
Development and Validation of the Brief Nursing Stress Scale (BNSS) in a Sample of End-of-Life Care Nurses



Abstract
1. Introduction
2. Materials and Methods
2.1. Development of the Brief Nursing Stress Scale
2.2. Design, Setting, and Participants
2.3. Variables
- Workload, measured with the item “I have too much workload”, ranging from 0 (never) to 3 (almost always).
- Work control, measured with the item “I have control over my workload”, ranging from 0 (never) to 3 (almost always).
- Burnout, measured with the Maslach Burnout Inventory—Human Services Survey (MBI) [31]. This is a 22-item questionnaire that relates to three constructs of burnout: emotional exhaustion (9 items), depersonalization (5 items), and personal accomplishment (8 items). Each item rated on a seven-point Likert-type scale for how frequently they experience the feeling, from 0 (never) to 6 (every day).
- Work satisfaction, measured with the General Work Satisfaction Scale from the Michigan Organizational Assessment Scale [32]. The scale is composed by three items. Each item rated on a five-point Likert-type scale, from 1 (completely disagree) to 5 (completely agree).
2.4. Analyses
2.5. Ethical Considerations
3. Results
3.1. Participants Description
3.2. Descriptive Statistics
3.3. Internal Structre and Reliability
3.4. Relations between Nursing Stress, Sex, Age, Working Place, Workload, and Work Control
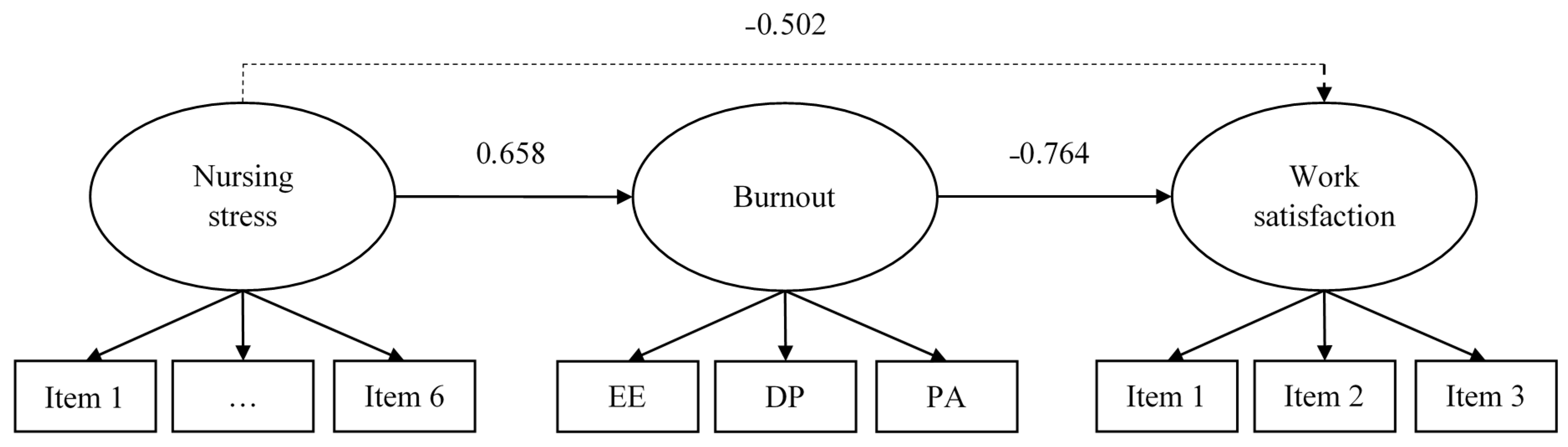
3.5. Prediction of Burnout and Work Satisfaction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hingley, P. The Humane Face of Nursing. Nurs. Mirror 1984, 159, 19–22. [Google Scholar] [PubMed]
- Cañadas-De la Fuente, G.A.; Vargas, C.; San Luis, C.; García, I.; Cañadas, G.R.; De la Fuente, E.I. Risk factors and prevalence of burnout syndrome in the nursing profession. Int. J. Nurs. Stud. 2015, 52, 240–249. [Google Scholar] [CrossRef] [PubMed]
- Mealer, M.; Burnham, E.L.; Goode, C.J.; Rothbaum, B.; Moss, M. The prevalence and impact of post traumatic stress disorder and burnout syndrome in nurses. Depress. Anxiety 2009, 26, 1118–1126. [Google Scholar] [CrossRef]
- Iglesias, M.E.; de Bengoa Vallejo, R.B.; Fuentes, P.S. The relationship between experiential avoidance and burnout syndrome in critical care nurses: A cross-sectional questionnaire survey. Int. J. Nurs. Stud. 2010, 47, 30–37. [Google Scholar] [CrossRef]
- Fornés-Vives, J.; García-Banda, G.; Frias-Navarro, D.; Pascual-Soler, M. Longitudinal study predicting burnout in Spanish nurses: The role of neuroticism and emotional coping. Pers. Individ. Differ. 2019, 138, 286–291. [Google Scholar] [CrossRef]
- Keidel, G.C. Burnout and compassion fatigue among hospice caregivers. Am. J. Hosp. Palliat. Care 2002, 19, 200–205. [Google Scholar] [CrossRef]
- Flanagan, N.A.; Flanagan, T.J. An analysis of the relationship between job satisfaction and job stress in correctional nurses. Res. Nurs. Health 2002, 25, 282–294. [Google Scholar] [CrossRef]
- Sarafis, P.; Rousaki, E.; Tsounis, A.; Malliarou, M.; Lahana, L.; Bamidis, P.; Niakas, D.; Papastavrou, E. The impact of occupational stress on nurses’ caring behaviors and their health related quality of life. BMC Nurs. 2016, 15, 56. [Google Scholar] [CrossRef]
- Teng, C.-I.; Hsiao, F.-J.; Chou, T.-A. Nurse-perceived time pressure and patient-perceived care quality. J. Nurs. Manag. 2010, 18, 275–284. [Google Scholar] [CrossRef]
