
Cochlear Implant in Patients with Intralabyrinthine Schwannoma without Tumor Removal



Abstract
:1. Introduction
2. Materials and Methods
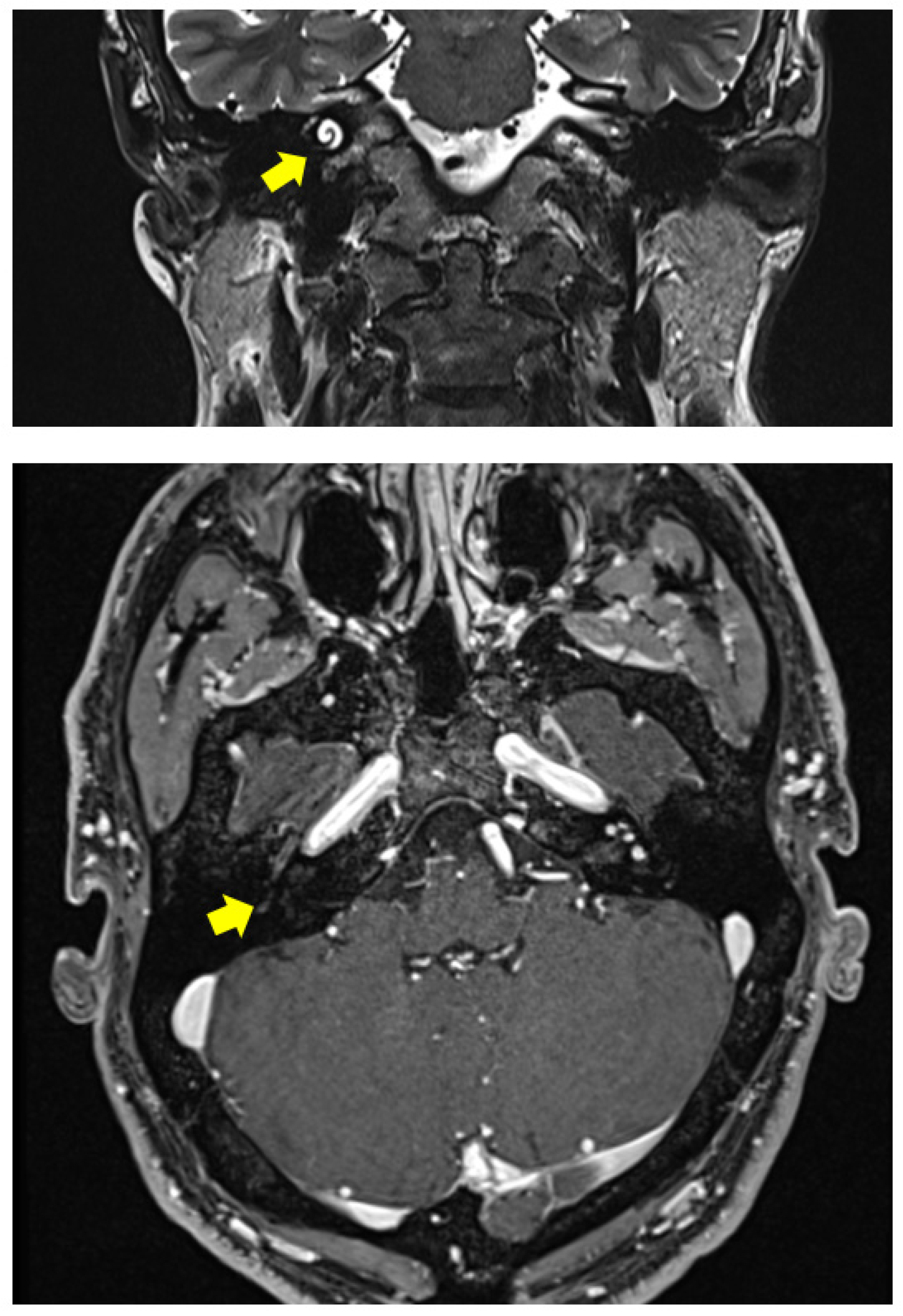
2.1. Clinical Case 1
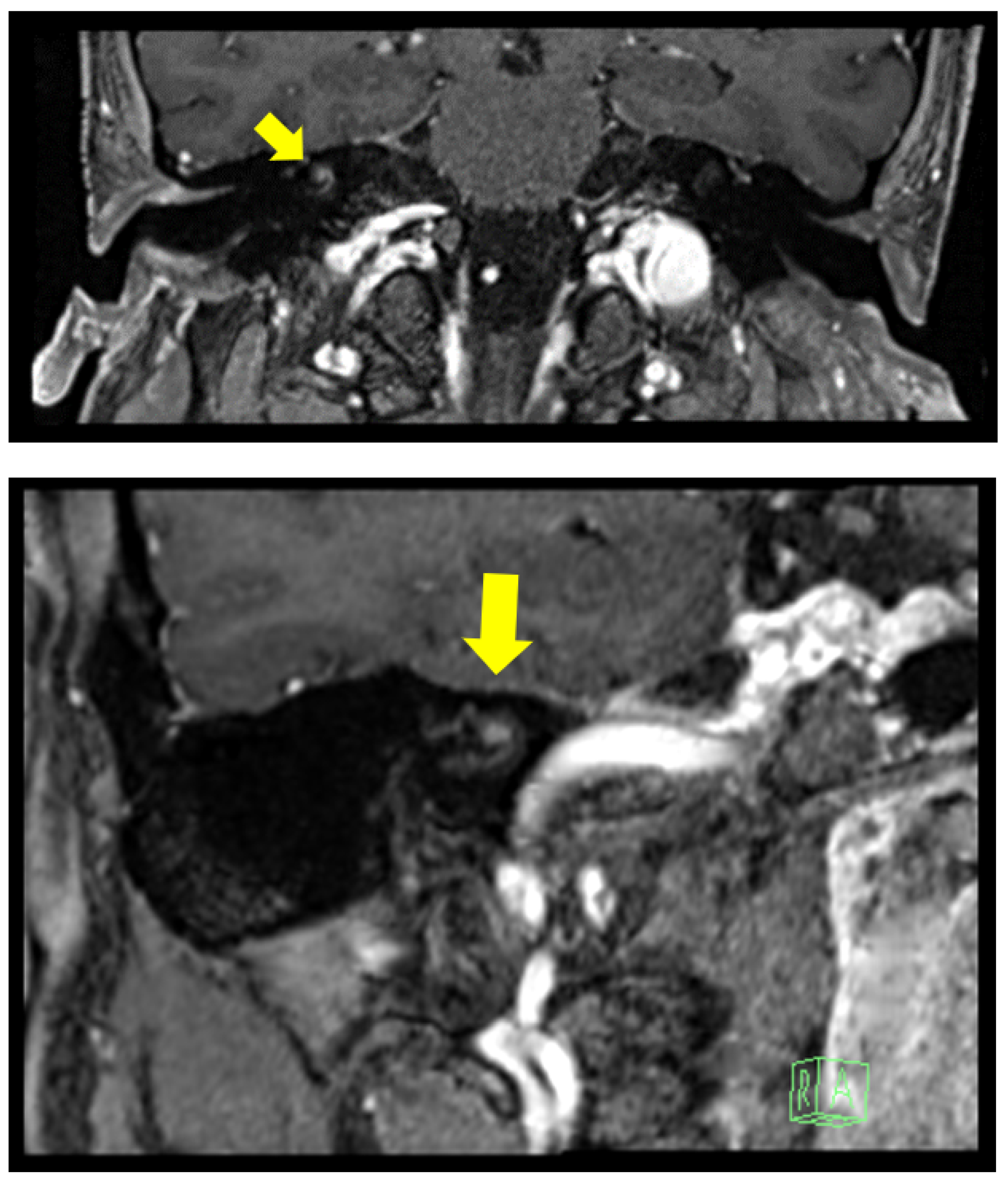
2.2. Clinical Case 2
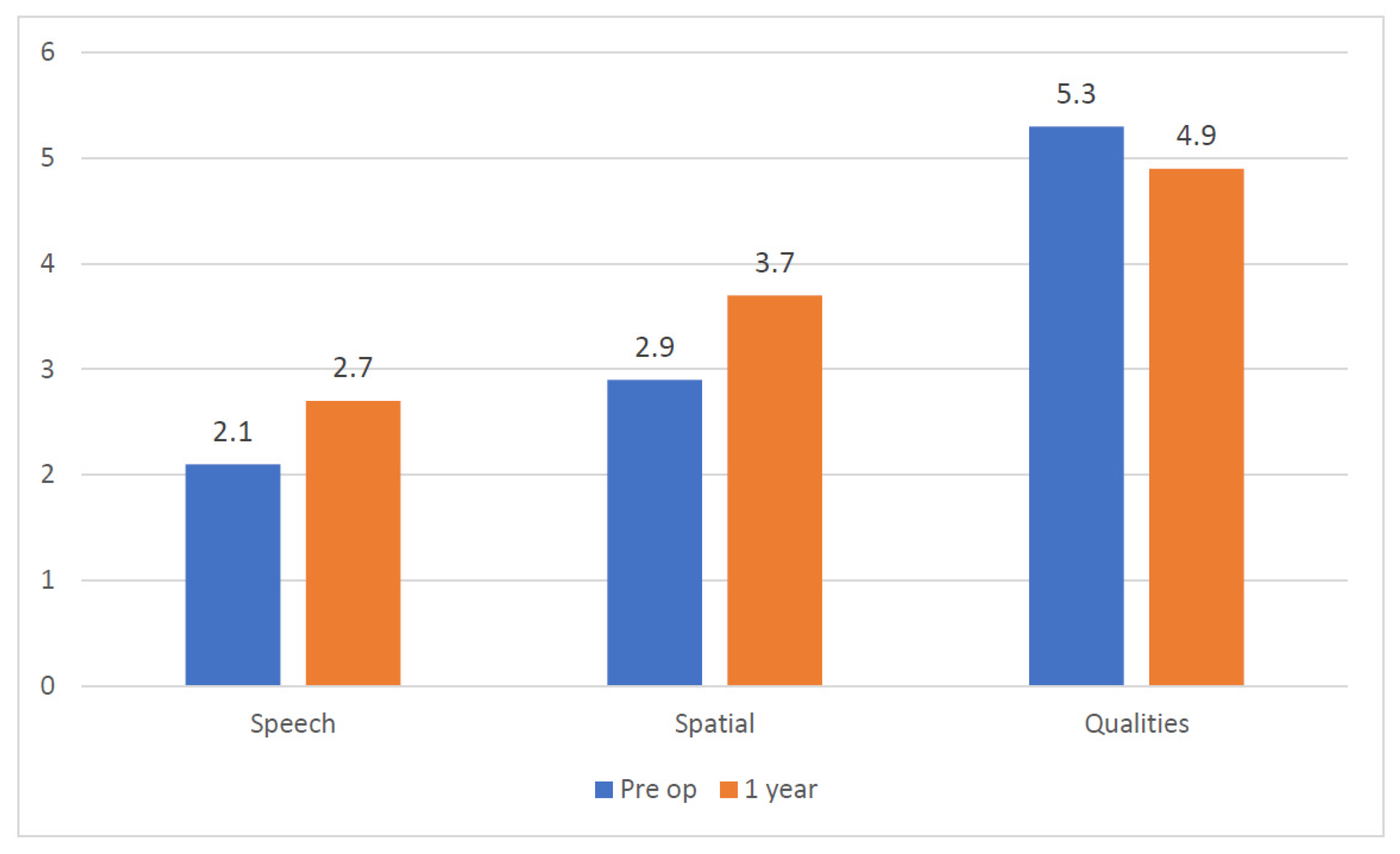
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kennedy, R.J.; Shelton, C.; Salzman, K.L.; Davidson, H.C.; Harnsberger, H.R. Intralabyrinthine schwannomas: Diagnosis, management, and a new classification system. Otol. Neurotol. 2004, 25, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Nager, F.R. Zur Anatomie der endemische Taubstummheit (mit einem Neurofibrom der Schneckenspindel). Z. Ohrenheilk. 1917, 75, 349–364. [Google Scholar]
- Karlan, M.S.; Basek, M.; Potter, G.B. Intracochlear neurilemmoma. Arch. Otolaryngol. 1972, 96, 573–575. [Google Scholar] [CrossRef] [PubMed]
- Grayeli, A.B.; Fond, C.; Kalamarides, M.; Bouccara, D.; Cazals-Hatem, D.; Cyna-Gorse, F.; Sterkers, O. Diagnosis and management of intracochlear schwannomas. Otol. Neurotol. 2007, 28, 951–957. [Google Scholar] [CrossRef] [PubMed]
- Carlson, M.L.; Neff, B.A.; Sladen, D.P.; Link, M.J.; Driscoll, C.L. Cochlear Implantation in Patients with Intracochlear and Intralabyrinthine Schwannomas. Otol Neurotol. 2016, 37, 647–653. [Google Scholar] [CrossRef] [PubMed]
- Newman, C.W.; Jacobson, G.P.; Spitzer, J.B. Development of the Tinnitus Handicap Inventory. Arch. Otolaryngol.–Head Neck Surg. 1996, 122, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Cutugno, F.; Prosser, S.; Turrini, M. Audiometria Vocale—Vol. I; GN Resound: Montegrotto Terme, Italy, 2000. [Google Scholar]
