1. Introduction
Vestibular neuritis (VN) is a clinical entity that refers to an otoneurological disorder characterized by acute, prolonged vertigo of peripheral origin, one of the most common causes of acute vestibular syndrome (AVS) and affects predominantly Vestibulo Ocular Reflex (VOR) [
1].
The acute phase, which usually coincides with the first seventy-two hours following the onset of symptoms [
2], is defined by severe rotatory vertigo with nausea and vomiting where only vestibular function and not hearing is affected [
1]. These patients fall into three main groups, suggesting that neuritis may affect the entire vestibular nerve or just one of the branches of it 3–6, and certainly the most frequent clinical entity is that which afflicts the upper compartment of the eighth pair of cranial nerves, called Superior Vestibular Neuritis (SVN) [
3].
VN diagnosis, especially in AVS, is a great challenge for the clinician. Nystagmus characteristics, other oculomotor findings, and the head impulse test are commonly used in combination often complemented with imaging. Clinicians can identify the classical signs and symptoms (vertigo is the main one) which are dependent on the absent function of the affected vestibular labyrinth differentiating strokes from peripheral vestibular disorders [
2].
After its clinical validation vs dual magnetic scleral search coil [
4] video Head Impulse Test (vHIT) constitutes the diagnostic clinical gold standard of the horizontal and vertical VOR. Thus, during a brief, passive, unpredictable, horizontal head turns towards the healthy ear, the subject maintains fixation on an earth-fixed target while the patient with reduced unilateral horizontal or vertical canal function fails to maintain fixation on an earth-fixed target and so makes corrective (overt or covert) saccades during or at the end of the head rotation in order to regain fixation [
5]. The saccades that occur during head movement are known as covert and those that occur following after the end of the head movement, as overt saccades [
6].These saccades are a substitution sign of the reduced VOR dynamic function. This paradigm is also called Head Impulse Paradigm (HIMP). A new complementary test paradigm was recently proposed to be an indicator of vestibular function [
7]. This paradigm has been named suppression head impulse test (SHIMP), where the subject is asked to look at a head-fixed target rather than at the earth-fixed target used in HIMP during the passive head turn. Healthy subjects make a corrective saccade (a “SHIMPs” saccade), whereas patients at the time of acute peripheral vestibular loss do not [
6]. SHIMPs paradigm gives more precise information on the VOR gain compared to HIMPs because the evaluation of the gain is not affected by covert saccades [
7].
Despite the evidence in diagnosing vestibular neuritis [
8,
9] through the vHIT, some relevant clinical aspects are poorly understood. Instead, it is still unclear which stage of the disease the VOR gain values correspond to, and above all, it is not clear if the VOR gain values are related to disability complained by patients. Our hypothesis is that the VOR gain values might be dissimilar according to the damage of the VIII pair of cranial nerves in the real acute stage (within seventy-two hours) or the subacute stage (seventy-two hours six weeks) and on patients’ perception of handicap due to the dizziness.
This study aims to retrospectively evaluate the VOR gain values during the acute and subacute stages of the VN and to correlate these values with the patients’ perception of handicap due to the dizziness.
4. Results
Twenty-eight patients with a diagnosis of unilateral superior VN (SVN) met the inclusion criteria and were enrolled in the study. Altered asymmetry ratio values compatible with the diagnosis of VN of ocular Air Conducted Sound and Bone Conducted Vibration VEMPs were found in all participants, whereas the asymmetry ratio values of cervical VEMPS were in the normal ranges.
VOR gain in the AVSg was 0.39 ± 0.17 and 0.54 ± 0.09 in the PAVSg, the DHI score was 78.80 ± 7.28 in the AVSg and 40 ± 16.08 in the PAVSg. Significant differences were found in the between-subjects analysis in DHI scores (p = 0.000) and in the ipsilesional hVOR gain values (p = 0.001), no differences were found in the contralesional VOR gain values (p = 0.601). Nine out of fifteen patients of AVSg evaluated in the post-acute phase showed a statistical significant difference from the baseline (p < 0.05) in the hVOR values (0.57 ± 0.25).
