
Evolution of Hyperventilation-Induced Nystagmus in Acute Unilateral Vestibulopathy—Interpretative Model and Etiopathogenetic Hypotheses

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
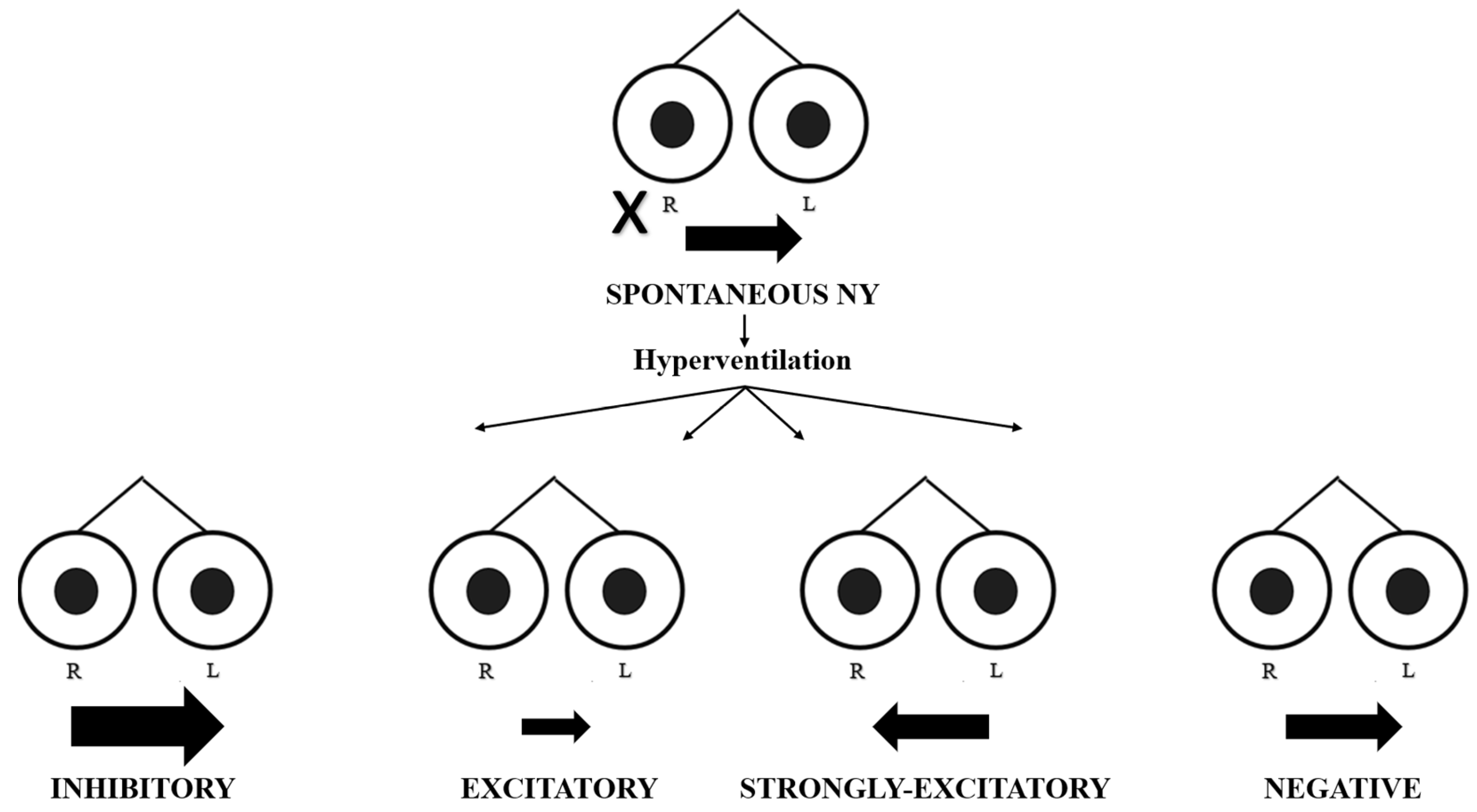
- In the presence of spontaneous nystagmus:
- -
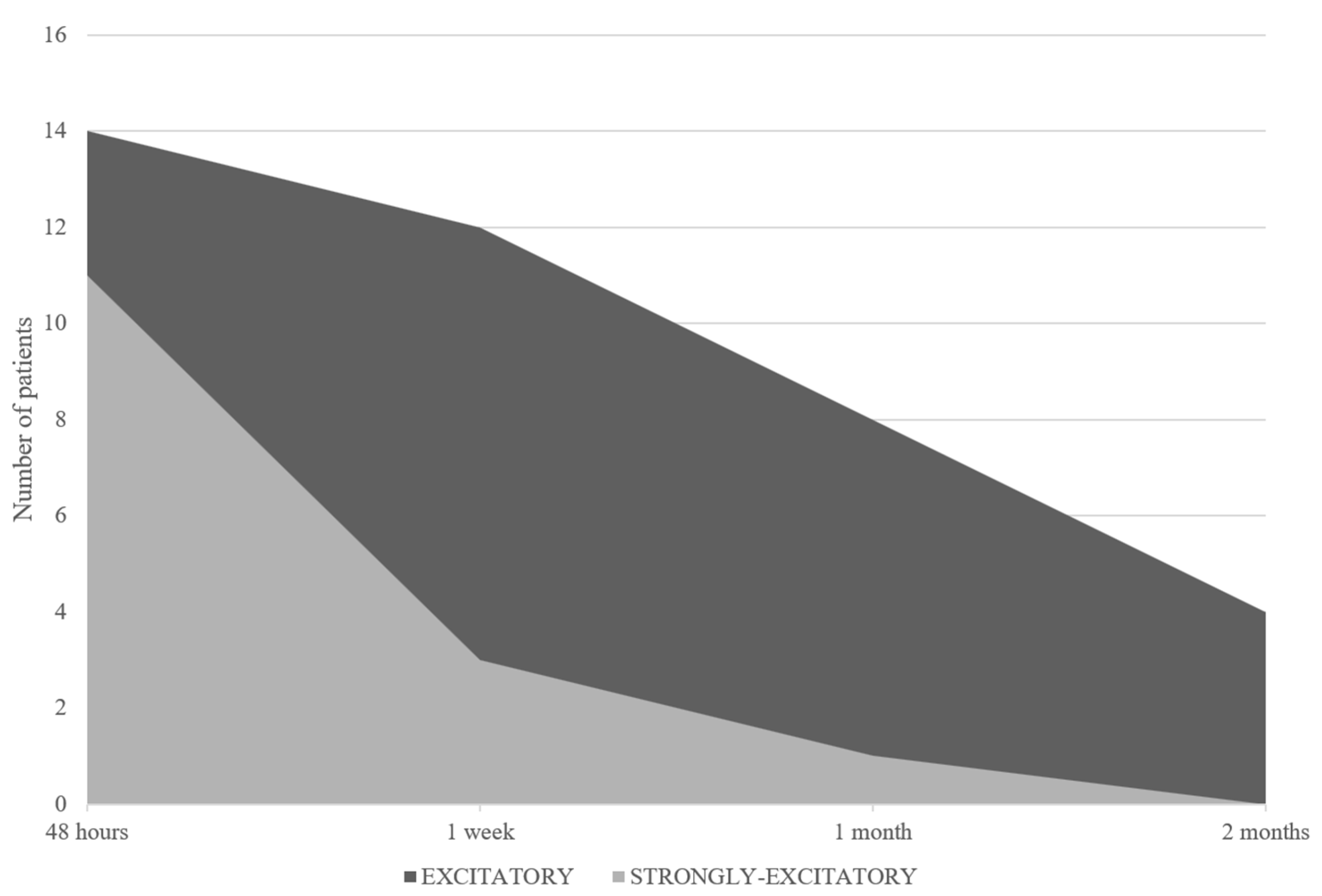
- Excitatory pattern = reduction in or reversal of nystagmus (in the case of reversal of nystagmus, we named the oculomotor pattern “strongly excitatory”);
- -
- Inhibitory pattern = increase in nystagmus intensity and frequency;
- -
- Negative pattern = no changes induced in nystagmus.
