
Characterization of Balance Problems and Rehabilitation Needs of Patients with Ménière’s Disease



Abstract
:1. Introduction
2. Method
2.1. Study Design and Participants
2.2. Data Collection
2.3. Data Analysis
3. Results
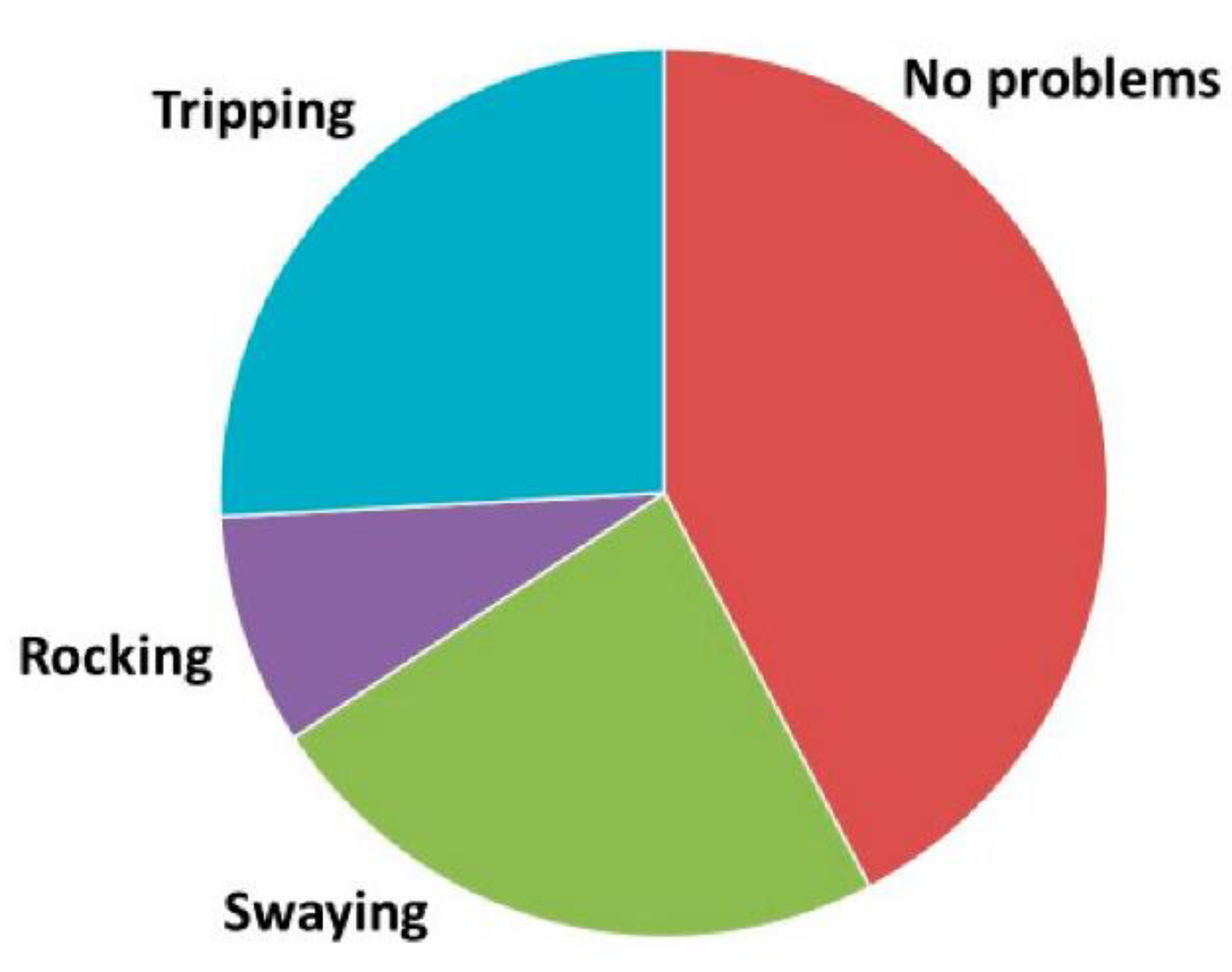
3.1. Prevalence of Postural and Gait Problems in MD
3.2. Characteristics of Body Sway and Balance Problems
3.3. Visual Complaints and Postural Problems
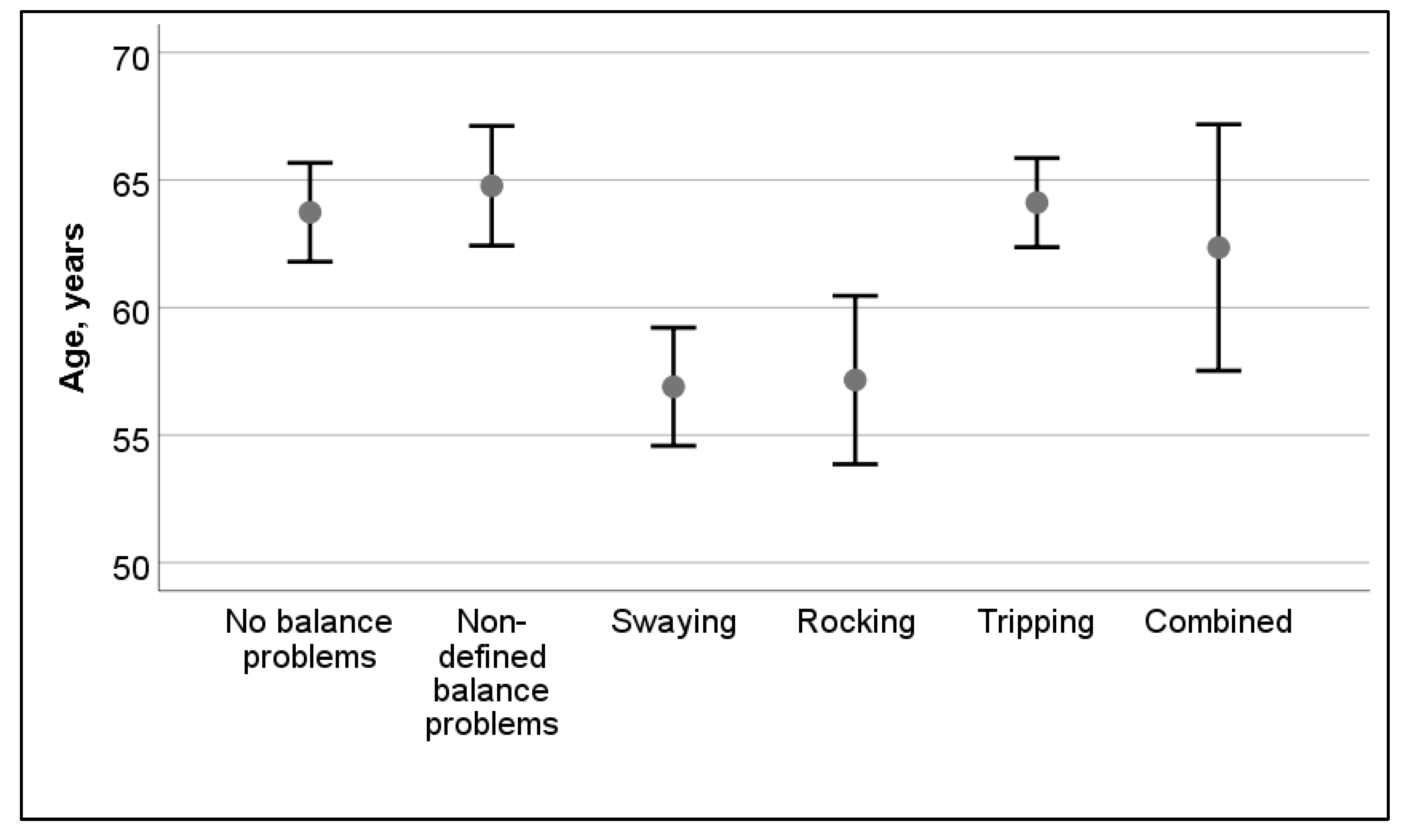
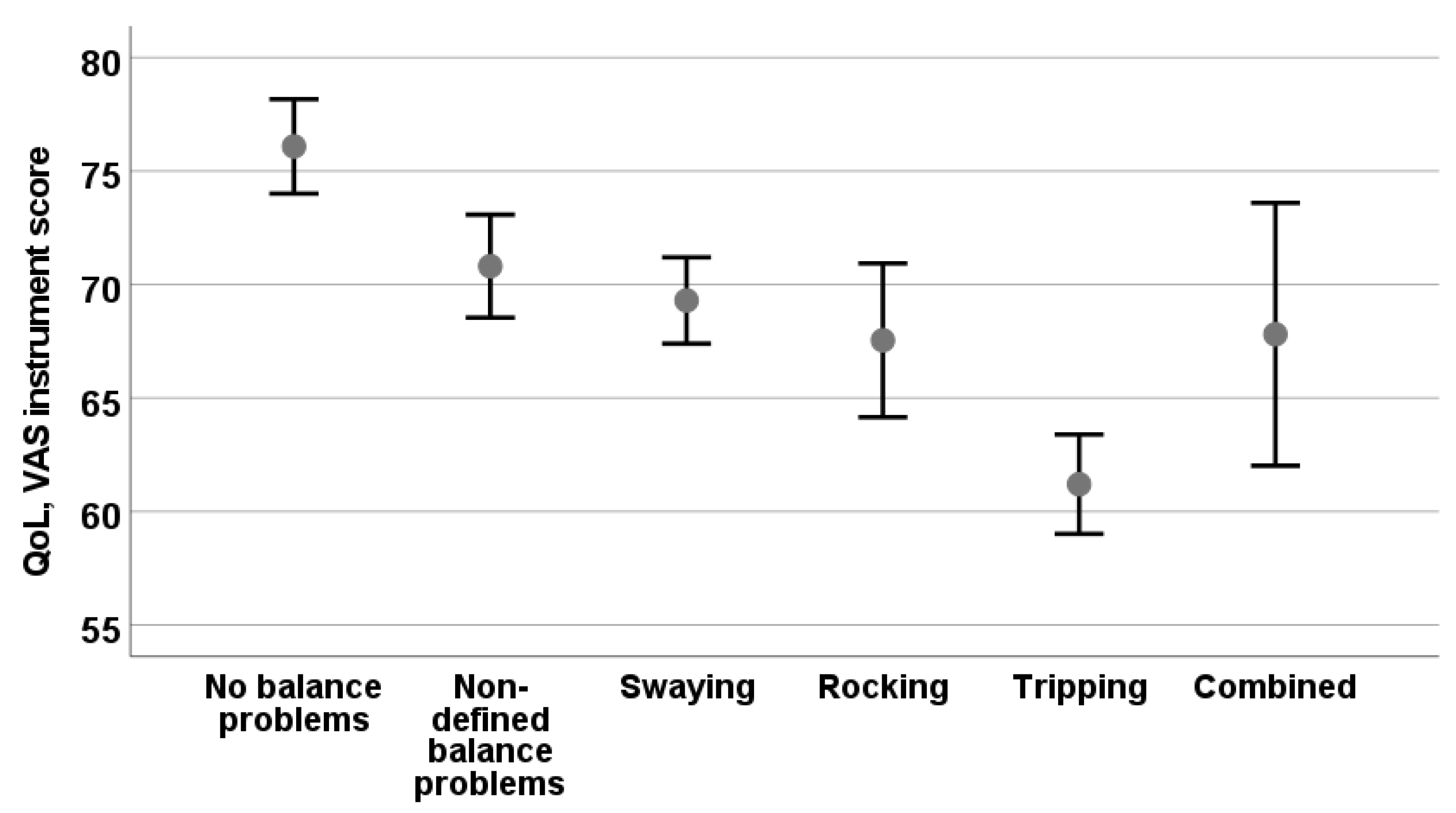
3.4. Association of Balance Problems in Patients with MD
4. Discussion
4.1. Tripping
4.2. Swaying
4.3. Rocking
4.4. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Levo, H.; Stephens, D.; Poe, D.; Kentala, E.; Pyykkö, I. Use of ICF in assessing the effects of Meniere’s disorder on life. Ann. Otol. Rhinol. Laryngol. 2010, 119, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Tyrrell, J.S.; Whinney, D.J.; Ukoumunne, O.C.; Fleming, L.E.; Osborne, N.J. Prevalence, associated factors, and comorbid conditions for Meniere’s disease. Ear Hear. 2014, 35, e162–e169. [Google Scholar] [CrossRef]
- Havia, M.; Kentala, E.; Pyykkö, I. Prevalence of Menière’s Disease in General Population of Southern Finland. Otolaryngol. Head Neck Surg. 2005, 133, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Tyrrell, J.; Whinney, D.J.; Taylor, T. The Cost of Ménière’s Disease: A Novel Multisource Approach. Ear Hear. 2016, 37, e202–e209. [Google Scholar] [CrossRef]
- Pyykkö, I.; Manchaiah, V.; Zou, J.; Levo, H.; Kentala, E. Impact of Tumarkin attacks on complaints and work ability in Ménière’s disease. J. Vestib. Res. 2017, 28, 319–330. [Google Scholar] [CrossRef] [PubMed]
