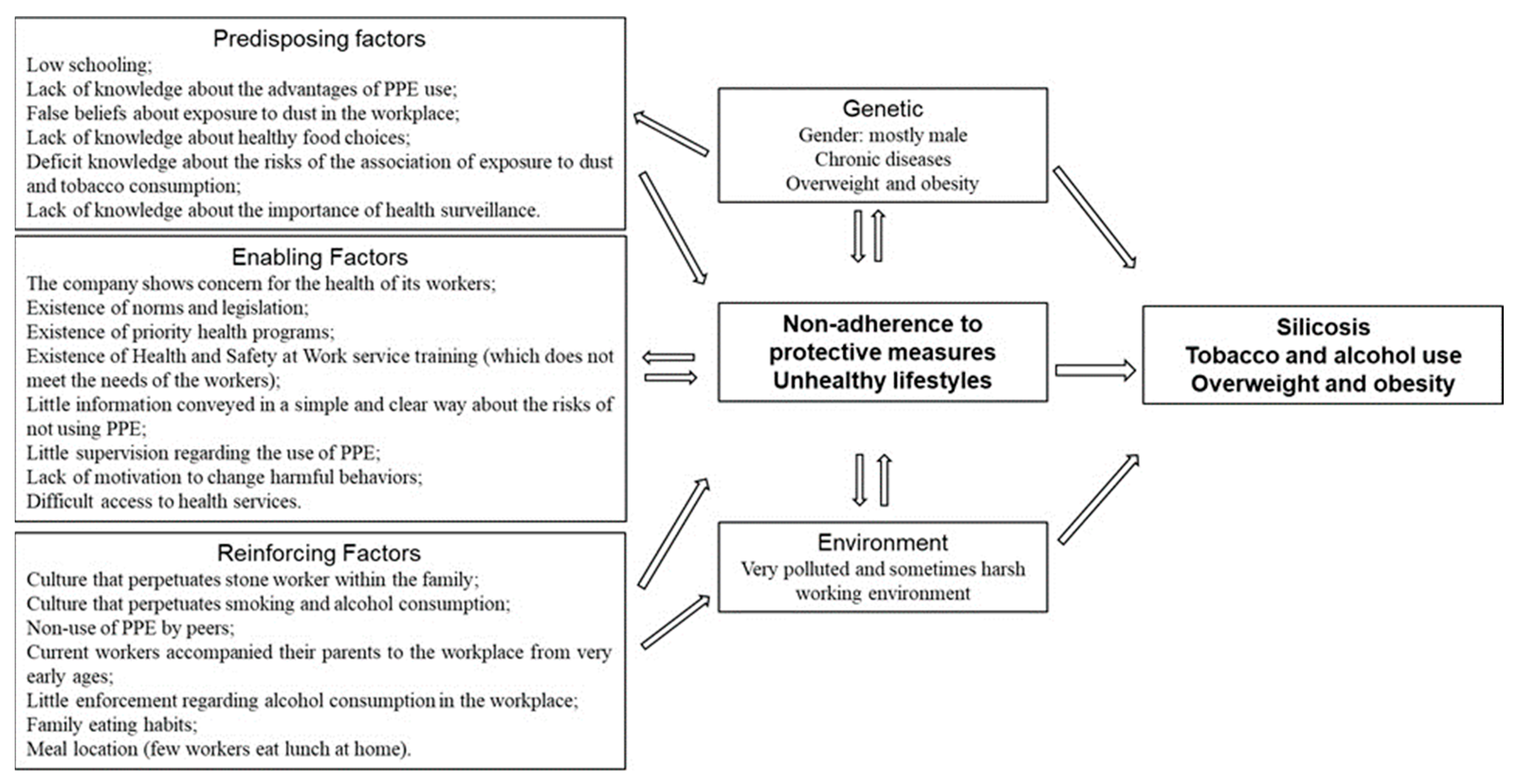
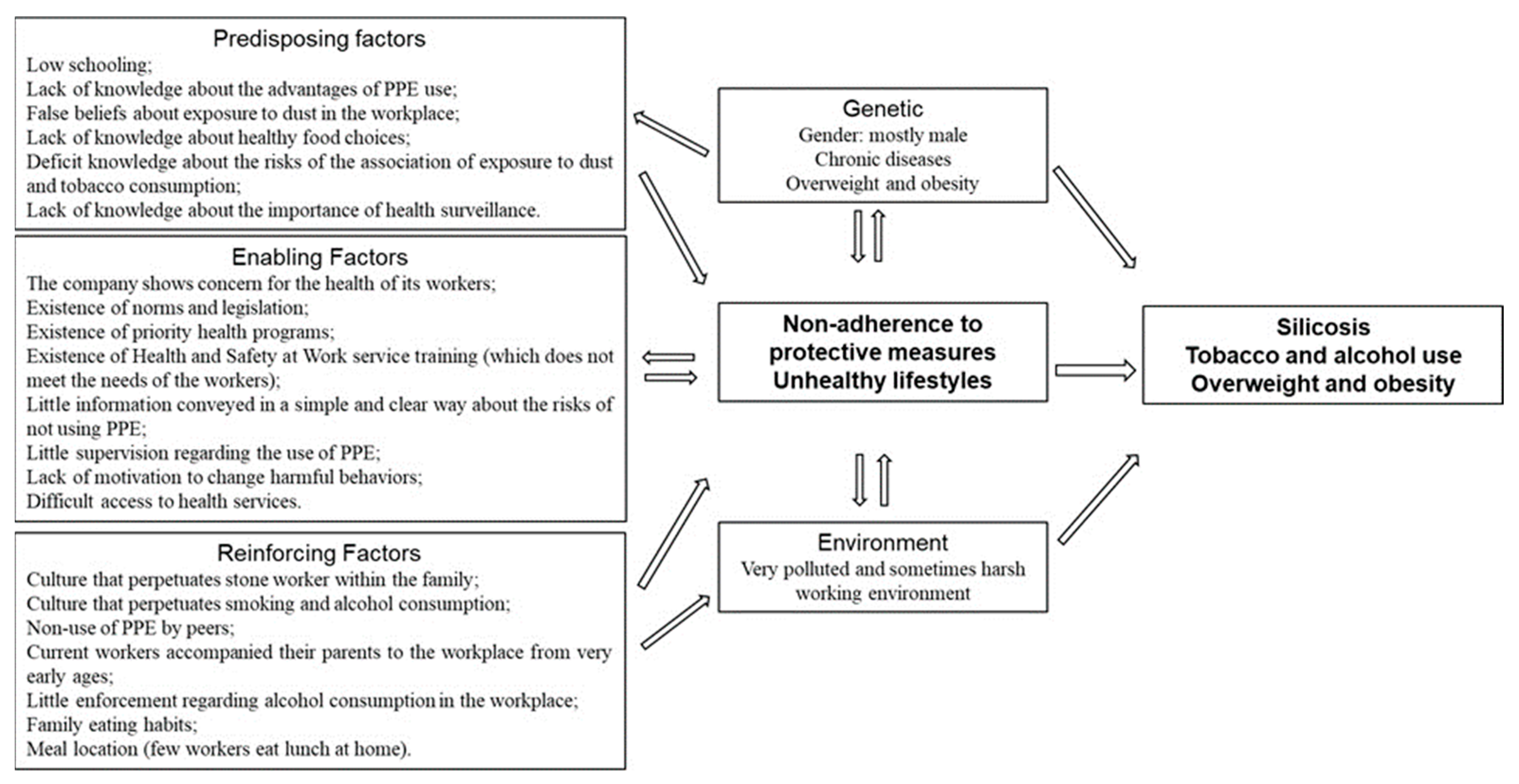
3.3. Phase 3: Educational and Ecological Assessment
3.4. Phase 4: Health Program and Policy Development
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Acknowledgments
Conflicts of Interest
References
- González Caballero, J. Una enfermería del trabajo con perspectiva holística. Arch. Prev. Riesgos Labor. 2021, 24, 175–184. [Google Scholar] [CrossRef] [PubMed]
- DGS. Programa Nacional de Saúde Ocupacional (PNSOC) Extensão 2018–2020. Lisboa. 2018. Available online: www.dgs.pt (accessed on 13 October 2023).