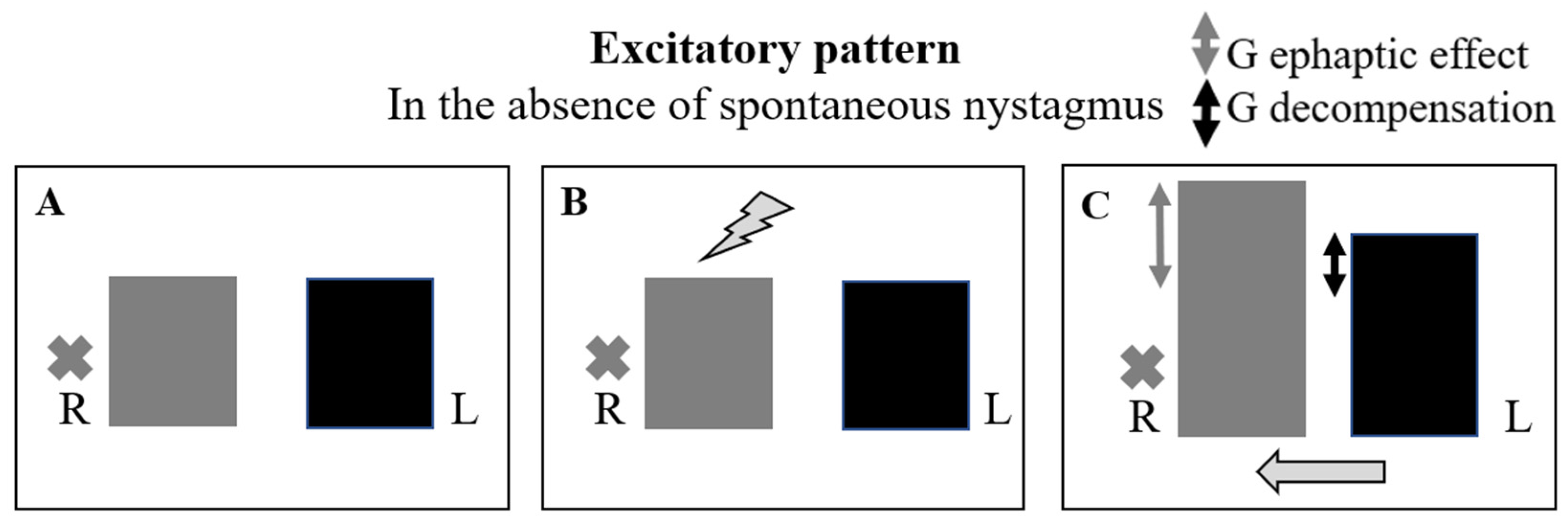
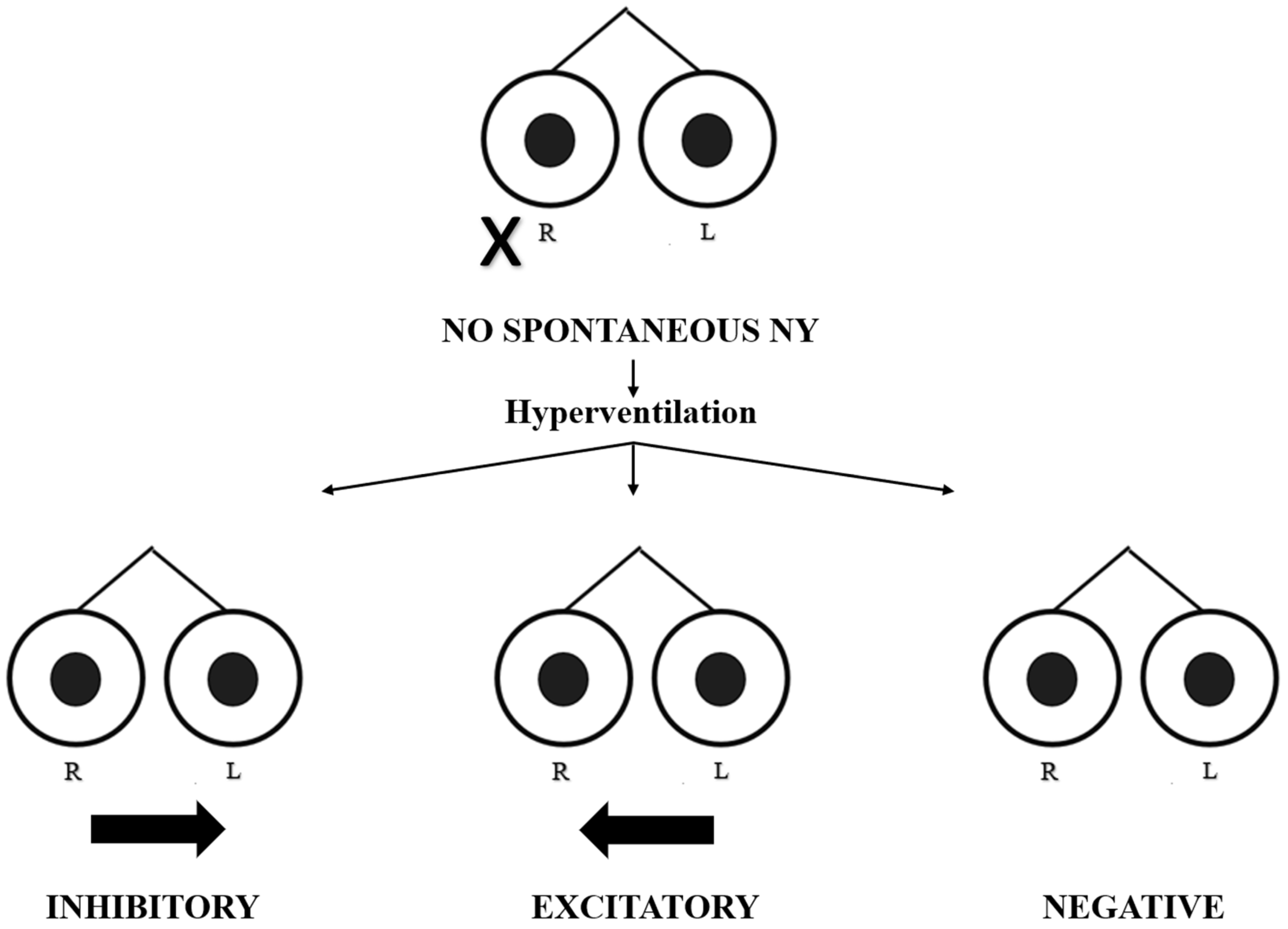
- In the absence of spontaneous nystagmus:
- -
- Excitatory pattern = induction of nystagmus beating towards the affected side;
- -
- Inhibitory pattern = induction of nystagmus beating towards the unaffected side;
- -
- Negative pattern = no nystagmus evoked.
3. Results
4. Discussion
4.1. Evoked Excitatory or Strongly Excitatory Oculomotor Pattern in the Presence of Spontaneous Nystagmus (Figure 5 and Table 3)


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ocular Pattern | Ephaptic Effect | Decompensation | Hypotesis |
|---|---|---|---|
| Excitatory or Strongly-Excitatory | Present | Absent or present but inferior to the ephaptic effect | NEURITIC |
4.2. Evoked Excitatory Oculomotor Pattern in the Absence of Spontaneous Nystagmus (Figure 6 and Table 3)
4.3. Evoked Inhibitory Oculomotor Pattern in the Presence of Spontaneous Nystagmus (Figure 7 and Table 4)

| Ocular Pattern | Ephaptic Effect | Decompensation | Hypotesis |
|---|---|---|---|
| Inhibitory | Present | Present and superior to the ephaptic effect | NEURITIC |
| Absent | Present | VASCULAR |
4.4. Evoked Inhibitory Oculomotor Pattern in the Absence of Spontaneous Nystagmus (Figure 8 and Table 4)

4.5. Negative Oculomotor Pattern in the Presence of Spontaneous Nystagmus (Table 5)
| Ocular Pattern | Ephaptic Effect | Decompensation | Hypotesis |
|---|---|---|---|
| Negative | Present | Present and equal to the ephaptic effect | NEURITIC |
| Absent | No compensation | VASCULAR | |
| Not evocable (ineffective test) | Not evocable (ineffective test) | NEURITIC/VASCULAR | |
| In the presence of spontaneous nystagmus | |||
4.6. Negative Oculomotor Pattern in the Absence of Spontaneous Nystagmus (Table 6)
| Ocular Pattern | Ephaptic Effect | Decompensation | Hypotesis |
|---|---|---|---|
| Negative | Not evocable (ineffective test) | Not evocable (ineffective test) | NEURITIC/ VASCULAR |
| Negative but previously excitatory or inhibitory | Previously present/absent (restitutio ad integrum) | Previously present/absent (restitutio ad integrum) | NEURITIC/ VASCULAR |
| In the absence of spontaneous nystagmus | |||
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Califano, L.; Mazzone, S.; Salafia, F. Utility of the hyperventilation test in the evaluation of the dizzy patient. Curr. Opin. Otolaryngol. Head Neck Surg. 2013, 21, 487–491. [Google Scholar] [CrossRef] [PubMed]
