
The Use of 360-Degree Video in Developing Emotional Coping Skills (Reduced Anxiety and Increased Confidence) in Mental Health Nursing Students: A Protocol Paper


 ,
, {kind=link}
Abstract
:1. Introduction
- (1)
- To provide validation for behaviour or communication and to avoid negative and unhelpful assumptions that may create barriers to engagement;
- (2)
- To engage with the emotional content of what is communicated;
- (3)
- To offer reassurance and to promote a sense of safety;
- (4)
- To take the communication forwards into meaningful activity or to reflect on the interaction.
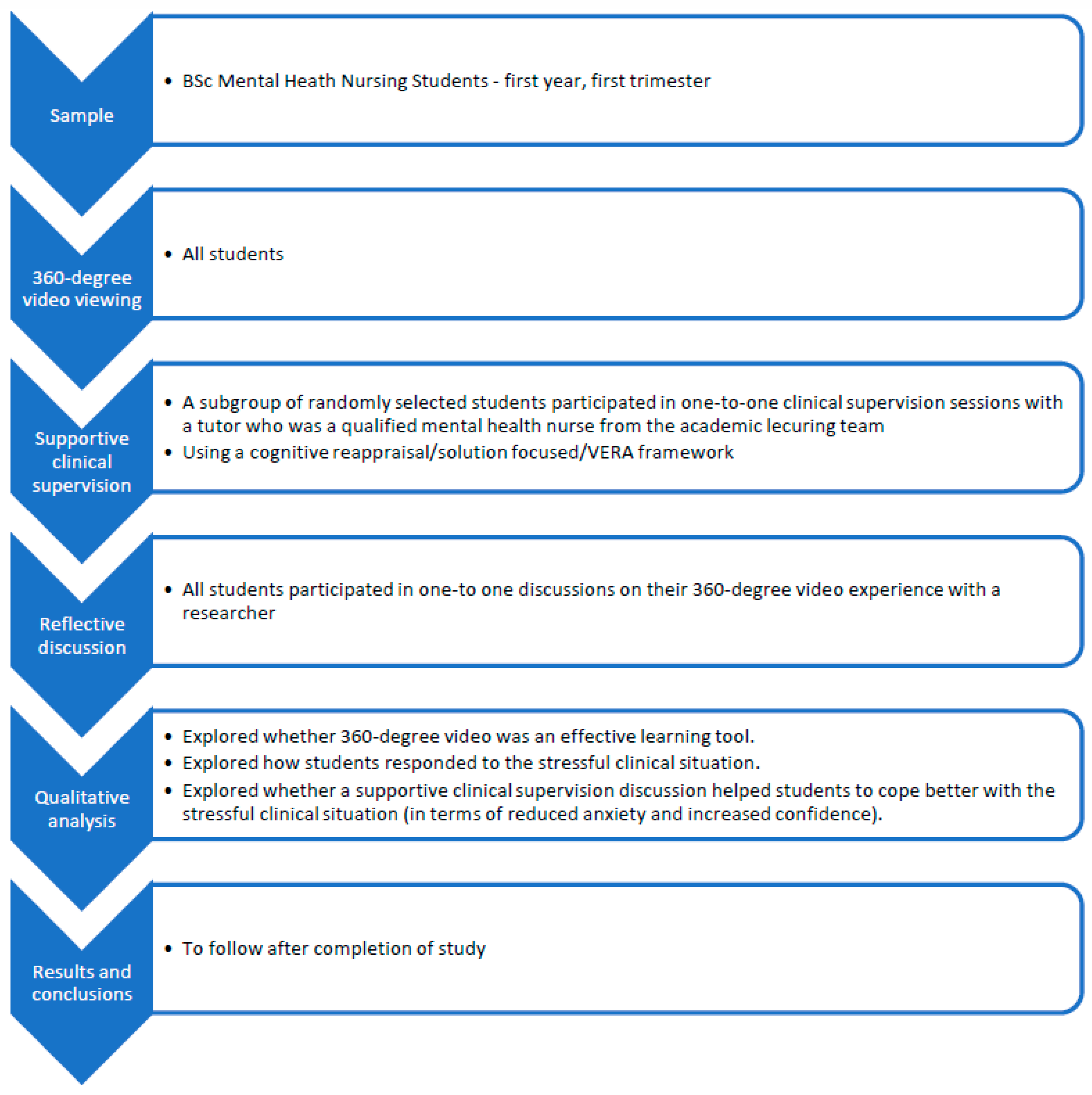
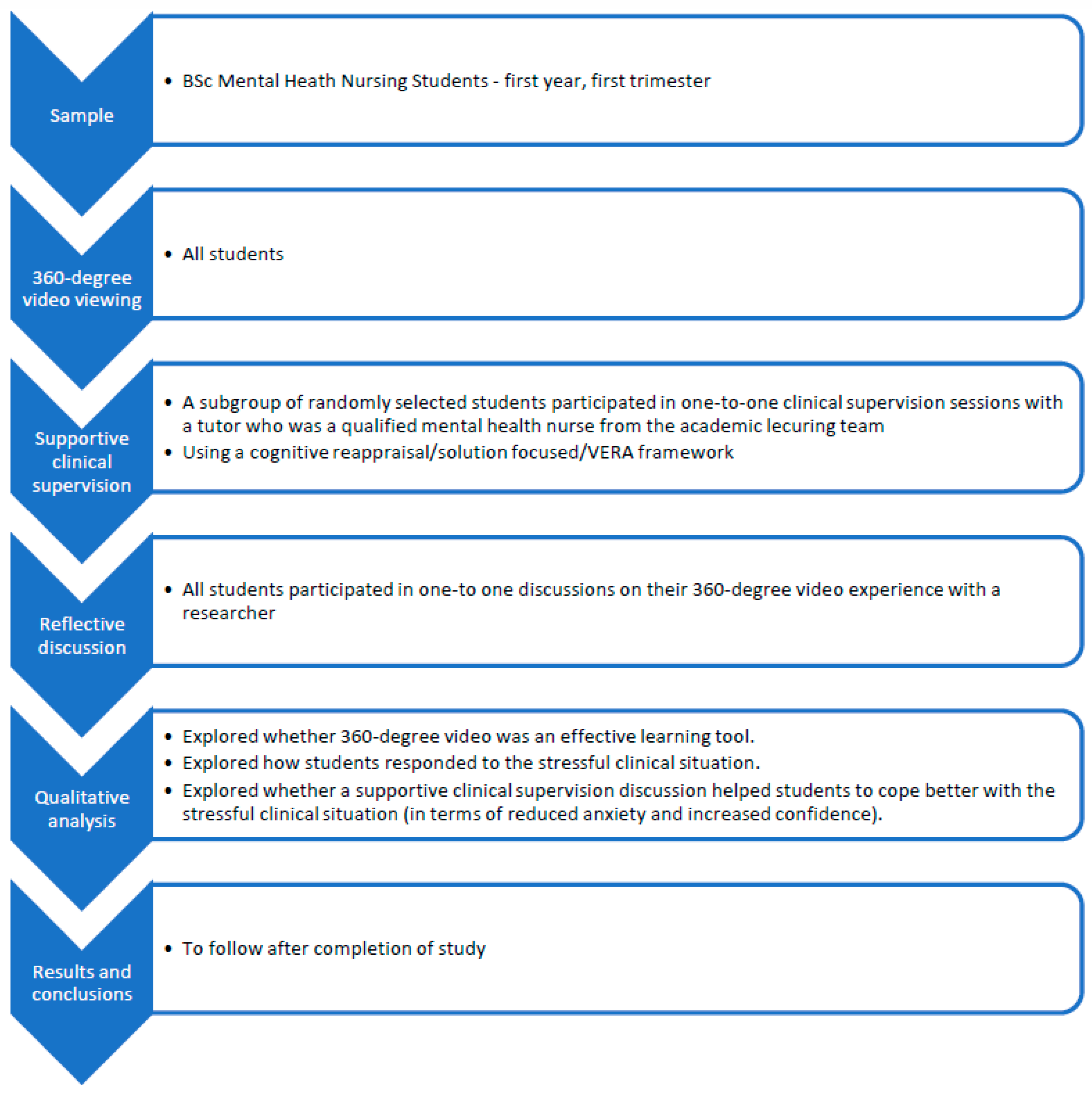
2. Methods
- To evaluate the use of 360-degree video as an educative tool.
