
Bisphosphonate Use for Glucocorticoid-Induced Osteoporosis in Elderly Patients with Immune Thrombocytopenia Receiving Prolonged Steroid Therapy: A Single Institute Retrospective Study



Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
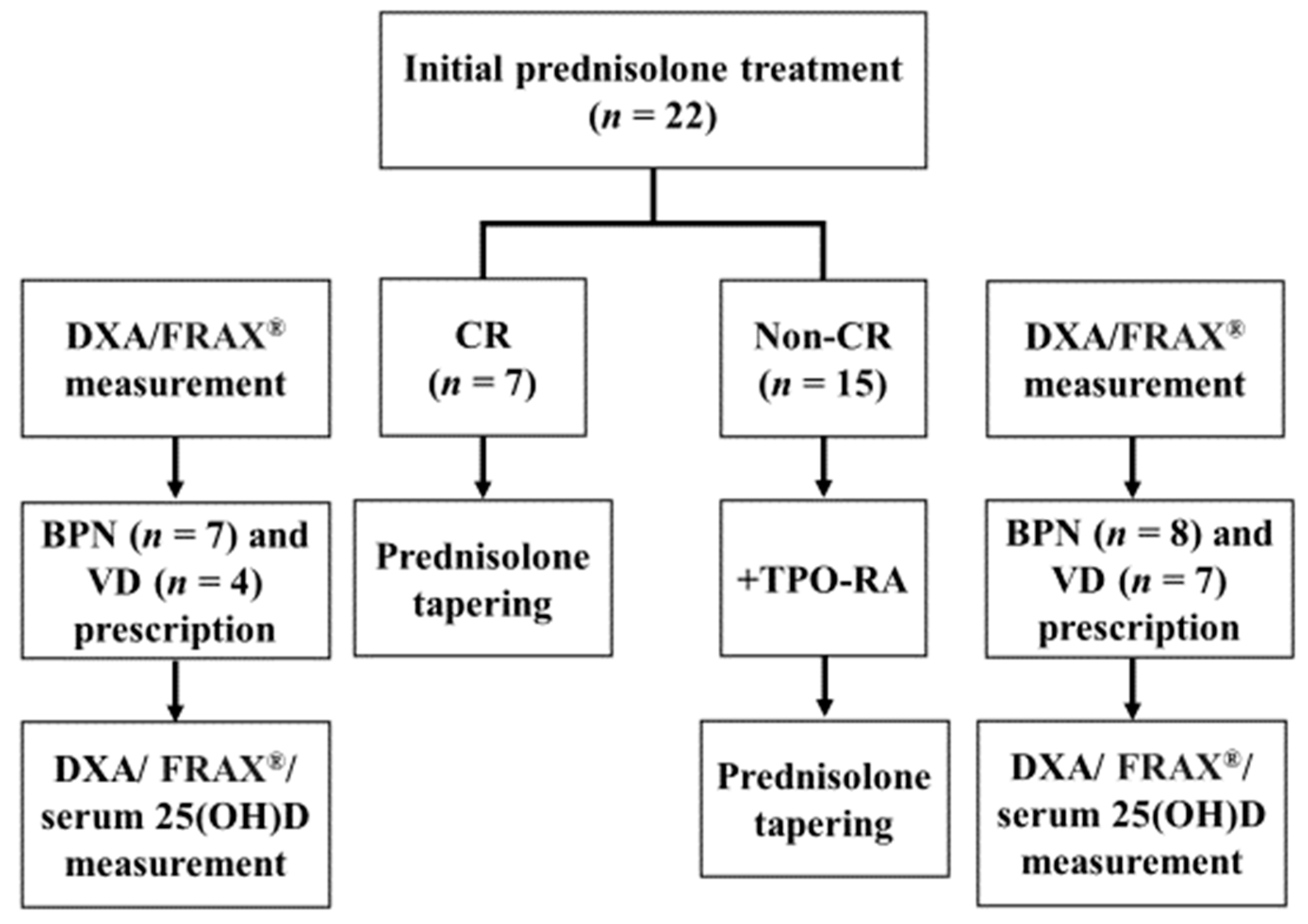
2.2. Treatment
2.3. Response Criteria
2.4. Prescription for the Prevention of Glucocorticoid-Induced Osteoporosis
2.5. Statistical Methods
3. Results
3.1. Patient Characteristics
3.2. Treatment Response to the Initial Prednisolone Treatment
3.3. Score Changes during the Initial Loading of Prednisolone Treatment
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hill, Q.A.; Grainger, J.D.; Thachil, J.; Provan, D.; Evans, G.; Garg, M.; Bradbury, C.; Bagot, C.; Kanis, J.A.; Compston, J.E.; et al. The prevention of glucocorticoid-induced osteoporosis in patients with immune thrombocytopenia receiving steroids: A British Society for Haematology Good Practice Paper. Br. J. Haematol. 2019, 185, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Gasbarrini, A.; Franceschi, F.; Tartaglione, R.; Landolfi, R.; Pola, P.; Gasbarrini, G. Regression of autoimmune thrombocytopenia after eradication of Helicobacter pylori. Lancet 1998, 352, 878. [Google Scholar] [CrossRef]
- Kuwana, M. Helicobacter pylori-associated immune thrombocytopenia: Clinical features and pathogenic mechanisms. World J. Gastroenterol. 2014, 20, 714–723. [Google Scholar] [CrossRef] [PubMed]
- Kashiwagi, H. Reference guide for the treatment of adult idiopathic thrombocytopenic purpura. Rinsho Ketsueki 2020, 61, 1325–1330. [Google Scholar] [PubMed]
- Kado, R.; McCune, W.J. Treatment of primary and secondary immune thrombocytopenia. Curr. Opin. Rheumatol. 2019, 31, 213–222. [Google Scholar] [CrossRef]
- Provan, D.; Arnold, D.M.; Bussel, J.B.; Chong, B.H.; Cooper, N.; Gernsheimer, T.; Ghanima, W.; Godeau, B.; González-López, T.J.; Grainger, J.; et al. Updated international consensus report on the investigation and management of primary immune thrombocytopenia. Blood Adv. 2019, 3, 3780–3817. [Google Scholar] [CrossRef]
- Canalis, E.; Mazziotti, G.; Giustina, A.; Bilezikian, J.P. Glucocorticoid-induced osteoporosis: Pathophysiology and therapy. Osteoporos. Int. 2007, 18, 1319–1328. [Google Scholar] [CrossRef]
- Neunert, C.; Terrell, D.R.; Arnold, D.M.; Buchanan, G.; Cines, D.B.; Cooper, N.; Cuker, A.; Despotovic, J.M.; George, J.N.; Grace, R.F.; et al. American Society of Hematology 2019 guidelines for immune thrombocytopenia. Blood Adv. 2019, 3, 3829–3866. [Google Scholar] [CrossRef]