- Bance, M.L.; O’Driscoll, M.; Patel, N.; Ramsden, R.T. Vestibular disease unmasked by hyperventilation. Laryngoscope 1998, 108 Pt 1, 610–614, Erratum in Laryngoscope 1998, 108, 948. [Google Scholar] [CrossRef] [PubMed]
- Sakellari, V.; Bronstein, A.M.; Corna, S.; Hammon, C.A.; Jones, S.; Wolsley, C.J. The effects of hyperventilation on postural control mechanisms. Brain 1997, 120 Pt 9, 1659–1673. [Google Scholar] [CrossRef] [PubMed]
- Califano, L.; Iorio, G.; Salafia, F.; Mazzone, S.; Califano, M. Hyperventilation-Induced Nystagmus in Patients with Vestibular Schwannoma. Otol. Neurotol. 2015, 36, 303–306. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.H.; Jeong, K.H.; Ahn, S.H.; Shin, D.H.; Kim, Y.W.; Shin, J.E. Vibration- and hyperventilation-induced nystagmus in patients with Ramsay Hunt syndrome with vertigo. Otolaryngol. Head Neck Surg. 2015, 152, 912–918. [Google Scholar] [CrossRef] [PubMed]
- Califano, L.; Melillo, M.G.; Vassallo, A.; Mazzone, S. Hyperventilation-induced nystagmus in a large series of vestibular patients. Acta Otorhinolaryngol. Ital. 2011, 31, 17–26. [Google Scholar] [PubMed] [PubMed Central]
- Strupp, M.; Bisdorff, A.; Furman, J.; Hornibrook, J.; Jahn, K.; Maire, R.; Newman-Toker, D.; Magnusson, M. Acute unilateral vestibulopathy/vestibular neuritis: Diagnostic criteria. J. Vestib. Res. 2022, 32, 389–406. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bae, C.H.; Na, H.G.; Choi, Y.S. Current diagnosis and treatment of vestibular neuritis: A narrative review. J. Yeungnam Med. Sci. 2022, 39, 81–88. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Le, T.N.; Westerberg, B.D.; Lea, J. Vestibular Neuritis: Recent Advances in Etiology, Diagnostic Evaluation, and Treatment. Adv. Otorhinolaryngol. 2019, 82, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Califano, L.; Locatelli, G.; Melillo, M.G. Can hyperventilation test and duration of spontaneous nystagmus help differentiate between vascular and inflammatory aetiology of acute unilateral vestibular deficit? Acta Otorhinolaryngol. Ital. 2022, 42, 560–568. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chiang, C.C.; Shivacharan, R.S.; Wei, X.; Gonzalez-Reyes, L.E.; Durand, D.M. Slow periodic activity in the longitudinal hippocampal slice can self-propagate non-synaptically by a mechanism consistent with ephaptic coupling. J. Physiol. 