
The Early Mobilization of Patients on Extracorporeal Membrane Oxygenation: A Systematic Review

 and
and
Abstract
1. Introduction
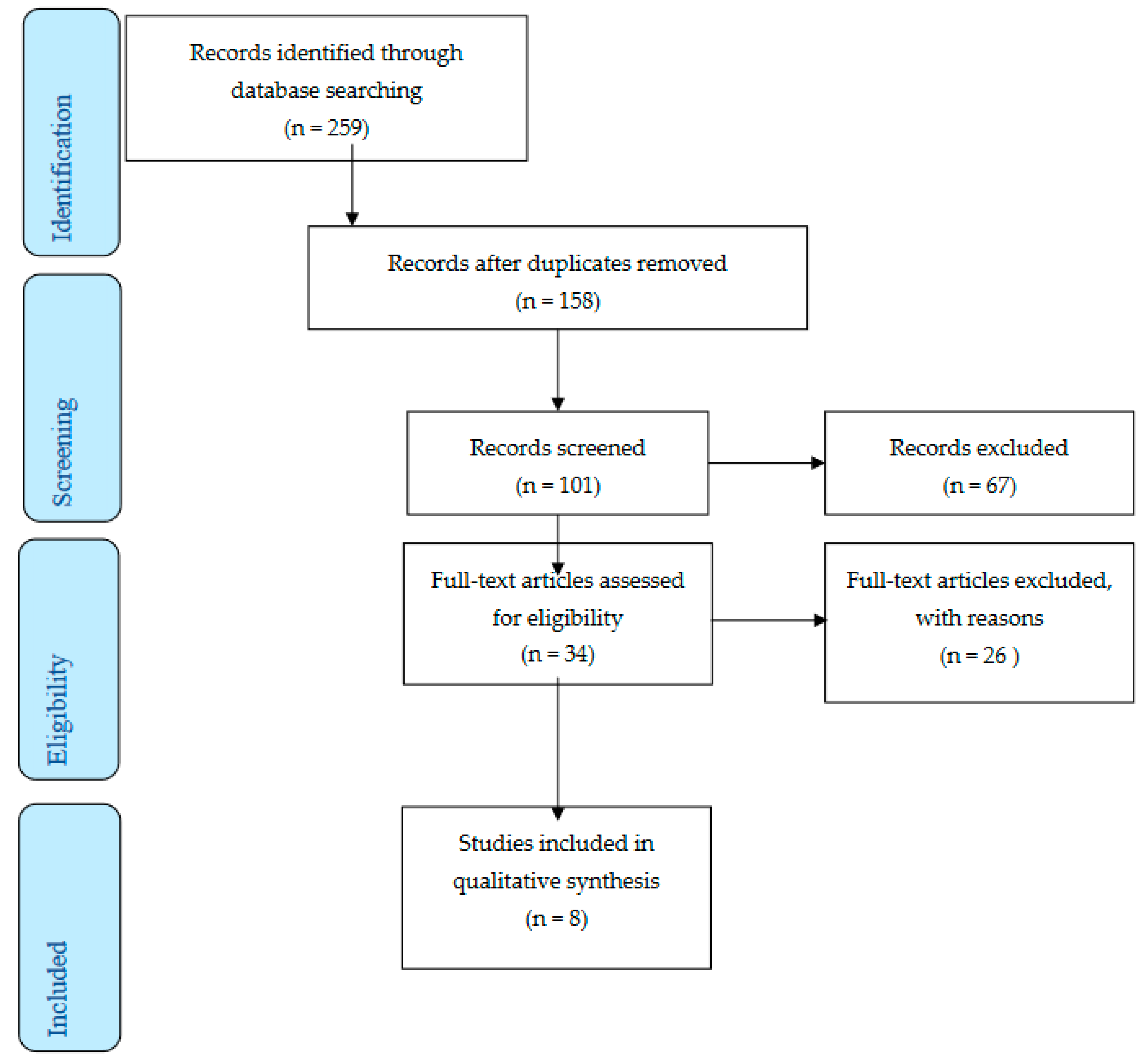
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abrams, D.; Combes, A.; Brodie, D. Extracorporeal membrane oxygenation in cardiopulmonary disease in adults. J. Am. Coll. Cardiol. 2014, 63, 2769–2778. [Google Scholar] [CrossRef] [PubMed]
- Allen, S.; Holena, D.; McCunn, M.; Kohl, B.; Sarani, B. A review of the fundamental principles and evidence base in the use of extracorporeal membrane oxygenation (ECMO) in critically ill adult patients. J. Intensive Care Med. 2011, 26, 13–26. [Google Scholar] [CrossRef] [PubMed]
- Fan, E.; Dowdy, D.W.; Colantuoni, E.; Mendez-Tellez, P.A.; Sevransky, J.E.; Shanholtz, C.; Himmelfarb, C.R.; Desai, S.V.; Ciesla, N.; Herridge, M.S.; et al. Physical complications in acute lung injury survivors: A two-year longitudinal prospective study. Crit. Care Med. 2014, 42, 849–859. [Google Scholar] [CrossRef] [PubMed]
- Hayes, K.; Holland, A.E.; Pellegrino, V.A.; Leet, A.S.; Fuller, L.M.; Hodgson, C.L. Physical function after extracorporeal membrane oxygenation in patients pre or post heart transplantation—An observational study. Heart Lung 2016, 45, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Todd, E.M.; Biswas Roy, S.; Hashimi, A.S.; Serrone, R.; Panchanathan, R.; Kang, P.; Varsch, K.E.; Steinbock, B.E.; Huang, J.; Omar, A.; et al. Extracorporeal membrane oxygenation as a bridge to lung transplantation: A single-center experience in the present era. J. Thorac. Cardiovasc. Surg. 2017, 154, 1798–1809. [Google Scholar] [CrossRef]
- Weill, D.; Benden, C.; Corris, P.A.; Dark, J.H.; Davis, R.D.; Keshavjee, S.; Lederer, D.J.; Mulligan, M.J.; Patterson, G.A.; Singer, L.G.; et al. A consensus document for the selection of lung transplant candidates: 2014—an update from the Pulmonary Transplantation Council of the International Society for Heart and Lung Transplantation. J. Heart Lung Transplant. Off. Publ. Int. Soc. Heart Transplant. 2015, 34, 1–15. [Google Scholar] [CrossRef]
- Abrams, D.; Brodie, D.; Arcasoy, S.M. Extracorporeal Life Support in Lung Transplantation. Clin. Chest Med. 2017, 38, 655–666. [Google Scholar] [CrossRef]
- Marhong, J.D.; DeBacker, J.; Viau-Lapointe, J.; Munshi, L.; Del Sorbo, L.; Burry, L.; Fan, E.; Mehta, S. Sedation and Mobilization During Venovenous Extracorporeal Membrane Oxygenation for Acute Respiratory Failure: An International Survey. Crit. Care Med. 2017, 45, 1893–1899. [Google Scholar] [CrossRef]
- Wells, C.L.; Forrester, J.; Vogel, J.; Rector, R.; Tabatabai, A.; Herr, D. Safety and Feasibility of Early Physical Therapy for Patients on Extracorporeal Membrane Oxygenator: University of Maryland Medical Center Experience. Crit. Care Med. 2018, 46, 53–59. [Google Scholar] [CrossRef]