- Rossini, M.; Viapiana, O.; Vitiello, M.; Malavolta, N.; La Montagna, G.; Maddali Bongi, S.; Di Munno, O.; Nuti, R.; Manzini, C.U.; Ferri, C.; et al. Prevalence and incidence of osteoporotic fractures in patients on long-term glucocorticoid treatment for rheumatic diseases: The Glucocorticoid Induced OsTeoporosis TOol (GIOTTO) study. Reumatismo 2017, 69, 30–39. [Google Scholar] [CrossRef]
- van Staa, T.P.; Leufkens, H.G.; Cooper, C. The epidemiology of corticosteroid-induced osteoporosis: A meta-analysis. Osteoporos. Int. 2002, 13, 777–787. [Google Scholar] [CrossRef]
- Buckley, L.; Guyatt, G.; Fink, H.A.; Cannon, M.; Grossman, J.; Hansen, K.E.; Humphrey, M.B.; Lane, N.E.; Magrey, M.; Miller, M.; et al. 2017 American College of Rheumatology Guideline for the Prevention and Treatment of Glucocorticoid-Induced Osteoporosis. Arthritis Rheumatol. 2017, 69, 1521–1537. [Google Scholar] [CrossRef]
- Kanis, J.A. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis: Synopsis of a WHO report. WHO Study Group. Osteoporos Int. 1994, 4, 368–381. [Google Scholar] [CrossRef] [PubMed]
- Nomura, S.; Kurata, Y.; Tomiyama, Y.; Takubo, T.; Hasegawa, M.; Saigo, K.; Nishikawa, M.; Higasa, S.; Maeda, Y.; Hayashi, K. Effects of bisphosphonate administration on the bone mass in immune thrombocytopenic purpura patients under treatment with steroids. Clin. Appl. Thromb. Hemost. 2010, 16, 622–627. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Nawata, H.; Soen, S.; Fujiwara, S.; Nakayama, H.; Tanaka, I.; Ozono, K.; Sagawa, A.; Takayanagi, R.; Tanaka, H.; et al. Guidelines on the management and treatment of glucocorticoid-induced osteoporosis of the Japanese Society for Bone and Mineral Research: 2014 update. J. Bone Miner. Metab. 2014, 32, 337–350. [Google Scholar] [CrossRef] [PubMed]
- Rodeghiero, F.; Stasi, R.; Gernsheimer, T.; Michel, M.; Provan, D.; Arnold, D.M.; Bussel, J.B.; Cines, D.B.; Chong, B.H.; Cooper, N.; et al. Standardization of terminology, definitions and outcome criteria in immune thrombocytopenic purpura of adults and children: Report from an international working group. Blood 2009, 113, 2386–2393. [Google Scholar] [CrossRef]