2019, 597, 249–269. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Anastassiou, C.A.; Perin, R.; Markram, H.; Koch, C. Ephaptic coupling of cortical neurons. Nat. Neurosci. 2011, 14, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Gatti, A.; Nartallo-Kaluarachchi, R.; Uppal, A.; Benedusi, P. Computational Modeling of Ephaptic coupling in Myelinated and Unmyelinated Axon Bundles Using the EMI Framework. In Computational Physiology; Simula Springer Briefs on Computing; McCabe, K.J., Ed.; Springer: Berlin/Heidelberg, Germany, 2024; Volume 17. [Google Scholar] [CrossRef]
- Ori, M.; Gambacorta, V.; Ricci, G.; Faralli, M. Vestibular Paroxysmia in Vestibular Neuritis: A Case Report. Audiol. Res. 2018, 8, 206. [Google Scholar] [CrossRef] [PubMed]
- Paterson, J.; Menzies, J.; Bergquist, F.; Dutia, M. Cellular Mechanisms of Vestibular Compensation. Neuroembryol. Aging 2004, 3, 183–193. [Google Scholar] [CrossRef]
- Dutia, M. Mechanisms of vestibular compensation: Recent advances. Curr. Opin. Otolaryngol. Head Neck Surg. 2010, 18, 420–424. [Google Scholar] [CrossRef] [PubMed]
- Barmack, N.; Qian, Z.; Kim, H.; Yoshimura, J. Activity-dependent distribution of protein kinase C-δ Within rat cerebellar Purkinje cells following unilateral labyrinthectomy. Exp. Brain Res. 2001, 141, 6–20. [Google Scholar] [CrossRef] [PubMed]
- Waissbluth, S.; Becker, J.; Sepúlveda, V.; Iribarren, J.; García-Huidobro, F. Benign Paroxysmal Positional Vertigo Secondary to Acute Unilateral Peripheral Vestibulopathy: Evaluation of Cardiovascular Risk Factors. J. Int. Adv. Otol. 2023, 19, 28–32. [Google Scholar] [CrossRef] [PubMed]

| Patient | Nystagmus (1° Test) | Pattern (1° Test) | Nystagmus (2° Test) | Pattern (2° Test) | Nystagmus (3° Test) | Pattern (3° Test) | Nystagmus (4° Test) | Pattern (4° Test) |
|---|---|---|---|---|---|---|---|---|
| 1 | Present | Excitatory | Present | Excitatory | Present | Excitatory | Absent | Negative |
| 2 | Present | Excitatory | Present | Inhibitory | Absent | Inhibitory | Absent | Inhibitory |
| 3 | Present | Inhibitory | Present | Inhibitory | Present | Inhibitory | Absent | Inhibitory |
| 4 | Present | Strongly-Excitatory | Present | Strongly-Excitatory | Present | Strongly-Excitatory | Present | Excitatory |
