1. Introduction
Currently, pancreaticoduodenectomy (PD) is the main surgical procedure for carcinoma of the head of the pancreas and periampullary adenocarcinoma. Since PD surgery requires the removal of several organs and complex anatomical relationships, as well as reconstruction of the digestive tract, the early postoperative mortality rate is 20–30%. In recent years, with the rapid development of surgical techniques and careful planning of the perioperative period, the mortality rate has decreased to less than 5% [
1], but the postoperative complication rate remains relatively high [
2,
3,
4], so PD is one of the most complicated procedures in abdominal surgery. Therefore, surgeons need to do early accurate diagnosis for such tumors, make clear the situation, such as the size the shape and adjacent organs of the tumor, whether the surrounding vascular system was invaded by the tumor, etc. Thus, we can make individualized surgery and treatment plan for patients according preoperative evaluation, that will reduce postoperative complications. In the past, some surgeons attempted to generate more intuitive images using imaging methods to achieve more accurate preoperative assessment. However, traditional imaging methods such as CT and MRI do not provide an accurate three-dimensional (3D) image, which affects the surgeon’s judgment of anatomical structures during the surgery. Because the image is still a two-dimensional plane image and lacks a sense of three-dimensional image, the surgeon still needs to carry out 3D reconstruction of the two-dimensional image in his mind to complete the preoperative surgical evaluation, which will inevitably make the surgeon make different judgments or even make wrong diagnosis due to their own experience. With the development of digital medicine, two-dimensional (2D) data can be transformed into 3D images through computer processing, which is more helpful to surgeons for preoperative assessment of patients and the development of surgical plans to improve the safety of surgery. This study retrospectively analyzed the clinical data of 47 patients who underwent PD at the Department of Hepatobiliary Surgery of Ningxia Medical University General Hospital between November 2018 and December 2019 to explore the value of 3D visualization technology in preoperative planning of PD.
2. Information and Methods
2.1. General Information
Inclusion criteria for this study: (1) patients whose systemic condition permitted surgical treatment; (2) the preoperative proposed surgical plan was PD; (3) the same group of physicians completed the surgery; (4) Child’s method was used if gastrointestinal reconstruction was performed; (5) preoperative imaging did not require re-vascularization and/or organ resection; (6) complete clinical data.
Exclusion criteria: (1) severe cardiopulmonary insufficiency; (2) patients who could not tolerate general anesthesia and surgical treatment; (3) missing data.
The clinical data of 47 patients who underwent PD at the Department of Hepatobiliary Surgery of Ningxia Medical University General Hospital between November 2018 and December 2019, including 23 males and 24 females; mean age (55.00 ± 10.06) years, were retrospectively collected. Those cases include seven cases of distal bile duct cancer, 27 cases of pancreatic head tumors, and 13 cases of periampullary tumors, the study patients were in early stage. All patients underwent enhanced CT as part of their routine preoperative assessment. No patient had any comorbid condition that made PD unsafe, and all patients provided written informed consent. The operation planning with 2D and 3D images was done by the same person in each case.
2.2. Study Methods
The included patients underwent preoperative enhanced CT scans of the abdomen. Spiral CT images were obtained using the GE Hispeed Advantage scanner (Milwaukee, Brookfield, WI, USA). Pre-contrast images were obtained and reconstructed at 10-mm intervals, followed by a dual-phase contrast study. The scanning parameters used for the contrast examination were collimation 737 mm, pitch 1.2:120 kV, and 120 mA. Approximately 100 mL contrast agent (Niopam 300, Merck Pharmaceuticals, West Drayton, UK) diluted in a 60:40 mix with saline was injected. The automated Smartprep facility (GE) was used to trigger the initial phase, and the region of intersection was placed on the portal vein. The two contrast phases were separated by a delay of 15 s.
Volumetric studies were conducted using the commercially available software (inlook 3D) 3D analysis package. The acquired 2D data information (DICOM form) was imported into medical image three-dimensional visualization system (MI-3DVS) software. The outline of each section was manually traced. The computer stacked the data from each section, allowing 3D volumetric reconstructions and measurements, and the different tissues such as the tumor, lymph node, surrounding organ and their adjacent vasculature were rendered to different colors. The 3D image models were then established. By splitting, combining, rotating, enlarging, or shrinking the 3D reconstructed images, and the 3D model also can be hyalinized, rotated, zoomed, and assembled arbitrarily at various degree angles, the operator can precisely understand the size, location, anatomical relationship with the surrounding vascular system and bile duct system as well as the existence of vascular variants, etc., and formulate the surgical plan and preoperative evaluation based on the 3D data. All of the above data and image processing were performed by the same surgical team and were calibrated by the operator.