- Iglesias, M.E.L.; de Bengoa Vallejo, R.B. Prevalence and relationship between burnout, job satisfaction, stress, and clinical manifestations in Spanish critical care nurses. Dimens. Crit. Care Nurs. 2013, 32, 130–137. [Google Scholar] [CrossRef]
- Levi, L. Occupational stress: Spice of life or kiss of death? Am. Psychol. 1990, 45, 1142–1145. [Google Scholar] [CrossRef]
- Olkinuora, M.A.; Lrappänen, R.A. Psychological stress experienced by health care personnel. Scand. J. Work Environ. Health 1987, 13, 1–8. [Google Scholar]
- Adriaenssens, J.; De Gucht, V.; Maes, S. Determinants and prevalence of burnout in emergency nurses: A systematic review of 25 years of research. Int. J. Nurs. Stud. 2015, 52, 649–661. [Google Scholar] [CrossRef] [PubMed]
- Clegg, A. Occupational stress in nursing: A review of the literature. J. Nurs. Manag. 2001, 9, 101–106. [Google Scholar] [CrossRef] [PubMed]
- McGrath, A.; Reid, N.; Boore, J. Occupational stress in nursing. Int. J. Nurs. Stud. 2003, 40, 555–565. [Google Scholar] [CrossRef]
- McHugh, M.D.; Kutney-Lee, A.; Cimiotti, J.P.; Sloane, D.M.; Aiken, L.H. Nurses’ Widespread Job Dissatisfaction, Burnout, And Frustration With Health Benefits Signal Problems For Patient Care. Health Aff. 2011, 30, 202–210. [Google Scholar] [CrossRef]
- Van Bogaert, P.; Clarke, S.; Willems, R.; Mondelaers, M. Nurse practice environment, workload, burnout, job outcomes, and quality of care in psychiatric hospitals: A structural equation model approach. J. Adv. Nurs. 2013, 69, 1515–1524. [Google Scholar] [CrossRef] [PubMed]
- Van Bogaert, P.; Meulemans, H.; Clarke, S.; Vermeyen, K.; Van De Heyning, P. Hospital nurse practice environment, burnout, job outcomes and quality of care: Test of a structural equation model. J. Adv. Nurs. 2009, 65, 2175–2185. [Google Scholar] [CrossRef] [PubMed]
- Benbunan-Bentata, B.; Cruz-Quintana, F.; Roa-Venegas, J.M.; Villaverde-Gutiérrez, C.; Benbunan-Bentata, B.R. Nursing Students’ Coping with Pain and Death: A Proposal for Ameliorative Action. Int. J. Clin. Health Psychol. 2007, 7, 197–205. [Google Scholar]
- Stone, P.; Thorns, A. Ethics and Palliative Care: A Case-Based Manual; Radcliffe Publishing: Oxford, UK, 2005. [Google Scholar]
- Maslach, C. Burnout: The Cost of Caring; Malor Books: Cambridge, MA, USA, 2003. [Google Scholar]
- Pavelková, H.; Bužgová, R. Burnout among healthcare workers in hospice care. Central Eur. J. Nurs. Midwifery 2015, 6, 218–223. [Google Scholar] [CrossRef]
- French, S.E.; Lenton, R.; Walters, V.; Eyles, J. An Empirical Evaluation of an Expanded Nursing Stress Scale. J. Nurs. Meas. 2000, 8, 161–178. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.H.; Badiani, A.; Miczek, K.A.; Müller, C.P. Non-pharmacological factors that determine drug use and addiction. Neurosci. Biobehav. Rev. 2020, 110, 3–27. [Google Scholar] [CrossRef] [PubMed]
- Gray-Toft, P.; Anderson, J.G. The Nursing Stress Scale: Development of an instrument. J. Behav. Assess. 1981, 3, 11–23. [Google Scholar] [CrossRef]
- Lazarus, R.S. Psychological Stress and the Coping Process; McGraw-Hill: New York, NY, USA, 1966. [Google Scholar]
- Appley, M.H.; Trumbull, R. Psychological Stress, Issues in Research; Appleton-Century-Crofts: New York, NY, USA, 1967. [Google Scholar]
- Escribà, V.; Más, R.; Cárdenas, M.; Pérez, S. Validación de la escala de estresores laborales en personal de enfermería: «The Nursing Stress Scale». Gac. Sanit. 1999, 13, 191–200. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef]
