
Development of HIV Drug Resistance in a Cohort of Adults on First-Line Antiretroviral Therapy in Tanzania during the Stavudine Era

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
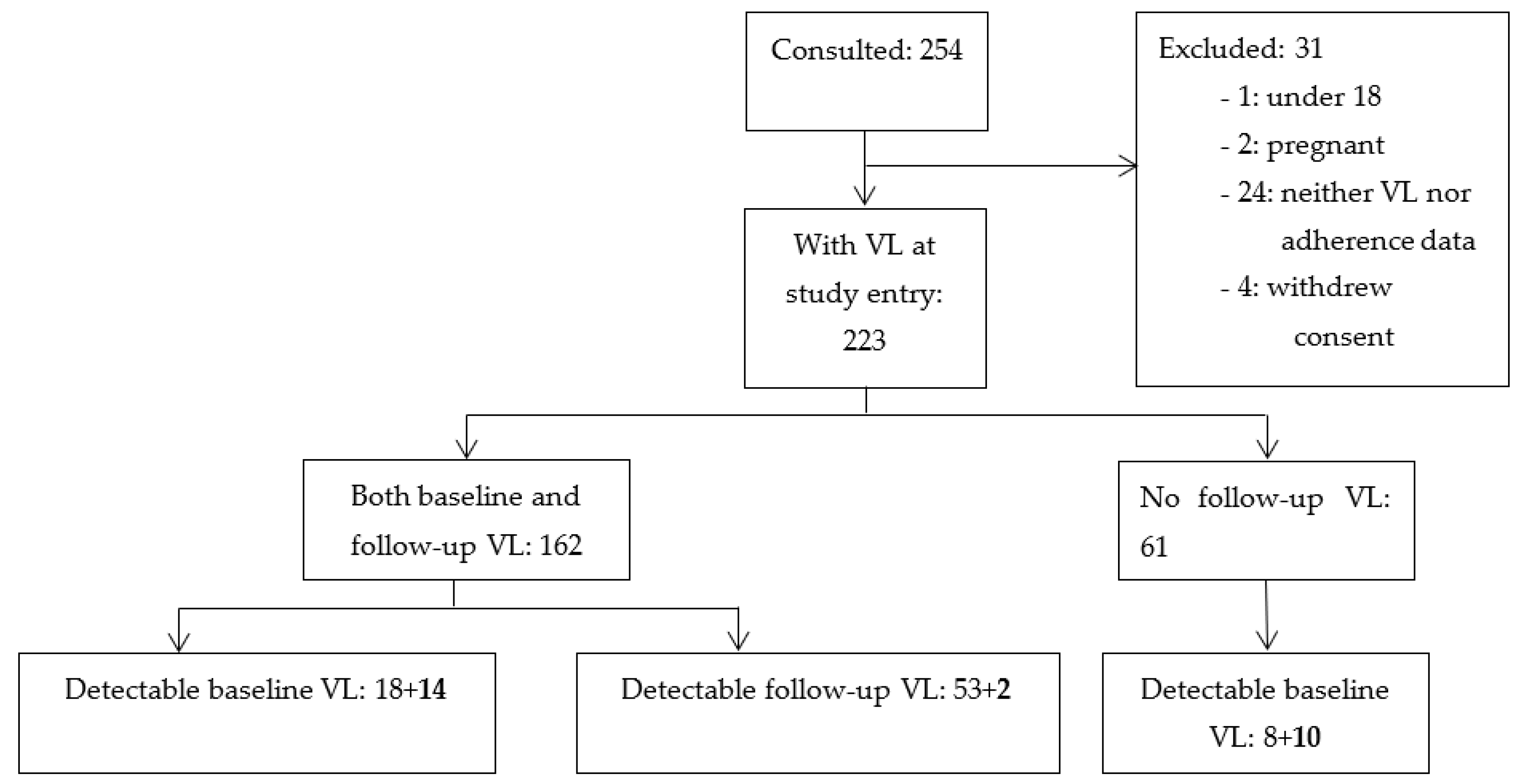
2.1. The Cohort Description
2.2. Data Collection Procedures
2.2.1. Treatment History and Clinical Data
2.2.2. Drawing of Blood Samples
2.2.3. Viral Load Measurement
2.2.4. Genotyping of Patients’ HIV Isolates
2.3. Data Storage and Analysis
3. Results
3.1. Description of Cohort Regimens
3.2. The Success Rate of Genotyping
3.3. Subtype Diversity
3.4. Virological Response Data
3.5. HIV Drug Resistance
3.5.1. Pre-Treatment Drug Resistance
3.5.2. Acquired Drug Resistance
4. Discussion
5. Study Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV Infection: Recommendations for a Public Health Approach, 2nd ed.; World Health Organization: Geneva, Switzerland, 2016; Available online: https://apps.who.int/iris/handle/10665/208825 (accessed on 15 November 2020).
