

Hyperbaric Oxygen Therapy in Plastic, Aesthetic, and Reconstructive Surgery: Systematic Review

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy
2.3. Evaluation of Criteria and Synthesis of the Manuscripts
2.4. Data Extraction
2.5. Outcomes
2.6. Quality Evaluation
3. Results
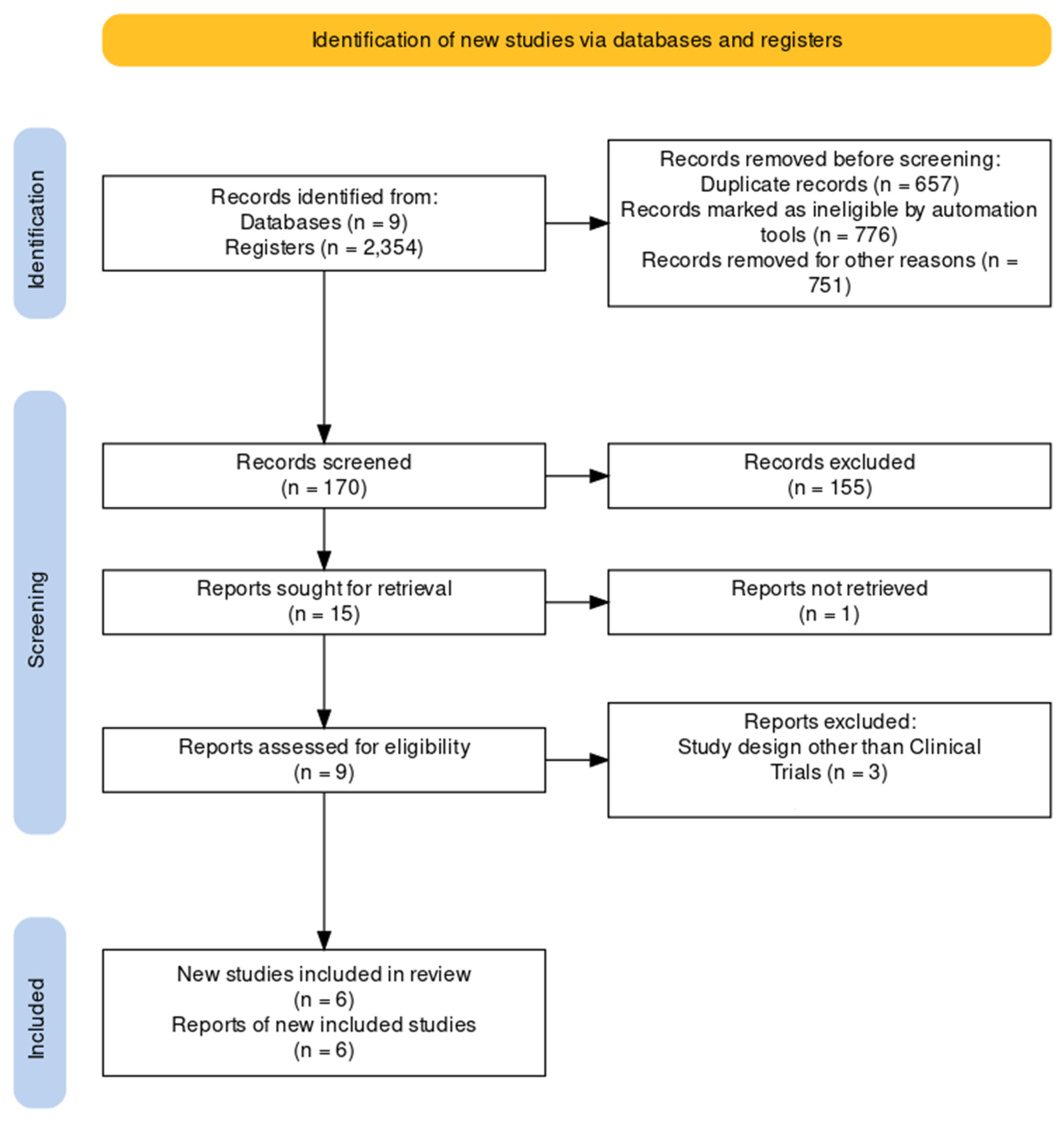
3.1. Studies Identified and Selected
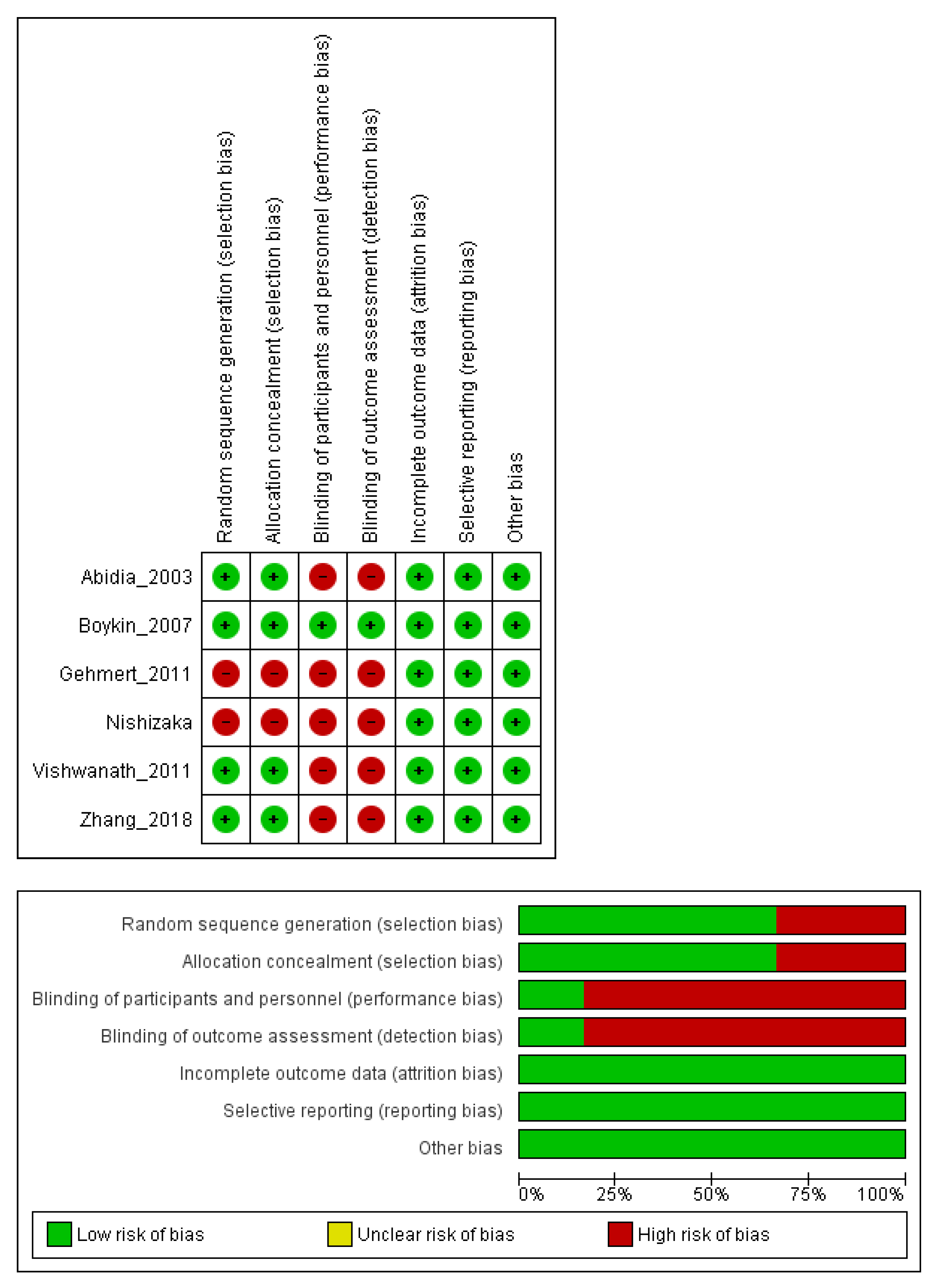
3.2. Risk of Bias
3.3. Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- de Andrade, S.M.; Santos, I.C.R.V. Oxigenoterapia Hiperbárica Para Tratamento de Feridas. Rev. Gaúcha Enferm. 2016, 37, e59257. [Google Scholar] [CrossRef]
- Bassetto, F.; Bosco, G.; Kohlscheen, E.; Tocco Tussardi, I.; Vindigni, V.; Tiengo, C. Hyperbaric Oxygen Therapy in Plastic Surgery Practice: Case Series and Literature Overview. Il G. Chir. 2019, 40, 257–275. [Google Scholar]
- Baltacıoğlu, E.; Bağış, B.; Arslan, A.; Kehribar, M.A.; Yuva, P.; Aydın, G.; Yılmaz, M.; Şenel, F.Ç. Effects of Peri-Implant Plastic Surgery and Hyperbaric Oxygen Therapy on Mandibular Avascular Necrosis After Implant Surgery. J. Oral Implantol. 