
Brief Report: Hispanic Patients’ Trajectory of Cancer Symptom Burden, Depression, Anxiety, and Quality of Life

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
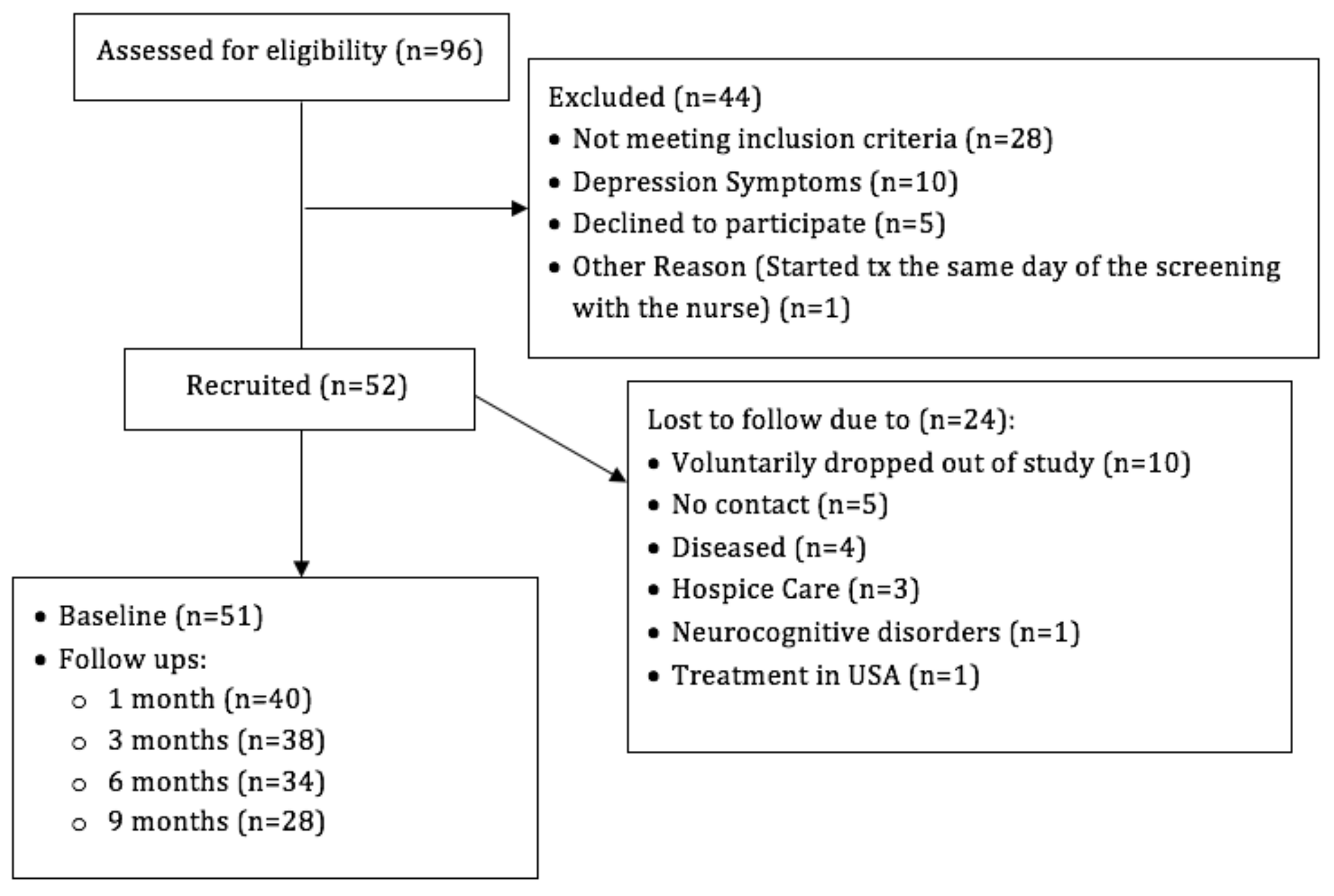
2.1. Participants
2.2. Measures
2.3. Data Analysis
3. Results
3.1. Participants’ Socio-Demographic and Clinical Characteristics
3.2. Correlations among Anxiety, Depression, Cancer Symptom Burden, and Quality of Life
3.3. Hypothesis Testing Multilevel Mixed-Effects Linear Regression Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mitchell, A.J.; Chan, M.; Bhatti, H.; Halton, M.; Grassi, L.; Johansen, C.; Meader, N. Prevalence of depression, anxiety, and adjustment disorder in oncological, haematological, and palliative-care settings: A meta-analysis of 94 interview-based studies. Lancet Oncol. 2011, 12, 160–174. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Ferguson, D.W.; Gill, J.; Paul, J.; Symonds, P. Depression and anxiety in long-term cancer survivors compared with spouses and healthy controls: A systematic review and meta-analysis. Lancet Oncol. 2013, 14, 721–732. [Google Scholar] [CrossRef]
- Jacob, L.; Kalder, M.; Kostev, K. Incidence of depression and anxiety among women newly diagnosed with breast or genital organ cancer in Germany. Psycho-Oncol. 2017, 26, 1535–1540. [Google Scholar] [CrossRef] [PubMed]
- Snyderman, D.; Wynn, D. Depression in cancer patients. Prim. Care 2009, 36, 703–719. [Google Scholar] [CrossRef]
- Luckett, T.; Goldstein, D.; Butow, P.N.; Gebski, V.; Aldridge, L.J.; McGrane, J.; Ng, W.; King, M.T. Psychological morbidity and quality of life of ethnic minority patients with cancer: A systematic review and meta-analysis. Lancet Oncol. 2011, 12, 1240–1248. [Google Scholar] [CrossRef]
- Costas, R.; Gany, F. Depressive symptoms in a sample of Afro-Caribbean and Latino immigrant cancer patients: A comparative analysis. Supportive Care Cancer 2013, 21, 2461–2468. [Google Scholar] [CrossRef] [PubMed]
- Yanez, B.; Thompson, E.H.; Stanton, A.L. Quality of life among Latina breast cancer patients: A systematic review of the literature. J. Cancer Surviv. 2011, 5, 191–207. [Google Scholar] [CrossRef] [PubMed]
- Gold, M.; Dunn, L.B.; Phoenix, B.; Paul, S.M.; Hamolsky, D.; Levine, J.D.; Miaskowski, C. Co-occurrence of anxiety and depressive symptoms following breast cancer surgery and its impact on quality of life. Eur. J. Oncol. Nurs. 2016, 20, 97–105. [Google Scholar] [CrossRef]
- Hulbert-Williams, N.; Neal, R.; Morrison, V.; Hood, K.; Wilkinson, C. Anxiety, depression and quality of life after cancer diagnosis: What psychosocial variables best predict how patients adjust? Psycho Oncol. 2012, 21, 857–867. [Google Scholar] [CrossRef]