- World Health Organization. Update of Recommendations on First- and Second-Line Antiretroviral Regimens. Available online: https://www.who.int/hiv/pub/arv/arv-update-2019-policy/en/ (accessed on 16 November 2020).
- Clutter, D.S.; Jordan, M.R.; Bertagnolio, S.; Shafer, R.W. HIV-1 drug resistance and resistance testing. Infect. Genet. Evol. 2016, 46, 292–307. [Google Scholar] [CrossRef] [PubMed]
- Menezes, C.N.; Maskew, M.; Sanne, I.; Crowther, N.J.; Raal, F.J. A longitudinal study of stavudine-associated toxicities in a large cohort of South African HIV infected subjects. BMC Infect. Dis. 2011, 11, 244. [Google Scholar] [CrossRef]
- Liu, P.; Liao, L.; Xu, W.; Yan, J.; Zuo, Z.; Leng, X.; Wang, J.; Kan, W.; You, Y.; Xing, H.; et al. Adherence, virological outcome, and drug resistance in Chinese HIV patients receiving first-line antiretroviral therapy from 2011 to 2015. Medicine 2018, 97, e13555. [Google Scholar] [CrossRef] [PubMed]
- Nachega, J.B.; Marconi, V.C.; van Zyl, G.U.; Gardner, E.M.; Preiser, W.; Hong, S.Y.; Mills, E.J.; Gross, R. HIV treatment adherence, drug resistance, virologic failure: Evolving concepts. Infect. Disord. Drug Targets 2011, 11, 167–174. [Google Scholar] [CrossRef]
- Goodall, R.L.; Dunn, D.T.; Nkurunziza, P.; Mugarura, L.; Pattery, T.; Munderi, P.; Kityo, C.; Gilks, C.; Kaleebu, P.; Pillay, D.; et al. Rapid accumulation of HIV-1 thymidine analogue mutations and phenotypic impact following prolonged viral failure on zidovudine-based first-line ART in sub-Saharan Africa. J. Antimicrob. Chemother. 2017, 72, 1450–1455. [Google Scholar] [CrossRef] [PubMed]
- Ndembi, N.; Murtala-Ibrahim, F.; Tola, M.; Jumare, J.; Aliyu, A.; Alabi, P.; Mensah, C.; Abimiku, A.; Quiñones-Mateu, M.E.; Crowell, T.A.; et al. Predictors of first-line antiretroviral therapy failure among adults and adolescents living with HIV/AIDS in a large prevention and treatment program in Nigeria. AIDS Res. Ther. 2020, 17, 64. [Google Scholar] [CrossRef]
- Van Laethem, K.; De Luca, A.; Antinori, A.; Cingolani, A.; Perna, C.F.; Vandamme, A.-M. A genotypic drug resistance interpretation algorithm that significantly predicts therapy response in HIV-1-infected patients. Antivir. Ther. 2002, 7, 123–129. [Google Scholar]
- Liu, T.F.; Shafer, R.W. Web resources for HIV type 1 genotypic-resistance test interpretation. Clin. Infect. Dis. 2006, 42, 1608–1618. [Google Scholar] [CrossRef]
- Vercauteren, J.; Vandamme, A.-M. Algorithms for the interpretation of HIV-1 genotypic drug resistance information. Antiviral Res. 2006, 71, 335–342. [Google Scholar] [CrossRef]
- Raposo, L.M.; Nobre, F.F. Ensemble Classifiers for Predicting HIV-1 Resistance from Three Rule-Based Genotypic Resistance Interpretation Systems. J. Med. Syst. 2017, 41, 155. [Google Scholar] [CrossRef]
- Van Laethem, K.; Vandamme, A.-M. Interpreting resistance data for HIV-1 therapy management--know the limitations. AIDS Rev. 2006, 8, 37–43. [Google Scholar]
- Vandamme, A.-M.; Camacho, R.J.; Ceccherini-Silberstein, F.; de Luca, A.; Palmisano, L.; Paraskevis, D.; Paredes, R.; Poljak, M.; Schmit, J.-C.; Soriano, V.; et al. European recommendations for the clinical use of HIV drug resistance testing: 2011 update. AIDS Rev. 2011, 13, 77–108. [Google Scholar] [PubMed]
