
Assessing the Impact of Obesity on Pregnancy and Neonatal Outcomes among Saudi Women


Abstract
:1. Introduction
Significance of the study
- − What is the effect of obesity on the maternal outcomes among Saudi women?
- − What is the effect of obesity on neonatal outcomes?
2. Methods
2.1. Study Design
Setting
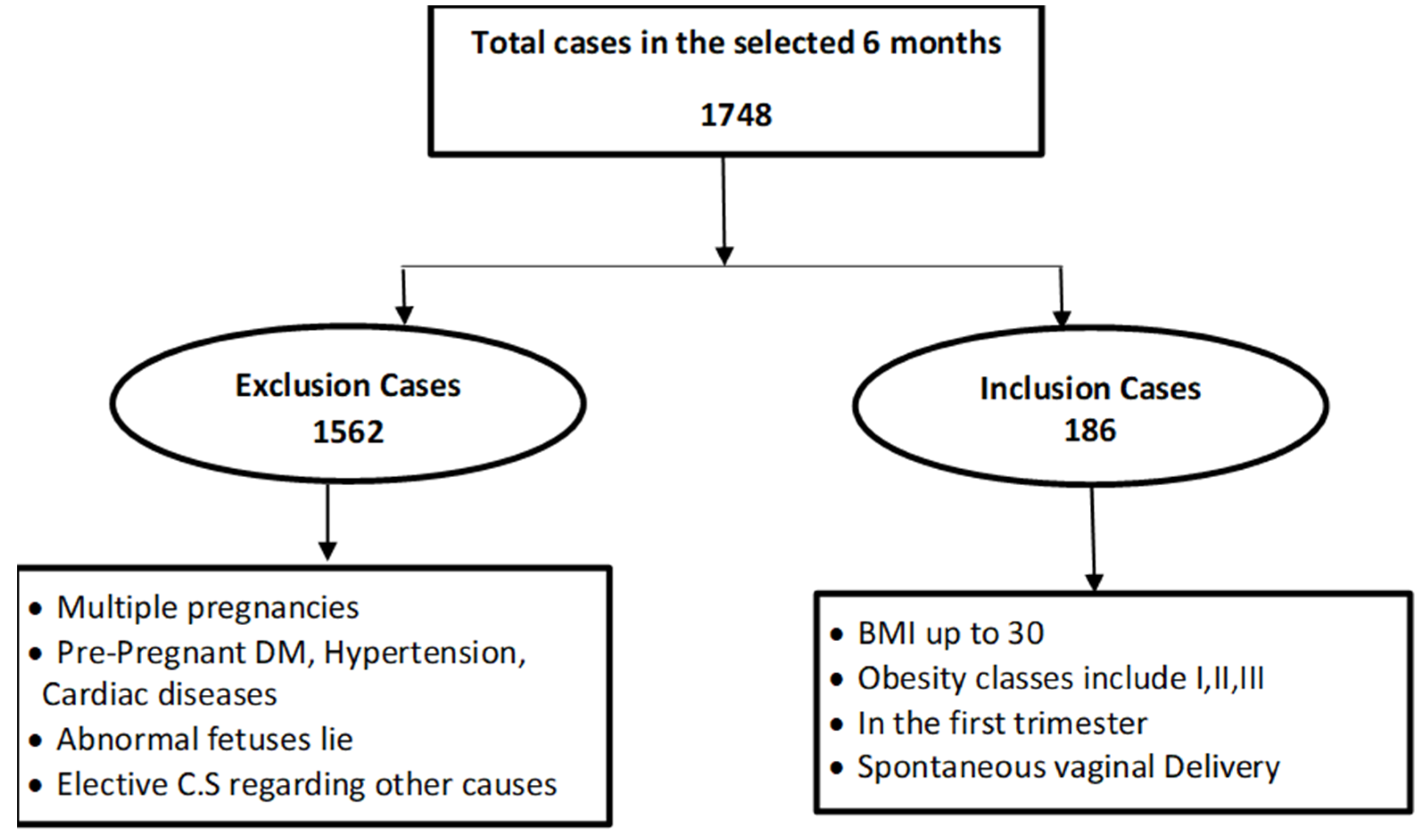
2.2. Participants
2.3. Sample Size
2.4. Data Collection
2.5. Data Collection Instrument
- The first category is sociodemographic and health-related characteristics which include eight subcategories: BMI, maternal age, primigravida, multigravida, mode of the previous delivery, smoking in the current pregnancy, pre-existing thyroid disease, and recurrent miscarriages.