2015, 41, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Covarrubias, L.; Sanchez-Rodriguez, E.C. Hyperbaric Oxygenation Therapy, Basic Concepts. Gac. Med. Mex. 2000, 136, 45–56. [Google Scholar]
- Cannellotto, M.; Romero-Feris, D.; Pascuccio, M.M.; Jordá-Vargas, L. Aplicaciones Médicas de Las Cámaras de Oxigenación Hiperbárica de Nueva Generación/Medical Applications of New Generation Hyperbaric Oxygenation Chambers. Rev. Asoc. Médica Argent. 2018, 131. [Google Scholar]
- Rodríguez, E.C.S.; Vidal, J.T.; Covarrubias, L.G.; Schmidt, A.C. Aplicaciones de La Terapia Con Oxigenación Hiperbárica En Cirugía Plástica. Cirugía Plást. Mex. 2001, 11, 25–32. [Google Scholar]
- Stoekenbroek, R.M.; Santema, T.B.; Legemate, D.A.; Ubbink, D.T.; van den Brink, A.; Koelemay, M.J.W. Hyperbaric Oxygen for the Treatment of Diabetic Foot Ulcers: A Systematic Review. Eur. J. Vasc. Endovasc. Surg. 2014, 47, 647–655. [Google Scholar] [CrossRef]
- Eskes, A.; Vermeulen, H.; Lucas, C.; Ubbink, D.T. Hyperbaric Oxygen Therapy for Treating Acute Surgical and Traumatic Wounds. Cochrane Database Syst. Rev. 2013, 12. [Google Scholar] [CrossRef]