- Gonzalez-Mercado, V.J.; Saligan, L.N.; Ji, M.; Groer, M.; Pedro, E.; McMillan, S. Differences in the severity, distress, interference, and frequency on cancer-related symptoms between Island Hispanic Puerto Ricans and Mainland non-Hispanic Whites. J. Immigr. Minority Health 2018, 20, 1029–1039. [Google Scholar] [CrossRef]
- Krok-Schoen, J.L.; Fernandez, K.; Unzeitig, G.W.; Rubio, G.; Paskett, E.D.; Post, D.M. Hispanic breast cancer patients’ symptom experience and patient-physician communication during chemotherapy. Supportive Care Cancer 2019, 27, 697–704. [Google Scholar] [CrossRef]
- Check, D.K.; Chawla, N.; Kwan, M.L.; Pinheiro, L.; Roh, J.M.; Ergas, I.J.; Stewart, A.L.; Kolevska, T.; Ambrosone, C.; Kushi, L.H. Understanding racial/ethnic differences in breast cancer-related physical well-being: The role of patient–provider interactions. Breast Cancer Res. Treat. 2018, 170, 593–603. [Google Scholar] [CrossRef]
- Wilson, I.B.; Cleary, P.D. Linking clinical variables with health-related quality of life. A conceptual model of patient outcomes. JAMA 1995, 273, 59–65. [Google Scholar] [CrossRef]
- Hyland, K.A.; Hoogland, A.I.; Gonzalez, B.D.; Nelson, A.M.; Lechner, S.; Tyson, D.M.; Barata, A.; Gomez, M.F.; Antoni, M.H.; Small, B.; et al. Evaluation of the Psychometric and Structural Properties of the Spanish Version of the Hospital Anxiety and Depression Scale in Latina Cancer Patients. J. Pain Symptom Manag. 2019. [Google Scholar] [CrossRef] [PubMed]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale: An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef]
- Cleeland, C.S.; Mendoza, T.R.; Wang, X.S.; Chou, C.; Harle, M.T.; Morrissey, M.; Engstrom, M.C. Assessing symptom distress in cancer patients: The MD Anderson Symptom Inventory. Cancer Interdiscip. Int. J. Am. Cancer Soc. 2000, 89, 1634–1646. [Google Scholar] [CrossRef]
- Cella, D.F.; Tulsky, D.S.; Gray, G.; Sarafian, B.; Linn, E.; Bonomi, A.; Silberman, M.; Yellen, S.B.; Winicour, P.; Brannon, J. The Functional Assessment of Cancer Therapy scale: Development and validation of the general measure. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 1993, 11, 570–579. [Google Scholar] [CrossRef]
- StataCorp. Stata Statistical Software: Release 14; StataCorp LP: College Station, TX, USA, 2015. [Google Scholar]
- Linden, W.; Vodermaier, A.; MacKenzie, R.; Greig, D. Anxiety and depression after cancer diagnosis: Prevalence rates by cancer type, gender, and age. J. Affect. Disord. 2012, 141, 343–351. [Google Scholar] [CrossRef]
- Hess, C.B.; Chen, A.M. Measuring psychosocial functioning in the radiation oncology clinic: A systematic review. Psycho-Oncol. 2014, 23, 841–854. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Tyson, D.M.; Gonzalez, B.D.; Small, B.J.; Lechner, S.C.; Antoni, M.H.; Vinard, A.; Krause, M.; Meade, C.; Jacobsen, P.B. Anxiety and depression in S Spanish-speaking Latina cancer patients prior to starting chemotherapy. Psycho Oncol. 2018, 27, 333–338. [Google Scholar] [CrossRef]
