
Towards Auditory Profile-Based Hearing-Aid Fittings: BEAR Rationale and Clinical Implementation

 ,
,  , , ,
, , , 
Abstract
1. Introduction
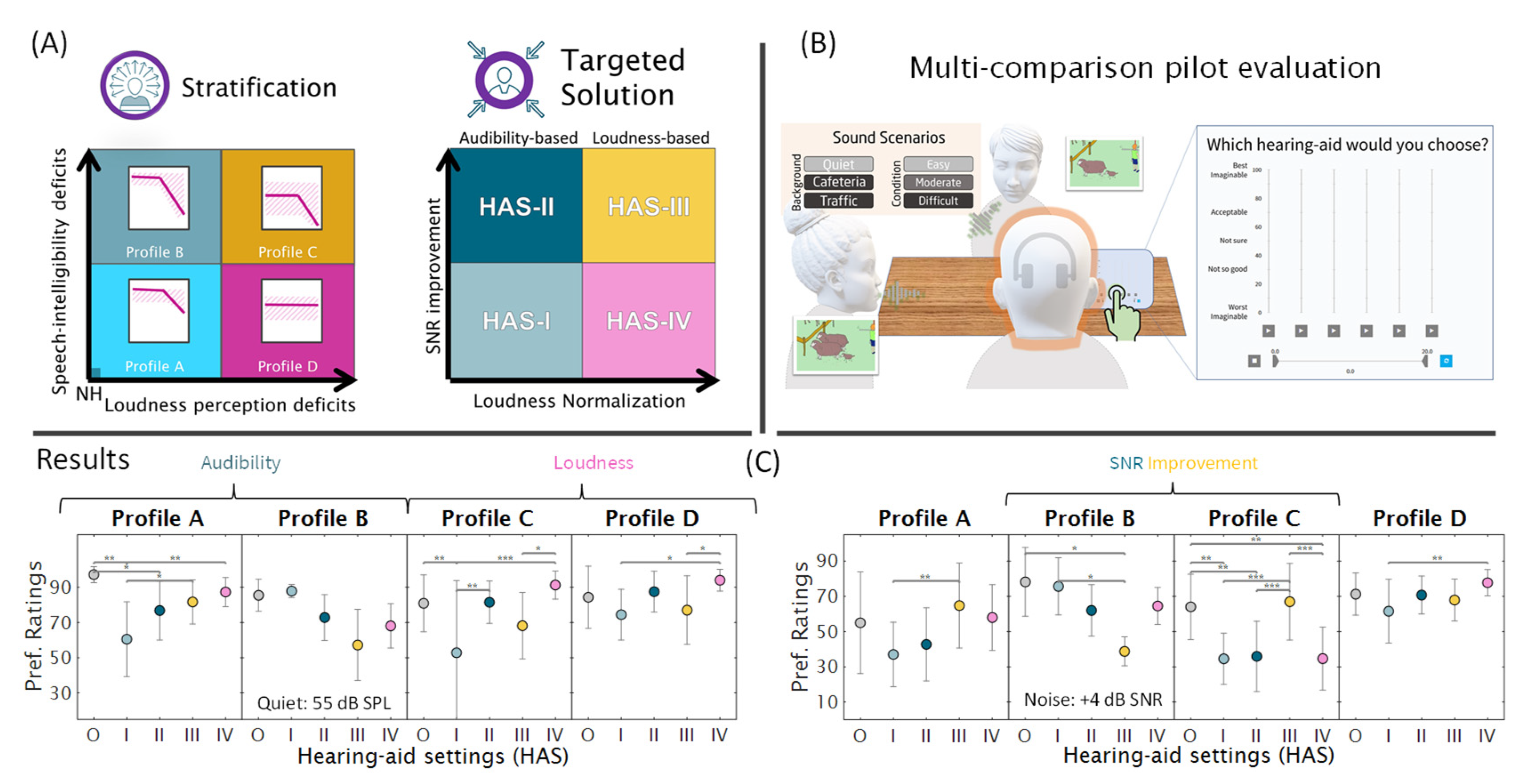
2. The BEAR Rationale at a Glance
3. Challenges to the Clinical BEAR Implementation
- Commercial fitting tools were not suited for the implementation, as they could not readily accommodate all required HA settings.