- Hirsch, M.S.; Günthard, H.F.; Schapiro, J.M.; Brun-Vézinet, F.; Clotet, B.; Hammer, S.M.; Johnson, V.A.; Kuritzkes, D.R.; Mellors, J.W.; Pillay, D.; et al. Antiretroviral drug resistance testing in adult HIV-1 infection: 2008 recommendations of an International AIDS Society-USA panel. Clin. Infect. Dis. 2008, 47, 266–285. [Google Scholar] [CrossRef] [PubMed]
- Bennett, D.E.; Jordan, M.R.; Bertagnolio, S.; Hong, S.Y.; Ravasi, G.; McMahon, J.H.; Saadani, A.; Kelley, K.F. HIV drug resistance early warning indicators in cohorts of individuals starting antiretroviral therapy between 2004 and 2009: World Health Organization global report from 50 countries. Clin. Infect. Dis. 2012, 54 (Suppl. 4), S280–S289. [Google Scholar] [CrossRef] [PubMed]
- Somi, G.R.; Kibuka, T.; Diallo, K.; Tuhuma, T.; Bennett, D.E.; Yang, C.; Kagoma, C.; Lyamuya, E.F.; Swai, R.O.; Kassim, S. Surveillance of transmitted HIV drug resistance among women attending antenatal clinics in Dar es Salaam, Tanzania. Antivir. Ther. 2008, 13 (Suppl. 2), 77–82. [Google Scholar] [PubMed]
- Barabona, G.; Mahiti, M.; Masoud, S.; Mbelele, P.; Mgunya, A.S.; Minja, L.; Sunguya, B.; Shigemi, U.; Matsuda, M.; Hachiya, A.; et al. Pre-treatment and acquired HIV drug resistance in Dar es Salaam, Tanzania in the era of tenofovir and routine viral load monitoring. J. Antimicrob. Chemother. 2019, 74, 3016–3020. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, C.; Ulenga, N.; Liu, E.; Aboud, S.; Mugusi, F.; Chalamilla, G.; Sando, D.; Aris, E.; Carpenter, D.; Fawzi, W. HIV virological failure and drug resistance in a cohort of Tanzanian HIV-infected adults. J. Antimicrob. Chemother. 2016, 71, 1966–1974. [Google Scholar] [CrossRef] [PubMed]
- Johannessen, A.; Naman, E.; Kivuyo, S.L.; Kasubi, M.J.; Holberg-Petersen, M.; Matee, M.I.; Gundersen, S.G.; Bruun, J.N. Virological efficacy and emergence of drug resistance in adults on antiretroviral treatment in rural Tanzania. BMC Infect. Dis. 2009, 9, 108. [Google Scholar] [CrossRef]
- Sangeda, R.Z.; Mosha, F.; Prosperi, M.; Aboud, S.; Vercauteren, J.; Camacho, R.J.; Lyamuya, E.F.; Van Wijngaerden, E.; Vandamme, A.-M. Pharmacy refill adherence outperforms self-reported methods in predicting HIV therapy outcome in resource-limited settings. BMC Public Health 2014, 14, 1035. [Google Scholar] [CrossRef]
- Sangeda, R.Z.; Mosha, F.; Aboud, S.; Kamuhabwa, A.; Chalamilla, G.; Vercauteren, J.; Van Wijngaerden, E.; Lyamuya, E.; Vandamme, A.-M. Predictors of non adherence to antiretroviral therapy at an urban HIV care and treatment center in Tanzania. Drug. Healthc. Patient Saf. 2018, 10, 79–88. [Google Scholar] [CrossRef]
- Fokam, J.; Salpini, R.; Santoro, M.M.; Cento, V.; D’Arrigo, R.; Gori, C.; Perno, C.F.; Colizzi, V.; Nanfack, A.; Gwom, L.C.; et al. Performance evaluation of an in-house human immunodeficiency virus type-1 protease-reverse transcriptase genotyping assay in Cameroon. Arch. Virol. 2011, 156, 1235–1243. [Google Scholar] [CrossRef] [PubMed]