- Programa Nacional para a Tuberculose. Relatório de Vigilância e Monitorização da Tuberculose em Portugal dados Definitivos 2020; DGS: Lisboa, Portugal, 2022. [Google Scholar]
- Carvalho Sousa, S.; Magalhães Alves, C.; Santos, S.; Marques, F.; Duarte, R.; Gonçalves, G.; Carvalho, C. Tuberculosis: Where and how fast are stone quarry workers infected? Eur. J. Public Health 2020, 30 (Suppl. S5), v292–v293. [Google Scholar] [CrossRef]
- MTSSS. DL no 71/2018 de 31 de Dezembro. Diário da República, 1.a Série—N.o 59—25 de Março de 2019 Portugal. 2019. Available online: https://files.dre.pt/1s/2019/03/05900/0169901700.pdf (accessed on 26 January 2023).
- WHO. Health Promotion. 2023. Available online: https://www.who.int/health-topics/health-promotion#tab=tab_1 (accessed on 11 December 2023).
- Brito, I. Pesquisa-Ação Participativa na co-Criação de Instituições de Ensino Superior Promotoras de Saúde; Coleção Conscientizar; Palimage: Coimbra, Portugal, 2018. [Google Scholar]
- MTSSS. Segurança e Saúde; Ministry of Labor, Solidarity and Social Security: Lisboa, Portugal, 2022. [Google Scholar]
- Green, L.W.; Carlson Gielen, A.; Ottoson, J.M.; Peterson, D.V.; Kreuter, M.W. Health Program Planning, Implementation, and Evaluation: Creating Behavioral, Environmental, and Policy Change; JHU Press: Baltimore, MD, USA, 2022. [Google Scholar]
- Green, L.W. Toward Cost-Benefit Evaluations of Health Education: Some Concepts, Methods, and Examples. Health Educ. Monogr. 1974, 2 (Suppl. S1), 34–64. [Google Scholar] [CrossRef]
- Kim, J.; Jang, J.; Kim, B.; Lee, K.H. Effect of the PRECEDE-PROCEED model on health programs: A systematic review and meta-analysis. Syst. Rev. 2022, 11, 213. [Google Scholar] [CrossRef] [PubMed]
- Instituto Nacional de Estatística. Objetivos de Desenvolvimento Sustentável—Agenda 2030. Indicadores para Portugal: 2015–2021. 2022; ISSN 2184-2264. ISBN 978-989-25-0603-6. Available online: https://www.ine.pt/xurl/pub/31592402 (accessed on 13 October 2023).
- ICPHR. O que é a Pesquisa-Ação Participativa em Saúde (ICPHR Position Paper 1); International Collaboration for Participatory Health Research: Baltimore, MD, USA, 2013. [Google Scholar]
- Silva, A.M.M.; Brito, I.D.S.; Amado, J.M.D.C. Tradução, adaptação e validação do questionário Fantastic Lifestyle Assessment em estudantes do ensino superior. Ciência Saúde Coletiva 2014, 19, 1901–1909. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, P.L.; Ferreira, L.N.; Pereira, L.N. Contributos para a Validação da Versão Portuguesa do EQ-5D Contribution for the Validation of the Portuguese Version of EQ-5D. 2013. Available online: www.actamedicaportuguesa.com (accessed on 4 June 2022).
- Bardin, L. Análise de Conteúdo, 70th ed.; Presses Universitaires de France: Paris, France, 1977. [Google Scholar]
- WHO. International Classification of Diseases 11th Revision. 2022. Available online: https://icd.who.int/en (accessed on 13 October 2023).
- WHO. Obesity and Overweight. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 13 October 2023).