- AAO-HNS. Committee on Hearing and Equilibrium guidelines for the diagnosis and evaluation of therapy in Meniere’s disease. Otolaryngol. Head Neck Surg. 1995, 113, 181–185. [Google Scholar] [CrossRef]
- Lopez-Escamez, J.A.; Carey, J.; Chung, W.H.; Goebel, J.A.; Magnusson, M.; Mandala, M.; Newman-Toker, D.E.; Strupp, M.; Suzuki, M.; Trabalzini, F.; et al. Classification Committee of the Barany, R. Japan Society for Equilibrium, O. European Academy of, Neurotology, O.-H. Equilibrium Committee of the American Academy of, S. Neck and S. Korean Balance, Diagnostic criteria for Meniere’s disease. J. Vestib. Res. 2015, 25, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saha, D.J.; Morasso, P. Stabilization Strategies for Unstable Dynamics. PLoS ONE 2012, 7, e30301. [Google Scholar] [CrossRef] [Green Version]
- Allum, J.H.J.; Keshner, E.A. Vestibular and proprioceptive control of sway stabilization. In Disorders of Posture and Gait; Bless, W., Brandt, T., Eds.; Elsevier: Amsterdam, The Netherlands, 1986; pp. 19–40. [Google Scholar]
- Peterka, R.J. Sensorimotor Integration in Human Postural Control. J. Neurophysiol. 2002, 88, 1097–1118. [Google Scholar] [CrossRef] [Green Version]
- Toppila, E.; Pyykkö, I. Chaotic model of postural stability-a position and velocity dependent system. Automedica 2000, 19, 115–134. [Google Scholar]
- Suzuki, Y.; Morimoto, H.; Kiyono, K.; Morasso, P.G.; Nomura, T. Dynamic Determinants of the Uncontrolled Manifold during Human Quiet Stance. Front. Hum. Neurosci. 2016, 10, 618. [Google Scholar] [CrossRef] [Green Version]
- Aramaki, Y.; Nozaki, D.; Masani, K.; Sato, T.; Nakazawa, K.; Yano, H. Reciprocal angular acceleration of the ankle and hip joints during quiet standing in humans. Exp. Brain Res. 2001, 136, 463–473. [Google Scholar] [CrossRef] [PubMed]
