
Hematologic Complications in Patients Hospitalized with COVID-19 Infection


Abstract
:1. Introduction
2. Materials and Methods
Study Population
3. Results
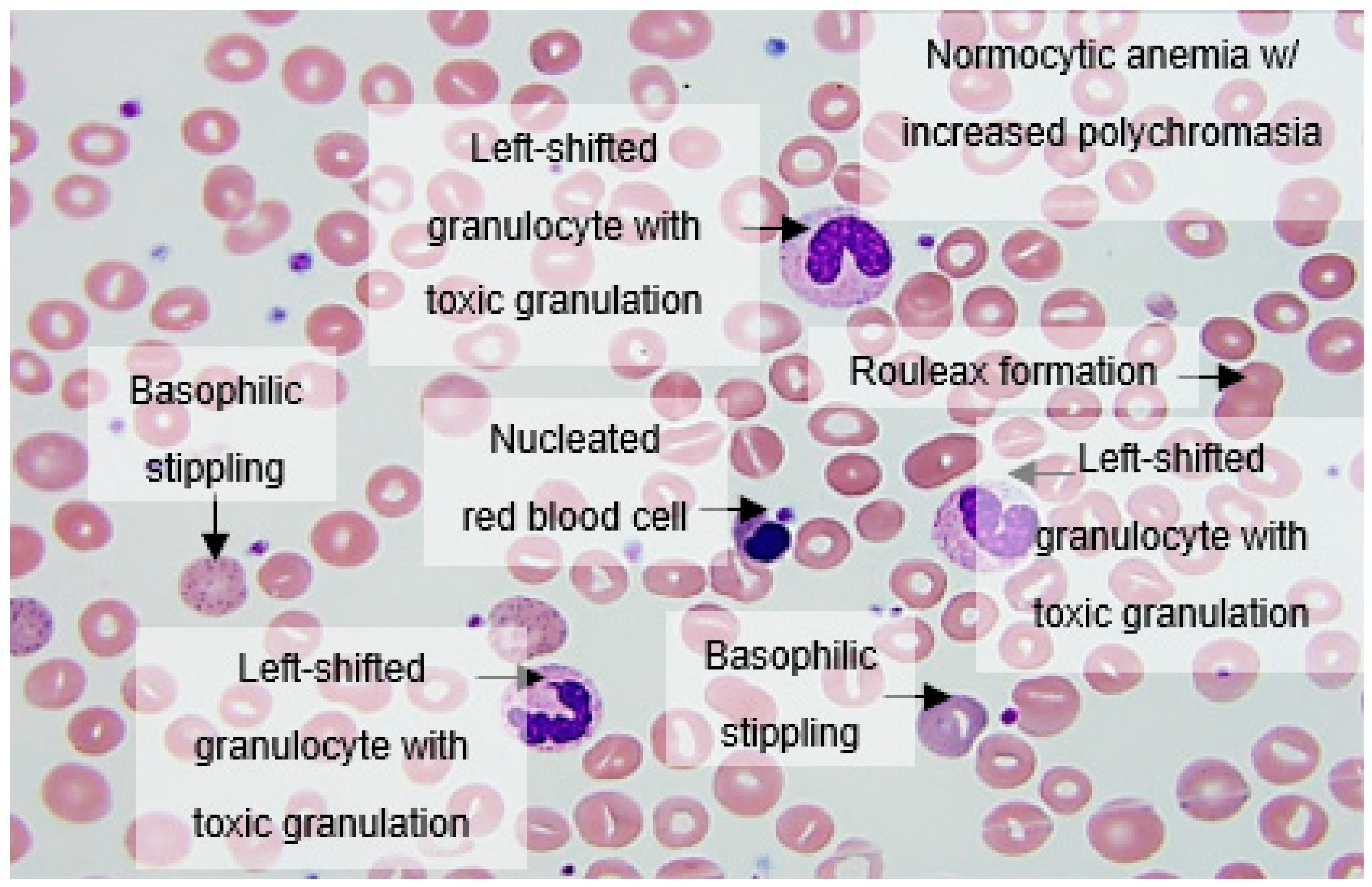
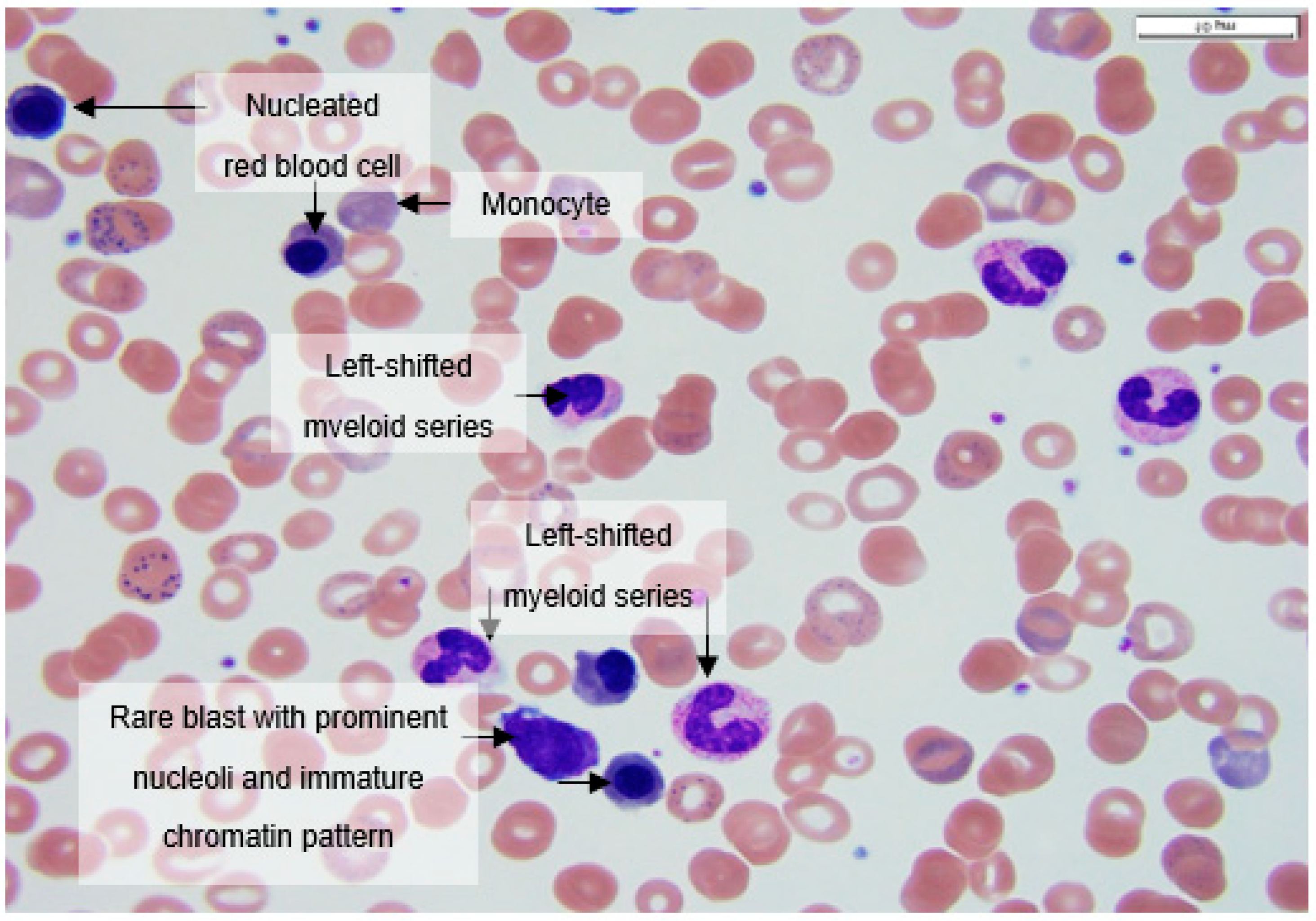
3.1. Morphological Anomalies in Peripheral Blood Smears from COVID-19 Patients
3.2. Hematologic Laboratory Abnormalities Correlate with Poor Clinical Outcome in COVID-19 Disease
4. Discussion
4.1. Hematologic Abnormalities in COVID-19 Are Related to Disease Progression, Severity, and Mortality
4.2. Lymphopenia in COVID-19
4.3. Hematologic Malignancies Put Patients at High Risk of COVID-19 Mortality
5. Conclusions
- Early diagnosis and follow-up of DIC by applying the ISTH score, which can determine prognosis and guide appropriate critical care support.
