
Long-Term Surgical Results of Cortical Mastoid Bone Osteomas


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Case 1
3.2. Case 2
3.3. Case 3
4. Discussion
4.1. Presentation
4.2. Origin
4.3. Histopathological Classification
- Compact or eburneum (the most common type): this type develops from the mastoid cortex but can involve mastoid air cells, and histologically, it is composed of dense, lamellated bone tissue, with few vessels;
- Cancellous (rare): this lesion consists of fibrous cellular tissue and cancellous bone;
- Cartilaginous (uncommon): this type consists of bone and cartilage;
- Mixed (uncommon): this tumor consists of a mixture of types of bone found in compact and cancellous osteomas.
4.4. Diagnosis and Differential Diagnosis
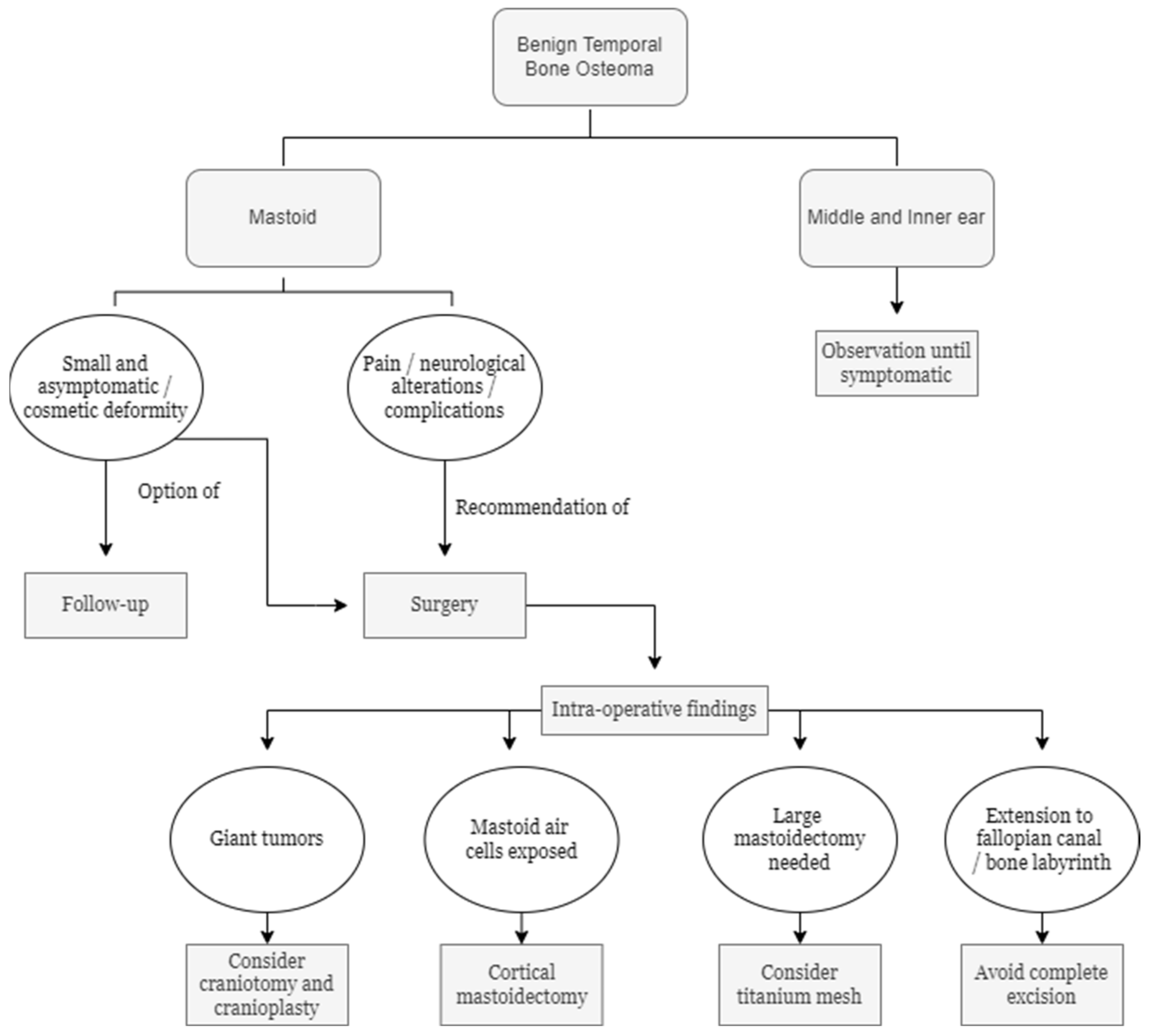
4.5. Surgical Intervention
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dhingra, R.; Davessar, J.L.; Midha, N.; Singh, H.; Monga, S. Osteoma: A Rare Case of Painless Postauricular Swelling. Indian J. Otolaryngol. Head Neck. Surg. 2019, 71 (Suppl. 2), 1238–1240. [Google Scholar] [CrossRef] [PubMed]
- Park, S.J.; Kim, Y.H. A case of giant osteoma developed from the mastoid cortical bone. Korean J. Audiol. 2012, 16, 95–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, R.K.; Goyal, A.; Kumar, A.; Kataria, G.; Kesarwani, A. Mastoid Osteoma of Temporal Bone—A Rare Case Report. J. Clin. Diagn. Res. 2017, 11, MD01–MD02. [Google Scholar] [CrossRef] [PubMed]
- Abhilasha, S.; Viswanatha, B. Osteomas of Temporal Bone: A Retrospective Study. Indian J. Otolaryngol. Head Neck Surg. 2019, 71 (Suppl. 2), 1135–1139. [Google Scholar] [CrossRef] [PubMed]
- Viswanatha, B. Extracanalicular osteoma of the temporal bone. Ear Nose Throat J. 2008, 87, 381–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marrocco, W.A. Multiple osteoma of the mastoid cavity. Arch. Otolaryngol. 1948, 47, 673–677. [Google Scholar] [CrossRef] [PubMed]
- Borissova, I.B.; Venturin, J.S.; Claro-Woodruff, W.I.; Shintaku, W.H. Mastoid osteoma: A rare incidental finding in an orthodontic patient. Imaging Sci. Dent. 2020, 50, 347–351. [Google Scholar] [CrossRef] [PubMed]
- Karataş, A.; Cebi, I.T.; Yanık, T.; Koçak, A.; Selçuk, T. Osteoma Originating from Mastoid Cortex. Turk. Arch. Otorhinolaryngol. 2017, 55, 48–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denia, A.; Perez, F.; Canalis, R.R.; Graham, M.D. Extracanalicular osteomas of the temporal bone. Arch. Otolaryngol. 1979, 105, 706–709. [Google Scholar] [CrossRef] [PubMed]
- Guarneri, G.L.; de Almeida Teixeira, B.C. Mastoid osteoma with stenosis of transverse and sigmoid sinuses as a cause of pseudotumor cerebri. Neurology 2019, 93, 37–38. [Google Scholar] [CrossRef] [Green Version]