- Holloway-Kew, K.L.; Zhang, Y.; Betson, A.G.; Anderson, K.B.; Hans, D.; Hyde, N.K.; Nicholson, G.C.; Pocock, N.A.; Kotowicz, M.A.; Pasco, J.A. How well do the FRAX (Australia) and Garvan calculators predict incident fractures? Data from the Geelong Osteoporosis Study. Osteoporos. Int. 2019, 30, 2129–2139. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Rizzoli, R.; Adachi, J.D.; Cooper, C.; Dere, W.; Devogelaer, J.P.; Diez-Perez, A.; Kanis, J.A.; Laslop, A.; Mitlak, B.; Papapoulos, S.; et al. Management of glucocorticoid-induced osteoporosis. Calcif. Tissue Int. 2012, 91, 225–243. [Google Scholar] [CrossRef]
- Rizzoli, R.; Biver, E. Glucocorticoid-induced osteoporosis: Who to treat with what agent? Nat. Rev. Rheumatol. 2015, 11, 98–109. [Google Scholar] [CrossRef]
- Lane, N.E. Glucocorticoid-Induced Osteoporosis: New Insights into the Pathophysiology and Treatments. Curr. Osteoporos. Rep. 2019, 17, 1–7. [Google Scholar] [CrossRef]
- Brauer, C.A.; Coca-Perraillon, M.; Cutler, D.M.; Rosen, A.B. Incidence and mortality of hip fractures in the United States. JAMA 2009, 302, 1573–1579. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Saito, T.; Oyama, M.; Oshiki, R.; Kobayashi, R.; Nishiwaki, T.; Nashimoto, M.; Tsuchiya, Y. Vitamin D sufficiency is associated with low incidence of limb and vertebral fractures in community-dwelling elderly Japanese women: The Muramatsu Study. Osteoporos. Int. 2011, 22, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Shulman, N.R.; Weinrach, R.S.; Libre, E.P.; Andrews, H.L. The role of the reticuloendothelial system in the pathogenesis of idiopathic thrombocytopenic purpura. Trans. Assoc. Am. Physicians 1965, 78, 374–390. [Google Scholar] [PubMed]
- Gernsheimer, T.; Stratton, J.; Ballem, P.J.; Slichter, S.J. Mechanisms of response to treatment in autoimmune thrombocytopenic purpura. N. Engl. J. Med. 1989, 320, 974–980. [Google Scholar] [CrossRef]
- Kitchens, C.S.; Weiss, L. Ultrastructural changes of endothelium associated with thrombocytopenia. Blood 1975, 46, 567–578. [Google Scholar] [CrossRef]
- Kitchens, C.S. Amelioration of endothelial abnormalities by prednisone in experimental thrombocytopenia in the rabbit. J. Clin. Investig. 1977, 60, 1129–1134. [Google Scholar] [CrossRef]
- Provan, D.; Stasi, R.; Newland, A.C.; Blanchette, V.S.; Bolton-Maggs, P.; Bussel, J.B.; Chong, B.H.; Cines, D.B.; Gernsheimer, T.B.; Godeau, B.; et al. International consensus report on the investigation and management of primary immune thrombocytopenia. Blood 2010, 115, 168–186. [Google Scholar] [CrossRef]