- Sauer, C.M.; Yuh, D.D.; Bonde, P. Extracorporeal membrane oxygenation use has increased by 433% in adults in the United States from 2006 to 2011. ASAIO J. (Am. Soc. Artif. Intern. Organs 1992) 2015, 61, 31–36. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Br. Med. J. (Clin. Res. ed.) 2021, 372, n71. [Google Scholar]
- Abrams, D.; Javidfar, J.; Farrand, E.; Mongero, L.B.; Agerstrand, C.L.; Ryan, P.; Zemmel, D.; Galuskin, K.; Morrone, T.M.; Boerem, P.; et al. Early mobilization of patients receiving extracorporeal membrane oxygenation: A retrospective cohort study. Crit. Care 2014, 18, R38. [Google Scholar] [CrossRef] [PubMed]
- Ko, Y.; Cho, Y.H.; Park, Y.H.; Lee, H.; Suh, G.Y.; Yang, J.H.; Park, C.M.; Jeon, K.; Chung, C.R. Feasibility and Safety of Early Physical Therapy and Active Mobilization for Patients on Extracorporeal Membrane Oxygenation. ASAIO J. (Am. Soc. Artif. Intern. Organs 1992) 2015, 61, 564–568. [Google Scholar] [CrossRef] [PubMed]
- Bain, J.C.; Turner, D.A.; Rehder, K.J.; Eisenstein, E.L.; Davis, R.D.; Cheifetz, I.M.; Zaas, D.W. Economic Outcomes of Extracorporeal Membrane Oxygenation With and Without Ambulation as a Bridge to Lung Transplantation. Respir. Care 2016, 61, 1–7. [Google Scholar] [CrossRef]
- Munshi, L.; Kobayashi, T.; DeBacker, J.; Doobay, R.; Telesnicki, T.; Lo, V.; Cote, N.; Cypel, M.; Keshavjee, S.; Ferguson, N.D.; et al. Intensive Care Physiotherapy during Extracorporeal Membrane Oxygenation for Acute Respiratory Distress Syndrome. Ann. Am. Thorac. Soc. 2017, 14, 246–253. [Google Scholar] [CrossRef]
- Hayes, K.; Hodgson, C.L.; Pellegrino, V.A.; Snell, G.; Tarrant, B.; Fuller, L.M.; Holland, A.E. Physical Function in Subjects Requiring Extracorporeal Membrane Oxygenation Before or After Lung Transplantation. Respir. Care 2018, 63, 194–202. [Google Scholar] [CrossRef]
- Bonizzoli, M.; Lazzeri, C.; Drago, A.; Tadini Boninsegni, L.; Donati, M.; Di Valvasone, S.; Pesenti, A.; Peris, A. Effects of a physiotherapic program in patients on veno-venous extracorporeal membrane oxygenation: An 8-year single-center experience. Minerva Anestesiol. 2019, 85, 989–994. [Google Scholar] [CrossRef]
- Hayes, K.; Holland, A.E.; Pellegrino, V.A.; Young, M.; Paul, E.; Hodgson, C.L. Early rehabilitation during extracorporeal membrane oxygenation has minimal impact on physiological parameters: A pilot randomised controlled trial. Aust. Crit. Care Off. J. Confed. Aust. Crit. Care Nurses 2021, 34, 217–225. [Google Scholar] [CrossRef]
- Javidfar, J.; Brodie, D.; Wang, D.; Ibrahimiye, A.N.; Yang, J.; Zwischenberger, J.B.; Sonett, J.; Bacchetta, M. Use of bicaval dual-lumen catheter for adult venovenous extracorporeal membrane oxygenation. Ann. Thorac. Surg. 2011, 91, 1763–1769. [Google Scholar] [CrossRef]
- Wang, D.; Zhou, X.; Liu, X.; Sidor, B.; Lynch, J.; Zwischenberger, J.B. Wang-Zwische double lumen cannula-toward a percutaneous and ambulatory paracorporeal artificial lung. ASAIO J. (Am. Soc. Artif. Intern. Organs 1992) 2008, 54, 606–611. [Google Scholar] [CrossRef]