- Optimization of thromboprophylaxis regimen with LMWH as first-line drug.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Announces COVID-19 Outbreak a Pandemic. Available online: www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/news/news/2020/3/who-announces-covid-19-outbreak-a-pandemic (accessed on 31 May 2021).
- Al-Saadi, E.A.; Abdulnabi, M.A. Hematological changes associated with COVID-19 infection. J. Clin. Lab. Anal. 2021, 36, e24064. [Google Scholar] [CrossRef] [PubMed]
- Rahman, A.; Niloofa, R.; Jayarajah, U.; De Mel, S.; Abeysuriya, V.; Seneviratne, S.L. Hematological abnormalities in COVID-19: A narrative review. Am. J. Trop. Med. Hyg. 2021, 104, 1188–1201. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Zeng, X.; Jiao, Y.; Li, Z.; Liu, Q.; Ye, J.; Yang, M. Mechanisms involved in the development of thrombocytopenia in patients with COVID-19. Thromb. Res. 2020, 193, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Johns Hopkins University of Medicine Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/ (accessed on 21 January 2022).
- Asakura, H.; Ogawa, H. COVID-19-associated coagulopathy and disseminated intravascular coagulation. Int. J. Hematol. 2021, 113, 45–57. [Google Scholar] [CrossRef] [PubMed]
- Henry, B.M.; De Oliveira, M.H.S.; Benoit, S.; Plebani, M.; Lippi, G. Hematologic, biochemical and immune biomarker abnormalities associated with severe illness and mortality in coronavirus disease 2019 (COVID-19): A meta-analysis. Clin. Chem. Lab. Med. (CCLM) 2020, 58, 1021–1028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahi, M.S.; Jindal, V.; Reyes, S.P.; Gunasekaran, K.; Gupta, R.; Jaiyesimi, I. Hematologic disorders associated with COVID-19: A review. Ann. Hematol. 2021, 100, 309–320. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.; Meng, M.; Kumar, R.; Wu, Y.; Huang, J.; Deng, Y.; Weng, Z.; Yang, L. Lymphopenia is associated with severe coronavirus disease 2019 (COVID-19) infections: A systemic review and meta-analysis. Int. J. Infect. Dis. 2020, 96, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Terpos, E.; Ntanasis-Stathopoulos, I.; Elalamy, I.; Kastritis, E.; Sergentanis, T.N.; Politou, M.; Psaltopoulou, T.; Gerotziafas, G.; Dimopoulos, M.A. Hematological findings and complications of COVID-19. Am. J. Hematol. 2020, 95, 834–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agbuduwe, C.; Basu, S. Haematological manifestations of COVID-19: From cytopenia to coagulopathy. Eur. J. Haematol. 2020, 105, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Yip, C.Y.C.; Yap, E.S.; De Mel, S.; Teo, W.Z.Y.; Lee, C.T.; Kan, S.; Lee, M.C.C.; Loh, W.N.H.; Lim, E.L.; Lee, S.Y. Temporal changes in immune blood cell parameters in COVID-19 infection and recovery from severe infection. Br. J. Haematol. 2020, 190, 33–36. [Google Scholar] [CrossRef] [PubMed]
- Connors, J.M.; Levy, J.H. COVID-19 and its implications for thrombosis and anticoagulation. Blood 2020, 135, 2033–2040. [Google Scholar] [CrossRef] [PubMed]
- Wool, G.D.; Miller, J.L. The impact of COVID-19 disease on platelets and coagulation. Pathobiology 2021, 88, 15–27. [Google Scholar] [CrossRef] [PubMed]
- Maquet, J.; Lafaurie, M.; Sommet, A.; Moulis, G. Thrombocytopenia is independently associated with poor outcome in patients hospitalized for COVID-19. Br. J. Haematol. 2020, 190, e276–e279. [Google Scholar] [CrossRef]
