
Psychometric Properties of the Caring Behaviors Inventory-16 in Ethiopia

 ,
,
Abstract
:1. Background
2. Methods and Materials
2.1. The Caring Behaviors Inventory-16
2.2. Translation and Cultural Adaptation of the CBI-16
2.3. Design and Setting
2.4. Participants
2.5. Data Collection
2.6. Patient Satisfaction Instrument
2.7. Data Collection Procedure
2.8. Data Quality Control
2.9. Statistical Analysis
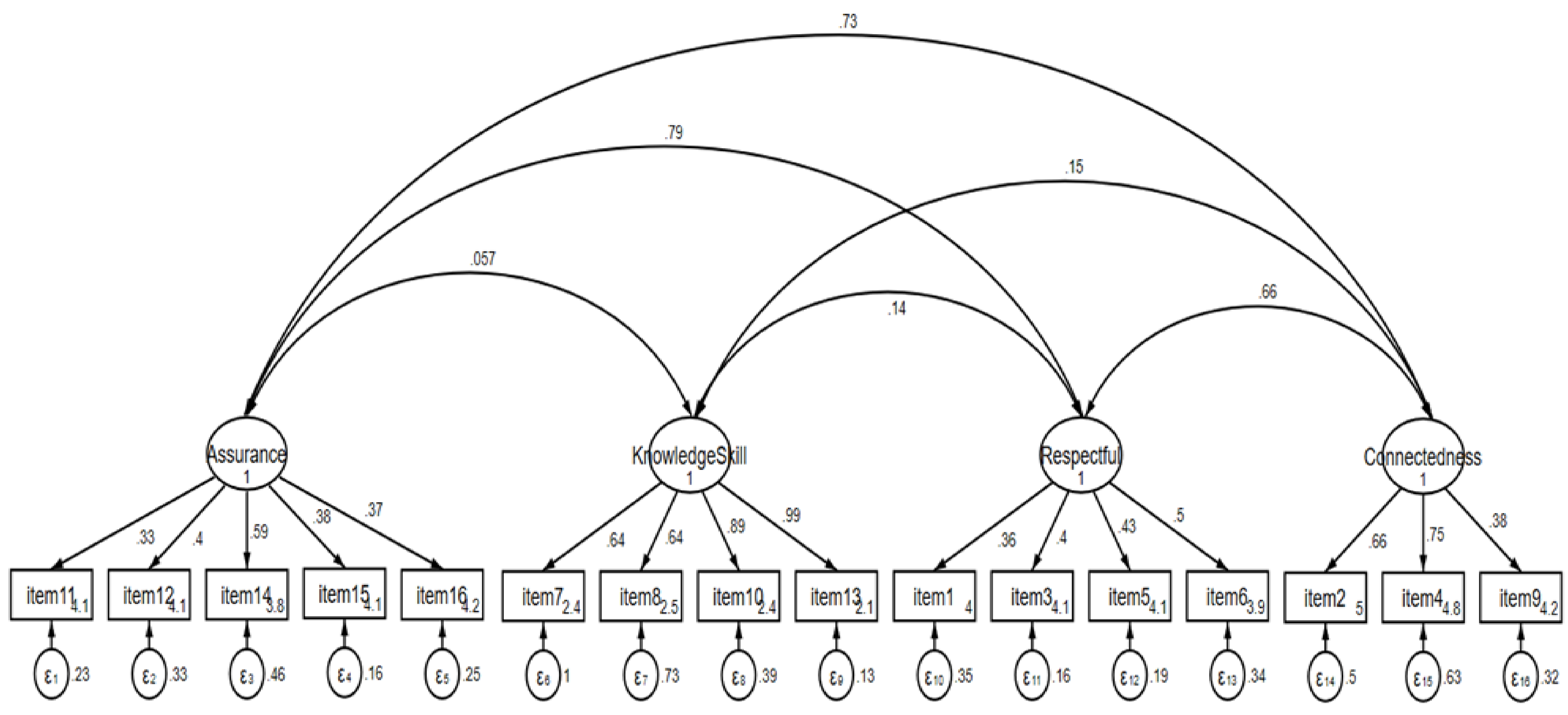
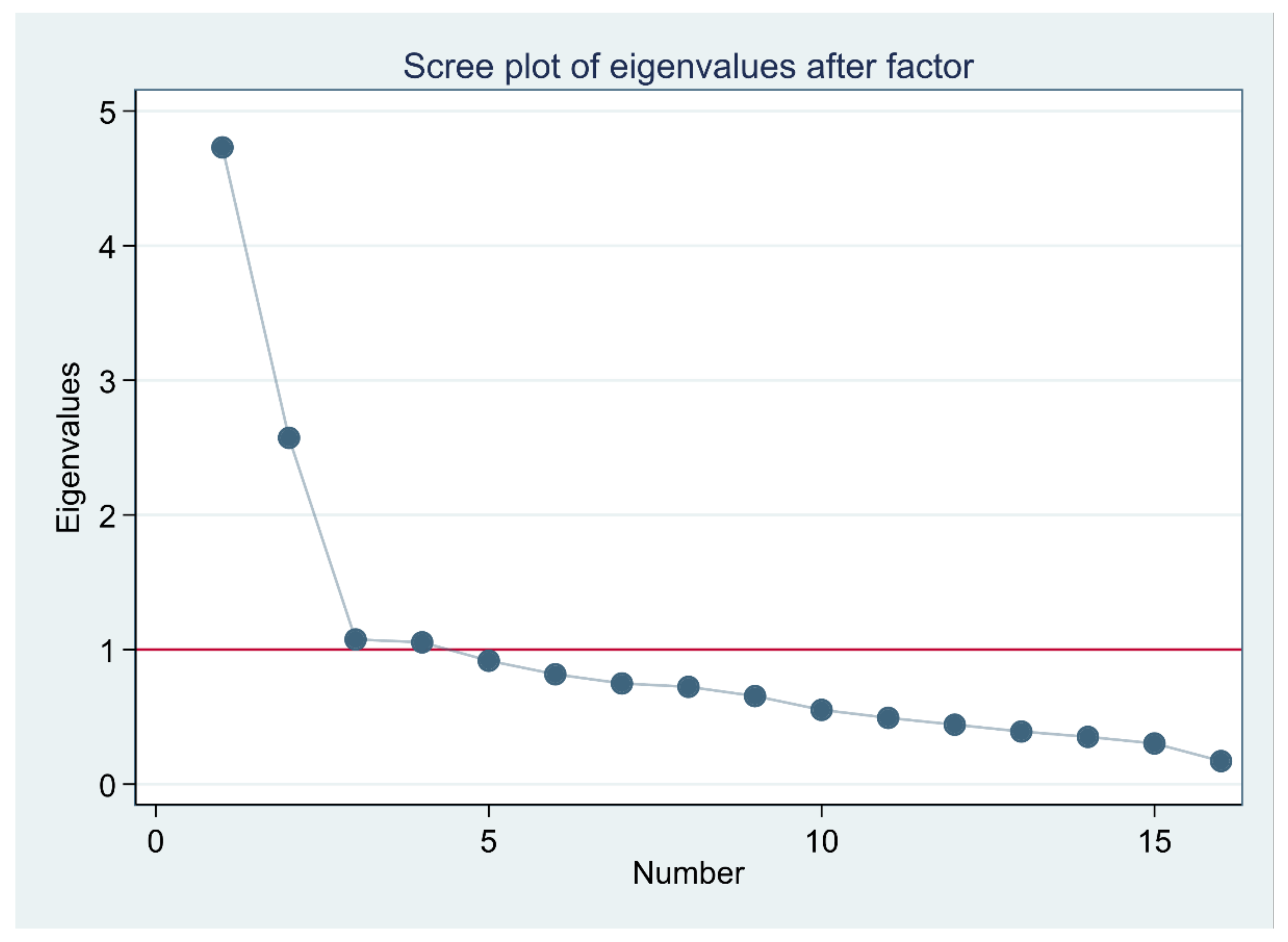
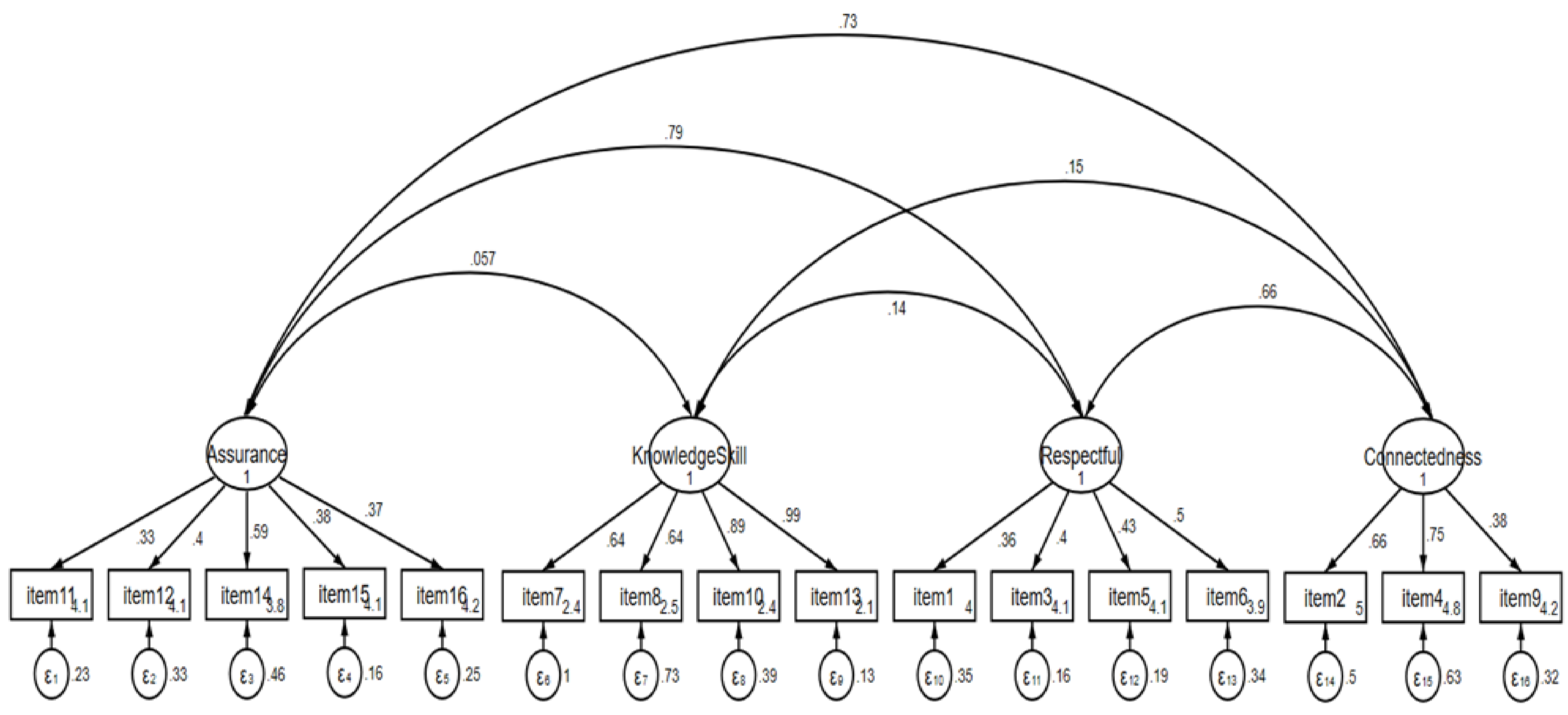
2.10. Construct Validity
2.11. Reliability
3. Results
3.1. Construct Validity
3.2. Reliability
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Watson, J. Caring science and human caring theory: Transforming personal and professional practices of nursing and health care. J. Health Hum. Serv. Adm. 2009, 31, 466–482. [Google Scholar] [PubMed]
- Papastavrou, E.; Efstathiou, G.; Tsangari, H.; Suhonen, R.; Leino-Kilpi, H.; Patiraki, E.; Karlou, C.; Balogh, Z.; Palese, A.; Tomietto, M.; et al. A cross-cultural study of the concept of caring through behaviours: Patients’ and nurses’ perspectives in six different EU countries. J. Adv. Nurs. 2011, 68, 1026–1037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilkin, K. The meaning of caring in the practice of intensive care nursing. Br. J. Nurs. 2003, 12, 1178–1185. [Google Scholar] [CrossRef] [PubMed]
- Morse, J.M.; Solberg, S.M.; Neander, W.L.; Bottorff, J.L.; Johnson, J.L. Concepts of caring and caring as a concept. ANS Adv. Nurs. Sci. 1990, 13, 1–14. [Google Scholar] [CrossRef]