- While REM could be used for verifying IG targets, no clinically feasible method for verifying SNR improvement targets is currently available.
- The BEAR strategy had to be sufficiently different from the current HA fitting strategy to warrant a formal investigation into its perceptual benefits.
- The HA solutions for the four auditory profiles had to be sufficiently different from each other to warrant a formal investigation into their perceptual benefits.
4. Methods
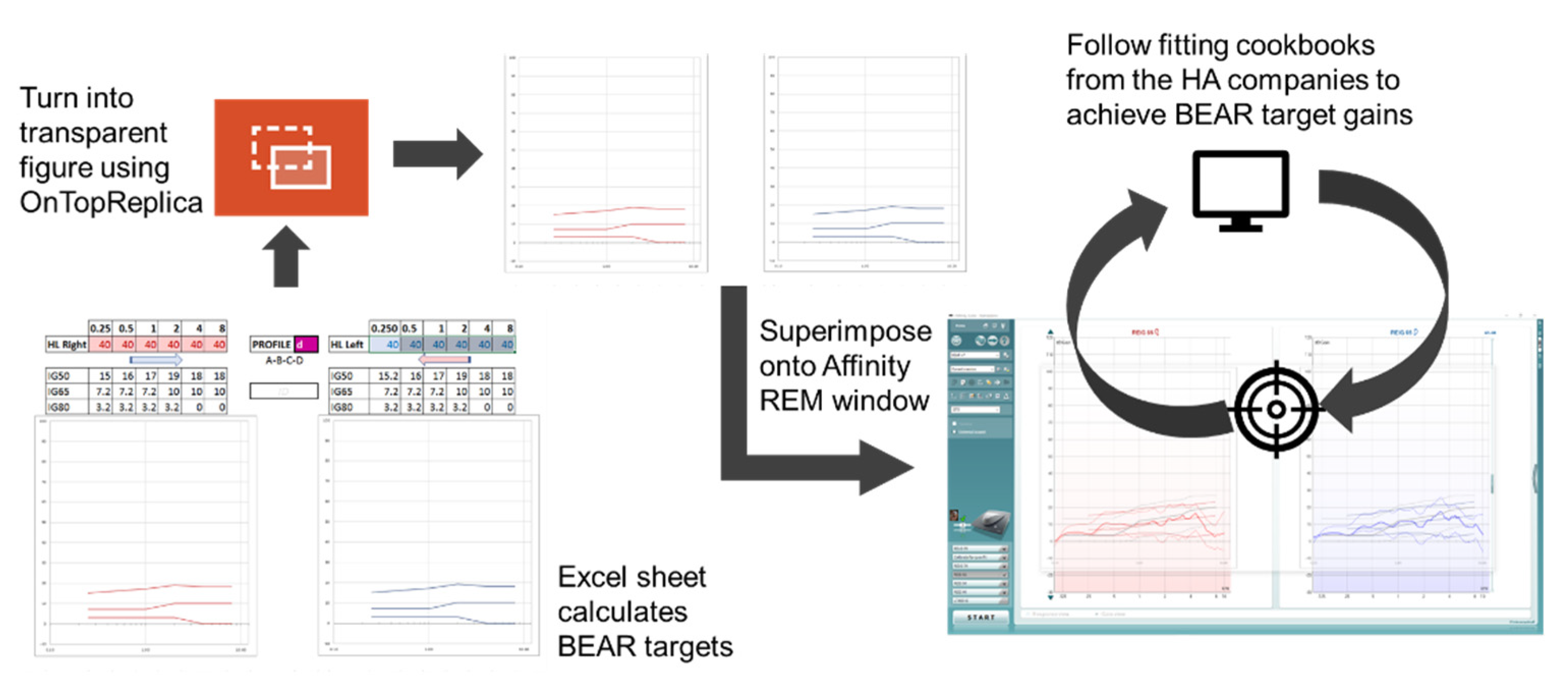
4.1. Clinical Fitting Tool
4.2. Real-Ear Insertion Gain Measurements
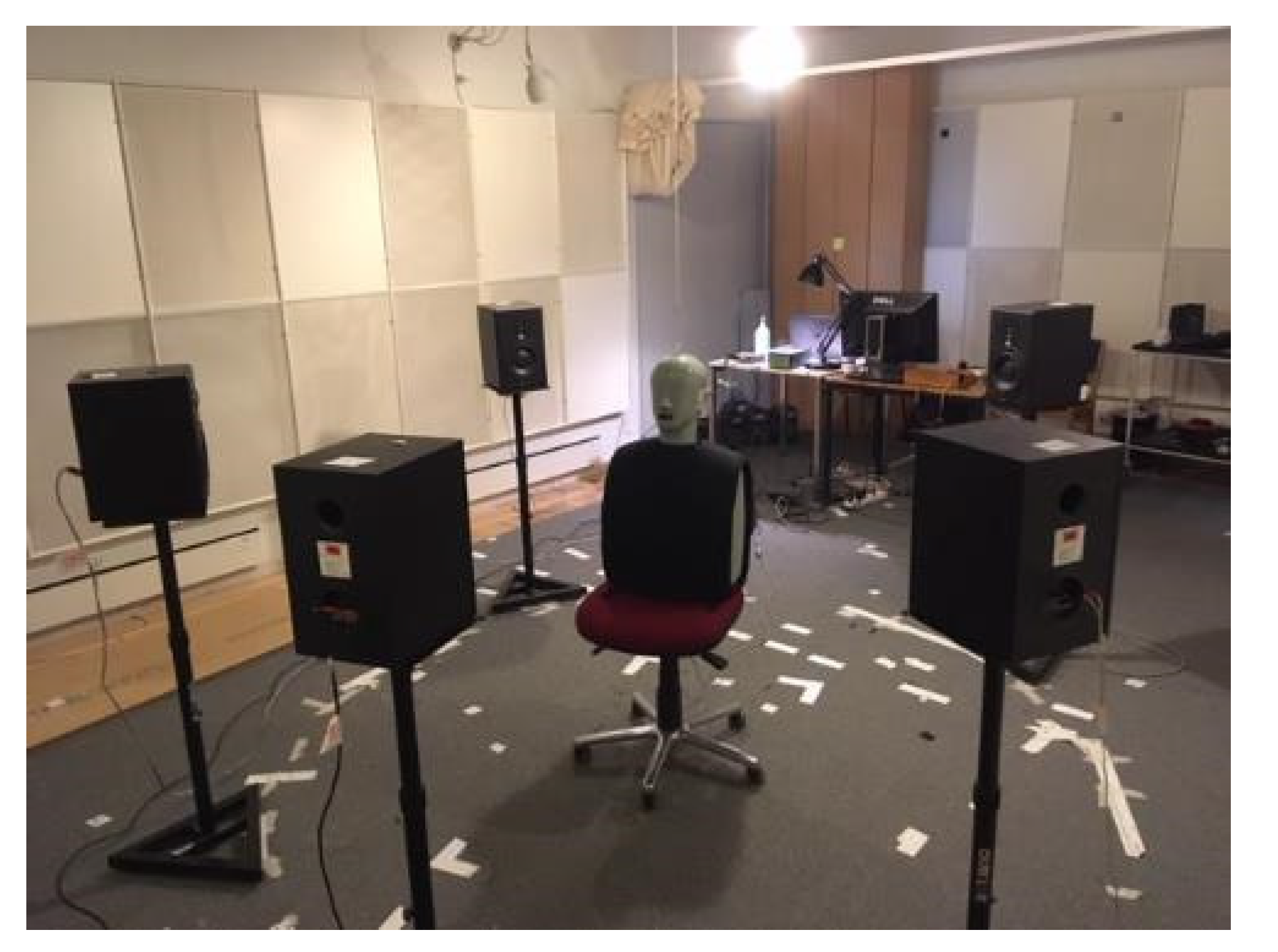
4.3. SNR Improvement Measurements
5. Results
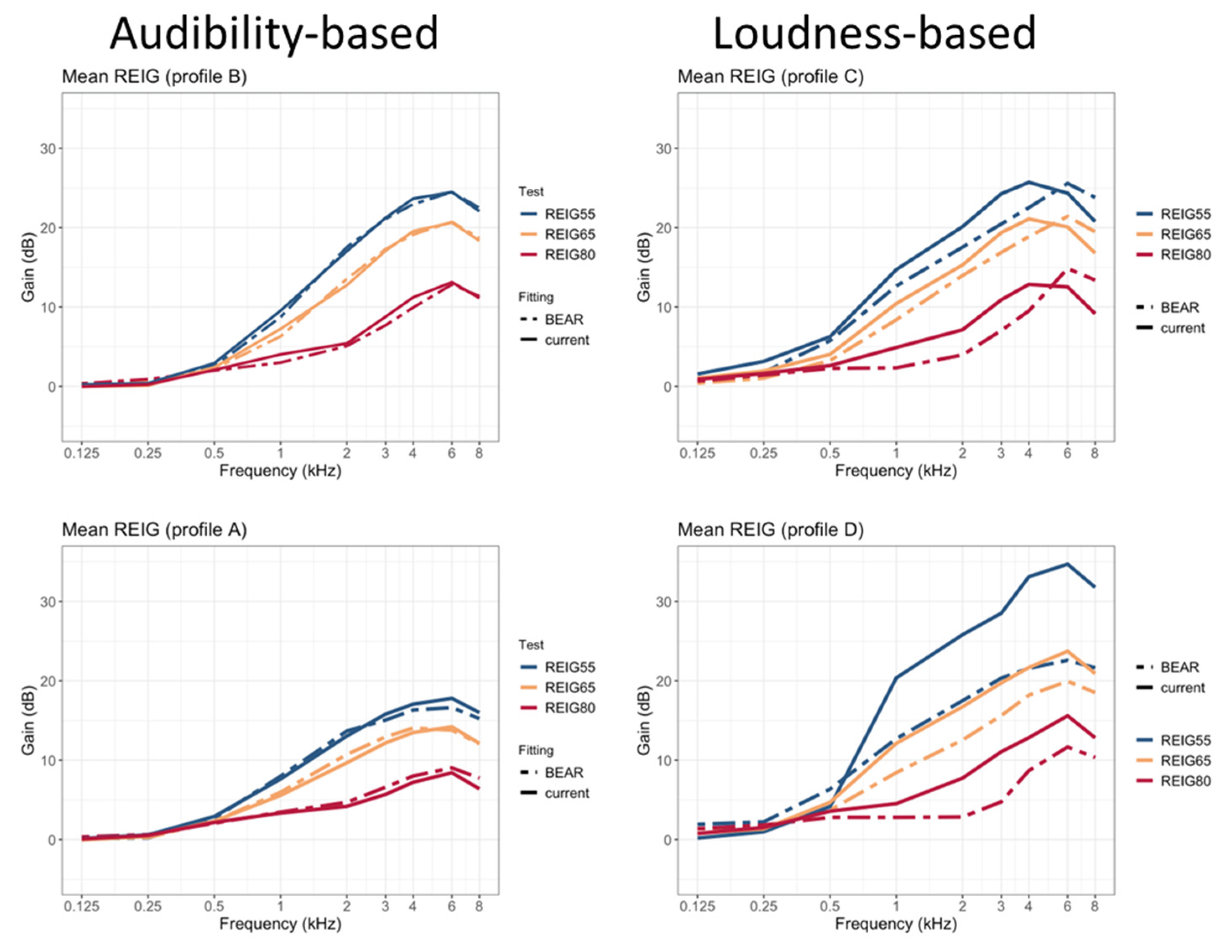
5.1. REIG Measurements
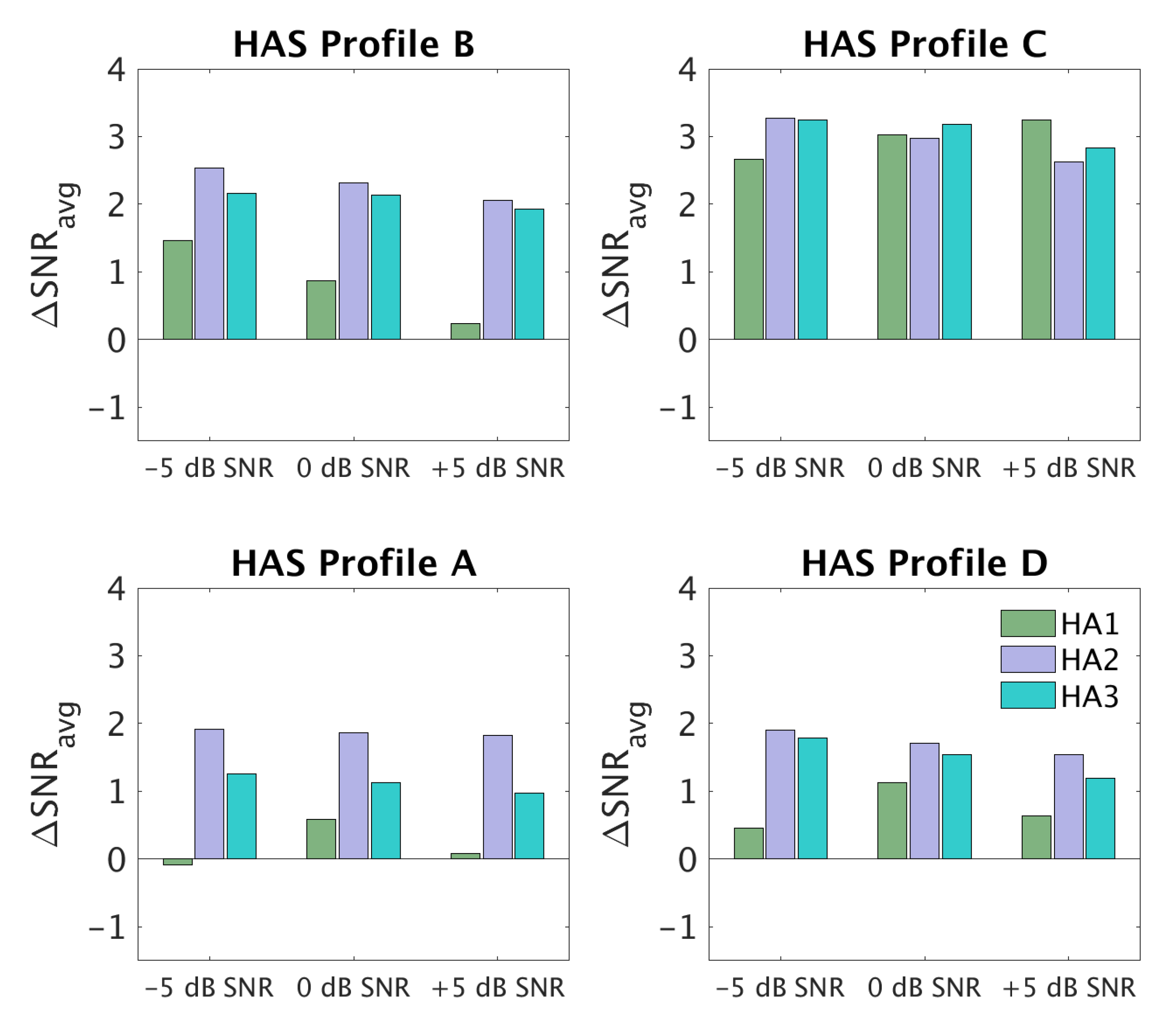
5.2. SNR Improvement Measurements