- Pedro, A.R.; Amaral, O.; Escoval, A. Literacia em saúde, dos dados à ação: Tradução, validação e aplicação do European Health Literacy Survey em Portugal. Rev. Port. Saude Publica 2016, 34, 259–275. [Google Scholar] [CrossRef]
- Ayaz, M.; Jehan, N.; Nakonieczny, J.; Mentel, U.; uz zaman, Q. Health costs of environmental pollution faced by underground coal miners: Evidence from Balochistan, Pakistan. Resour. Policy 2022, 76, 102536. [Google Scholar] [CrossRef]
- Glenview, I. Silicosis: Ominous Resurgence of an Occupational Lung Condition Reported. 2020. Available online: https://www.elsevier.com/about/press-releases/research-and-journals/silicosis-ominous-resurgence-of-an-occupational-lung-condition-reported (accessed on 7 May 2023).
- OCDE/Observatório Europeu dos Sistemas e Políticas de Saúde. Estado da Saúde na UE Portugal: Perfil de Saúde do País; OCDE: Paris, France, 2021. [Google Scholar]
- Tokgozoglu, L.; Hekimsoy, V.; Costabile, G.; Calabrese, I.; Riccardi, G. Diet, Lifestyle, Smoking. In Prevention and Treatment of Atherosclerosis: Improving State-of-the-Art Management and Search for Novel Targets; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar]
- DGS. Portugal-The Nation’s Health 1990–2016. 2018. Available online: https://comum.rcaap.pt/bitstream/10400.26/22502/1/Portugal-The%20Nation%27s%20Health%201990-2016.pdf (accessed on 25 January 2023).
- Taylor, G.M.J.; Lindson, N.; Farley, A.; Leinberger-Jabari, A.; Sawyer, K.; te Water Naudé, R.; Theodoulou, A.; King, N.; Burke, C.; Aveyard, P. Cochrane review finds stopping smoking is linked to improved mental health. Saudi Med. J. 2021, 42, 459–460. Available online: https://newsroom.wiley.com/press-releases/press-release-details/2021/Cochrane-Review-finds-stopping-smoking-is-linked-to-improved-mental-health/default.aspx (accessed on 26 January 2023).
- Correia, A.M.; Antunes, D.; Ramos, E.; Nogueira, J.R.; Castro, L.; Azevedo, M.; Frutuoso, M.A.; Neto, M. Relatório Saúde na Região Norte Medir para Mudar; Centro Regional de Saúde Pública do Norte: Porto, Portugal, 2005; 245536/06. [Google Scholar]
- GEP/MTSSS. Segurança e Saúde no Trabalho; Gabinete de Estratégia e Planeamento: Lisboa, Portugal, 2022. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alves, C.M.; Morais, C.; Alves, F.; Magalhães, D.; Gonçalves, G.; Brito, I. Community-Based Action Research Intervention to Promote Occupational Health Nursing of Portuguese Quarry Workers. Nurs. Rep. 2024, 14, 390-399. https://doi.org/10.3390/nursrep14010030
Alves CM, Morais C, Alves F, Magalhães D, Gonçalves G, Brito I. Community-Based Action Research Intervention to Promote Occupational Health Nursing of Portuguese Quarry Workers. Nursing Reports. 2024; 14(1):390-399. https://doi.org/10.3390/nursrep14010030
Chicago/Turabian StyleAlves, Catarina Magalhães, Carminda Morais, Filipe Alves, Diogo Magalhães, Guilherme Gonçalves, and Irma Brito. 2024. "Community-Based Action Research Intervention to Promote Occupational Health Nursing of Portuguese Quarry Workers" Nursing Reports 14, no. 1: 390-399. https://doi.org/10.3390/nursrep14010030
APA StyleAlves, C. M., Morais, C., Alves, F., Magalhães, D., Gonçalves, G., & Brito, I. (2024). Community-Based Action Research Intervention to Promote Occupational Health Nursing of Portuguese Quarry Workers. Nursing Reports, 14(1), 390-399. https://doi.org/10.3390/nursrep14010030