- Wu, Y.; Larrabee, J.H.; Putman, H.P. Caring Behaviors Inventory: A reduction of the 42-item instrument. Nurs. Res. 2006, 55, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Alikari, V.; Fradelos, E.C.; Papastavrou, E.; Alikakou, S.; Zyga, S. Psychometric Properties of the Greek Version of the Caring Be-haviors Inventory-16. Cureus 2021, 13, e15186. [Google Scholar] [PubMed]
- Watson, J. Assessing and Measuring Caring in Nursing and Health Sciences, 2nd ed.; Springer: Berlin/Heidelberg, Germany, 2009; p. 366. [Google Scholar]
- Wolf, Z.R.; Dillon, P.M.; Townsend, A.B.; Glasofer, A. Caring Behaviors Inventory-24 Revised: CBI-16 Validation and Psychometric Properties. Int. J. Hum. Caring 2017, 21, 185–192. [Google Scholar] [CrossRef]
- Ghafouri, R.; Nasiri, M.; Atashzadeh-Shoorideh, F.; Tayyar-Iravanlou, F.; Rahmaty, Z. Translation and validation of caring be-haviors inventory among nurses in Iran. PLoS ONE 2021, 16, e0254317. [Google Scholar] [CrossRef]
- Baldursdottir, G.; Jonsdottir, H. The importance of nurse caring behaviors as perceived by patients receiving care at an emergency department. Heart Lung 2002, 31, 67–75. [Google Scholar] [CrossRef] [Green Version]
- Coulombe, K.H.; Yeakel, S.; Maljanian, R.; Bohannon, R.W. Caring Behaviors Inventory: Analysis of responses by hospitalized sur-gical patients. Outcomes Manag. 2002, 6, 138–141. [Google Scholar]
- Hwang, H.L.; Tu, C.T.; Chen, S.; Wang, H.H. Caring behaviors perceived by elderly residents of long-term care facilities: Scale development and psychometric assessment. Int. J. Nurs. Stud. 2012, 49, 183–190. [Google Scholar] [CrossRef]