- Jacobson, G.P.; Newman, C.W. The development of the Dizziness Handicap Inventory. Arch. Otolaryngol.–Head Neck Surg. 1990, 116, 424–427. [Google Scholar] [CrossRef] [PubMed]
- Tieleman, A.; Casselman, J.W.; Somers, T.; Delanote, J.; Kuhweide, R.; Ghekiere, J.; De Foer, B.; Offeciers, E.F. Imaging of intralabyrinthine schwannomas: A retrospective study of 52 cases with emphasis on lesion growth. Am. J. Neuroradiol. 2008, 29, 898–905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donnelly, M.J.; Daly, C.A.; Briggs, R.J. MR imaging features of an intracochlear acoustic schwannoma. J. Laryngol. Otol. 1994, 108, 1111–1114. [Google Scholar] [CrossRef] [PubMed]
- Elias, T.G.A.; Perez Neto, A.; Zica, A.T.S.; Antunes, M.L.; Penido, N.O. Different clinical presentation of intralabyrinthine schwannomas—A systematic review. Braz. J. Otorhinolaryngol. 2019, 85, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Reda, J.D.; West, N.; Cayé-Thomasen, P. Intracochlear Vestibular Schwannoma Presenting with Mixed Hearing Loss. J. Int. Adv. Otol. 2021, 17, 265–268. [Google Scholar] [CrossRef] [PubMed]
- Hegarty, J.L.; Patel, S.; Fischbein, N.; Jackler, R.K.; Lalwani, A.K. The value of enhanced magnetic resonance imaging in the evaluation of endocochlear disease. Laryngoscope 2002, 112, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Van