- Wolf, E.J.; Harrington, K.M.; Clark, S.L.; Miller, M.W. Sample Size Requirements for Structural Equation Models: An Evaluation of Power, Bias, and Solution Propriety. Educ. Psychol. Meas. 2013, 73, 913–934. [Google Scholar] [CrossRef] [PubMed]
- Maslach, C.; Jackson, S.E.; Leiter, M.P.; Schaufeli, W.B.; Schwab, R.L. Maslach Burnout Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1986. [Google Scholar]
- Seashore, S.E.; Lawler, E.E., III; Mirvis, P.H.; Cammann, C. (Eds.) Assessing Organizational Change. A Guide to Methods, Measures, and Practices; Wiley: New York, NY, USA, 1983. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling; Guilford Press: New York, NY, USA, 2015; ISBN 978-1-60623-876-9. [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Windows, Version 24.0.; IBM Corp.: Armonk, NY, USA, 2016. [Google Scholar]
- Muthén, L.K.; Muthén, B. (Eds.) Mplus. The Comprehensive Modelling Program for Applied Researchers: User’s Guide; Muthén & Muthén: Los Angeles, CA, USA, 2017. [Google Scholar]
- World Medical Association. World Medical Association Declaration of Helsinki. Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Kenny, D.A.; Kaniskan, B.; McCoach, D.B. The Performance of RMSEA in Models with Small Degrees of Freedom. Sociol. Methods Res. 2014, 44, 486–507. [Google Scholar] [CrossRef]
- Kim, H.; Kim, K. Palliative Cancer Care Stress and Coping Among Clinical Nurses Who Experience End-of-Life Care. J. Hosp. Palliat. Nurs. 2020, 22, 115–122. [Google Scholar] [CrossRef] [PubMed]
- McKinney, B.K. Withstanding the Pressure of the Profession. J. Nurses Staff Dev. 2011, 27, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Mojoyinola, J. Effects of Job Stress on Health, Personal and Work Behaviour of Nurses in Public Hospitals in Ibadan Metropolis, Nigeria. Stud. Ethno-Med. 2008, 2, 143–148. [Google Scholar] [CrossRef]
- Nabirye, R.C.; Brown, K.C.; Pryor, E.R.; Maples, E.H. Occupational stress, job satisfaction and job performance among hospital nurses in Kampala, Uganda. J. Nurs. Manag. 2011, 19, 760–768. [Google Scholar] [CrossRef]
- Wazqar, D.Y.; Kerr, M.; Regan, S.; Orchard, C. Overview of Cancer Care and Oncology Nursing in the Kingdom of Saudi Arabia. Am. J. Nurs. Sci. 2017, 6, 324. [Google Scholar] [CrossRef]
- Xie, Z.; Wang, A.; Chen, B. Nurse burnout and its association with occupational stress in a cross-sectional study in Shanghai. J. Adv. Nurs. 2011, 67, 1537–1546. [Google Scholar] [CrossRef] [PubMed]
- Kakemam, E.; Raeissi, P.; Raoofi, S.; Soltani, A.; Sokhanvar, M.; Visentin, D.; Cleary, M. Occupational stress and associated risk factors among nurses: A cross-sectional study. Contemp. Nurse 2019, 55, 237–249. [Google Scholar] [CrossRef]
- Kwiatosz-Muc, M.; Fijałkowska-Nestorowicz, A.; Fijałkowska, M.; Aftyka, A.; Kowalczyk, M. Stress prevalence and stressors among anaesthesiology and intensive care unit workers: A multicentre survey study. Aust. Crit. Care 2018, 31, 391–395. [Google Scholar] [CrossRef]
- Jaracz, M.; Rosiak, I.; Bertrand-Bucińska, A.; Jaskulski, M.; Nieżurawska, J.; Borkowska, A. Affective temperament, job stress and professional burnout in nurses and civil servants. PLoS ONE 2017, 12, e0176698. [Google Scholar] [CrossRef]
- Stecker, M.; Stecker, M.M. Disruptive Staff Interactions: A Serious Source of Inter-Provider Conflict and Stress in Health Care Settings. Issues Ment. Health Nurs. 2014, 35, 533–541. [Google Scholar] [CrossRef]
- Al-Kandari, F.; Thomas, D. Adverse nurse outcomes: Correlation to nurses’ workload, staffing, and shift rotation in Kuwaiti hospitals. Appl. Nurs. Res. 2008, 21, 139–146. [Google Scholar] [CrossRef]