- Stafford, L.; Judd, F.; Gibson, P.; Komiti, A.; Mann, G.B.; Quinn, M. Anxiety and depression symptoms in the 2 years following diagnosis of breast or gynaecologic cancer: Prevalence, course and determinants of outcome. Supportive Care Cancer 2015, 23, 2215–2224. [Google Scholar] [CrossRef]
- Chung, J.; Ju, G.; Yang, J.; Jeong, J.; Jeong, Y.; Choi, M.K.; Kwon, J.; Lee, K.H.; Kim, S.T.; Han, H.S. Prevalence of and factors associated with anxiety and depression in Korean patients with newly diagnosed advanced gastrointestinal cancer. Korean J. Intern. Med. 2018, 33, 585. [Google Scholar] [CrossRef]
- Mols, F.; Schoormans, D.; de Hingh, I.; Oerlemans, S.; Husson, O. Symptoms of anxiety and depression among colorectal cancer survivors from the population-based, longitudinal PROFILES Registry: Prevalence, predictors, and impact on quality of life. Cancer 2018, 124, 2621–2628. [Google Scholar] [CrossRef]
- Hipkins, J.; Whitworth, M.; Tarrier, N.; Jayson, G. Social support, anxiety and depression after chemotherapy for ovarian cancer: A prospective study. Br. J. Health Psychol. 2004, 9, 569–581. [Google Scholar] [CrossRef]
- Hellstadius, Y.; Lagergren, J.; Zylstra, J.; Gossage, J.; Davies, A.; Hultman, C.M.; Lagergren, P.; Wikman, A. A longitudinal assessment of psychological distress after oesophageal cancer surgery. Acta Oncol. 2017, 56, 746–752. [Google Scholar] [CrossRef] [PubMed]
- Vahdaninia, M.; Omidvari, S.; Montazeri, A. What do predict anxiety and depression in breast cancer patients? A follow-up study. Soc. Psychiatry Psychiatr. Epidemiol. 2010, 45, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Shi, Q.; Smith, T.G.; Michonski, J.D.; Stein, K.D.; Kaw, C.; Cleeland, C.S. Symptom burden in cancer survivors 1 year after diagnosis: A report from the American Cancer Society’s Studies of Cancer Survivors. Cancer 2011, 117, 2779–2790. [Google Scholar] [CrossRef] [PubMed]
- Grotmol, K.S.; Lie, H.C.; Loge, J.H.; Aass, N.; Haugen, D.F.; Stone, P.C.; Kaasa, S.; Hjermstad, M.J. Patients with advanced cancer and depression report a significantly higher symptom burden than non-depressed patients. Palliat. Support. Care 2019, 17, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Yennurajalingam, S.; Tayjasanant, S.; Balachandran, D.; Padhye, N.S.; Williams, J.L.; Liu, D.D.; Frisbee-Hume, S.; Bruera, E. Association between daytime activity, fatigue, sleep, anxiety, depression, and symptom burden in advanced cancer patients: A preliminary report. J. Palliat. Med. 2016, 19, 849–856. [Google Scholar] [CrossRef] [PubMed]
- McFarland, D.C.; Shaffer, K.M.; Tiersten, A.; Holland, J. Physical symptom burden and its association with distress, anxiety, and depression in breast cancer. Psychosomatics 2018, 59, 464–471. [Google Scholar] [CrossRef]