- To evaluate whether using a clinical supervision discussion builds confidence and reduces anxiety in relation to stressful clinical interactions, using a combined cognitive reappraisal/solution-focused/VERA framework.
3. Exploring 360-Degree Video as an Educational Tool—All Participants
4. Exploring A Supportive Clinical Supervision Using a Cognitive Reappraisal/Solution-Focused/Vera Framework—With a Subgroup of Participants
- Identify emotions: as part of the process of cognitive reappraisal, the participants will describe how they felt whilst watching the scenario. They will rate the intensity of their emotional responses using a scale from 0 (not intense at all) to 10 (the most intense I have ever felt).
- -
- What is going through my mind as I am feeling this emotion?
- -
- What am I telling myself about this situation?
- -
- What am I afraid might happen?
- -
- How anxious do you feel about this situation on a scale of 0–10?
- -
- What would move your anxiety levels down the scale?
- -
- How confident are you that you would be able to deliver an intervention that would help the service user move on from this situation on a scale of 0–10?
- -
- What would move your confidence levels further up the scale?
- -
- Why might the service user in the video be feeling this way?
- -
- What do you think they are trying to communicate?
- -
- What response might you give to this distressed service user?
- -
- What clinical decisions might you undertake based on the scenario?
5. Qualitative Data Analyses
- Whether pre-registration mental health nursing students consider 360-degree video to be an effective learning tool.
- How pre-registration nursing students interpret and respond to stressful clinical situations.
- Whether working through a process of cognitive appraisal and clinical supervision (to introduce concepts of SFBT and the VERA framework) helped students to cope better with a stressful interaction (in terms of reduced anxiety and increased confidence).
6. How the Research Will Be Communicated to the Wider Community/Research Outputs
7. Ethical Considerations
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A
Appendix B
- Reappraisal Task Worksheet
- Thank you for participating in this task. You will be shown a 360-degree experiential video. The scenario depicts an interaction between you, the viewer, and a service user called Mary. She will interact with you and others on the ward.
- Scenario
- How would you describe the difficult or stressful experience that you have just viewed? One sentence is sufficient.
- 2.
- Feelings
- Describe the feelings/emotions that you felt during the experience
- A. Limit your description to the a few words or phrases that best describe the feelings.
- B. Record the intensity of the feelings. Use a scale from 0 (no feelings) to 10 (very intense feelings).
- How intense were your feelings during the experience?_________
- How intense are your feelings about the experience now?_______
- How anxious did you feel when viewing this situation?__________
- What would have moved your anxiety levels down the scale?
- 3.
- Thoughts
- A. As you were viewing the scenario, what was going through your mind?
- Consider the following:
- How did I look at this experience?
- What did it mean to me?
- What did it mean about me/my imminent future?
- B. As you were feeling the emotion, (stated above), what was going through your mind?
- Consider the following:
- What were you telling yourself about the situation?
- What were you afraid might happen?
- SCALING
- Taking your thoughts and feelings into consideration, how reasonable does your view seem? Use a scale from 0 (not reasonable) to 10 (very reasonable)_______________________________________________
- Now that you have considered your view, how reasonable does it seem? (0–10)______________________________________________________
- How confident are you that you could deliver an intervention that would help the service user move forwards on a scale of 0–10_______________________________________________________
- What would move your confidence levels further up the scale?
- 4.
- Reframing feelings and thoughts using a Solution Focused approach
- Think about a situation in your past where you dealt successfully with an anxiety provoking incident.
- What did you do then to successfully manage the situation?
- What did you say, keep in mind, feel or remember that helped you solve the situation in a positive way?