- The second category is the maternal outcomes which divided into two sections:
- The antenatal complication includes four subcategories: Pregnancy-induced hypertension (preeclampsia or eclampsia), gestational diabetes, venous thromboembolism, and urinary tract infection.
- The intra-natal outcomes include twelve subcategories: Gestational age at delivery, preterm labor, induction of labor, augmentation of labor, mode of current delivery, perineal tears (first-degree second degree and third-degree), perineal episiotomy, placental complete or incomplete, duration of 3ed stage of labor, emergency cesarean delivery, postpartum hemorrhage, and prolonged labor.
- The third category is the neonatal outcomes, which includes ten subcategories: Intrauterine growth restriction IUGR, intra-uterine fetal death IUFD, congenital anomalies, preterm baby, shoulder dystocia, stillbirth, APGAR score, neonatal mortality, birth weight (appropriate for gestational age [AGA]-small for gestational age [SGA]-large for gestational age [LGA]) and admission to NICU.
2.6. Validity and Reliability
2.7. Data Management
2.8. Ethical Considerations
3. Results
4. Discussion
5. Limitation of the Study
Generalizability
6. Conclusions
7. Implication for Future Practice
8. Recommendations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- DeNicola, E.; Aburizaiza, O.S.; Siddique, A.; Khwaja, H.; Carpenter, D.O. Obesity and public health in the Kingdom of Saudi Arabia. Rev. Environ. Health 2015, 30, 191–205. [Google Scholar] [CrossRef] [PubMed]
- Paul, E.; Mtumwa, A.H.; Ntwenya, J.E.; Vuai, S.A.H. Disparities in Risk Factors Associated with Obesity between Zanzibar and Tanzania Mainland among Women of Reproductive Age Based on the 2010 TDHS. J. Obes. 2016, 2016, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Gómez-Ambrosi, J.; Silva, C.; Galofré, J.C.; Escalada, J.; Santos, S.; Millán, D.; Vila, N.; Ibañez, P.; Gil, M.J.; Valentí, V.; et al. Body mass index classification misses subjects with increased cardiometabolic risk factors related to elevated adiposity. Int. J. Obes. 2012, 36, 286–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Othman, M.; Himayda, S.S.; Shaaban, L. Obesity and Pregnancy in Saudi Women. Arch. Clin. Med. Case Rep. 2018, 2, 50–55. [Google Scholar] [CrossRef]
- Saudi Ministry of Health. The National Guidelines for Management of Cardio-Metabolic Risk Factors in Primary Health Care; Saudi Ministry of Health: Saudi Arabia, 2014.