- Shafii, A.E.; McCurry, K.R. Subclavian insertion of the bicaval dual lumen cannula for venovenous extracorporeal membrane oxygenation. Ann. Thorac. Surg. 2012, 94, 663–665. [Google Scholar] [CrossRef] [PubMed]
- Javidfar, J.; Brodie, D.; Costa, J.; Miller, J.; Jurrado, J.; LaVelle, M.; Newmark, A.; Takayama, H.; Sonett, J.R.; Bacchetta, M. Subclavian artery cannulation for venoarterial extracorporeal membrane oxygenation. ASAIO J. (Am. Soc. Artif. Intern. Organs 1992) 2012, 58, 494–498. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors/Year | Country | Type | N | Intervention | Results |
|---|---|---|---|---|---|
| Abrams et al. [12]/2014 | USA | Retrospective cohort study | 35 | Group 1: patients on ECMO as a bridge to transplant (N = 19) Group 2: patients on ECMO as a bridge to recovery (Ν = 16) |
|
| Ko et al. [13]/2015 | South Korea | Retrospective single-center study | 8 | One group on ECMO |
|
| Bain et al. [14]/2016 | USA | Single-center retrospective cohort study | 9 | Group 1: exercise training (Ν = 5) Group 2: usual care (Ν = 4) |
|
| Wells et al. [9]/2017 | USA | Retrospective cohort study | 254 | Group 1: exercise training group (Ν = 167) Group 2: usual care (Ν = 87) |
|
| Munshi et al. [15]/2017 | Canada | Retrospective cohort study | 107 | Group 1: exercise training (N = 50) Group 2: usual care (N = 11) |
|
| Hayes et al. [16]/2018 | Australia | Retrospective single-center study | 42 | Group 1: patients on ECMO (N = 17) Group 2: patients without ECMO (N = 25) |
|
| Bonizzoli et al. [17]/2019 | Italy | Retrospective observational study | 101 | Group 1: physiotherapy within the 1st week from ECMO (N = 33) Group 2: physiotherapy after the 1st week from ECMO (N = 68) |
|
| Hayes et al. [18]/2021 | Australia | A multicenter randomized controlled study | 15 | Group 1: cardiac rehabilitation moderate intense (N = 7) Group 2: usual care (N = 8) |
|
| Authors/Year | Diagnosis | Group | Results |
|---|---|---|---|
| Abrams et al. [12]/2014 | Refractory respiratory or cardiac failure | Bridge to recovery N = 19 | ECMO blood flow rate pre-PT (LPM, mean ± SD): 3.00 ± 0.99 ECMO blood flow rate during PT (LPM, mean ± SD): 2.92 ± 1.09 ECMO sweep gas flow rate pre-PT (LPM, mean ± SD): 2.39 ± 1.77 ECMO sweep gas flow rate during PT (LPM, mean ± SD): 2.35 ± 1.78 Dose of norepinephrine (mcg/min, median, IQR): 1.3 (0.5 to 2) Dose of vasopressin (units/min): 0.04 Maximum distance ambulated (ft, median, IQR): 170 (55 to 525) |
| Bridge to transplant Ν = 16 | ECMO blood flow rate pre-PT (LPM, mean ± SD): 2.99 ± 0.81 ECMO blood flow rate during PT (LPM, mean ± SD): 3.02 ± 0.82 ECMO sweep gas flow rate pre-PT (LPM, mean ± SD): 3.45 ± 1.71 ECMO sweep gas flow rate during PT (LPM, mean ± SD): 3.46 ± 1.71 Dose of norepinephrine (mcg/min, median, IQR): 3.5 (1.3 to 5) Dose of vasopressin (units/min): 0.04 Maximum distance ambulated (ft, median, IQR): 195 (60 to 398) | ||