| 5 | Present | Inhibitory | Present | Inhibitory | Absent | Inhibitory | Absent | Inhibitory |
| 6 | Present | Excitatory | Present | Inhibitory | Absent | Negative | Absent | Negative |
| 7 | Present | Strongly-Excitatory | Present | Excitatory | Absent | Inhibitory | Absent | Inhibitory |
| 8 | Present | Strongly-Excitatory | Present | Excitatory | Absent | Excitatory | Absent | Inhibitory |
| 9 | Present | Excitatory | Present | Inhibitory | Present | Inhibitory | Absent | Inhibitory |
| 10 | Present | Negative | Absent | Negative | Absent | Negative | Absent | Negative |
| 11 | Present | Inhibitory | Present | Inhibitory | Present | Inhibitory | Present | Inhibitory |
| 12 | Present | Excitatory | Present | Excitatory | Present | Inhibitory | Absent | Inhibitory |
| 13 | Present | Strongly-Excitatory | Present | Excitatory | Absent | Inhibitory | Absent | Inhibitory |
| 14 | Present | Strongly-Excitatory | Present | Excitatory | Present | Excitatory | Absent | Inhibitory |
| 15 | Present | Negative | Present | Negative | Present | Negative | Present | Negative |
| 16 | Present | Excitatory | Present | Inhibitory | Absent | Inhibitory | Absent | Inhibitory |
| 17 | Present | Strongly-Excitatory | Present | Excitatory | Present | Inhibitory | Absent | Inhibitory |
| 18 | Present | Strongly-Excitatory | Present | Excitatory | Present | Excitatory | Present | Inhibitory |
| 19 | Present | Inhibitory | Present | Inhibitory | Absent | Inhibitory | Absent | Inhibitory |
| 20 | Present | Strongly-Excitatory | Present | Excitatory | Absent | Excitatory | Absent | Excitatory |
| 21 | Present | Excitatory | Present | Inhibitory | Present | Inhibitory | Present | Inhibitory |
| 22 | Present | Inhibitory | Present | Inhibitory | Absent | Inhibitory | Absent | Inhibitory |
| 23 | Present | Excitatory | Present | Inhibitory | Present | Inhibitory | Present | Inhibitory |
| 24 | Present | Inhibitory | Absent | Inhibitory | Absent | Inhibitory | Absent | Inhibitory |
| 25 | Present | Strongly-Excitatory | Present | Excitatory | Present | Excitatory | Absent | Inhibitory |
| 26 | Present | Excitatory | Present | Inhibitory | Absent | Inhibitory | Absent | Inhibitory |
| 27 | Present | Excitatory | Present | Excitatory | Present | Inhibitory | Present | Inhibitory |
| 28 | Present | Inhibitory | Present | Inhibitory | Absent | Negative | Absent | Negative |