- Libin, P.; Beheydt, G.; Deforche, K.; Imbrechts, S.; Ferreira, F.; Van Laethem, K.; Theys, K.; Carvalho, A.P.P.; Cavaco-Silva, J.; Lapadula, G.; et al. RegaDB: Community-driven data management and analysis for infectious diseases. Bioinformatics 2013, 29, 1477–1480. [Google Scholar] [CrossRef] [PubMed]
- Pineda-Peña, A.A.-C.; Faria, N.R.; Imbrechts, S.; Libin, P.; Abecasis, A.B.; Deforche, K.; Gomez, A.; Camacho, R.J.; de Oliveira, T.; Vandamme, A.-M.; et al. Automated subtyping of HIV-1 genetic sequences for clinical and surveillance purposes: Performance evaluation of the new Rega version 3 and seven other tools. Infect. Genet. Evol. 2013, 29. [Google Scholar] [CrossRef]
- Bennett, D.E.; Camacho, R.J.; Otelea, D.; Kuritzkes, D.R.; Fleury, H.; Kiuchi, M.; Heneine, W.; Kantor, R.; Jordan, M.R.; Schapiro, J.M.; et al. Drug resistance mutations for surveillance of transmitted HIV-1 drug-resistance: 2009 update. PLoS ONE 2009, 4, e4724. [Google Scholar] [CrossRef] [PubMed]
- Johnson, V.A.; Calvez, V.; Gunthard, H.F.; Paredes, R.; Pillay, D.; Shafer, R.W.; Wensing, A.M.; Richman, D.D. Update of the drug resistance mutations in HIV-1: March 2013. Top. Antivir. Med. 2013, 21, 6–14. [Google Scholar]
- Wensing, A.M.; Calvez, V.; Ceccherini-Silberstein, F.; Charpentier, C.; Günthard, H.F.; Paredes, R.; Shafer, R.W.; Richman, D.D. 2019 update of the drug resistance mutations in HIV-1. Top. Antivir. Med. 2019, 27, 111–121. [Google Scholar]
- R Development Core Team. R: A Language and Environment for Statistical Computing. 2020. [Google Scholar]
- EACS European AIDS Clinical Society Guidelines Version10.0—November 2019. Available online: http://www.europeanaidsclinicalsociety.org/ (accessed on 12 April 2021).
- Arroyo, M.A.; Hoelscher, M.; Sanders-Buell, E.; Herbinger, K.-H.; Samky, E.; Maboko, L.; Hoffmann, O.; Robb, M.R.; Birx, D.L.; McCutchan, F.E. HIV type 1 subtypes among blood donors in the Mbeya region of southwest Tanzania. AIDS Res. Hum. Retroviruses 2004, 20, 895–901. [Google Scholar] [CrossRef]
- Arroyo, M.A.; Hoelscher, M.; Sateren, W.; Samky, E.; Maboko, L.; Hoffmann, O.; Kijak, G.; Robb, M.; Birx, D.L.; McCutchan, F.E. HIV-1 diversity and prevalence differ between urban and rural areas in the Mbeya region of Tanzania. AIDS 2005, 19, 1517–1524. [Google Scholar] [CrossRef]
- Kiwelu, I.E.; Renjifo, B.; Chaplin, B.; Sam, N.; Nkya, W.M.; Shao, J.; Kapiga, S.; Essex, M. HIV type 1 subtypes among bar and hotel workers in Moshi, Tanzania. AIDS Res. Hum. Retrovir. 2003, 19, 57–64. [Google Scholar] [CrossRef]
- Hoelscher, M.; Kim, B.; Maboko, L.; Mhalu, F.; von Sonnenburg, F.; Birx, D.L.; McCutchan, F.E. High proportion of unrelated HIV-1 intersubtype recombinants in the Mbeya region of southwest Tanzania. AIDS 2001, 15, 1461–1470. [Google Scholar] [CrossRef]