- Merrill, A.S.; Hayes, J.S.; Clukey, L.; Curtis, D. Do they Really Care? How Trauma Patients Perceive Nurses’ Caring Behaviors. J. Trauma Nurs. 2012, 19, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Green, A. Caring Behaviors as Perceived by Nurse Practitioners. J. Am. Acad. Nurse Pract. 2004, 16, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Yam, B.M.C.; Rossiter, J.C. Caring in nursing: Perceptions of Hong Kong nurses. J. Clin. Nurs. 2000, 9, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Karlou, C.; Papathanassoglou, E.; Patiraki, E. Caring behaviours in cancer care in Greece. Comparison of patients’, their caregivers’ and nurses’ perceptions. Eur. J. Oncol. Nurs. 2015, 19, 244–250. [Google Scholar] [CrossRef]
- O’Connell, E.; Landers, M. The importance of critical care nurses’ caring behaviours as perceived by nurses and relatives. Intensiv. Crit. Care Nurs. 2008, 24, 349–358. [Google Scholar] [CrossRef]
- Labrague, L.J.; McEnroe-Petitte, D.M.; Papathanasiou, I.V.; Edet, O.B.; Arulappan, J.; Tsaras, K.; Fronda, D.C. Nursing students’ perceptions of their instructors’ caring behaviors: A four-country study. Nurse Educ. Today 2016, 41 (Suppl. C), 44–49. [Google Scholar] [CrossRef]
- Zamanzadeh, V.; Shohani, M.; Palmeh, T. Nursing Students’ Perception of Instructors’ Caring Behaviors in Tabriz University of Medical Sciences. J. Caring Sci. 2015, 4, 55–62. [Google Scholar] [CrossRef]
- He, T.; Du Ms, Y.; Wang, L.; Zhong, Z.; Ye, X.; Liu, X. Perceptions of caring in China: Patient and nurse questionnaire survey. Int. Nurs. Rev. 2013, 60, 487–493. [Google Scholar] [CrossRef]
- Von Essen, L.; Sjödén, P.O. The importance of nurse caring behaviors as perceived by Swedish hospital patients and nursing staff. Int. J. Nurs. Stud. 1991, 28, 267–281. [Google Scholar] [CrossRef]