- Leonhart, R.; Tang, L.; Pang, Y.; Li, J.; Song, L.; Fischer, I.; Koch, M.; Wuensch, A.; Fritzsche, K.; Schaefert, R. Physical and psychological correlates of high somatic symptom severity in Chinese breast cancer patients. Psycho-Oncol. 2017, 26, 656–663. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Guo, W.J.; Mo, L.L.; Luo, S.X.; Yu, J.Y.; Dong, Z.Q.; Liu, Y.; Huang, M.J.; Wang, Y.; Chen, L.; et al. Prevalence and strong association of high somatic symptom severity with depression and anxiety in a Chinese inpatient population. Asia-Pacific Psychiatry 2017, 9, e12282. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Socio-Demographics | |
|---|---|
| Age | |
| Mean ± SD | 63.3 ± 14.6 |
| Median (min, max) | 66 (23, 86) |
| Sex, n (%) | |
| Male | 30 (58.8) |
| Female | 21 (41.2) |
| Household composition, n (%) | |
| Alone | 8 (15.7) |
| Partner | 19 (37.3) |
| Son/Daughter | 5 (9.8) |
| Parents | 2 (3.9) |
| Partner and Son/Daughter | 10 (19.6) |
| Parents and Son/Daughter | 2 (3.9) |
| Son/Daughter and Grandchildren | 2 (3.9) |
| Partner, Son/Daughter, and Grandchildren | 1 (2.0) |
| Other Family Members | 2 (3.9) |
| Employment, n (%) | |
| Employed | 6 (11.8) |
| Unemployed | 8 (15.7) |
| Disabled | 4 (7.8) |
| Retired | 30 (58.8) |
| Student | 1 (2.0) |
| Other (did not specify) | 2 (3.9) |
| Education, n (%) | |
| <High School | 15 (29.4) |
| ≥High School | 36 (70.6) |
| Civil Status, n (%) | |
| Single | 7 (13.7) |
| Married/Living with Partner | 32 (62.8) |
| Divorced | 6 (11.8) |
| Widowed | 6 (11.8) |
| Medical Insurance †, n (%) | |
| Private ‡ | 14 (28.0) |
| Health Care Reform § | 14 (28.0) |
| Medicare | 22 (44.0) |
| Household Income, n (%) | |
| ≤$19,000 | 37 (72.6) |
| >$19,000 | 14 (27.4) |
| Clinical Features | |
| Tumour site (primary), n (%) | |
| Breast | 6 (11.8) |
| Prostate †† | 5 (9.8) |
| Multiple Myeloma | 2 (3.9) |
| Head and Neck | 3 (5.9) |
| Leukaemia | 2 (3.9) |
| Lung | 3 (5.9) |
| Pancreatic | 6 (11.8) |
| Lymphoma | 5 (9.8) |
| Colorectal | 10 (19.6) |
| Stomach | 2 (3.9) |
| Melanoma | 2 (3.9) |
| Other sites ‡‡ | 5 (9.8) |
| Disease stage, n (%) | |
| I †† | 6 (12.0) |
| II | 9 (18.0) |
| III | 13 (26.0) |
| IV | 22 (44.0) |
| Characteristics | Without Depressive Symptoms (n = 17) | With Depressive Symptoms (n = 11) | p-Value † |
|---|---|---|---|
| Sex | 0.14 ‡ | ||
| Male | 11 (64.7) | 4 (36.4) | |
| Female | 6 (35.3) | 7 (63.6) | |
| Age | 0.72 | ||
| Mean (+/− SD) | 59.2 (14.9) | 62.4 (15.5) | |
| Median (P25–P75) | 65 (55–67) | 63 (47–78) | |
| Household Income | 0.08 | ||
| ≤$19,000 | 15 (88.2) | 6 (54.6) | |
| >$19,000 | 2 (11.8) | 5 (45.5) | |
| Income-Enough | 0.14 ‡ | ||
| No | 6 (35.3) | 7 (63.6) | |
| Yes | 11 (64.7) | 4 (36.4) | |
| Education | 0.65 | ||
| <High School | 3 (17.7) | 3 (27.3) | |