- Speers, R.A.; Paloski, W.H.; Kuo, A.D. Multivariate changes in coordination of postural control following spaceflight. J. Biomech. 1998, 31, 883–889. [Google Scholar] [CrossRef]
- Cha, Y.-H.; Baloh, R.W.; Cho, C.; Magnusson, M.; Song, J.-J.; Strupp, M.; Wuyts, F.; Staab, J.P. Mal de Débarquement Syndrome: Diagnostic Criteria. Consensus document of the Classification Committee of the Bárány Society Barany Society. J. Vestib. Res. 2020, 30, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Dai, M.; Cohen, B.; Smouha, E.; Cho, C. Readaptation of the Vestibulo-Ocular Reflex Relieves the Mal De Debarquement Syndrome. Front. Neurol. 2014, 5, 124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pyykkö, I.; Aalto, H.; Starck, J.; Ishizaki, H. Postural Control in Meniere’s Disease and Acoustic Neurinoma when Studied on a Linearly Oscillating Platform. Acta Otolaryngol. Suppl. 1995, 520 Pt 1, 19–21. [Google Scholar] [CrossRef] [PubMed]
- Pyykkö, N.; Pyykkö, I.; Zou, J.; Manchaiah, V. Does the self-training in Ménière’s disease fit the disease characteristics and help alleviate the balance problems? Int. J. Adv. Otol. 2021, in press. [Google Scholar]
- Dietz, A. Afferent and efferent control of gait. In Disorders of Posture and Gait; Bless, W., Brandt, T., Eds.; Elsevier: Amsterdam, The Netherlands, 1986; pp. 69–81. [Google Scholar]
- Pyykkö, I.; Magnusson, M. Neural Activity, Alertness and Visual Orientation in Intact and Unilaterally Labyrinthectomized Rabbits. J. Otorhinolaryngol. Relat. Spec. 1987, 49, 26–34. [Google Scholar] [CrossRef]
- Bigelow, R.T.; Agrawal, Y. Vestibular involvement in cognition: Visuospatial ability, attention, executive function, and memory. J. Vestib. Res. 2015, 25, 73–89. [Google Scholar] [CrossRef]