- Thom, S.R. Hyperbaric Oxygen: Its Mechanisms and Efficacy. Plast. Reconstr. Surg. 2011, 127, 131S–141S. [Google Scholar] [CrossRef]
- Dauwe, P.B.; Pulikkottil, B.J.; Lavery, L.; Stuzin, J.M.; Rohrich, R.J. Does Hyperbaric Oxygen Therapy Work in Facilitating Acute Wound Healing. Plast. Reconstr. Surg. 2014, 133, 208e–215e. [Google Scholar] [CrossRef]
- Fodor, L.; Ramon, Y.; Meilik, B.; Carmi, N.; Shoshani, O.; Ullmann, Y. Effect of Hyperbaric Oxygen on Survival of Composite Grafts in Rats. Scand. J. Plast. Reconstr. Surg. Hand Surg. 2006, 40, 257–260. [Google Scholar] [CrossRef] [PubMed]
- Booth, A.; Clarke, M.; Dooley, G.; Ghersi, D.; Moher, D.; Petticrew, M.; Stewart, L. The Nuts and Bolts of PROSPERO: An International Prospective Register of Systematic Reviews. Syst. Rev. 2012, 1, 2. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions [Manual Cochrane de Revisiones Sistemáticas de Intervenciones, in Spanish]; Cochrane Collab: London, UK, 2011; pp. 1–639. Available online: www.cochrane-handbook.org (accessed on 20 June 2022).