- What qualities have you shown in life and work that suggest that you can cope well in this sort of situation?
- Think about an individual that you have helped successfully in the past. If they were here, what would they say to you about your skills/abilities to deal with this scenario?
- Knowing your strengths and your life and work experiences so far, what would you do / say in this situation if it happened again?
- How would you help Mary to feel listened to and show her you value her as a whole person?
- What is the emotional content of what Mary is saying in this situation?
- What do you think she is feeling?
- If you had to reassure Mary and give her some sort of positive compliment what would that be?
- How could you and Mary work together to address her concerns and to keep the conversation going?
- NOW RE-WATCH THE VIDEO
- RE-SCALING
- How do you feel about the experience now after considering these points-of-view?
- If you consider your thoughts and feelings about the scenario now, how reasonable were your initial views? Use a scale from 0 (not reasonable) to 10 (very reasonable).__________________________
- How anxious do you now feel about this situation on a scale of 0–10?______________________________________________________
- How confident are you now that you would be able to deliver an intervention that would help Mary move on from this situation on a scale of 0–10?___________________________________________________
- Qualitative questions about the 360-degree experience
- With these questions, we are not testing your knowledge. We are only interested in your opinion. There is no right answer. It is not a test/nor does it form any part of your assessment…….
- In the video, the service user is talking to someone. In your view, who was that person?
- How did you relate with/to the interaction?
- How able were you to relate to the service user?
- How did you feel overall about the 360-degree video experience?
- What emotions were evoked for you, when watching the video?
- Can you describe how you felt whilst watching the video?
- How realistic did you think the video was?
- Can you elaborate on your relationship with what was happening in the scenario?
References
- Thompson, D.; O’Leary, K.; Jensen, E.; Scott-Findlay, S.; O’Brien-Pallas, L.; Estabrooks, C. The relationship between busyness and research utilization: It is about time. J. Clin. Nurs. 2008, 17, 539–548. [Google Scholar] [CrossRef] [PubMed]
- Yadav, B.; Fealy, G. Irish psychiatric nurses’ self-reported barriers, facilitators and skills for developing evidence-based practice. J. Psychiatr. Ment. Health Nurs. 2012, 19, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Brennan, G.; Flood, C.; Bowers, L. Constraints and blocks to change and improvement on acute psychiatric wards—Lessons from the City Nurses project. J. Psychiatr. Ment. Health Nurs. 2006, 13, 475–482. Available online: https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1365-2850.2006.00956.x (accessed on 12 March 2021). [CrossRef] [PubMed]
- McVicar, A. Scoping the common antecedents of job stress and job satisfaction for nurses (2000–2013) using the job demands–resources model of stress. J. Nurs. Manag. 2016, 24, E112–E136. [Google Scholar] [CrossRef] [PubMed]
- Laker, C.; Rose, D.; Flach, C.; Csipke, E.; McCrone, P.; Craig, T.; Kelland, H.; Wykes, T. Views of the Therapeutic Environment (VOTE): Stakeholder involvement in measuring staff perceptions of acute in-patient care. Int. J. Nurs. Stud. 2012, 49, 1403–1410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rose, D.; Evans, E.; Laker, C.; Wykes, T. Life in acute mental health settings: Experiences and perceptions of service users and nurses. Epidemiol. Psychiatr. Sci. 2015, 24, 90–96. [Google Scholar] [CrossRef] [Green Version]