- Aitken, P.; Zheng, Y.; Smith, P.F. The modulation of hippocampal theta rhythm by the vestibular system. J. Neurophysiol. 2018, 119, 548–562. [Google Scholar] [CrossRef] [Green Version]
- Gottshall, K.R.; Hoffer, M.E.; Moore, R.J.; Balough, B.J. The Role of Vestibular Rehabilitation in the Treatment of Meniere’s Disease. Otolaryngol. Head Neck Surg. 2005, 133, 326–328. [Google Scholar] [CrossRef] [PubMed]
- Cha, Y.-H.; Brodsky, J.; Ishiyama, G.; Sabatti, C.; Baloh, R.W. Clinical features and associated syndromes of mal de debarquement. J. Neurol. 2008, 255, 1038–1044. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Character of Visual Problem | No Balance Problems (n = 126) | Non-Defined Balance Problems (n = 95) | Swaying (n = 122) | Rocking (n = 44) | Tripping (n = 135) | Combined Balance Problems (n = 17) | All (n = 522) | Chi-Square Test, p-Value |
|---|---|---|---|---|---|---|---|---|
| During head turn items jump/move in visual field | 3 (2%) | 12 (14%) | 49 (40%) *,† | 12 (27%) | 30 (22%) * | 4 (23%) | 110 (21%) | Χ2 = 59.7, p < 0.001 |
| Objects seem to float or move | 0 (0%) | 6 (6%) | 14 (11%) * | 11 (25%) *,† | 7 (5%) | 6 (35%) | 44 (8%) | Χ2 = 48.3, p = 0.002 |
| Problems in focusing the eyes | 7 (6%) | 19 (20%) | 35 (29%) *,† | 22 (50%) * | 56 (41%) * | 12 (70%) | 151 (29%) | Χ2 = 72.5, p < 0.001 |
| Problems in visualizing the horizon | 0 (0%) | 7 (7%) | 29 (24%) * | 9 (20%) | 34 (25%) * | 5 (29%) | 84 (16%) | Χ2 = 47.1, p < 0.001 |
| Item | Unstandardized Beta (B) | Standard Error (S.E.) | Wald | Significance | Exponentiation of the B Coefficient | 95% C.I. for Exp(B) Lower | 95% C.I. for Exp(B) Upper |