2.3. Development of the Surgical Plan
According to the anatomical relationship between the tumor, blood vessels and surrounding organs [
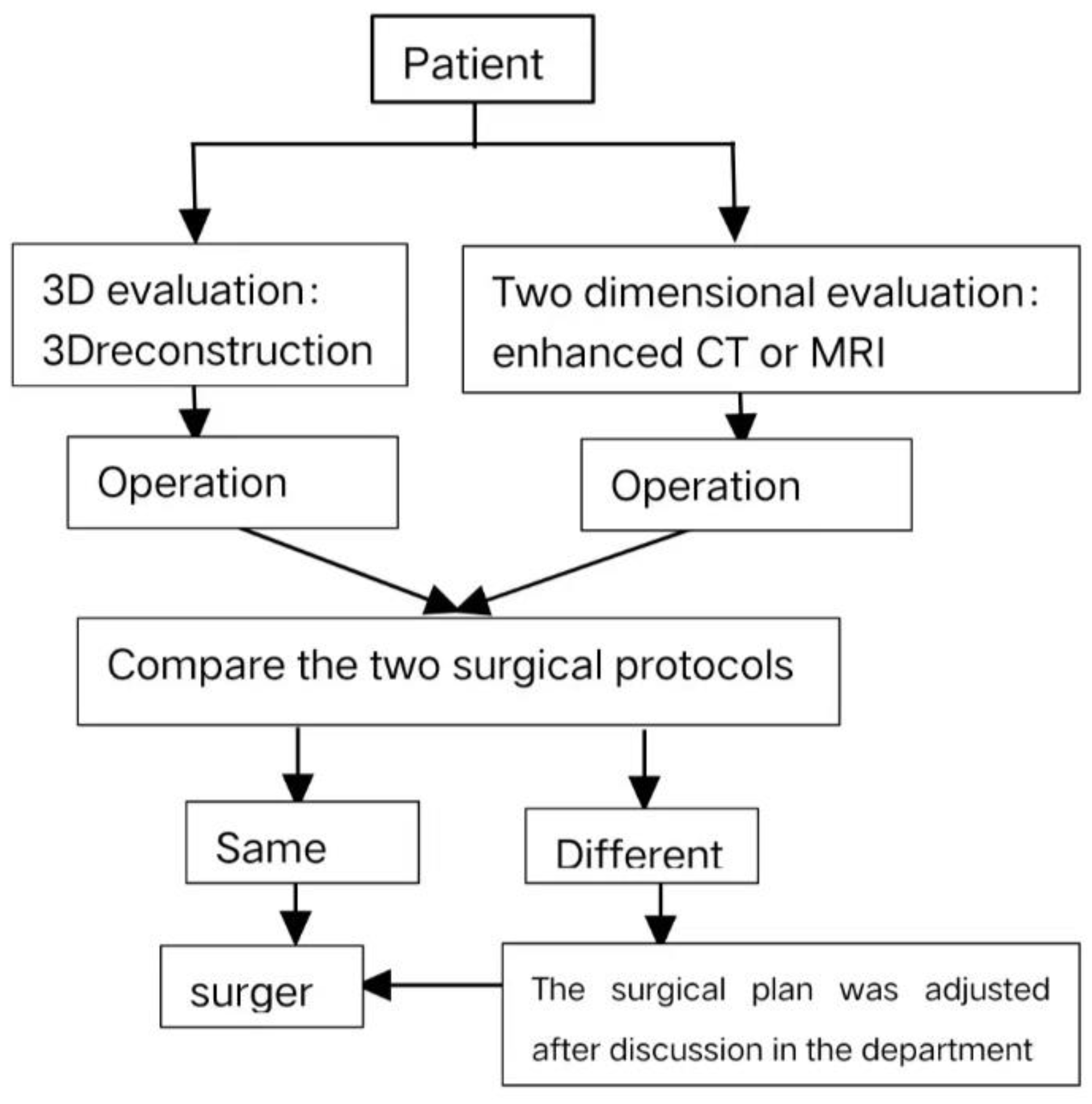
5], the surgical plan was developed separately by applying 2D CT or MRI images and 3D reconstruction models. If the two plans were consistent, the surgery was performed according to the 2D evaluation images, and if the tumor invaded the surrounding tissues and vascular variants, the surgery was performed mainly according to the 3D evaluation images. The specific process is shown in
Figure 1.