| Ko et al. [13]/2015 | Unknown | Bridge to transplantation Ν = 8 | Blood flow before PT: 2.93 ± 0.93 During PT: 3.02 ± 0.90 Sweep gas flow before PT: 4.89 ± 1.78 During PT: 4.90 ± 1.78 |
| Bain et al. [14]/2016 | Unknown | Bridge to transplantation Non-rehabilitation group N = 4 | Pre-transplant: $52,124 ($23,824–69,929) Post-transplant ICU: $143,407 ($112,199–168,993) Post-ICU through discharge: $143,407 ($112,199–168,993) Total hospital: $273,291 ($237,299–374,175) Total: $300,307 ($274,262–394,913) Pre-transplant ICU stay: 12 (4–41) Pre-transplant mechanical ventilation duration: 1 (1–5) Post-transplant mechanical ventilation duration: 29.5 (22–54) Post-transplant ICU stay: 45 (34–56) Post-ICU to discharge stay: 34 (11–63) Total hospital stay: 94 (51–151) ECMO support: 1.5 (1–9) |
| Bridge to transplantation Rehabilitation group N = 5 | Pre-transplant: $98,460 ($38,589–122,111) Post-transplant ICU: $43,929 ($23,611–64,126) Post-ICU through discharge: $15,544 ($11,499–43,870) Total hospital: $209,590 ($166,767–264,536) Total: $244,508 ($219,972–268,914) Pre-transplant ICU stay: 20 (17–30) Pre-transplant mechanical ventilation duration: 12 (5–15) Post-transplant mechanical ventilation duration: 2 (1–5) Post-transplant ICU stay: 8 (6–22) Post-ICU to discharge stay: 11 (7–25) Total hospital stay: 50 (31–63) ECMO support: 9 (5–14) | ||
| Wells et al. [9]/2017 | Unknown | Bridge to transplantation Total N = 254 | Discharge outcomes, N (%) Home: 34 (13.38) Rehabilitation facility: 96 (37.79) Skilled nursing: 10 (2.82) Acute care facility: 5 (1.96) |
| Bridge to transplantation Physical therapy group N = 167 | Discharge outcomes, N (%) Home: 26 (15.56) Rehabilitation facility: 75 (44.91) Skilled nursing: 4 (2.39) Acute care facility: 4 (2.39) | ||
| Munshi et al. [15]/2017 | ARDS | N = 61 | Days on ECMO: 12 (9–19) Duration of mechanical ventilation: 21 (18–34) ICU mortality: 18 (30) In hospital mortality: 18 (30) Complications on ECMO Barotrauma: 4 (7) Limb ischemia: 1 (2) Intracerebral hemorrhage: 1 (2) Heparin induced thrombocytopenia: 4 (7) Air embolism: 1 (2) |
| Hayes et al. [16]/2018 | Cystic fibrosis/bronchiectasis, COPD, asthma, and obliterative bronchiolitis, Pulmonary hypertension, Pulmonary fibrosis, Re-transplant | ΕCMO Ν = 42 | Physical function IMS ICU at discharge: 6 (5–7) IMS at hospital discharge: 10 (9–10) 6MWD at hospital discharge, m: 285 ± 112 6MWD at 3 months, m: 541 ± 133 Discharge destination, N (%) Home: 12 (85.7) In-patient rehabilitation: 2 (14.3) |
| Non-ECMO N = 28 | Physical function IMS ICU at discharge: 7 (6–8) IMS at hospital discharge: 10 (10–10) 6MWD at hospital discharge, m: 384 ± 93 6MWD at 3 months, m: 584 ± 67 Discharge destination, N (%) Home: 28 (100)) In-patient rehabilitation: 0 (0) | ||