- Abidia, A.; Laden, G.; Kuhan, G.; Johnson, B.F.; Wilkinson, A.R.; Renwick, P.M.; Masson, E.A.; McCollum, P.T. The Role of Hyperbaric Oxygen Therapy in Ischaemic Diabetic Lower Extremity Ulcers: A Double-Blind Randomised-Controlled Trial. Eur. J. Vasc. Endovasc. Surg. 2003, 25, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Boykin, J.V.; Baylis, C. Hyperbaric Oxygen Therapy Mediates Increased Nitric Oxide Production Associated With Wound Healing. Adv. Ski. Wound Care 2007, 20, 382–389. [Google Scholar] [CrossRef]
- Gehmert, S.; Geis, S.; Lamby, P.; Roll, C.; Braumandl, U.; Hidayat, M.; Sultan, M.; Fuechtmeier, B.; Jung, E.M.; Prantl, L. Evaluation of Hyperbaric Oxygen Therapy for Free Flaps Using Planar Optical Oxygen Sensors. Preliminary Results. Clin. Hemorheol. Microcirc. 2011, 48, 75–79. [Google Scholar] [CrossRef]
- Vishwanath, G. Hyperbaric Oxygen Therapy in Free Flap Surgery: Is It Meaningful? Med. J. Armed India 2011, 67, 253–256. [Google Scholar] [CrossRef]
- Zhang, M.; Liu, S.; Guan, E.; Liu, H.; Dong, X.; Hao, Y.; Zhang, X.; Zhao, P.; Liu, X.; Pan, S.; et al. Hyperbaric Oxygen Therapy Can Ameliorate the EMT Phenomenon in Keloid Tissue. Medicine 2018, 97, e11529. [Google Scholar] [CrossRef]
- Nishizaka, T.; Nomura, T.; Sano, T.; Higuchi, K.; Nagatomo, F.; Ishihara, A. Hyperbaric Oxygen Improves Ultraviolet B Irradiation-Induced Melanin Pigmentation and Diminishes Senile Spot Size. Ski. Res. Technol. 2011, 17, 332–338. [Google Scholar] [CrossRef]
- Long, F.; Wang, X. Potential Therapeutic Effects of Hyperbaric Oxygen for Improving Cosmetic Outcomes in Skin Grafts. Burns 2013, 39, 1026–1027. [Google Scholar] [CrossRef]
- Andel, H.; Kamolz, L.; Andel, D.; Brenner, L.; Frey, M.; Zimpfer, M. Sauerstoff Als Medikament Und Seine Bedeutung Für Die Wundheilung. Handchir. Mikrochir. Plast. Chir. 2007, 39, 328–332. [Google Scholar] [CrossRef]
- Sarabahi, S.; Tiwari, V.K. Principles and Practice of Wound Care, 1st ed.; Pearson: London, UK, 2012; Chapter 38. Hyperbaric Oxygen Therapy in Management of Wounds; ISBN 978-93-5025-864-4. [Google Scholar]
- Bhutani, S.; Vishwanath, G. Hyperbaric Oxygen and Wound Healing. Indian J. Plast. Surg. 2012, 45, 316–324. [Google Scholar] [CrossRef] [PubMed]
- Camison, L.; Naran, S.; Lee, W.-W.; Grunwaldt, L.J.; Davit, A.J.; Goldstein, J.A.; O’Toole, K.S.; Losee, J.E.; Adetayo, O.A. Hyperbaric Oxygen Therapy for Large Composite Grafts: An Alternative in Pediatric Facial Reconstruction. J. Plast. Reconstr. Aesthetic Surg. 2020, 73, 2178–2184. [Google Scholar] [CrossRef]
- Korambayil, P.; Ambookan, P.; Karangath, R. Necrotising Soft-Tissue Infections with Hyperbaric Oxygen Therapy as an Adjunct: A Tertiary Care Experience. J. Clin. Sci. Res. 2021, 10, 173. [Google Scholar] [CrossRef]
- Walden, W.C.; Hentges, D.J. Differential Effects of Oxygen and Oxidation Reduction Potential on the Multiplication of Three Species of Anaerobic Intestinal Bacteria. Appl. Microbiol. 1975, 30, 781–785. [Google Scholar] [CrossRef] [PubMed]
- Tsuneyoshi, I.; Boyle III, W.A.; Kanmura, Y.; Fujimoto, T. Hyperbaric Hyperoxia Suppresses Growth of Staphylococcus Aureus, Including Methicillin-Resistant Strains. J. Anesth. 2001, 15, 29–32. [Google Scholar] [CrossRef] [PubMed]
- Altunay, I.; Kucukunal, A.; Sarikaya, S.; Tukenmez Demirci, G. A Favourable Response to Surgical Intervention and Hyperbaric Oxygen Therapy in Pyoderma Gangrenosum. Int. Wound J. 2012, 11, 350–353. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. Hyperbaric Oxygen Therapy: Get the Facts. Available online: https://www.fda.gov/consumers/consumer-updates/hyperbaric-oxygen-therapy-get-facts (accessed on 6 February 2023).