2.4. Observation Indexes
(1) The degree of conformity between the surgical plan assessed in two dimensions, the surgical plan assessed by 3D reconstruction and the actual surgical plan performed; (2) the tumor volume measured by preoperative 3D reconstruction and the tumor volume measured by postoperative pathology; (3) the peri-pancreatic vascular variation; (4) the operating time, intraoperative bleeding volume, postoperative hospitalization days, postoperative complications (pancreatic fistula, bile leakage, gastric emptying disorder, thoracoabdominal fluid); (5) analysis of typical cases.
2.5. Statistical Analysis
SPSS 25.0 statistical software was used to analyze the data. The measurement data were expressed as Mean ± SD for normal distribution and M (range) for skewed distribution. The count data were expressed as percentages or absolute values. The predicted tumor volume after 3D reconstruction and postoperative pathological tumor volume data were analyzed. Paired sample t-test was used if normal distribution was observed, and Wilcoxon test was used if normal distribution was not observed. The Pearson’s correlation coefficient (r) was applied to analyze the correlation between them. A p < 0.05 indicated statistically significant difference.
3. Results
Among 47 cases before surgery, 37 cases (78.7%) were consistent with the surgical plan made by 2D evaluation and 3D evaluation, and 10 cases (21.3%) were inconsistent with the surgical plan made by 2D evaluation and 3D evaluation, mainly because the 3D evaluation revealed the invasion of adjacent vessels and organs by the tumor, and the surgical plan was adjusted according to the analysis of the 3D reconstruction before surgery, and the actual surgery changed in three cases, and the proposed PD was optimized and improved in seven cases, it include to change of the surgical dissection approach, to improve the methods of pancreatic-intestinal anastomosis and so on. The preoperative 3D reconstructed surgical plan matched 100% with the actual surgical plan.
The tumor volume measured by preoperative 3D reconstruction was (19.69 ± 23.47) mL, and the postoperative pathological tumor volume was (17.07 ± 20.29) mL. The difference between the two
t-test results (t = 0.54,