6. Discussion
6.1. Differences between HA Settings for the Four BEAR Profiles
6.2. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
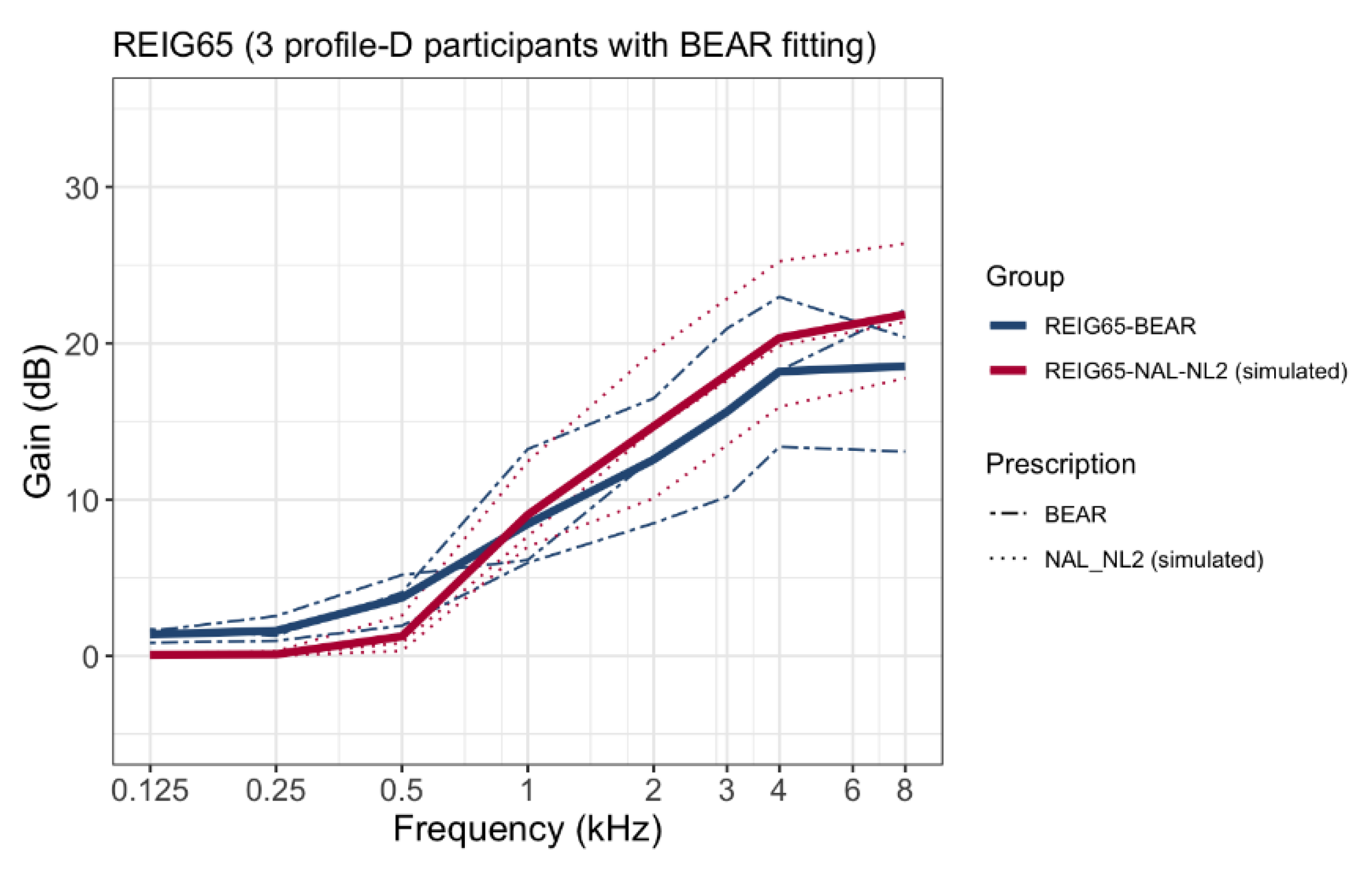
Appendix A. Comparison between BEAR and Current REIGs in Profile-D Participants

Appendix B. Hearing Devices and Advanced Features

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| A | B | C | D | |
|---|---|---|---|---|
| Oticon Opn S1 | Dir: Open Automatic Low transition NR simpler = 0 dB NR complex = −5 dB | Dir: Open Automatic Medium transition NR simpler = −3 dB NR complex = −7 dB | Dir: Open Automatic Very High transition NR simpler = −3 dB NR complex = −9 dB | Dir: Open Automatic Low transition NR simpler = 0 dB NR complex = −5 dB |