Abel, K.M.; Carlson, M.L.; Link, M.J.; Neff, B.A.; Beatty, C.W.; Lohse, C.M.; Eckel, L.J.; Lane, J.I.; Driscoll, C.L. Primary inner ear schwannomas: A case series and systematic review of the literature. Laryngoscope 2013, 123, 1957–1966. [Google Scholar] [CrossRef] [PubMed]
- Salzman, K.L.; Childs, A.M.; Davidson, H.C.; Kennedy, R.J.; Shelton, C.; Harnsberger, H.R. Intralabyrinthine schwannomas: Imaging diagnosis and classification. Am. J. Neuroradiol. 2012, 33, 104–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mafee, M.F.; Lachenauer, C.S.; Kumar, A.; Arnold, P.M.; Buckingham, R.A.; Valvassori, G.E. CT and MR imaging of intralabyrinthine schwannoma: Report of two cases and review of the literature. Radiology 1990, 174, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Kronenberg, J.; Horowitz, Z.; Hlldesheimer, M. Intracochlear Schwannoma and Cochlear Implantation. Ann. Otol. Rhinol. Laryngol. 1999, 108, 659–660. [Google Scholar] [CrossRef] [PubMed]
- Plontke, S.K.; Rahne, T.; Pfister, M.; Götze, G.; Heider, C.; Pazaitis, N.; Strauss, C.; Caye-Thomasen, P.; Kösling, S. Intralabyrinthine schwannomas: Surgical management and hearing rehabilitation with cochlear implants. HNO 2017, 65 (Suppl. 2), 136–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aschendorff, A.; Arndt, S.; Laszig, R.; Wesarg, T.; Hassepaß, F.; Beck, R. Treatment and auditory rehabilitation of intralabyrinthine schwannoma by means of cochlear implants. HNO 2017, 65 (Suppl. 1), 46–51. [Google Scholar] [CrossRef] [PubMed]