- Papastavrou, E.; Karlou, C.; Tsangari, H.; Efstathiou, G.; Sousa, V.D.; Merkouris, A.; Patiraki, E. Cross-cultural validation and psychometric properties of the Greek version of the Caring Behaviors Inventory: A methodological study. J. Eval. Clin. Pr. 2010, 17, 435–443. [Google Scholar] [CrossRef] [PubMed]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the Process of Cross-Cultural Adaptation of Self-Report Measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrington, D. Confirmatory Factor Analysis; Oxford University Press: New York, NY, USA, 2008; 128p. [Google Scholar]
- Hinshaw, A.S.; Atwood, J.R. A Patient Satisfaction Instrument: Precision by replication. Nurs. Res. 1982, 31, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Bucco, T. The Relationships Between Patients’ Perceptions of Nurse Caring Behaviors, Nurses’ Perceptions of Nurse Caring Behaviors and Patient Satisfaction in the Emergency Department. Seton Hall University Dissertations and Theses (ETDs), [In-ternet], 16 May 2015. Available online: https://scholarship.shu.edu/dissertations/2048 (accessed on 6 October 2019).
- McHorney, C.A.; Tarlov, A.R. Individual-patient monitoring in clinical practice: Are available health status surveys adequate? Int. J. Qual. Life Asp. Treat. Care Rehabil. 1995, 4, 293–307. [Google Scholar] [CrossRef] [PubMed]
- Randall, E.S.; Richard, G.L. A Beginner’s Guide to Structural Equation Modeling, 4th ed; Routledge: New York, NY, USA, 2016; 375p. [Google Scholar]
- Waltz, C.F.; Strickland, O.L.; Lenz, E.R. Measurement in Nursing and Health Research, 3rd ed.; Springer: New York, NY, USA, 2005. [Google Scholar]
- Schermelleh-Engel, K.; Moosbrugger, H.; Müller, H. Evaluating the Fit of Structural Equation Models: Tests of Significance and Descriptive Goodness-of-Fit Measures. Methods Psychol. Res. 2003, 8, 23–74. [Google Scholar]