- Currid, T. Experiences of stress among nurses in acute mental health settings. Nurs. Stand. 2009, 23, 40–46. [Google Scholar] [CrossRef]
- Laker, C.; Cella, M.; Callard, F.; Wykes, T. Why is change a challenge in acute mental health wards? A cross-sectional investigation of the relationships between burnout, occupational status and nurses’ perceptions of barriers to change. Int. J. Ment. Health Nurs. 2018, 28, 190–198. Available online: https://www.ncbi.nlm.nih.gov/pubmed/29993168 (accessed on 12 March 2021). [CrossRef] [Green Version]
- Menzies Lyth, I. Agency, Health and Social Survival: The Ecopolitics of Rival Psychologies; Taylor and Francis: London, UK, 1998. [Google Scholar]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Nachdr, Ed.; Springer: New York, NY, USA, 2006. [Google Scholar]
- Furnes, M.; Kvaal, K.S.; Høye, S. Communication in mental health nursing—Bachelor Students’ appraisal of a blended learning training programme—An exploratory study. BMC Nurs. 2018, 17, 20. [Google Scholar] [CrossRef] [Green Version]
- Turton, W. Honing cognitive behaviour therapy skills through experiential learning. Ment. Health Pract. 2012, 15, 33. Available online: https://search.proquest.com/docview/1030130490 (accessed on 12 March 2021). [CrossRef]
- Gross, J.J. Antecedent- and response-focused emotion regulation: Divergent consequences for experience, expression, and physiology. J. Personal. Soc. Psychol. 1998, 74, 224–237. [Google Scholar] [CrossRef]
- Ochsner, K.N.; Bunge, S.A.; Gross, J.J.; Gabrieli, J.D.E. Rethinking feelings: An fMRI study of the cognitive regulation of emotion. J. Cogn. Neurosci. 2002, 14, 1215–1229. [Google Scholar] [CrossRef] [Green Version]
- Mauss, I.B.; Cook, C.L.; Cheng, J.Y.J.; Gross, J.J. Individual differences in cognitive reappraisal: Experiential and physiological responses to an anger provocation. Int. J. Psychophysiol. 2007, 66, 116–124. [Google Scholar] [CrossRef]
- Folkman, S. Positive psychological states and coping with severe stress. Soc. Sci. Med. 1997, 45, 1207–1221. [Google Scholar] [CrossRef]
- Gross, J.J.; John, O.P. Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. J. Personal. Soc. Psychol. 2003, 85, 348–362. [Google Scholar] [CrossRef]
- Garnefski, N.; Kraaij, V. Relationships between cognitive emotion regulation strategies and depressive symptoms: A comparative study of five specific samples. Personal. Individ. Differ. 2006, 40, 1659–1669. [Google Scholar] [CrossRef]
- Beck, A.T. Cognitive Therapy: Nature and Relation to Behavior Therapy—Republished Article. Behav. Ther. 2016, 47, 776–784. Available online: https://www.clinicalkey.es/playcontent/1-s2.0-S0005789416300910 (accessed on 12 March 2021). [CrossRef]
- De Shazer, S. Putting Difference to Work, 1st ed.; Norton: New York, NY, USA, 1991. [Google Scholar]
- Hawkes, D. Solution Focused Therapy: A Handbook for Health Care Professionals; Butterworth-Heinemann Books: Oxford, UK, 1998. [Google Scholar]
- De Shazer, S.; Dolan, Y. More than Miracles; Haworth Press: New York, NY, USA, 2007. [Google Scholar]
- Hawkes, D. Heidegger undisclosed: Is Heidegger and phenomenology hiding or hidden from Solution Focus? InterAction J. Solut. Focus Organ. 2011, 3, 28–31. [Google Scholar]
- Ratner, H.; George, E.; Iveson, C. Solution Focused Brief Therapy; Routledge: London, UK, 2012. [Google Scholar]
- De Jong, P.; Berg, I.K. Interviewing for Solutions, 4th ed.; Brooks/Cole, Cengage Learning: South Melbourne, Victoria, 2013. [Google Scholar]
- Bond, F.; Dryden, W. Handbook of Brief Cognitive Behaviour Therapy, 1st ed.; Wiley: Hoboken, NJ, USA, 2005. [Google Scholar]