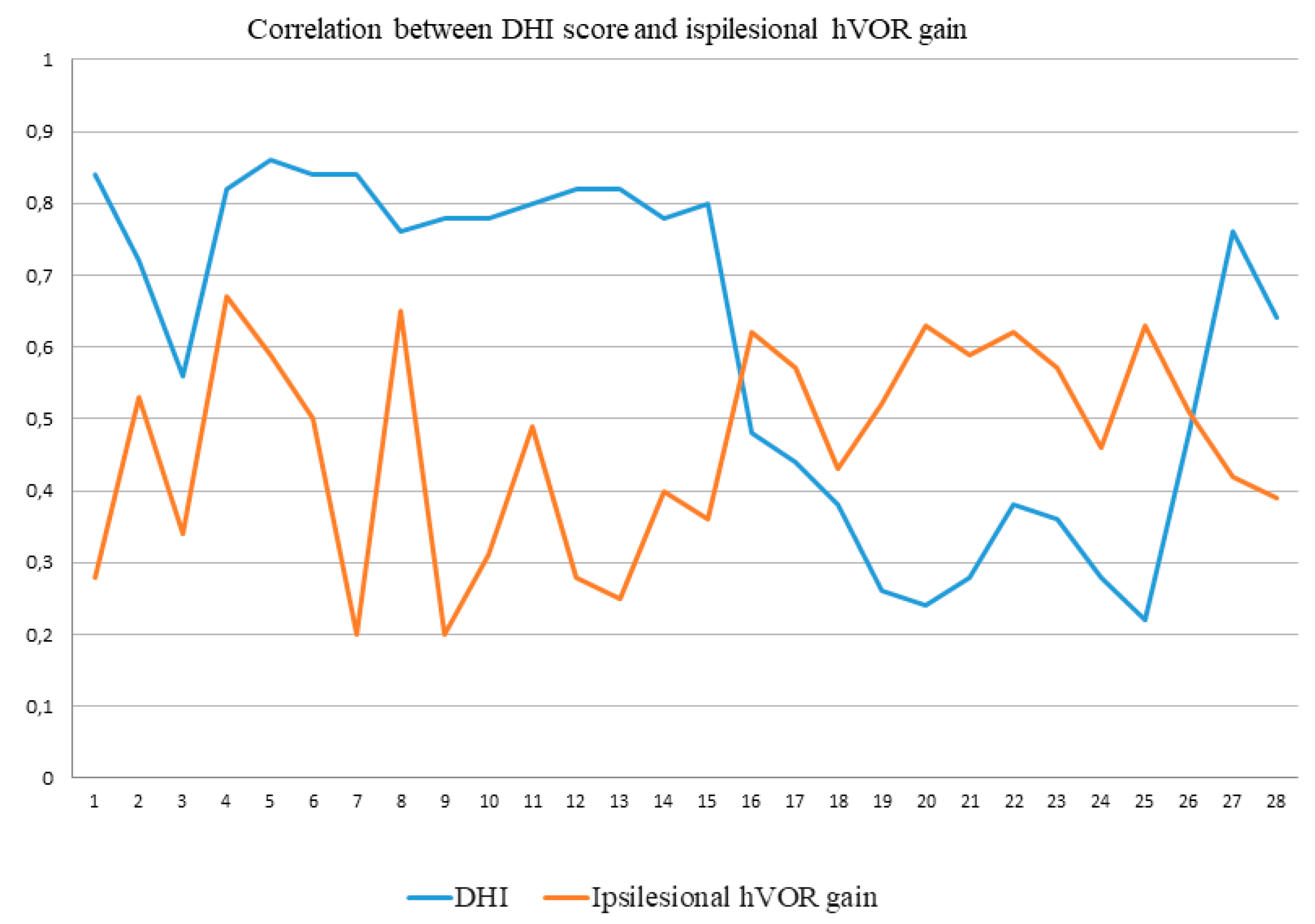
The correlation analysis showed significant results (
p = 0.03) between DHI score (40 ± 16.08) and ipsilesional VOR gain (0.54 ± 0.09) in the subacute PAVSg as reported in
Figure 1.
All AVSg patients and three of the PAVSg presented AcS on the contralesional side. All patients of the AVSg evaluated in the post-acute phase did not show more AcS.
5. Discussion
This retrospective study aimed to evaluate the VOR gain values during the acute and subacute stages of the VN. Great emphasis in the last few years was given about the changes in the timing and pattern of corrective saccades during the different stages of VN [
6,
7,
8,
13].