| Widex Evoke 440 | Urban program. Speech and noise mode: Noise reduction comfort | Default Urban program settings | Default Impact program settings | Urban program. Speech and noise mode: Noise reduction comfort |
| GN Linx Quattro 9 | Omni NTII: Off | Fixed Dir. NTII: Strong | Fixed Dir. NTII: Strong | Omni NTII: Off |
References
- Grant, K.W.; Walden, B.E.; Summers, V.; Leek, M.R. Introduction: Auditory models of suprathreshold distortion in persons with impaired hearing. J. Am. Acad. Audiol. 2013, 24, 254–257. [Google Scholar] [CrossRef] [PubMed]
- Humes, L.E.; Dubno, J.R. A Comparison of the Perceived Hearing Difficulties of Community and Clinical Samples of Older Adults. J. Speech Lang. Hear. Res. 2021, 64, 3653–3667. [Google Scholar] [CrossRef] [PubMed]
- Kollmeier, B.; Kiessling, J. Functionality of hearing aids: State-of-the-art and future model-based solutions. Int. J. Audiol. 2018, 57, S3–S28. [Google Scholar] [CrossRef] [PubMed]
- Vermiglio, A.J.; Soli, S.D.; Freed, D.J.; Fang, X. The Effect of Stimulus Audibility on the Relationship between Pure-Tone Average and Speech Recognition in Noise Ability. J. Am. Acad. Audiol. 2020, 31, 224–232. [Google Scholar] [CrossRef]
- Sanchez-Lopez, R.; Fereczkowski, M.; Neher, T.; Santurette, S.; Dau, T. Robust Data-Driven Auditory Profiling Towards Precision Audiology. Trends Hear. 2020, 24, 2331216520973539. [Google Scholar] [CrossRef]
- Sanchez-Lopez, R.; Nielsen, S.G.; El-Haj-Ali, M.; Bianchi, F.; Fereczkowski, M.; Canete, O.M.; Wu, M.; Neher, T.; Dau, T.; Santurette, S. Auditory Tests for Characterizing Hearing Deficits in Listeners With Various Hearing Abilities: The BEAR Test Battery. Front. Neurosci. 