- Vijenthira, A.; Gong, I.Y.; Fox, T.A.; Booth, S.; Cook, G.; Fattizzo, B.; Martín-Moro, F.; Razanamahery, J.; Riches, J.C.; Zwicker, J.; et al. Outcomes of patients with hematologic malignancies and COVID-19: A systematic review and meta-analysis of 3377 patients. Blood 2020, 136, 2881–2892. [Google Scholar] [CrossRef]
- Chari, A.; Samur, M.K.; Martinez-Lopez, J.; Cook, G.; Biran, N.; Yong, K.; Hungria, V.; Engelhardt, M.; Gay, F.; García Feria, A.; et al. Clinical features associated with COVID-19 outcome in multiple myeloma: First results from the International Myeloma Society data set. Blood 2020, 136, 3033–3040. [Google Scholar] [CrossRef]
- Pagano, L.; Salmanton-García, J.; Marchesi, F.; Corradini, P.; Hoenigl, M.; Klimko, N.; Koehler, P.; Pagliuca, A.; Passamonti, F.; Verga, L.; et al. COVID-19 infection in adult patients with hematological malignancies: A European Hematology Association Survey (EPICOVIDEHA). J. Hematol. Oncol. 2021, 14, 168. [Google Scholar] [CrossRef] [PubMed]
- Yigenoglu, T.N.; Ata, N.; Altuntas, F.; Bascı, S.; Dal, M.S.; Korkmaz, S.; Namdaroglu, S.; Basturk, A.; Hacıbekiroglu, T.; Dogu, M.H.; et al. The outcome of COVID-19 in patients with hematological malignancy. J. Med. Virol. 2021, 93, 1099–1104. [Google Scholar] [CrossRef] [PubMed]
- Cattaneo, C.; Daffini, R.; Pagani, C.; Salvetti, M.; Mancini, V.; Borlenghi, E.; D’Adda, M.; Oberti, M.; Paini, A.; De Ciuceis, C.; et al. Clinical characteristics and risk factors for mortality in hematologic patients affected by COVID-19. Cancer 2020, 126, 5069–5076. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Manifestation | Number (%) |
|---|---|
| Severe dyspnea and high fever, admitted to ICU Severe hypoxic respiratory failure requiring intubation | 21/31 (70%) 17/21 (81%) |
| Lymphopenia (<1.3 × 109/L) and occasional plasmacytoid reactive lymphocytes with exacerbation of lymphopenia over course of disease | 15/31 (48%) |
| Absolute neutrophilia (>5 × 109/L) with left-shifted granulocytes Decreasing trend in subsequent week (1.48–3.23 × 109/L) | 16/31 (52%) 7/16 (44%) |
| Hematologic malignancies or immunosuppressionICU admission and intubation, death | 8/31 (26%) 5/8 (63%) |
| Elevated LDH (>225 u/L) LDH > 1000 U/L | 21/31 (68%) 2/21 (10%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, E.; Araj, E.; Markantonis, J.; Luu, H.; Chen, M. Hematologic Complications in Patients Hospitalized with COVID-19 Infection. Hematol. Rep. 2022, 14, 228-234. https://doi.org/10.3390/hematolrep14030031
Lin E, Araj E, Markantonis J, Luu H, Chen M. Hematologic Complications in Patients Hospitalized with COVID-19 Infection. Hematology Reports. 2022; 14(3):228-234. https://doi.org/10.3390/hematolrep14030031
Chicago/Turabian StyleLin, Elisa, Ellen Araj, John Markantonis, Hung Luu, and Mingyi Chen. 2022. "Hematologic Complications in Patients Hospitalized with COVID-19 Infection" Hematology Reports 14, no. 3: 228-234. https://doi.org/10.3390/hematolrep14030031
APA StyleLin, E., Araj, E., Markantonis, J., Luu, H., & Chen, M. (2022). Hematologic Complications in Patients Hospitalized with COVID-19 Infection. Hematology Reports, 14(3), 228-234. https://doi.org/10.3390/hematolrep14030031