On the contrary, we focused our attention on other aspects of the clinical course observation timing as well as on the valid indicator of semicircular canal function (eye movements) in response to small, brief, fast, unpredictable horizontal head turns (head impulses) angular acceleration up to 4000°/s2.
Firstly our findings show a significant difference of hVOR gain values in the two groups (
Table 1), suggesting that the hVOR gain values can change, just like saccades pattern, during the different stages of VN. These clinical data are important because it represents an important indicator of lesion evolution in the SCC dynamic function, especially at the time of the attack. Our findings can provide useful clues about the clinical timing and progress of recovery from the lesion through the value of the hVOR gain which can, therefore, accompany changes and now known evolution of the saccades pattern that allows the patient to stabilize vision on the retina.
Testing patients within seventy-two hours and after this period allows highlighting an increase in the hVOR gain as previously described but in a longer observation period [
8,
9,
14]. Furthermore, correlating the hVOR gain with the DHI score in the different phases emerged that the subjective symptoms are significantly lower in the PAVSg as reported in
Figure 1. The data could therefore also correlate with the modifications in VOR gain values (increase) which in the early stages is strongly and suddenly compromised if compared with the contralesional side. Of course an increase of VOR gain can predict an improvement of the clinical condition, but possibly other factors may play a role, as the evolution of the saccades pattern, i.e., from overt to covert saccades and as recently published [
13], the reappearance of SHIMPs saccades.
The finding of an increase in the VOR gain could be the prelude to a restitutio ad integrum [
9].
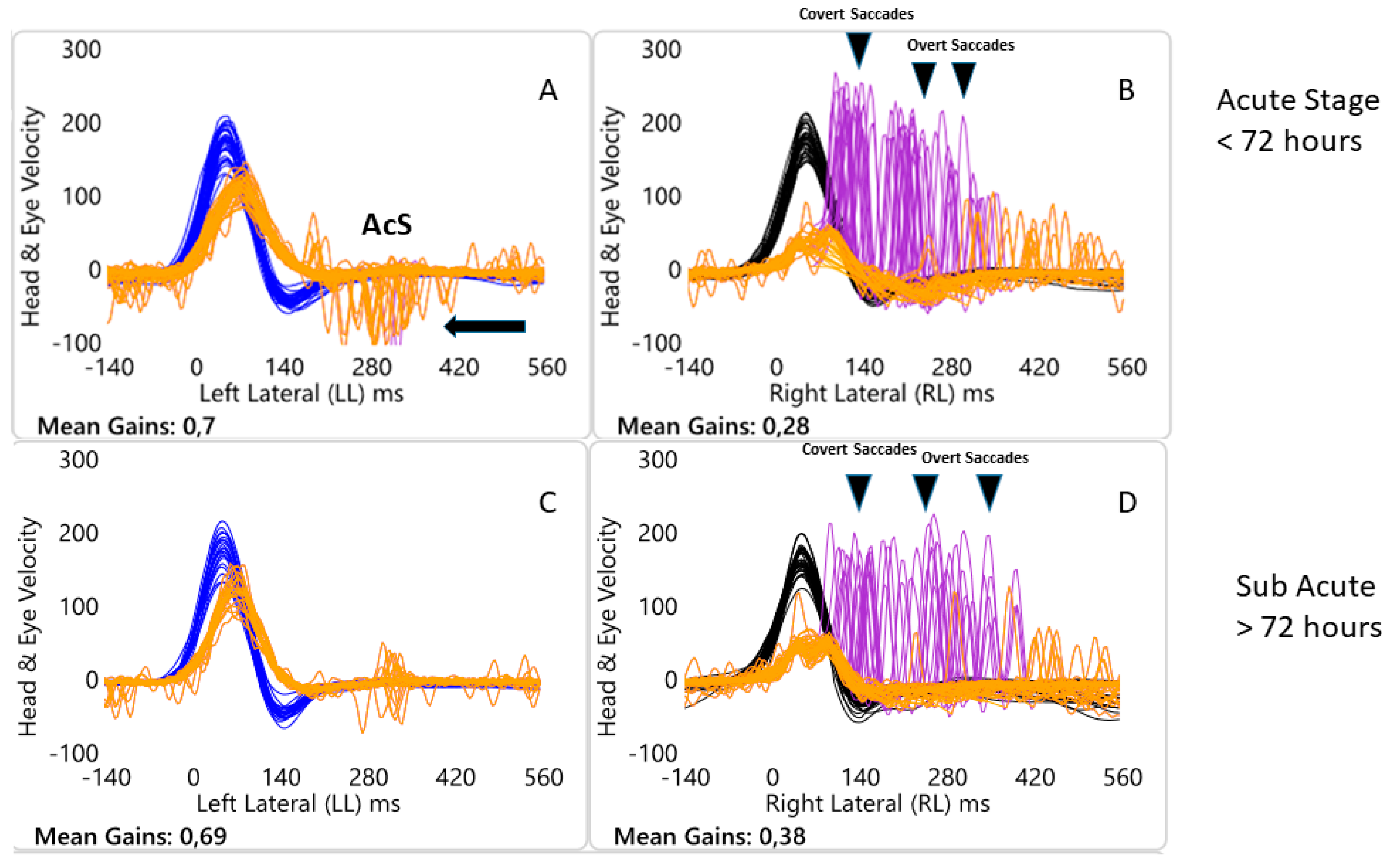
Secondly, VOR destabilization process that occurs during SVN can also be associated with the presence of AcS (
Figure 2) [
12], that can be highlighted in particular, by turning the head towards the healthy side, in the early stages of the disease and which tend to be absent in the PAVSg (73%) as well as disappear in all patients of VASg at second evaluation (
Figure 2).
About this phenomenon, AcS presence could be associated, in our opinion, as a sign of peripheral deficit due to the contribution to the process of the quick eye movements linked to the failure of the affected side to contribute to the desired realization of the reflex. These saccadic movements are in the same direction of the head movement and it has been previously hypothesized that they are an indicator of peripheral injury [
12]. Last but not least, considering our sample, we can hypothesize that this phenomenon could be an indicator of acute peripheral injury in the very early stages of the inflammatory process.