- Raykov, T.; Marcoulides, G.A. Introduction to Psychometric Theory; Routledge/Taylor & Francis Group: New York, NY, USA, 2011; p. 335, (Introduction to psychometric theory). [Google Scholar]
- Bland, J.M.; Altman, D.G. Statistics notes: Cronbach’s alpha. BMJ 1997, 314, 572. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Characteristic | Median (Range) | n (%) |
|---|---|---|
| Sex | ||
| Male | 188 (61.8) | |
| Female | 116 (38.2) | |
| Marital status | ||
| Married | 182 (59.9) | |
| Single | 108 (35.5) | |
| Divorced | 14 (4.6) | |
| Residence | ||
| Urban | 159 (52.3) | |
| Rural | 145 (47.7) | |
| Educational level | ||
| No formal education | 111 (36.5) | |
| Can read and write | 24 (7.9) | |
| Elementary school | 55 (18.1) | |
| High school | 64 (21.1) | |
| Diploma | 34 (11.2) | |
| Bachelor and above | 16 (5.3) | |
| Current unit | ||
| Internal medicine | 160 (52.6) | |
| Surgery | 144 (47.4) | |
| Hospitalization days | Median = 5 (2–210) | |
| Number of admissions in the last 5 years | Median = 1 (1–10) | |
| Time spent by the nurse in minutes | Median = 30 (5–480) |
| Subscales | Mean (SD) | Correlation | α If Item Deleted | R2 | Floor-Ceiling Effect | |
|---|---|---|---|---|---|---|
| Item-Test | Item-Rest | |||||
| Assurance | 4.07 (0.14) | 4.0–4.5 | ||||
| Item 11 | 4.09 (0.58) | 0.55 | 0.46 | 0.82 | 0.31 | 4.0–4.5 |
| Item 12 | 4.12 (0.70) | 0.55 | 0.46 | 0.82 | 0.33 | 4.5–5.0 |
| Item 14 | 3.82 (0.89) | 0.60 | 0.52 | 0.82 | 0.43 | 4.0–4.5 |
| Item 15 | 4.13 (0.56) | 0.61 | 0.53 | 0.82 | 0.47 | 4.5–5.0 |
| Item 16 | 4.17 (0.63) | 0.54 | 0.45 | 0.82 | 0.36 | 4.0–4.5 |
| Knowledge and Skill | 2.37 (0.17) | 2.0–2.5 | ||||
| Item 7 | 2.42 (1.19) | 0.43 | 0.33 | 0.83 | 0.29 | 3.5–4.0 |