- de Smet, G.H.J.; Kroese, L.F.; Menon, A.G.; Jeekel, J.; van Pelt, A.W.J.; Kleinrensink, G.-J.; Lange, J.F. Oxygen Therapies and Their Effects on Wound Healing. Wound Repair Regen. 2017, 25, 591–608. [Google Scholar] [CrossRef]
- Kindwall, E.P.; Gottlieb, L.J.; Larson, D.L. Hyperbaric Oxygen Therapy in Plastic Surgery. Plast. Reconstr. Surg. 1991, 88, 898–908. [Google Scholar] [CrossRef]
- Eskes, A.M.; Ubbink, D.T.; Lubbers, M.J.; Lucas, C.; Vermeulen, H. Hyperbaric Oxygen Therapy: Solution for Difficult to Heal Acute Wounds? Systematic Review. World J. Surg. 2010, 35, 535–542. [Google Scholar] [CrossRef]
- Nigro, L.C.; Feldman, M.J.; Blanchet, N.P. Burn in an Irradiated Prepectoral Breast Reconstruction. Plast. Reconstr. Surg. Glob. Open 2018, 6, e1874. [Google Scholar] [CrossRef]
- Enomoto, M.; Yagishita, K.; Okuma, K.; Oyaizu, T.; Kojima, Y.; Okubo, A.; Maeda, T.; Miyamoto, S.; Okawa, A. Hyperbaric Oxygen Therapy for a Refractory Skin Ulcer after Radical Mastectomy and Radiation Therapy: A Case Report. J. Med. Case Rep. 2017, 11, 5. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, V.M.; Borgen, A.E.; Jansen, E.C.; Rotbøll Nielsen, P.H.; Werner, M.U. Hyperbaric Oxygen Therapy Attenuates Central Sensitization Induced by a Thermal Injury in Humans. Acta Anaesthesiol. Scand. 2015, 59, 749–762. [Google Scholar] [CrossRef] [PubMed]
- Adorno Filho, E.T.; Almeida, K.G.D.; Reis, G.D.C.; Costa, G.R.; Kracik, A.S.; Tuluche, L.H.F.; Souza, A.S.D.; Marques, G.D.S. Cost Analysis in Patients Admitted to the Santa Casa Misericórdia de Campo Grande, Treated with and without the Aid of Hyperbaric Oxygen Therapy. Rev. Bras. De Cir. Plástica (RBCP) Braz. J. Plast. Sugery 2014, 29, 562–566. [Google Scholar] [CrossRef]
- Rahman, M.U.; Khan, M.R.K.; Ahmed, T.; Islam, M.S.B.; Nayeem, R.; Kalam, M.A. Hyperbaric Oxygen Therapy in Non Healing Wounds in a Referral Hospital of Bangladesh. J. Bangladesh Coll. Physicians Surg. 2019, 37, 109–118. [Google Scholar] [CrossRef]
- Siewiera, J.; Brodaczewska, K.; Jermakow, N.; Lubas, A.; Kłos, K.; Majewska, A.; Kot, J. Effectiveness of Hyperbaric Oxygen Therapy in SARS-CoV-2 Pneumonia: The Primary Results of a Randomised Clinical Trial. J. Clin. Med. 2023, 12, 8. [Google Scholar] [CrossRef]
- Kitala, D.; Łabuś, W.; Kozielski, J.; Strzelec, P.; Nowak, M.; Knefel, G.; Dyjas, P.; Materniak, K.; Kosmala, J.; Pająk, J.; et al. Preliminary Research on the Effect of Hyperbaric Oxygen Therapy in Patients with Post-COVID-19 Syndrome. J. Clin. Med. 2023, 12, 308. [Google Scholar] [CrossRef]
- Gierek, M.; Łabuś, W.; Kitala, D.; Lorek, A.; Ochała-Gierek, G.; Zagórska, K.M.; Waniczek, D.; Szyluk, K.; Niemiec, P. Human Acellular Dermal Matrix in Reconstructive Surgery—A Review. Biomedicines 2022, 10, 2870. [Google Scholar] [CrossRef]
- Gierek, M.; Łabuś, W.; Słaboń, A.; Ziółkowska, K.; Ochała-Gierek, G.; Kitala, D.; Szyluk, K.; Niemiec, P. Co-Graft of Acellular Dermal Matrix and Split Thickness Skin Graft—A New Reconstructive Surgical Method in the Treatment of Hidradenitis Suppurativa. Bioengineering 2022, 9, 389. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Abidia [14] | Boykin [15] | Zhang [18] | Gehmert [16] | Vishwanat [17] | Nishizaka [19] | |
|---|---|---|---|---|---|---|