- Tankha, G. A Comparative Study of Role Stress in Government and Private Hospital Nurses. J. Health Manag. 2006, 8, 11–22. [Google Scholar] [CrossRef]
- Martens, M.L. A Comparison of Stress Factors in Home and Inpatient Hospice Nurses. J. Hosp. Palliat. Nurs. 2009, 11, 144–153. [Google Scholar] [CrossRef]
- Kogoj, T.K.; Cebašek-Travnik, Z.; Zaletel-Kragelj, L. Role of Stress in Burnout among Students of Medicine and Dentistry--a Study in Ljubljana, Slovenia, Faculty of Medicine. Coll. Antropol. 2014, 38, 879–887. [Google Scholar] [PubMed]
- Munnangi, S.; Dupiton, L.; Boutin, A.; Angus, L.D.G. Burnout, Perceived Stress, and Job Satisfaction among Trauma Nurses at a Level I Safety-Net Trauma Center. J. Trauma Nurs. 2018, 25, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Khamisa, N.; Oldenburg, B.; Peltzer, K.; Ilic, D. Work Related Stress, Burnout, Job Satisfaction and General Health of Nurses. Int. J. Environ. Res. Public Health 2015, 12, 652–666. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Zhao, Y.; While, A. Job satisfaction among hospital nurses: A literature review. Int. J. Nurs. Stud. 2019, 94, 21–31. [Google Scholar] [CrossRef]


{kind=link}
| Item Number | Item Content Please Indicate How Frequently You Suffer… |
|---|---|
| 1 | stressful situations derived from the process of dying or death |
| 2 | stressful situations derived from conflicts with doctors |
| 3 | stressful situations derived from lack of support |
| 4 | stressful situations derived from conflict between nurses |
| 5 | stressful situations derived from workload |
| 6 | stressful situations derived from the uncertainty of the treatment |
| Variable | Mean | SD 1 | Minimum | Maximum | λ |
|---|---|---|---|---|---|
| Item 1 | 2.60 | 0.65 | 1.00 | 4.00 | 0.347 |
| Item 2 | 2.35 | 0.67 | 1.00 | 4.00 | 0.338 |
| Item 3 | 1.96 | 0.61 | 1.00 | 4.00 | 0.664 |
| Item 4 | 2.35 | 0.67 | 1.00 | 4.00 | 0.710 |
| Item 5 | 2.74 | 0.75 | 1.00 | 4.00 | 0.478 |
| Item 6 | 2.16 | 0.67 | 1.00 | 4.00 | 0.666 |
| Nursing stress | 2.36 | 0.40 | 1.33 | 3.67 | --- |
| Workload | 2.91 | 0.78 | 1.00 | 4.00 | --- |
| Work control | 2.44 | 1.03 | 1.00 | 4.00 | --- |
| Emotional exhaustion | 17.53 | 8.68 | 2.00 | 45.00 | --- |
| Depersonalization | 4.55 | 3.67 | 0.00 | 19.00 | --- |
| Personal acceptance | 33.30 | 6.22 | 14.00 | 48.00 | --- |
| Work satisfaction | 4.36 | 0.75 | 1.67 | 5.00 | --- |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sansó, N.; Vidal-Blanco, G.; Galiana, L. Development and Validation of the Brief Nursing Stress Scale (BNSS) in a Sample of End-of-Life Care Nurses. Nurs. Rep. 2021, 11, 311-319. https://doi.org/10.3390/nursrep11020030
Sansó N, Vidal-Blanco G, Galiana L. Development and Validation of the Brief Nursing Stress Scale (BNSS) in a Sample of End-of-Life Care Nurses. Nursing Reports. 2021; 11(2):311-319. https://doi.org/10.3390/nursrep11020030
Chicago/Turabian StyleSansó, Noemí, Gabriel Vidal-Blanco, and Laura Galiana. 2021. "Development and Validation of the Brief Nursing Stress Scale (BNSS) in a Sample of End-of-Life Care Nurses" Nursing Reports 11, no. 2: 311-319. https://doi.org/10.3390/nursrep11020030
APA StyleSansó, N., Vidal-Blanco, G., & Galiana, L. (2021). Development and Validation of the Brief Nursing Stress Scale (BNSS) in a Sample of End-of-Life Care Nurses. Nursing Reports, 11(2), 311-319. https://doi.org/10.3390/nursrep11020030