p = 0.59) was not statistically significant, and the Pearson’s correlation test (r = 0.766,
p = 0.00) showed a significant correlation, as shown in
Figure 2.
The operative time was (4.85 ± 1.75) h, intraoperative bleeding was 447.05 (50–5000) mL, postoperative hospital stay was (26.13 ± 11.13) days. The postoperative complications included pancreatic fistula in six cases, including 0 cases of grade C pancreatic fistula, two cases of bile leakage, four cases of gastric emptying disorder, and three cases of thoracoabdominal fluid. According to the typing of hepatic artery variants by Michels et al. [
6], there were two cases (4.25%) of type II, four cases (8.51%) of type III, and the remaining had no variants.
Typical Case
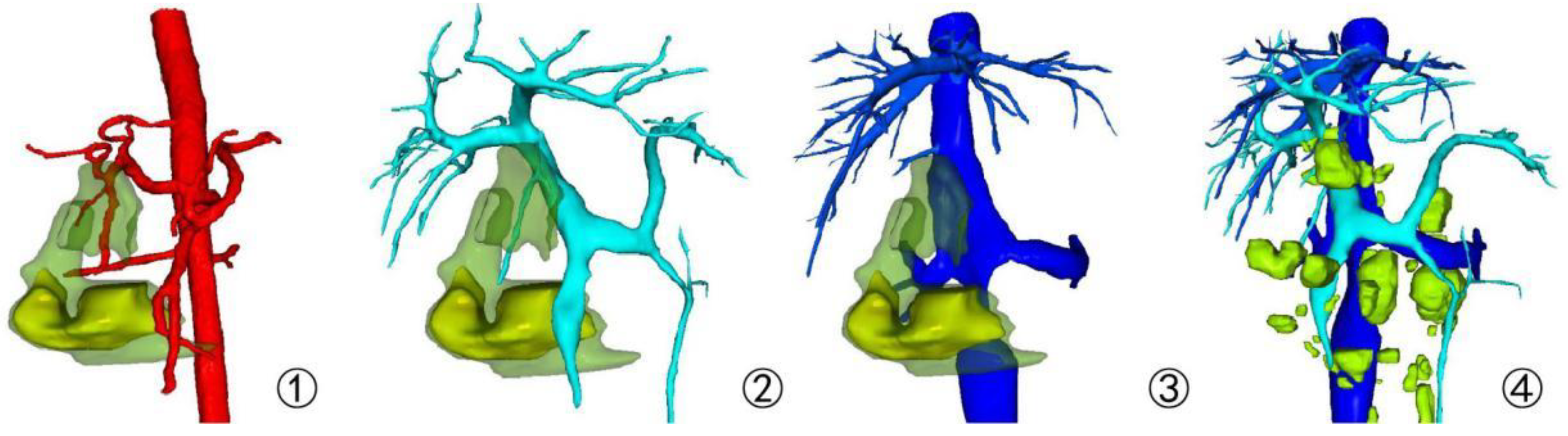
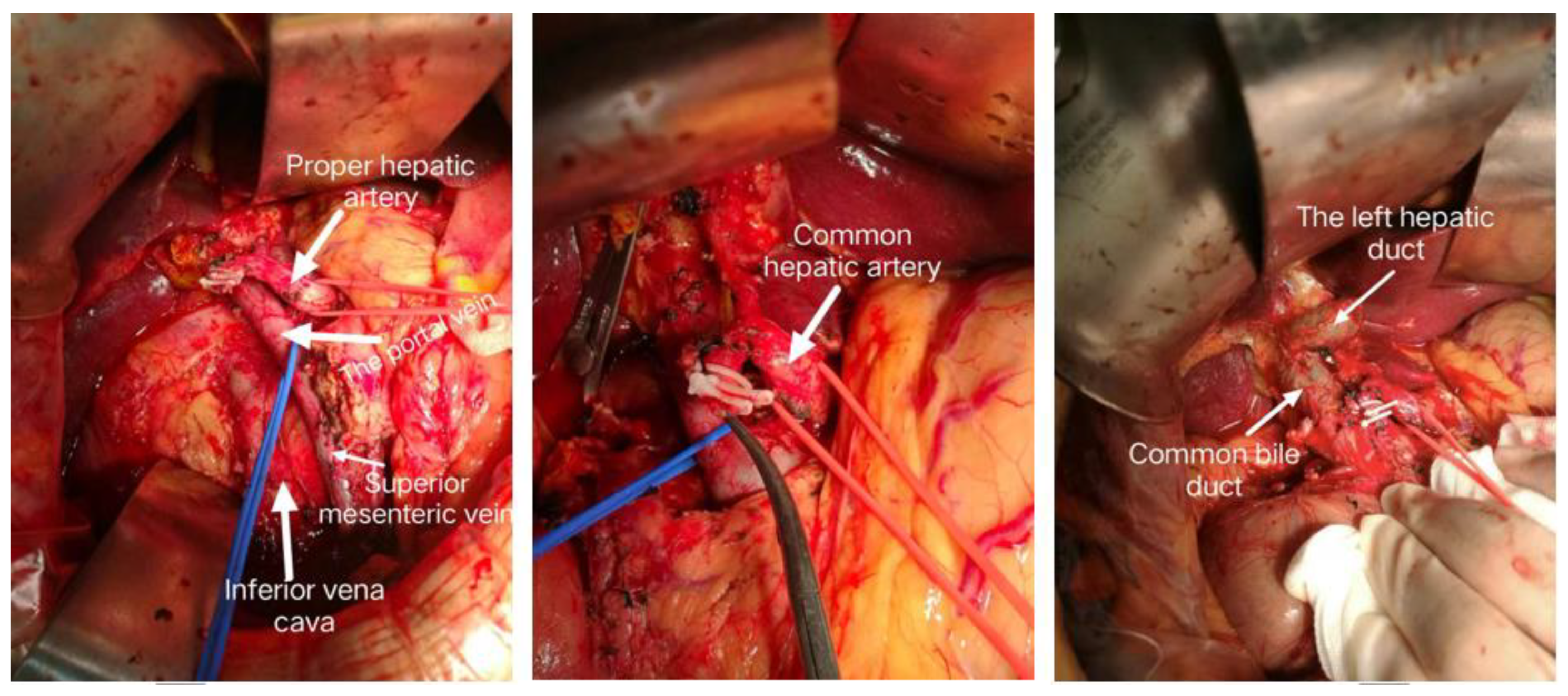
A 64-year-old female patient was admitted with obstructive jaundice. MRCP showed an irregular soft tissue mass in the descending duodenum, approximately 5.3 × 5.0 cm, and a mildly dilated pancreatic duct. There were multiple enlarged lymph nodes adjacent to the abdominal aorta. The surgical plan was formulated according to the 2D images. Considering that the tumor originated from the duodenum, the tumor was poorly defined with the portal vein and inferior vena cava, excluding invasion, the proposed PD was not radical. The tumor volume was 50.15 mL. The tumor was considered to originate from the head of the pancreas and invade the duodenum, and there was a gap between the tumor and the portal vein, inferior vena cava and abdominal aorta, and no vascular invasion was seen. Multiple enlarged lymph nodes were seen next to the peri-pancreatic vessels, and radical surgery and lymph node dissection were feasible, as shown in
Figure 3 and
Figure 4. The tumor was located in the head of the pancreas and invaded the intestinal lumen of the duodenum. The size of the tumor was assessed in the preoperative 3D evaluation, and there were gaps between the tumor and the surrounding blood vessels. The intraoperative bleeding was 300 mL, without blood transfusion. The operation time was 240 min, without postoperative complications. Postoperative pathology showed pancreatic head adenocarcinoma, hypofractionated lymph nodes (0/15), with nerve invasion (
Figure 5).