| ≥High School | 14 (82.4) | 8 (72.7) | |
| Marital status | 0.08 | ||
| Single | 4 (23.5) | 0 (0.0) | |
| Married/Living with a partner | 9 (52.9) | 10 (90.1) | |
| Divorced | 3 (17.7) | 0 (0.0) | |
| Widowed | 1 (5.9) | 1 (9.1) |
| Fixed Effect | Depression Symptoms | Anxiety Symptoms |
|---|---|---|
| Intercept | 7.97 (4.43, 11.51) | 11.06 (6.76, 15.36) |
| Time point (visits) | ||
| Baseline | REFERENCE | REFERENCE |
| 1 | −0.23 (−0.94, 0.48) | −0.72 (−1.60, 0.16) |
| 2 | 0.19 (−0.54, 0.92) | −0.19 (−1.10, 0.71) |
| 3 | −0.00 (−0.75, 0.75) | −0.54 (−1.47, 0.39) |
| 4 | −0.39 (−1.23, 0.45) | −1.23 (−2.27, −0.19) ‡ |
| Sex | ||
| Male | REFERENCE | REFERENCE |
| Female | 0.85 (−0.26, 1.96) | 1.91 (0.58, 3.24) ‡ |
| Age† | −0.12 (−0.33, 0.10) | −0.24 (−0.50, 0.02) |
| Marital Status | ||
| Single | REFERENCE | REFERENCE |
| Married/Living with Partner | 1.57 (−0.24, 3.38) | 1.00 (−1.15, 3.16) |
| Divorced | 0.29 (−1.95, 2.54) | −0.37 (−3.05, 2.31) |
| Widowed | 0.95 (−1.74, 3.65) | 1.80 (−1.43, 5.03) |
| Quality of Life† | −0.33 (−0.47, −0.18) ‡ | −0.38 (−0.55, −0.20) ‡ |
| Burden of Cancer Symptoms† | 0.04 (−0.03, 0.11) | 0.11 (0.02, 0.19) ‡ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castro-Figueroa, E.M.; Torres-Blasco, N.; Rosal, M.C.; Jiménez, J.C.; Castro-Rodríguez, W.P.; González-Lorenzo, M.; Vélez-Cortés, H.; Toro-Bahamonde, A.; Costas-Muñiz, R.; Armaiz-Peña, G.N.; et al. Brief Report: Hispanic Patients’ Trajectory of Cancer Symptom Burden, Depression, Anxiety, and Quality of Life. Nurs. Rep. 2021, 11, 475-483. https://doi.org/10.3390/nursrep11020044
Castro-Figueroa EM, Torres-Blasco N, Rosal MC, Jiménez JC, Castro-Rodríguez WP, González-Lorenzo M, Vélez-Cortés H, Toro-Bahamonde A, Costas-Muñiz R, Armaiz-Peña GN, et al. Brief Report: Hispanic Patients’ Trajectory of Cancer Symptom Burden, Depression, Anxiety, and Quality of Life. Nursing Reports. 2021; 11(2):475-483. https://doi.org/10.3390/nursrep11020044
Chicago/Turabian StyleCastro-Figueroa, Eida M., Normarie Torres-Blasco, Milagros C. Rosal, Julio C. Jiménez, Wallesca P. Castro-Rodríguez, Marilis González-Lorenzo, Héctor Vélez-Cortés, Alia Toro-Bahamonde, Rosario Costas-Muñiz, Guillermo N. Armaiz-Peña, and et al. 2021. "Brief Report: Hispanic Patients’ Trajectory of Cancer Symptom Burden, Depression, Anxiety, and Quality of Life" Nursing Reports 11, no. 2: 475-483. https://doi.org/10.3390/nursrep11020044
APA StyleCastro-Figueroa, E. M., Torres-Blasco, N., Rosal, M. C., Jiménez, J. C., Castro-Rodríguez, W. P., González-Lorenzo, M., Vélez-Cortés, H., Toro-Bahamonde, A., Costas-Muñiz, R., Armaiz-Peña, G. N., & Jim, H. (2021). Brief Report: Hispanic Patients’ Trajectory of Cancer Symptom Burden, Depression, Anxiety, and Quality of Life. Nursing Reports, 11(2), 475-483. https://doi.org/10.3390/nursrep11020044