|---|---|---|---|---|---|---|---|
| Age | 0.04 | 0.009 | 18.31 | 0.0001 | 1.04 | 1.02 | 1.06 |
| VDA | 1.19 | 0.42 | 7.985 | 0.005 | 3.29 | 1.44 | 7.50 |
| Fatigue | 0.83 | 0.21 | 15.03 | 0.0001 | 2.29 | 1.51 | 3.48 |
| Tinnitus | 0.53 | 0.19 | 7.25 | 0.007 | 1.69 | 1.15 | 2.48 |
| Black spots | 0.42 | 0.21 | 4.15 | 0.042 | 1.52 | 1.02 | 2.28 |
| Constant vertigo | 1.28 | 0.41 | 9.79 | 0.002 | 3.59 | 1.61 | 8.02 |
| Vertigo in attacks with constant vertigo | 0.82 | 0.29 | 8.29 | 0.004 | 2.27 | 1.30 | 3.98 |
| Head movement-provoked vertigo | 0.73 | 0.32 | 5.20 | 0.023 | 2.07 | 1.11 | 3.86 |
| Syncope | 1.10 | 0.46 | 5.81 | 0.016 | 3.00 | 1.23 | 7.33 |
| Constant | −3.70 | 0.62 | 35.28 | 0.0001 | 0.025 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pyykkö, I.; Pyykkö, N.; Zou, J.; Manchaiah, V. Characterization of Balance Problems and Rehabilitation Needs of Patients with Ménière’s Disease. Audiol. Res. 2022, 12, 22-32. https://doi.org/10.3390/audiolres12010003
Pyykkö I, Pyykkö N, Zou J, Manchaiah V. Characterization of Balance Problems and Rehabilitation Needs of Patients with Ménière’s Disease. Audiology Research. 2022; 12(1):22-32. https://doi.org/10.3390/audiolres12010003
Chicago/Turabian StylePyykkö, Ilmari, Nora Pyykkö, Jing Zou, and Vinaya Manchaiah. 2022. "Characterization of Balance Problems and Rehabilitation Needs of Patients with Ménière’s Disease" Audiology Research 12, no. 1: 22-32. https://doi.org/10.3390/audiolres12010003
APA StylePyykkö, I., Pyykkö, N., Zou, J., & Manchaiah, V. (2022). Characterization of Balance Problems and Rehabilitation Needs of Patients with Ménière’s Disease. Audiology Research, 12(1), 22-32. https://doi.org/10.3390/audiolres12010003