- Aljabri, K.S.; Bokhari, S.A.; Khan, A.; Ebu Elsaoud, H.M.; Aljabri, B.K.; Boraie, R.E. Overweight and Obesity in Saudi Women of Childbearing Age. Endocrinol. Metab. Res. 2018, 3, 53–62. [Google Scholar]
- Al-Hamdan, R.; Avery, A.; Salter, A.; Al-Disi, D.; Al-Daghri, N.M.; McCullough, F. Identification of Education Models to Improve Health Outcomes in Arab Women with Pre-Diabetes. Nutrients 2019, 11, 1113. [Google Scholar] [CrossRef] [Green Version]
- Mirabelli, M.; Russo, D.; Brunetti, A. The Role of Diet on Insulin Sensitivity. Nutrients 2020, 12, 3042. [Google Scholar] [CrossRef]
- Davies-Tuck, M.; Mockler, J.C.; Stewart, L.; Knight, M.; Wallace, E.M. Obesity and pregnancy outcomes: Do the relationships differ by maternal region of birth? A retrospective cohort study. BMC Pregnancy Childbirth 2016, 16, 288. [Google Scholar] [CrossRef] [Green Version]
- Al Shanqeeti, S.A.; Alkhudairy, Y.N.; Alabdulwahed, A.A.; Ahmed, A.E.; Al-Adham, M.S.; Mahmood, N.M. Prevalence of subclinical hypothyroidism in pregnancy in Saudi Arabia. Saudi Med. J. 2018, 39, 254–260. [Google Scholar] [CrossRef]
- Ali, H.S.; Lakhani, N. Effect of obesity and its outcome among pregnant women. Pak. J. Med. Sci. 2011, 27, 1126–1128. [Google Scholar]
- Alshahrani, M.; Alqahtani, N.; Alqahtani, A.; Almaqbul, W.; AlWadei, A.; Alzamanan, S.; Salhi, A.; Musallam, S.; Almoqati, S.; Alyami, A.; et al. Overweight and obesity awareness before pregnancy in Najran, Saudi Arabia. Int. J. Med Sci. Public Heal. 2018, 7, 1. [Google Scholar] [CrossRef]
- Sinha, K.; Pandey, S.; Das, C.R. Impact of Maternal Obesity on Pregnancy Outcome. J. Nepalgunj Med Coll. 2018, 14, 18–22. [Google Scholar] [CrossRef]
- Garretto, D.; Lin, B.B.; Syn, H.L.; Judge, N.; Beckerman, K.; Atallah, F.; Friedman, A.; Brodman, M.; Bernstein, P.S. Obesity May Be Protective against Severe Perineal Lacerations. J. Obes. 2016, 2016, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braga, G.C.; Clementino, S.T.P.; Da Luz, P.F.N.; Scavuzzi, A.; Neto, C.N.; Amorim, M.M.R. Risk factors for episiotomy: A case-control study. Revista da Associação Médica Brasileira 2014, 60, 465–472. [Google Scholar] [CrossRef] [Green Version]
- Joseph, N.; Sneha, V.; Nelliyanil, M.; Rai, S.; Supriya, K.; Bhat, K. Awareness of consequences of obesity on reproductive health problems among women in an urban area in South India. IJRCOG 2015, 4, 1109–1116. [Google Scholar] [CrossRef] [Green Version]
- Vittal, D.S.; Rani, V.U. Maternal obesity and its outcome in the fetus. IJAM 2016, 3, 125–129. [Google Scholar] [CrossRef] [Green Version]
- Polit, D.; Beck, C.T. Essentials of Nursing Research Evidence for Nursing Practice; Wolters Kluwer: Hong Kong, China, 2010. [Google Scholar]
- Collares, F.M.; Korevaar, T.I.; Hofman, A.; Steegers, E.A.; Peeters, R.P.; Jaddoe, V.W.; Gaillard, R. Maternal thyroid function, prepregnancy obesity and gestational weight gain-The Generation R Study: A prospective cohort study. Clin. Endocrinol. 2017, 87, 799–806. [Google Scholar] [CrossRef]