| Publication year | 2003 | 2007 | 2018 | 2011 | 2011 | 2011 |
| Number of patients | 18 | 6 | 27 | 6 | 10 | 21 |
| Diagnosis | Skin ulcers | Skin ulcers | Wound healing disorders: Keloids. | Free flaps | Free flaps | Melanin pigmentation, age spot |
| Country of the study | United Kingdom | United Sates | China | Germany | India | Japan |
| Comorbidities | Yes | Yes | No | No | No | No |
| Type of comorbidity | Mellitus Diabetes | Mellitus Diabetes | None | None | None | None |
| Comparator | Hyperbaric air | No reports | No reports | No alternative treatment | No reports | Normobaric environment at 1ATA with 21% oxygen |
| Abidia et al. [14] | Boykin [15] | Zhang [18] | Gehmert [16] | Vishwanath [17] | Nishizaka [19] | |
|---|---|---|---|---|---|---|
| Session duration | 90 | 90 | 90 | 90 | 60 | 60 |
| Days of the week | 5 | 7 | 1 | 7 | 2 to 3 | |
| Number of cycles | 30 | 20 | 7 | 1 | 1 | 4 to 12 |
| HBOT Atmospheres Absolute ATA | 2.4 | 2 | 2 | 2.4 | No reports | 1.25 |
| Author | Outcome | p Value |
|---|---|---|
| Abidia [14] | Reduction in the size of the ulcer | 0.026 |
| Healing of the ulcer after one year of treatment | 0.027 | |
| Decrease in medical visits for bandages (33.75 vs. 136.5) Lower cost of care (GBP1972 vs. GBP7946) | ||
| Boykin [15] | Progressive reduction in area Increased formation of granulation tissue Significant increase in local levels of nitric oxide in the wound | <0.05 |
| Zhang [18] | Perfusion in the keloid was significantly reduced after HBOT. Lower expression levels of vimentin, vibronectin, vascular endothelial growth factor, and hypoxia-inducible factor-1a, and expression of E-cadherin and Zonula ocludens (ZO-1) were observed. The expression of E-cadherin and ZO-1 mRNA was also increased. | <0.01 |
| Gehmert [16] | Increased partial pressure of transcutaneous oxygen in the flap 83.45 ± 13.80 Torr. | <0.001 |
| Vishwanath [17] | No significant differences were found in flap survival, time to resolution of venous congestion, resolution of edema, and postoperative recovery period. | >0.05 |
| Nishizaka [19] | Accelerates both the fading of melanin pigmentation and the decrease in age spot size. | <0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ríos-Gómez, M.; Gómez-Ortega, V.; Cardona, C.; De la Hoz-Valle, J.A. Hyperbaric Oxygen Therapy in Plastic, Aesthetic, and Reconstructive Surgery: Systematic Review. Surg. Tech. Dev. 2023, 12, 43-52. https://doi.org/10.3390/std12010003
Ríos-Gómez M, Gómez-Ortega V, Cardona C, De la Hoz-Valle JA. Hyperbaric Oxygen Therapy in Plastic, Aesthetic, and Reconstructive Surgery: Systematic Review. Surgical Techniques Development. 2023; 12(1):43-52. https://doi.org/10.3390/std12010003
Chicago/Turabian StyleRíos-Gómez, Mariana, Viviana Gómez-Ortega, Cesar Cardona, and Jose A. De la Hoz-Valle. 2023. "Hyperbaric Oxygen Therapy in Plastic, Aesthetic, and Reconstructive Surgery: Systematic Review" Surgical Techniques Development 12, no. 1: 43-52. https://doi.org/10.3390/std12010003
APA StyleRíos-Gómez, M., Gómez-Ortega, V., Cardona, C., & De la Hoz-Valle, J. A. (2023). Hyperbaric Oxygen Therapy in Plastic, Aesthetic, and Reconstructive Surgery: Systematic Review. Surgical Techniques Development, 12(1), 43-52. https://doi.org/10.3390/std12010003