| 29 | Present | Strongly-Excitatory | Present | Strongly-Excitatory | Present | Excitatory | Present | Excitatory |
| 30 | Present | Excitatory | Present | Inhibitory | Absent | Inhibitory | Absent | Inhibitory |
| 31 | Present | Excitatory | Present | Inhibitory | Present | Inhibitory | Absent | Inhibitory |
| 32 | Present | Negative | Absent | Negative | Absent | Negative | Absent | Negative |
| 33 | Present | Excitatory | Present | Inhibitory | Absent | Inhibitory | Absent | Negative |
| 34 | Present | Strongly-Excitatory | Present | Strongly-Excitatory | Present | Excitatory | Present | Excitatory |
| 35 | Present | Excitatory | Present | Excitatory | Absent | Inhibitory | Absent | Inhibitory |
| Test | Spontaneous Nystagmus | No Sspontaneous nNystagmus | Positive HVIN Test | Negative HVIN Test | Incidence % Positive HVIN Test/ Spontaneous Nystagmus | Incidence % Positive HVIN Test/ No Spontaneous Nystagmus |
|---|---|---|---|---|---|---|
| 1st | 35 | 0 | 32 | 3 | 91.4% | 0% |
| 2nd | 32 | 3 | 32 | 3 | 96.8% | 33.3% |
| 3rd | 17 | 18 | 30 | 5 | 94.1% | 77.7% |
| 4th | 9 | 26 | 28 | 7 | 88.8% | 76.9% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frati, F.; D’Orazio, A.; Gambacorta, V.; Ciacca, G.; Ricci, G.; Faralli, M. Evolution of Hyperventilation-Induced Nystagmus in Acute Unilateral Vestibulopathy—Interpretative Model and Etiopathogenetic Hypotheses. Audiol. Res. 2024, 14, 442-456. https://doi.org/10.3390/audiolres14030037
Frati F, D’Orazio A, Gambacorta V, Ciacca G, Ricci G, Faralli M. Evolution of Hyperventilation-Induced Nystagmus in Acute Unilateral Vestibulopathy—Interpretative Model and Etiopathogenetic Hypotheses. Audiology Research. 2024; 14(3):442-456. https://doi.org/10.3390/audiolres14030037
Chicago/Turabian StyleFrati, Francesco, Alessandra D’Orazio, Valeria Gambacorta, Giacomo Ciacca, Giampietro Ricci, and Mario Faralli. 2024. "Evolution of Hyperventilation-Induced Nystagmus in Acute Unilateral Vestibulopathy—Interpretative Model and Etiopathogenetic Hypotheses" Audiology Research 14, no. 3: 442-456. https://doi.org/10.3390/audiolres14030037
APA StyleFrati, F., D’Orazio, A., Gambacorta, V., Ciacca, G., Ricci, G., & Faralli, M. (2024). Evolution of Hyperventilation-Induced Nystagmus in Acute Unilateral Vestibulopathy—Interpretative Model and Etiopathogenetic Hypotheses. Audiology Research, 14(3), 442-456. https://doi.org/10.3390/audiolres14030037