- Xu, G.; Yamamoto, N.; Hayashi, K.; Takeuchi, A.; Miwa, S.; Igarashi, K.; Taniguchi, Y.; Araki, Y.; Yonezawa, H.; Morinaga, S. The accuracy of different FRAX tools in predicting fracture risk in Japan: A comparison study. J. Orthop. Surg. 2020, 28, 2309499020917276. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | n= 22 | |
| Median age (range), years | 79 (70–90) | |
| >85 years old, n (%) | 7 (32) | |
| Body mass index, median (range), kg/m2 | 23 (17–31) | |
| Sex, n (%) | male | 7 (32) |
| female | 15 (68) | |
| Antinuclear antibody positive, n (%) | 4 (18) | |
| Autoimmune disease, n (%) | 2 (9) | |
| History of Helicobacter pylori eradication, n (%) | 6 (27) | |
| Baseline platelet level (×109/L), median (range) | 16 (1–19) | |
| Total prednisolone dose for treatment until<5 mg prednisolone daily administration, median (range), g/kg | 46 (34–50) | |
| ≥5 mg prednisolone daily administration period, median (range), months | 21 (2–31) | |
| Thrombopoietin receptor agonist administration,n(%) | 15 (68) | |
| Bisphosphonate prescription, n (%) | 15 (68) | |
| Active vitamin D prescription, n (%) | 11 (50) | |
| Serum 25-hydroxyvitamin D post-prednisolone treatment, median (range), ng/mL | 30.5 (17.0–34.0) | |
| Follow-up time, median (range), months | 26 (8–86) | |
| Characteristic, Median (Range) | n = 22 | OR a | 95% CI | p | |
|---|---|---|---|---|---|
| Lumbar BMD T-score | initial loading | −1.1 (−1.6–0.3) | reference | ||
| tapering phases | −1.3 (−1.8–−0.3) | 0.46 | −0.05–0.98 | 0.07 | |
| Femoral neck bone BMD T-score | initial loading | −1.1 (−1.6–0) | reference | ||
| tapering phases | −1.5 (−2.0–0) | 0.23 | −0.21–0.59 | 0.29 | |
| FRAX® b (major osteoporotic, %) | initial loading | 11.5 (5.4–23.0) | reference | ||
| tapering phases | 12.0 (6.0–21.0) | 0.94 | 0.86–0.97 | <0.01 | |
| FRAX® b (hip, %) | initial loading | 3.1 (0.8–7.8) | reference | ||
| tapering phases | 3.5 (0.6–8.7) | 0.84 | 0.66–0.93 | <0.01 | |
| Garvan-defined osteoporotic fracture (5 year, %) | initial loading | 9 (4–27) | reference | ||
| tapering phases | 9.5 (4–31) | 0.89 | 0.76–0.95 | <0.01 | |
| Garvan-defined osteoporotic fracture (10 year, %) | initial loading | 18 (7–45) | reference | ||
| tapering phases | 19 (8–51) | 0.91 | 0.79–0.96 | <0.01 | |
| Garvan-defined hip fracture (5 year, %) | initial loading | 2 (0.2–5) | reference | ||
| tapering phases | 2 (0.4–11) | 0.83 | 0.65–0.93 | <0.01 | |