- Barlow, D.; Farchione, T.; Bullis, J.; Gallagher, M.W.; Murray-Latin, H.; Sauer-Zavala, S.; Bentley, K.; Thompson-Hollands, J.; Conklin, L.; Boswell, J.; et al. The Unified Protocol for Transdiagnostic Treatment of Emotional Disorders Compared With Diagnosis-Specific Protocols for Anxiety Disorders: A Randomized Clinical Trial. JAMA Psychiatry 2017, 74, 875–884. [Google Scholar] [CrossRef]
- Miu, A.; Crişan, L. Cognitive reappraisal reduces the susceptibility to the framing effect in economic decision making. Personal. Individ. Differ. 2011, 51, 478–482. Available online: https://www.sciencedirect.com/science/article/pii/S0191886911002200 (accessed on 12 March 2021). [CrossRef]
- Einstein, D. Innovations and Advances in Cognitive Behaviour Therapy, 1st ed.; Australian Academic Press: Brisbane, Australia, 2007. [Google Scholar]
- Blackhall, A.; Hawkes, D.; Hingley, D.; Wood, S. VERA framework: Communicating with people who have dementia. Nurs. Stand. 2011, 26, 35–39. [Google Scholar] [CrossRef]
- Hawkes, D.; Hingley, D.; Wood, S.; Blackhall, A. Evaluating the VERA framework for communication. Nurs. Stand. 2015, 30, 44–48. Available online: https://www.ncbi.nlm.nih.gov/pubmed/26350870 (accessed on 12 March 2021). [CrossRef]
- Trivedi, P.; Wykes, T. From passive subjects to equal partners: Qualitative review of user involvement in research. Br. J. Psychiatry 2003, 181, 468–472. [Google Scholar] [CrossRef]
- Weng, H.; Fox, A.; Shackman, A.; Stodola, D.; Caldwell, J.; Olson, M.; Rogers, G.; Davidson, R. Compassion Training Alters Altruism and Neural Responses to Suffering. Psychol. Sci. 2013, 24, 1171–1180. Available online: https://journals.sagepub.com/doi/full/10.1177/0956797612469537 (accessed on 12 March 2021). [CrossRef] [Green Version]
- Center for Healthy Minds. Tools for Scientists. 2018. Available online: https://centerhealthyminds.org/science/tools-for-scientists (accessed on 12 March 2021).
- Flick, U. An Introduction to Qualitative Research, 4th ed.; Sage Publ: Los Angeles, CA, USA, 2010. [Google Scholar]
- Boyatzis, R. Transforming Qualitative Information; Sage Publ: Thousand Oaks, CA, USA, 1998. [Google Scholar]
- Baxter, L. Content Analysis. In Studying Interpersonal Analysis; Guildford Press: New York, NY, USA, 1991. [Google Scholar]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laker, C.; Knight-Davidson, P.; Hawkes, D.; Driver, P.; Nightingale, M.; Winter, A.; McVicar, A. The Use of 360-Degree Video in Developing Emotional Coping Skills (Reduced Anxiety and Increased Confidence) in Mental Health Nursing Students: A Protocol Paper. Nurs. Rep. 2022, 12, 536-544. https://doi.org/10.3390/nursrep12030052
Laker C, Knight-Davidson P, Hawkes D, Driver P, Nightingale M, Winter A, McVicar A. The Use of 360-Degree Video in Developing Emotional Coping Skills (Reduced Anxiety and Increased Confidence) in Mental Health Nursing Students: A Protocol Paper. Nursing Reports. 2022; 12(3):536-544. https://doi.org/10.3390/nursrep12030052
Chicago/Turabian StyleLaker, Caroline, Pamela Knight-Davidson, David Hawkes, Paul Driver, Maxine Nightingale, Ann Winter, and Andrew McVicar. 2022. "The Use of 360-Degree Video in Developing Emotional Coping Skills (Reduced Anxiety and Increased Confidence) in Mental Health Nursing Students: A Protocol Paper" Nursing Reports 12, no. 3: 536-544. https://doi.org/10.3390/nursrep12030052
APA StyleLaker, C., Knight-Davidson, P., Hawkes, D., Driver, P., Nightingale, M., Winter, A., & McVicar, A. (2022). The Use of 360-Degree Video in Developing Emotional Coping Skills (Reduced Anxiety and Increased Confidence) in Mental Health Nursing Students: A Protocol Paper. Nursing Reports, 12(3), 536-544. https://doi.org/10.3390/nursrep12030052