- Mosha, F.; Urassa, W.; Aboud, S.; Lyamuya, E.F.; Sandstrom, E.; Bredell, H.; Williamson, C. Prevalence of genotypic resistance to antiretroviral drugs in treatment-naive youths infected with diverse HIV type 1 subtypes and recombinant forms in Dar es Salaam, Tanzania. AIDS Res. Hum. Retrovir. 2011, 27, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Nyombi, B.M.; Nkya, W.M.; Barongo, L.; Bjune, G.; Kristiansen, K.I.; Müller, F.; Holm-Hansen, C. Evolution of human immunodeficiency virus type 1 serotypes in northern Tanzania: A retrospective study. APMIS 2008, 116, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Nyombi, B.M.; Kristiansen, K.I.; Bjune, G.; Müller, F.; Holm-Hansen, C. Diversity of human immunodeficiency virus type 1 subtypes in Kagera and Kilimanjaro regions, Tanzania. AIDS Res. Hum. Retrovir. 2008, 24, 761–769. [Google Scholar] [CrossRef]
- Nyombi, B.M.; Holm-Hansen, C.; Kristiansen, K.I.; Bjune, G.; Müller, F. Prevalence of reverse transcriptase and protease mutations associated with antiretroviral drug resistance among drug-naïve HIV-1 infected pregnant women in Kagera and Kilimanjaro regions, Tanzania. AIDS Res. Ther. 2008, 5, 13. [Google Scholar] [CrossRef]
- Bertagnolio, S.; Kelley, K.; Hassani, A.; Obeng-Aduasare, Y.; Jordan, M.R. Surveillance of Transmitted and Acquired HIV Drug Resistance Using WHO Surveys in Resource-limited Settings. In Proceedings of the 18th Conference on Retroviruses and Opportunistic Infections, Boston, MA, USA, 27 Feburary–2 March 2011. [Google Scholar]
- Cozzi-Lepri, A.; Ruiz, L.; Loveday, C.; Phillips, A.N.; Clotet, B.; Reiss, P.; Ledergerber, B.; Holkmann, C.; Staszewski, S.; Lundgren, J.D. Thymidine analogue mutation profiles: Factors associated with acquiring specific profiles and their impact on the virological response to therapy. Antivir. Ther. 2005, 10, 791–802. [Google Scholar] [PubMed]
- Shafer, R.W.; Schapiro, J.M. HIV-1 drug resistance mutations: An updated framework for the second decade of HAART. AIDS Rev. 2008, 10, 67–84. [Google Scholar]
- Kasang, C.; Kalluvya, S.; Majinge, C.; Stich, A.; Bodem, J.; Kongola, G.; Jacobs, G.B.; Mlewa, M.; Mildner, M.; Hensel, I.; et al. HIV drug resistance (HIVDR) in antiretroviral therapy-naïve patients in Tanzania not eligible for WHO threshold HIVDR survey is dramatically high. PLoS ONE 2011, 6, e23091. [Google Scholar] [CrossRef] [PubMed]
- Lambert-Niclot, S.; Charpentier, C.; Storto, A.; Fofana, D.B.; Soulié, C.; Fourati, S.; Visseaux, B.; Wirden, M.; Morand-Joubert, L.; Masquelier, B.; et al. Prevalence of pre-existing resistance-associated mutations to rilpivirine, emtricitabine and tenofovir in antiretroviral-naive patients infected with B and non-B subtype HIV-1 viruses. J. Antimicrob. Chemother. 2013, 68, 1237–1242. [Google Scholar] [CrossRef] [PubMed]
- Sluis-Cremer, N.; Jordan, M.R.; Huber, K.; Wallis, C.L.; Bertagnolio, S.; Mellors, J.W.; Parkin, N.T.; Richard Harrigan, P. E138A in HIV-1 reverse transcriptase is more common in subtype C than B: Implications for rilpivirine use in resource-limited settings. Antiviral Res. 2014, 107, 31–34. [Google Scholar] [CrossRef]
- Barth, R.E.; van der Loeff, M.F.S.; Schuurman, R.; Hoepelman, A.I.; Wensing, A.M. Virological follow-up of adult patients in antiretroviral treatment programmes in sub-Saharan Africa: A systematic review. Lancet Infect. Dis. 2010, 10, 155–166. [Google Scholar] [CrossRef]
- UNAIDS Fast-Track: Ending the AIDS Epidemic by 2030. Available online: http://www.unaids.org/sites/default/files/media_asset/JC2686_WAD2014report_en.pdf (accessed on 12 April 2021).