| Item 8 | 2.55 (1.07) | 0.40 | 0.29 | 0.83 | 0.36 | 2.0–2.5 |
| Item 10 | 2.36 (1.08) | 0.40 | 0.30 | 0.83 | 0.67 | 2.5–3.0 |
| Item 13 | 2.14 (1.06) | 0.40 | 0.29 | 0.83 | 0.88 | 4.0–4.5 |
| Respectful | 4.03 (0.08) | 4.0–4.5 | ||||
| Item 1 | 4.01 (0.69) | 0.46 | 0.36 | 0.83 | 0.27 | 2.0–2.5 |
| Item 3 | 4.10 (0.56) | 0.63 | 0.56 | 0.81 | 0.50 | 4.0–4.5 |
| Item 5 | 4.08 (0.61) | 0.60 | 0.52 | 0.82 | 0.49 | 4.0–4.5 |
| Item 6 | 3.92 (0.77) | 0.63 | 0.56 | 0.81 | 0.42 | 2.0–2.5 |
| Connectedness | 4.66 (0.43) | 4.5–5.0 | ||||
| Item 2 | 4.99 (0.97) | 0.56 | 0.47 | 0.82 | 0.47 | 3.5–4.0 |
| Item 4 | 4.83 (1.09) | 0.57 | 0.48 | 0.82 | 0.47 | 4.0–4.5 |
| Item 9 | 4.17 (0.68) | 0.57 | 0.46 | 0.82 | 0.32 | 4.0–4.5 |
| Overall | 0.83 | 0.99 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferede, A.J.; Erlandsson, K.; Gezie, L.D.; Geda, B.; Wettergren, L. Psychometric Properties of the Caring Behaviors Inventory-16 in Ethiopia. Nurs. Rep. 2022, 12, 387-396. https://doi.org/10.3390/nursrep12020037
Ferede AJ, Erlandsson K, Gezie LD, Geda B, Wettergren L. Psychometric Properties of the Caring Behaviors Inventory-16 in Ethiopia. Nursing Reports. 2022; 12(2):387-396. https://doi.org/10.3390/nursrep12020037
Chicago/Turabian StyleFerede, Abebaw Jember, Kerstin Erlandsson, Lemma Derseh Gezie, Biftu Geda, and Lena Wettergren. 2022. "Psychometric Properties of the Caring Behaviors Inventory-16 in Ethiopia" Nursing Reports 12, no. 2: 387-396. https://doi.org/10.3390/nursrep12020037
APA StyleFerede, A. J., Erlandsson, K., Gezie, L. D., Geda, B., & Wettergren, L. (2022). Psychometric Properties of the Caring Behaviors Inventory-16 in Ethiopia. Nursing Reports, 12(2), 387-396. https://doi.org/10.3390/nursrep12020037