- Pérez, A.D.D.; Romero, R.R.; Durán, E.D.; Montaño, P.R.; Bernal, R.A.; Rodríguez, C.M. El osteoma en la mastoides, ¿un hallazgo incidental? The mastoid osteoma, an incidental feature? Acta Otorrinolaringol. Esp. 2011, 62, 140–143. [Google Scholar] [CrossRef]
- Ben-Yaakov, A.; Wohlgelernter, J.; Gross, M. Osteoma of the lateral semicircular canal. Acta Otolaryngol. 2006, 126, 1005–1007. [Google Scholar] [CrossRef] [PubMed]
- Birrell, J.F. Osteoma of the mastoid. J. R. Coll. Surg. Edinb. 1978, 23, 305–309. [Google Scholar] [PubMed]
- Stuart, E.A. Osteoma of the mastoid: Report of a case with investigations of the constitutional background. Arch. Otolaryngol. 1940, 31, 838–854. [Google Scholar] [CrossRef]
- Yamasoba, T.; Harada, T.; Okuno, T.; Nomura, Y. Osteoma of the middle ear: Report of a case. Arch. Otolaryngol. Head Neck Surg. 1990, 116, 1214–1216. [Google Scholar] [CrossRef] [PubMed]
- Kandakure, V.T.; Lahane, V.J.; Mishra, S. Osteoma of Mastoid Bone; A Rare Presentation: Case Report. Indian J. Otolaryngol. Head Neck Surg. 2019, 71 (Suppl. 2), 1030–1032. [Google Scholar] [CrossRef] [PubMed]
- El Fakiri, M.; El Bakkouri, W.; Halimi, C.; Mansour, A.A.; Ayache, D. Mastoid osteoma: Report of two cases. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2011, 128, 266–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdel Tawab, H.M.; Kumar, V.R.; Tabook, S.M. Osteoma presenting as a painless solitary mastoid swelling. Case Rep. Otolaryngol. 2015, 2015, 590783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Remacha, J.; Navarro-Díaz, M.; Larrosa, F. Experience with 3-Dimensional exoscope-assisted surgery of giant mastoid process osteoma. J. Laryngol. Otol. 2022, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.H.; Wilson, D.F. Titanium mesh for functional reconstruction of the mastoid cortex after mastoidectomy. Otol. Neurotol. 2006, 27, 33–36. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Donati, G.; Redaelli de Zinis, L.O. Long-Term Surgical Results of Cortical Mastoid Bone Osteomas. Audiol. Res. 2022, 12, 290-296. https://doi.org/10.3390/audiolres12030030
Donati G, Redaelli de Zinis LO. Long-Term Surgical Results of Cortical Mastoid Bone Osteomas. Audiology Research. 2022; 12(3):290-296. https://doi.org/10.3390/audiolres12030030
Chicago/Turabian StyleDonati, Giulia, and Luca Oscar Redaelli de Zinis. 2022. "Long-Term Surgical Results of Cortical Mastoid Bone Osteomas" Audiology Research 12, no. 3: 290-296. https://doi.org/10.3390/audiolres12030030
APA StyleDonati, G., & Redaelli de Zinis, L. O. (2022). Long-Term Surgical Results of Cortical Mastoid Bone Osteomas. Audiology Research, 12(3), 290-296. https://doi.org/10.3390/audiolres12030030