2021, 15, 724007. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Lopez, R.; Nielsen, S.; Cañete, O.; Fereczkowski, M.; Wu, M.; Neher, T.; Dau, T.; Santurette, S. A Clinical Test Battery for Better Hearing Rehabilitation (BEAR). Towards the Prediction of Individual AUDITORY Deficits and Hearing-Aid Benefit; Universitätsbibliothek der RWTH Aachen: Aachen, Germany, 2019. [Google Scholar] [CrossRef]
- Sanchez-Lopez, R.; Fereczkowski, M.; Santurette, S.; Dau, T.; Neher, T. Towards Auditory Profile-Based Hearing-Aid Fitting: Fitting Rationale and Pilot Evaluation. Audiol. Res. 2021, 11, 2. [Google Scholar] [CrossRef] [PubMed]
- Keidser, G.; Dillon, H.; Carter, L.; O’Brien, A. NAL-NL2 empirical adjustments. Trends Amplif. 2012, 16, 211–223. [Google Scholar] [CrossRef] [PubMed]
- Keidser, G.; Dillon, H.; Flax, M.; Ching, T.; Brewer, S. The NAL-NL2 Prescription Procedure. Audiol. Res. 2011, 1, e24. [Google Scholar] [CrossRef] [PubMed]
- Zenker, F. Real-ear measurements by probe microphone. Definition and applications. Auditio 2001, 1, 9–14. [Google Scholar] [CrossRef]
- Byrne, D.; Parkinson, A.; Newall, P. Hearing Aid Gain and Frequency Response Requirements for the Severely/Profoundly Hearing Impaired. Ear Hear. 1990, 11, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Byrne, D.; Tonisson, W. Selecting the Gain of Hearing Aids for Persons with Sensorineural Hearing Impairments. Scand. Audiol. 1976, 5, 51–59. [Google Scholar] [CrossRef]
- Klopfenstein, L.C. “OnTopReplica” v3.5.1. 2018. Available online: https://github.com/LorenzCK/OnTopReplica.git (accessed on 20 August 2022).