- Pop, V.J.; Biondi, B.; Wijnen, H.A.; Kuppens, S.M.; Vader, H.H. Maternal thyroid parameters, body mass index and subsequent weight gain during pregnancy in healthy euthyroid women. Clin. Endocrinol. 2013, 79, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Kahr, M.K.; Antony, K.M.; DelBeccaro, M.; Hu, M.; Aagaard, K.M.; Suter, M.A. Increasing maternal obesity is associated with alterations in both maternal and neonatal thyroid hormone levels. Clin. Endocrinol. 2016, 84, 551–557. [Google Scholar] [CrossRef]
- Zayed, E.S.; Allah, R.K.F.; Shaman, A.A.; Yousef, R.S.; Elsaifi, O.; Bakheit, K.H. The Effects of Maternal Obesity and Gestational Diabetes on the Pregnancy Outcomes. Life Sci. J. 2018, 14, 20–25. [Google Scholar] [CrossRef]
- Young, O.M.; Twedt, R.; Catov, J.M. Pre-pregnancy maternal obesity and the risk of preterm preeclampsia in the American primigravida. Obesity 2016, 24, 1226–1229. [Google Scholar] [CrossRef] [Green Version]
- Marchi, J.; Berg, M.V.D.; Dencker, A.; Olander, E.K.; Begley, C. Risks associated with obesity in pregnancy, for the mother and baby: A systematic review of reviews. Obes. Rev. 2015, 16, 621–638. [Google Scholar] [CrossRef]
- Paré, E.; Parry, S.; McElrath, T.F.; Pucci, D.; Newton, A.; Lim, K.-H. Clinical Risk Factors for Preeclampsia in the 21st Century. Obstet. Gynecol. 2014, 124, 763–770. [Google Scholar] [CrossRef]
- Salihu, H.M.; De La Cruz, C.; Rahman, S.; August, E.M. Does maternal obesity cause preeclampsia? A systematic review of the evidence. Minerva Ginecol. 2012, 64, 259–280. [Google Scholar]
- Blomberg, M. Maternal Body Mass Index and Risk of Obstetric Anal Sphincter Injury. BioMed Res. Int. 2014, 2014, 1–8. [Google Scholar] [CrossRef]
- Gaillard, R.; AP Steegers, E.; Hofman, A.; Jaddoe, V.W. Associations of maternal obesity with blood pressure and the risks of gestational hypertensive disorders. The Generation R Study. J. Hypertens. 2011, 29, 937–944. [Google Scholar] [CrossRef]
- Durnea, C.M.; Jaffery, A.E.; Gauthaman, N.; Doumouchtsis, S.K. Effect of body mass index on the incidence of perineal trauma. Int. J. Gynecol. Obstet. 2017, 141, 166–170. [Google Scholar] [CrossRef]
- Al Ghamdi, T.; Al Thaydi, A.H.; Chamsi, A.T.; Al Mardawi, E. Incidence and Risk Factors for Development of Third and Fourth Degree Perineal Tears: A Four Year Experience in a Single Saudi Center. J. Women’s Heal. Care 2018, 7, 1–4. [Google Scholar] [CrossRef]
- Kamel, H.A.H.; Ibrahim, A.S.M.; Abdo, M.M. Maternal Obesity and Its Effect in Late Pregnancy and Labour. Egypt. J. Hosp. Med. 2018, 71, 2982–2988. [Google Scholar]