| Garvan-defined hip fracture (10 year, %) | initial loading | 3 (0.4–10) | reference | ||
| tapering phases | 4 (0.7–20) | 0.85 | 0.68–0.94 | <0.01 | |
| with Bisphosphonate | with Active Vitamin D | |||||
|---|---|---|---|---|---|---|
| Characteristic | c.e. | 95%-CI | p | c.e. | 95%-CI | p |
| Lumbar BMDT-score | 0.61 | 0.14–1.08 | 0.01 | 0.36 | −8.77–9.50 | 0.93 |
| Femoral neck bone BMD T-score | 1.05 | 0.24–1.86 | 0.01 | −0.37 | −1.13–0.37 | 0.30 |
| FRAX® a (major osteoporotic, %) | −1.81 | −4.13–0.51 | 0.11 | 1.87 | −0.29–4.03 | 0.08 |
| FRAX® a (hip, %) | −1.36 | −3.12–0.39 | 0.12 | 1.26 | −0.37–2.90 | 0.12 |
| Garvan-defined osteoporotic fracture (5 year, %) | −2.39 | −7.88–3.10 | 0.37 | 2.43 | −2.68–7.54 | 0.33 |
| Garvan-defined osteoporotic fracture (10 year, %) | −4.82 | −13.0–3.42 | 0.23 | 4.70 | −2.97–12.3 | 0.21 |
| Garvan-defined hip fracture (5 year, %) | −1.77 | −4.26–0.70 | 0.15 | 1.35 | −0.96–3.66 | 0.23 |
| Garvan-defined hip fracture (10 year, %) | −3.13 | −7.66–1.40 | 0.16 | 2.56 | −1.66–6.79 | 0.22 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamasaki, S.; Kamezaki, K.; Ito, Y.; Horiuchi, T. Bisphosphonate Use for Glucocorticoid-Induced Osteoporosis in Elderly Patients with Immune Thrombocytopenia Receiving Prolonged Steroid Therapy: A Single Institute Retrospective Study. Hematol. Rep. 2022, 14, 276-285. https://doi.org/10.3390/hematolrep14030039
Yamasaki S, Kamezaki K, Ito Y, Horiuchi T. Bisphosphonate Use for Glucocorticoid-Induced Osteoporosis in Elderly Patients with Immune Thrombocytopenia Receiving Prolonged Steroid Therapy: A Single Institute Retrospective Study. Hematology Reports. 2022; 14(3):276-285. https://doi.org/10.3390/hematolrep14030039
Chicago/Turabian StyleYamasaki, Satoshi, Kenjiro Kamezaki, Yoshikiyo Ito, and Takahiko Horiuchi. 2022. "Bisphosphonate Use for Glucocorticoid-Induced Osteoporosis in Elderly Patients with Immune Thrombocytopenia Receiving Prolonged Steroid Therapy: A Single Institute Retrospective Study" Hematology Reports 14, no. 3: 276-285. https://doi.org/10.3390/hematolrep14030039
APA StyleYamasaki, S., Kamezaki, K., Ito, Y., & Horiuchi, T. (2022). Bisphosphonate Use for Glucocorticoid-Induced Osteoporosis in Elderly Patients with Immune Thrombocytopenia Receiving Prolonged Steroid Therapy: A Single Institute Retrospective Study. Hematology Reports, 14(3), 276-285. https://doi.org/10.3390/hematolrep14030039