- Eitutis, S.T.; Jansen, T.; Borsetto, D.; Scoffings, D.J.; Tam, Y.C.; Panova, T.; Tysome, J.R.; Donnelly, N.P.; Axon, P.R.; Bance, M.L. Cochlear Implantation in NF2 Patients Without Intracochlear Schwannoma Removal. Otol. Neurotol. 2021, 42, 1014–1021. [Google Scholar] [CrossRef] [PubMed]
- Todt, I.; Rademacher, G.; Mittmann, P.; Mutze, S.; Ernst, A. Postoperative imaging of the internal auditory canal: Visualization of active auditory implants. HNO 2017, 65 (Suppl. 2), 81–86. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Pre-Op Evaluation | 1 Year | |
|---|---|---|
| S0 N0 | −3.6 | −4.8 |
| S0 Nic | −9 | −8.5 |
| S0 Nnh | −0.1 | −1.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laborai, A.; Ghiselli, S.; Cuda, D. Cochlear Implant in Patients with Intralabyrinthine Schwannoma without Tumor Removal. Audiol. Res. 2022, 12, 33-41. https://doi.org/10.3390/audiolres12010004
Laborai A, Ghiselli S, Cuda D. Cochlear Implant in Patients with Intralabyrinthine Schwannoma without Tumor Removal. Audiology Research. 2022; 12(1):33-41. https://doi.org/10.3390/audiolres12010004
Chicago/Turabian StyleLaborai, Andrea, Sara Ghiselli, and Domenico Cuda. 2022. "Cochlear Implant in Patients with Intralabyrinthine Schwannoma without Tumor Removal" Audiology Research 12, no. 1: 33-41. https://doi.org/10.3390/audiolres12010004
APA StyleLaborai, A., Ghiselli, S., & Cuda, D. (2022). Cochlear Implant in Patients with Intralabyrinthine Schwannoma without Tumor Removal. Audiology Research, 12(1), 33-41. https://doi.org/10.3390/audiolres12010004