- Wainberg, M.A.; Brenner, B.G. The Impact of HIV Genetic Polymorphisms and Subtype Differences on the Occurrence of Resistance to Antiretroviral Drugs. Mol. Biol. Int. 2012, 2012, 256982. [Google Scholar] [CrossRef]
- Camacho, R.J.; Vandamme, A.-M. Antiretroviral resistance in different HIV-1 subtypes: Impact on therapy outcomes and resistance testing interpretation. Curr. Opin. HIV AIDS 2007, 2, 123–129. [Google Scholar] [CrossRef]
- Theys, K.; Vercauteren, J.; Snoeck, J.; Zazzi, M.; Camacho, R.J.; Torti, C.; Schülter, E.; Clotet, B.; Sönnerborg, A.; De Luca, A.; et al. HIV-1 subtype is an independent predictor of reverse transcriptase mutation K65R in HIV-1 patients treated with combination antiretroviral therapy including tenofovir. Antimicrob. Agents Chemother. 2013, 57, 1053–1056. [Google Scholar] [CrossRef] [PubMed]
- Abecasis, A.B.; Deforche, K.; Snoeck, J.; Bacheler, L.T.; McKenna, P.; Carvalho, A.P.; Gomes, P.; Camacho, R.J.; Vandamme, A.-M. Protease mutation M89I/V is linked to therapy failure in patients infected with the HIV-1 non-B subtypes C, F or G. AIDS 2005, 19, 1799–1806. [Google Scholar] [CrossRef]
- Abecasis, A.B.; Deforche, K.; Bacheler, L.T.; McKenna, P.; Carvalho, A.P.; Gomes, P.; Vandamme, A.-M.; Camacho, R.J. Investigation of baseline susceptibility to protease inhibitors in HIV-1 subtypes C, F, G and CRF02_AG. Antivir. Ther. 2006, 11, 581–589. [Google Scholar] [PubMed]
- Ministry of Health Community Development Gender Elderly and Children National Guidelines for the Management of HIV and AIDS in Tanzania. Available online: https://www.differentiatedservicedelivery.org/Portals/0/adam/Content/NqQGryocrU2RTj58iR37uA/File/NATIONAL_GUIDELINES_FOR_THE_MANAGEMENT_OF_HIV_AND_AIDS_2019.pdf (accessed on 18 October 2021).
- Lemey, P.; Derdelinckx, I.; Rambaut, A.; Van Laethem, K.; Dumont, S.; Vermeulen, S.; Van Wijngaerden, E.; Vandamme, A.-M. Molecular footprint of drug-selective pressure in a human immunodeficiency virus transmission chain. J. Virol. 2005, 79, 11981–11989. [Google Scholar] [CrossRef] [PubMed][Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient # | Sequence ID | Age at Study Entry | Gender | Subtype † | Pharmacy Refill Adherence (%) | Therapy * (in Addition to AZT+3TC) | Log VL at Study Baseline | Log VL at one Year | NNRTI Resistance-Related Polymorphisms | PI Resistance-Related Polymorphisms |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | N001 | 29 | F | CRF 10_CD | NA | EFV | 4.74 | NA | None | 36I, 63P |
| 2 | N002 | 32 | F | A | 100 | EFV | 5.94 | ≤2.60 | None | 10I, 36I, 69K, 89M |
| 3 | N003 | 26 | F | A | 100 | EFV | 5.81 | NA | 138A | 36I, 62V, 69K, 89M |
| 4 | N004 | 35 | M | A | 77.1 | EFV | 5.06 | NA | 138A | 20I, 36I, 64M, 69K, 89M |
| 5 | N006 | 35 | F | A | 95.84 | NVP | 5.12 | ≤2.60 | 44D | 36I, 69K, 89M |