For this reason, why are AcS, in “early” vHIT evaluation, so potentially valuable especially as an indicator of VN acute stage? Following unilateral vestibular loss, it is known that the spontaneous nystagmus pattern is characterized by a slow phase of its horizontal component in the opposite direction of head rotation while the quick phase, rapid eye movement in the direction of head rotation, is directed away from the lesioned side, in the same direction of head rotation.
It is also known: (a) quick phases and saccades are both rapid eye movements with similar kinematics characteristics and (b) there are two distinct neural circuits responsible for the genesis of horizontal eye movements. The first for the slow phase in response to head turns, generated by the direct three neurons pathway: receptor/vestibular nucleus/abducens motoneurons/extraocular eye muscles.
The second is instead responsible for the generation of a separate neural circuit involving a network of burst neurons and pause neurons in the brainstem extremely close to abducens nucleus [
15]. This last circuit can be triggered by vestibular input thereby generating the quick phase of vestibular nystagmus during prolonged horizontal angular acceleration or by descending axons from the superior colliculus causing voluntary saccades but there is also evidence that input from neck afferents can also trigger this quick phase neural circuit [
15].
In our patients, the horizontal slow phase mechanism was disabled at the acute stage (as shown by the very low gain VOR <72 h after the AVS onset, see
Figure 2A,B) most probably because of the acute damage to the superior vestibular nerve component. However, the quick phase mechanism was unaffected as shown by the saccades at each head turn toward affected side and just like in the case of spontaneous nystagmus, when the head is passively and abruptly turned towards the healthy side, a quick phase (AcS), similar to that of spontaneous nystagmus directed away from the lesioned side, is generated. Essentially these quick eye movements seem to be related to the presence of spontaneous nystagmus. The latter in the acute phases of unilateral SVN can be reduced but not completely suppressed in the light. In fact, vHIT test is usually conducted not in darkness but in an illuminated environment.
We acknowledge some limitations of the present study. First, we reported only the hVOR values of the patients with unilateral Superior VN but further studies could be carried out also in patients with complete VN. Another limitation is that patients of PAVSg were evaluated in a larger range of time with respect to AVSg but to the best of our knowledge there is not a scientific consensus on the time of VN phases (e.g., acute, post acute or chronic). Furthermore, a follow up is needed in further studies to better evaluate the true clinical evolution of AVS in these patients.






{kind=link}
{kind=link}