| Bonizzoli et al. [17]/2019 | ARDS | Within the first week mobilization N = 33 | ECMO (days) (median, IQR): 7 (2.5–13.5) MV (days) (median, IQR): 11 (5–17.75) LOS (days) (median, IQR): 12 (7.25–21) In-ICU mortality: 12 |
| After the first week N = 68 | ECMO (days) (median, IQR): 11 (8.75–22) MV (days) (median, IQR): 23 (13.75–33.25) LOS (days) (median, IQR): 25 (18.75–36.25) In-ICU mortality:14 | ||
| Hayes et al. [18]/2021 | ARDS, pots lung or heart transplantation primary graft failure, cardiac arrest, cardiac failure- infraction and pulmonary hypertension after lung transplantation | Mobilization group N = 7 | Hospital outcomes In-hospital mortality: 3 (42.9) ECMO duration (days): 8.1 ± 4.9 ECMO duration for survivors: 10.5 ± 5.5 Ventilation (days): 6.2 ± 2.5 Ventilation for survivors: 7.3 ± 2.8 LOS in the ICU (days): 12.9 (7.2 ± 16.7) LOS in the ICU for survivors: 16.7 (14.6 ± 21.6) LOS in the hospital for survivors: 41.9 (34.3 ± 56.4) Mobility milestones Time to first SOOB (days): 12.6 ± 6.6 Time to first stand (days): 5.5 ± 4.5 Time to first walk (days): 16.1 (11.5 ± 21.0) Discharge destination of survivors Home: 4 (100) Inpatient rehabilitation: 0 (0) Transfer to the local acute hospital: 0 (0) |
| Usual care group Ν = 8 | Hospital outcomes In-hospital mortality: 1 (12.5) ECMO duration (days): 10.9 ± 5.5 ECMO duration for survivors: 11.5 ± 5.7 Ventilation (days): 9.2 ± 3.8 Ventilation for survivors: 9.4 ± 4.1 LOS in the ICU (days): 21.4 (15.5 ± 38.5) LOS in the ICU for survivors: 22.2 (16.2 ± 38.5) LOS in the hospital for survivors: 34.4 (29.3 ± 87.2) Mobility milestones Time to first SOOB (days): 12.5 ± 7.7 Time to first stand (days): 20.8 ± 12.3 Time to first walk (days): 21.9 (16.5±52.4) Discharge destination of survivors Home: 3 (43) Inpatient rehabilitation: 3 (43) Transfer to the local acute hospital: 1 (14) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chatziefstratiou, A.A.; Fotos, N.V.; Giakoumidakis, K.; Brokalaki, H. The Early Mobilization of Patients on Extracorporeal Membrane Oxygenation: A Systematic Review. Nurs. Rep. 2023, 13, 751-764. https://doi.org/10.3390/nursrep13020066
Chatziefstratiou AA, Fotos NV, Giakoumidakis K, Brokalaki H. The Early Mobilization of Patients on Extracorporeal Membrane Oxygenation: A Systematic Review. Nursing Reports. 2023; 13(2):751-764. https://doi.org/10.3390/nursrep13020066
Chicago/Turabian StyleChatziefstratiou, Anastasia A., Nikolaos V. Fotos, Konstantinos Giakoumidakis, and Hero Brokalaki. 2023. "The Early Mobilization of Patients on Extracorporeal Membrane Oxygenation: A Systematic Review" Nursing Reports 13, no. 2: 751-764. https://doi.org/10.3390/nursrep13020066
APA StyleChatziefstratiou, A. A., Fotos, N. V., Giakoumidakis, K., & Brokalaki, H. (2023). The Early Mobilization of Patients on Extracorporeal Membrane Oxygenation: A Systematic Review. Nursing Reports, 13(2), 751-764. https://doi.org/10.3390/nursrep13020066