4. Discussion
Pancreaticoduodenectomy (PD) is one of the most complicated operations in abdominal surgery, with high postoperative complication rate [
7]. Among modern medical imaging methods, US, CT, and MRI are commonly used for evaluation, and surgeons need to accurately localize the lesion and understand its surrounding invasion based on these imaging examinations to facilitate accurate intraoperative judgments and avoid unnecessary intraoperative injuries and bleeding, thus ensuring safe and smooth operation [
8]. However, these traditional imaging examinations provide 2D images, and surgeons can only recognize these anatomical relationships and the spatial adjacency of surrounding organs based on their own comprehensive thinking process when reading the films, and such 3D reconstructions formed in the mind are often subjective and unstable, sometimes differing greatly from the actual situation, and the surgical planning lacks a practical and realistic basis. With the rapid development of minimally invasive techniques in recent years, laparoscopic PD, which is a more refined operation, is gradually accepted [
9], and a more effective, safe, and intuitive diagnostic imaging method that can accurately display the peri-pancreatic anatomy and make accurate assessment is urgently needed.
With the development of digital medical technology and surgical techniques, 3D visualization technology has been widely used in preoperative planning of abdominal surgery [
10], especially in complex surgeries. Compared with the traditional 2D images of CT or MRI, 3D visualization technology can clearly reproduce the 3D morphology of the pancreas and the characteristics of the anatomical structures around the membrane gland, which can provide a more intuitive, and accurate understanding of the size and location of the tumor; the depth and invasion of the vasculature and bile duct system, as well as the existence and degree of variation. The preoperative implementation of simulated surgical operations through 3D visualization technology can help reduce intraoperative medical injury, and improve the efficiency and safety of the surgery [
11,
12,
13]. In this study, all 47 cases were preoperatively assessed as resectable by 3D visualization technology, and all cases were successfully operated with 100% accuracy of resectability assessment, among which three cases were converted from classical PD to PD with preserved pylorus after careful analysis of local anatomy with the aid of navigation by 3D visualization technology. In seven cases, after preoperative conventional imaging suggested that only palliative surgery could be performed due to vascular invasion, radical PD was successfully performed by optimizing the surgical plan and using techniques such as arterial access after 3D visualization assessment. In the cases we evaluated preoperatively, the measurement of tumor volume was consistent with the actual postoperative pathology, without statistical differences. In addition, we carefully studied the alignment of the vessels in the region of the pancreatic head, variants and other common intraoperative conditions by splitting, rotating, magnifying or reducing the images, so that they could be handled safely and timely during the operation. Considering the most common hepatic artery variation as an example, according to the typing method of Michels [
6] and others, type III is the most common, with an incidence of 10.56%, i.e., the right hepatic artery originates from the superior mesenteric artery, which is also one of the easily mislaid vessels intraoperatively. The intraoperative findings were consistent with this, and damage to the variant hepatic artery was effectively avoided. These findings reflect the advantage of 3D visualization techniques for accurate preoperative evaluation.
According to the literature, the use of 3D visualization technology to assist PD, optimize the surgical path, and choose the optimal surgical plan can shorten the operative time and reduce intraoperative bleeding, thus reducing postoperative complications such as pancreatic fistula [
14,
15]. In our group of 47 patients, the operation time was (4.85 ± 1.75) h, intraoperative bleeding was 447.05 (50–5000) mL, and there were no severe grade C pancreatic fistulas. However, no control group was used for comparison. The above results may be statistically biased due to the greater influence of different operators’ surgical proficiency, patients’ underlying diseases, specific factors of the pancreas, and pancreatic-intestinal anastomosis methods, which is why a control group was not set up in this study. In our experience, the 3D visualization technique enabled the operator to have a good understanding of the surgical anatomical procedures, major structural variants, etc., as well as the preoperative virtualized surgical training, which will increase the operator’s self-confidence and ease of intraoperative operation, thus significantly improving the above situation. However, the above needs to be validated by a large sample and multi-center stratified experimental design.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}