| 6 | N007 | 35 | M | URF | 100 | NVP | 3.31 | NA | None | 36I, 69K, 89M |
| 7 | N008 | 30 | F | A | 93.29 | NVP | 4.79 | 4.72 | None | 10I, 16E, 36I, 69K, 77I, 89M |
| 8 | N010 | 34 | F | A | 81.02 | EFV | 4.32 | ≤2.60 | None | |
| 9 | N011 | 42 | M | D | 91.47 | EFV | 6.00 | ≤2.60 | None | 10V, 63P, 64V |
| 10 | N012 | 38 | F | URF | 93.38 | EFV | 5.74 | ≤2.60 | None | 64V |
| 11 | N013 | 54 | M | D | 100 | EFV | 4.23 | NA | None | 64M, 77I |
| 12 | N015 | 55 | M | A | 97.39 | NVP | 5.47 | ≤2.60 | None | 11I, 36I, 63P, 69K, 89M/I |
| 13 | N016 | 52 | M | C | 92.57 | EFV | 5.65 | ≤2.60 | None | 36I, 89M, 93L |
| 14 | N017 | 32 | M | C | 100 | EFV | 4.93 | ≤2.60 | None | 36I, 69K, 89M, 93L |
| 15 | N018 | 33 | F | D | 100 | EFV | 5.05 | ≤2.60 | None | 64V, 77I |
| 16 | N019 | 32 | M | C | 48.19 | EFV | 5.56 | NA | None | 16E, 36I, 69K, 89M, 93L |
| 17 | N020 | 56 | F | A | 70.45 | EFV | 5.58 | NA | None | 20R, 36I, 64L, 69K, 89M |
| 18 | N022 | 31 | F | A | 84.87 | EFV | 5.16 | ≤2.60 | None | 10I, 11I, 36I, 63P, 69K, 89M |
| Detectable Viral Load | ||||||
|---|---|---|---|---|---|---|
| At Study Entry | At One Year Follow-Up | |||||
| Time of Therapy Initiation | Number of Patients | Duration of Therapy at Study Entry Median Months (IQR) | N (%) | Log VL Median (IQR) | N (%) | Log VL Median (IQR) |
| At study entry | 14 | 0 | 14 (100%) | 5.1 (4.9–5.6) | 2 (14.3%) | 4.4 (4.1–4.6) |
| Before study entry | 148 | 25 (18–36) | 18 (12.2%) | 4.4 (3.5–4.7) | 53 (35.8%) | 3.9 (2.9–4.8) |
| NRTI Mutations | N | % | NNRTI Mutations | N | % | PI Polymorphisms | N | % |
|---|---|---|---|---|---|---|---|---|
| 184V | 17 | 70.8 | 103N | 8 | 33.3 | 36I | 20 | 83.3 |
| 67N | 7 | 29.2 | 181C | 7 | 29.2 | 69K | 19 | 79.2 |
| 70R | 6 | 25.0 | 190A | 5 | 20.8 | 89M | 15 | 62.5 |
| 215F | 5 | 20.8 | 108I | 3 | 12.5 | 20R | 10 | 41.7 |
| 219E | 3 | 12.5 | 138Q | 2 | 8.3 | 16E | 8 | 33.3 |
| 219Q | 2 | 8.3 | 221Y | 2 | 8.3 | 93L | 7 | 29.2 |
| 215Y | 2 | 8.3 | 118I | 1 | 4.2 | 63P | 5 | 20.8 |
| 41L | 2 | 8.3 | 138A | 1 | 4.2 | 64V | 4 | 16.7 |
| 75I | 2 | 8.3 | 179L | 1 | 4.2 | 10V | 2 | 8.3 |
| 151M | 1 | 4.2 | 181I | 1 | 4.2 | 10I | 1 | 4.2 |
| 116Y | 1 | 4.2 | 181V | 1 | 4.2 | 36L | 1 | 4.2 |
| 210W | 1 | 4.2 | 225H | 1 | 4.2 | 62V | 1 | 4.2 |
| 64L | 1 | 4.2 | ||||||
| 89I | 1 | 4.2 |
| GSS of Regimen | GSS of Potential Second-Line | ||||||
|---|---|---|---|---|---|---|---|
| Patient # | Sequence ID | Resistance to NRTIs | Intermediate Resistance to NRTIs | Resistance to NNRTIs | At Sampling | ABC + FTC + LPV/r | TDF + FTC + LPV/r |
| 19 | F001 | None | none | none | 3 | 3.5 | 3.5 |
| 20 | W0141 | None | none | none | 3 | 3.5 | 3.5 |
| 21 | W0067 | None | none | none | 3 | 3.5 | 3.5 |
| 22 | F110 | None | AZT, D4T | none | 3 | 3.5 | 3.5 |
| 23 | F189 | None | none | EFV, NVP | 2 | 3.5 | 3.5 |