- Lindholm, E.; Altman, D. Risk of obstetric anal sphincter lacerations among obese women. BJOG: Int. J. Obstet. Gynaecol. 2013, 120, 1110–1115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anzaku, A.; Idikwu, O.; Emmanuel, O.; Kingsley, O. Impacts of Obesity on Maternal and Fetal Outcomes in Women with Singleton Pregnancy at a Nigerian Clinical Setting. Br. J. Med. Med Res. 2015, 6, 1159–1165. [Google Scholar] [CrossRef]
- Onubi, O.J.; Marais, D.; Aucott, L.; Okonofua, F.; Poobalan, A.S. Maternal obesity in Africa: A systematic review and meta-analysis. J. Public Health 2016, 38, e218–e231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiefari, E.; Quaresima, P.; Visconti, F.; Mirabelli, M.; Brunetti, A. Gestational diabetes and fetal overgrowth: Time to rethink screening guidelines. Lancet Diabetes Endocrinol. 2020, 8, 561–562. [Google Scholar] [CrossRef]
- Quaresima, P.; Visconti, F.; Chiefari, E.; Mirabelli, M.; Borelli, M.; Caroleo, P.; Foti, D.; Puccio, L.; Venturella, R.; Di Carlo, C.; et al. Appropriate Timing of Gestational Diabetes Mellitus Diagnosis in Medium- and Low-Risk Women: Effectiveness of the Italian NHS Recommendations in Preventing Fetal Macrosomia. J. Diabetes Res. 2020, 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Categories | N = 186 | % |
|---|---|---|---|
| Age | Less 24 | 15 | 8.1 |
| 25–29 | 53 | 28.5 | |
| 30–34 | 50 | 26.9 | |
| 35–39 | 45 | 24.2 | |
| 40–45 | 23 | 12.4 | |
| Primigravida | Yes | 31 | 16.7 |
| Multigravida | Yes | 155 | 83.3 |
| Previous delivery | SVD (Spontaneous vaginal delivery) | 126 | 67.7 |
| CS (Caesarean section) | 26 | 14.0 | |
| Obesity | (Primigravida) | 31 | 16.7 |
| Class I (BMI 30–34) | 128 | 68.8 | |
| Class II (BMI 35–39) | 44 | 23.7 | |
| Class III (BMI more than 40) | 14 | 7.5 | |
| Current Smoking | Yes | 4 | 2.2 |
| Pre-existing thyroid diseaseRecurrent miscarriages | No | 182 | 97.8 |
| Yes | 16 | 8.6 | |
| No | 170 | 90.4 | |
| Yes | 10 | 5.4 | |
| No | 176 | 93.6 |
| KERRYPNX | Obesity | |||
|---|---|---|---|---|
| Class I (BMI 3–34 kg/m2) n = 128 (%) | Class II (BMI 35–39.9kg/m2) n = 44 (%) | Class III (BMI > 40.0 kg/m2) n = 14 (%) | p Value * | |
| Pre-existing thyroid disease | 0.015 * | |||
| Yes | 16 (12.5) | 0 | 0 | |
| No | 112 (87.5) | 44 (100) | 14 (100) | |
| Pregnancy induced hypertension | 0.075 | |||
| Yes | 0 | 0 | 1 (7.1) | |
| No | 128 (100) | 44 (100) | 13 (92.9) | |
| Gestational diabetes | 0.624 | |||
| Yes | 29 (22.7) | 12 (27.3) | 12 (27.3) | |
| No | 99 (77.3) | 32 (72.7) | 32 (72.7) | |
| Urinary tract infection | 0.528 | |||
| Yes | 1 (0.8) | 1 (2.3) | 0 | |
| No | 127 (99.2) | 43 (97.7) | 14 (100) | |
| Perineal tear | 0.020 * | |||
| First degree | 45 (35.2) | 13 (29.5) | 1 (7.1) | |
| Second degree | 24 (18.8) | 4 (9.1) | 4 (28.6) | |
| Third degree | 1(0.8) | 0 | 0 | |
| Intact | 55 (43.0) | 24(54.5) | 6(42.9) | |
| Episiotomy | 0.037 * | |||
| Yes | 5 (3.9) | 3 (6.8) | 3(21.4) | |
| No | 123 (96.1) | 41 (93.2) | 11 (78.6) | |
| Induction of Labor | 33 (25.8) | 11 (25.0) | 5 (35.7) | 0.730 |
| Augmentation of labor | 26 (20.3) | 9 (20.5) | 6 (42.9) | 0.163 |