- Holube, I.; Fredelake, S.; Vlaming, M.; Kollmeier, B. Development and analysis of an International Speech Test Signal (ISTS). Int. J. Audiol. 2010, 49, 891–903. [Google Scholar] [CrossRef] [PubMed]
- Hagerman, B.; Olofsson, Å. A method to measure the effect of noise reduction algorithms using simultaneous speech and noise. Acta Acust. United Acust. 2004, 90, 356–361. [Google Scholar]
- Fereczkowski, M.; Neher, T. Predicting Aided Outcome With Aided Word Recognition Scores Measured With Linear Amplification at Above-conversational Levels. Ear Hear. 2022, 10–1097. [Google Scholar] [CrossRef] [PubMed]
- Oetting, D.; Bach, J.-H.; Krueger, M.; Vormann, M.; Schulte, M.; Meis, M. Subjective loudness ratings of vehicle noise with the hearing aid fitting methods NAL-NL2 and trueLOUDNESS. Proc. Int. Symp. Audit. Audiol. Res. 2019, 7, 289–296. [Google Scholar]
- Oetting, D.; Hohmann, V.; Appell, J.-E.; Kollmeier, B.; Ewert, S.D. Restoring perceived loudness for listeners with hearing loss. Ear Hear. 2018, 39, 664–678. [Google Scholar] [CrossRef] [PubMed]
- Rallapalli, V.; Anderson, M.; Kates, J.; Balmert, L.; Sirow, L.; Arehart, K.; Souza, P. Quantifying the Range of Signal Modification in Clinically Fit Hearing Aids. Ear Hear. 2020, 41, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Bell, S.L.; Creeke, S.A.; Lutman, M.E. Measuring real-ear signal-to-noise ratio: Application to directional hearing aids. Int. J. Audiol. 2010, 49, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Laugesen, S. How to compare hearing-aid processing of real speech and a speech-modified stimulus for objective validation of hearing-aid fittings? Proc. Int. Symp. Audit. Audiol. Res. 2020, 7, 317–324. [Google Scholar]





| HA Setting | Acoustic Coupling | Gain Prescription | SNR Improvement | |
|---|---|---|---|---|
| BEAR strategy | A | Standard or custom ear-tips (open fit) | Maximize speech audibility | Small |
| B | Custom ear-molds with venting | Maximize speech audibility | Large | |
| C | Custom ear-molds (closed fit *) | Loudness normalization | Large | |
| D | Custom ear-molds (closed fit *) | Loudness normalization | Small | |
| Current strategy | O | Same as for BEAR | NAL-NL2 | Manufacturer default settings |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanchez-Lopez, R.; Wu, M.; Fereczkowski, M.; Santurette, S.; Baumann, M.; Kowalewski, B.; Piechowiak, T.; Bisgaard, N.; Ravn, G.; Narayanan, S.K.; et al. Towards Auditory Profile-Based Hearing-Aid Fittings: BEAR Rationale and Clinical Implementation. Audiol. Res. 2022, 12, 564-573. https://doi.org/10.3390/audiolres12050055
Sanchez-Lopez R, Wu M, Fereczkowski M, Santurette S, Baumann M, Kowalewski B, Piechowiak T, Bisgaard N, Ravn G, Narayanan SK, et al. Towards Auditory Profile-Based Hearing-Aid Fittings: BEAR Rationale and Clinical Implementation. Audiology Research. 2022; 12(5):564-573. https://doi.org/10.3390/audiolres12050055
Chicago/Turabian StyleSanchez-Lopez, Raul, Mengfan Wu, Michal Fereczkowski, Sébastien Santurette, Monika Baumann, Borys Kowalewski, Tobias Piechowiak, Nikolai Bisgaard, Gert Ravn, Sreeram Kaithali Narayanan, and et al. 2022. "Towards Auditory Profile-Based Hearing-Aid Fittings: BEAR Rationale and Clinical Implementation" Audiology Research 12, no. 5: 564-573. https://doi.org/10.3390/audiolres12050055
APA StyleSanchez-Lopez, R., Wu, M., Fereczkowski, M., Santurette, S., Baumann, M., Kowalewski, B., Piechowiak, T., Bisgaard, N., Ravn, G., Narayanan, S. K., Dau, T., & Neher, T. (2022). Towards Auditory Profile-Based Hearing-Aid Fittings: BEAR Rationale and Clinical Implementation. Audiology Research, 12(5), 564-573. https://doi.org/10.3390/audiolres12050055