| 24 | F134 | None | none | EFV, NVP | 2 | 3.5 | 3.5 |
| 25 | F141 | None | none | EFV, NVP | 2 | 3.5 | 3.5 |
| 26 | F144 | 3TC, FTC | none | EFV, NVP | 1 | 2.5 | 2.5 |
| 27 | F176 | 3TC, FTC | none | EFV, NVP | 1 | 2.5 | 2.5 |
| 27 | W0037 | 3TC, AZT, D4T, FTC | ABC | EFV, NVP | 0 | 2 | 2.5 |
| 27 | W0116 | 3TC, ABC, AZT, D4T, FTC | TDF | EFV, NVP | 0 | 1.5 | 2 |
| 28 | W0065 | 3TC, FTC | none | EFV, NVP | 1 | 2.5 | 2.5 |
| 29 | W0021 | 3TC, FTC | none | EFV, NVP | 1 | 2.5 | 2.5 |
| 30 | F064 | 3TC, FTC | none | EFV, NVP | 1 | 2.5 | 2.5 |
| 31 | W0079 | 3TC, FTC | none | EFV, NVP | 1 | 2.5 | 2.5 |
| 32 | W0127 | 3TC, FTC | none | EFV, NVP | 1 | 2.5 | 2.5 |
| 33 | W0019 | 3TC, FTC | none | EFV, NVP | 1 | 2.5 | 2.5 |
| 34 | W0066 | 3TC, FTC | none | EFV, NVP | 1 | 2.5 | 2.5 |
| 35 | F003 | 3TC, FTC | ABC, AZT, D4T | EFV, NVP | 0.5 | 2 | 2.5 |
| 35 | W0108 | 3TC, ABC, AZT, D4T, FTC | TDF | EFV, NVP | 0 | 1.5 | 2 |
| 36 | W0158 | 3TC, ABC, AZT, D4T, FTC | TDF | EFV, NVP | 0 | 1.5 | 2 |
| 37 | F068 | 3TC, FTC | ABC, AZT, D4T | EFV, NVP | 0.5 | 2 | 2.5 |
| 38 | W0120 | 3TC, FTC | ABC, AZT, D4T | EFV, NVP | 0.5 | 2 | 2.5 |
| 39 | W0054 | 3TC, ABC, AZT, D4T, FTC | none | EFV, NVP | 0 | 1.5 | 2.5 |
| 40 | W0062 | 3TC, D4T, FTC | ABC, AZT | EFV, NVP | 1 | 2 | 2.5 |
| 41 | F183 | 3TC, AZT, FTC | ABC, D4T | EFV, NVP | 0.5 | 2 | 2.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sangeda, R.Z.; Gómes, P.; Rhee, S.-Y.; Mosha, F.; Camacho, R.J.; Van Wijngaerden, E.; Lyamuya, E.F.; Vandamme, A.-M. Development of HIV Drug Resistance in a Cohort of Adults on First-Line Antiretroviral Therapy in Tanzania during the Stavudine Era. Microbiol. Res. 2021, 12, 847-861. https://doi.org/10.3390/microbiolres12040062
Sangeda RZ, Gómes P, Rhee S-Y, Mosha F, Camacho RJ, Van Wijngaerden E, Lyamuya EF, Vandamme A-M. Development of HIV Drug Resistance in a Cohort of Adults on First-Line Antiretroviral Therapy in Tanzania during the Stavudine Era. Microbiology Research. 2021; 12(4):847-861. https://doi.org/10.3390/microbiolres12040062
Chicago/Turabian StyleSangeda, Raphael Z., Perpétua Gómes, Soo-Yon Rhee, Fausta Mosha, Ricardo J. Camacho, Eric Van Wijngaerden, Eligius F. Lyamuya, and Anne-Mieke Vandamme. 2021. "Development of HIV Drug Resistance in a Cohort of Adults on First-Line Antiretroviral Therapy in Tanzania during the Stavudine Era" Microbiology Research 12, no. 4: 847-861. https://doi.org/10.3390/microbiolres12040062
APA StyleSangeda, R. Z., Gómes, P., Rhee, S.-Y., Mosha, F., Camacho, R. J., Van Wijngaerden, E., Lyamuya, E. F., & Vandamme, A.-M. (2021). Development of HIV Drug Resistance in a Cohort of Adults on First-Line Antiretroviral Therapy in Tanzania during the Stavudine Era. Microbiology Research, 12(4), 847-861. https://doi.org/10.3390/microbiolres12040062