| Method of Delivery | ||||
| spontaneous vaginal delivery (SVD) | 97 (75.8) | 31 (70.5) | 9 (64.3) | 0.505 |
| Instrumental | 8 (6.3) | 2 (4.5) | 0 | |
| Caesarean section (CS) | 23 (18.0) | 11 (25.0) | 5 (35.7) | 0.112 |
| Labor complications | ||||
| postpartum haemorrhage | ||||
| Yes | 3 (2.3) | 1 (2.3) | 1 (7.1) | 0.399 |
| Obesity | ||||
|---|---|---|---|---|
| Class I (BMI 30–34 kg/m2) n = 128(%) | Class II (BMI 35.0–39.9kg/m2) 44 (%) | Class III (BMI—40.0 kg/m2) n = 14 (%) | p Value * | |
| Gestational age | 0.325 | |||
| Preterm | 10 (7.8) | 3 (6.8) | 0 | |
| Full term | 117 (91.4) | 41 (93.2) | 13 (92.9) | |
| Post date | 1 (0.8) | 0 | 1 (7.1) | |
| IUFD | 0 | 1 (2.3) | 0 | 0.312 |
| Preterm baby | 10 (7.8) | 3 (6.8) | 0 | 0.894 |
| APGAR score | 0.751 | |||
| 0–2 need resuscitation | 1 (0.8) | 1 (2.3) | 0 | |
| 3–6 stimulation | 3 (2.3) | 1 (2.3) | 0 | |
| 7–10 no action | 124 (96.9) | 42 (95.5) | 14 (100) | |
| Birth weight | 1.000 | |||
| AGA (Appropriate for gestational age) | 108 (84.4) | 38 (86.4) | 13 (92.9) | |
| SGA (Small for gestational age) | 12 (9.4) | 4 (9.1) | 1 (7.1) | |
| LGA (Large for gestational age) | 8 (6.3) | 2 (4.5) | 0 | |
| Admission to NICU | 4 (3.1) | 1 (2.3) | 0 | 1.000 |
| Neonatal mortality | 0 | 1 (2.3) | 0 | 0.312 |
| Obesity | Test Statistic | Pre-Existing Thyroid Disease | p Value |
|---|---|---|---|
| Class I-class II | −11.625 | 0.033 * | |
| Class I-class III | −11.625 | 0.343 | |
| Class II-class III | 0.000 | 1.000 | |
| Obesity | Induced Hypertension Test Statistic | p Value | |
| Class III-class I | 6.643 | 0.001 ** | |
| Class III-class II | 6.643 | 0.001 ** | |
| Class I-class II | 0.000 | 1.000 | |
| Obesity | Perineal tears Test Statistic | p Value | |
| Class I-class II | −14.077 | 0.108 | |
| Class I-class III | −32.876 | 0.020 * | |
| Class II-class III | −18.799 | 0.222 | |
| Obesity | Episiotomy Test Statistic | p Value | |
| Class III-class II | 13.588 | 0.044 | |
| Class III-class I | 16.296 | 0.008 * | |
| Class II-class I | 2.708 | 0.481 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adwani, N.; Fouly, H.; Omer, T. Assessing the Impact of Obesity on Pregnancy and Neonatal Outcomes among Saudi Women. Nurs. Rep. 2021, 11, 279-290. https://doi.org/10.3390/nursrep11020027
Adwani N, Fouly H, Omer T. Assessing the Impact of Obesity on Pregnancy and Neonatal Outcomes among Saudi Women. Nursing Reports. 2021; 11(2):279-290. https://doi.org/10.3390/nursrep11020027
Chicago/Turabian StyleAdwani, Nadia, Howieda Fouly, and Tagwa Omer. 2021. "Assessing the Impact of Obesity on Pregnancy and Neonatal Outcomes among Saudi Women" Nursing Reports 11, no. 2: 279-290. https://doi.org/10.3390/nursrep11020027
APA StyleAdwani, N., Fouly, H., & Omer, T. (2021). Assessing the Impact of Obesity on Pregnancy and Neonatal Outcomes among Saudi Women. Nursing Reports, 11(2), 279-290. https://doi.org/10.3390/nursrep11020027