
Assessment of Long-Term Changes in Knowledge and Attitudes of Household Contacts of COVID-19 Cases in Northern Spain

 , , , , ,
, , , , ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Questionnaire
2.3. Statistical Analyses
2.4. Ethical Considerations
3. Results
3.1. Characteristics of Participants
3.2. Long-Term Changes in Knowledge towards COVID-19 and Its Preventive Measures
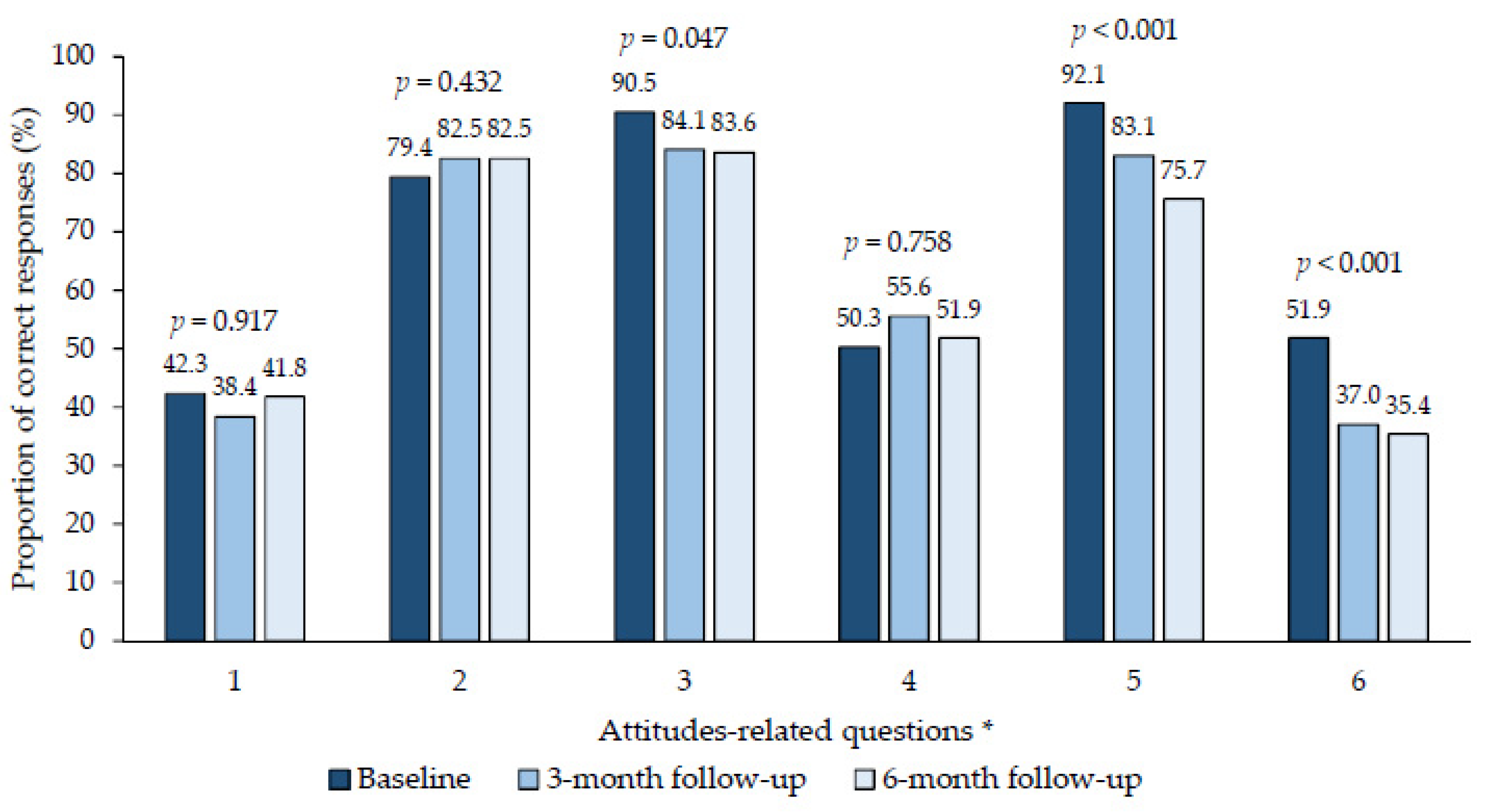
3.3. Long-Term Changes in Attitudes towards COVID-19 and Its Preventive Measures
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Munster, V.J.; Koopmans, M.; van Doremalen, N.; van Riel, D.; de Wit, E. A novel coronavirus emerging in China—Key questions for impact assessment. N. Engl. J. Med. 2020, 382, 692–694. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.C.; Shih, T.P.; Ko, W.C.; Tang, H.J.; Hsueh, P.R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges. Int. J. Antimicrob. Agents 2020, 55, 105924. [Google Scholar] [CrossRef] [PubMed]
- Kaur, S.; Bherwani, H.; Gulia, S.; Vijay, R.; Kumar, R. Understanding COVID-19 transmission, health impacts and mitigation: Timely social distancing is the key. Environ. Dev. Sustain. 2021, 23, 6681–6697. [Google Scholar] [CrossRef]
- Liu, Y.; Morgenstern, C.; Kelly, J.; Lowe, R. CMMID COVID-19 Working Group; Jit, M. The impact of non-pharmaceutical interventions on SARS-CoV-2 transmission across 130 countries and territories. BMC Med. 2021, 19, 40. [Google Scholar] [CrossRef] [PubMed]
- Falcón-Romero, M.; Rodriguez-Blázquez, C.; Romay-Barja, M.; Forjaz, M.J. Evolución de las preocupaciones, percepciones y actitudes de la población española ante la pandemia de COVID-19. Rev. Esp. Sociol. 2023, 32, a162. [Google Scholar] [CrossRef]
- Martínez-Baz, I.; Miqueleiz, A.; Egüés, N.; Casado, I.; Burgui, C.; Echeverría, A.; Navascués, A.; Fernández-Huerta, M.; García Cenoz, M.; Trobajo-Sanmartín, C.; et al. Effect of COVID-19 vaccination on the SARS-CoV-2 transmission among social and household close contacts: A cohort study. J. Infect. Public Health 2023, 16, 410–417. [Google Scholar] [CrossRef]
- Barbeito, I.; Precioso, D.; Sierra, M.J.; Vegas-Azcárate, S.; Fernández Balbuena, S.; Vitoriano, B.; Goméz-Ullate, D.; Cao, R.; Monge, S. Study Group for Non-Pharmaceutical Interventions in Spain. Effectiveness of non-pharmaceutical interventions in nine fields of activity to decrease SARS-CoV-2 transmission (Spain, September 2020–May 2021). Front. Public Health 2023, 11, 1061331. [Google Scholar] [CrossRef]
- Rodríguez-Blázquez, C.; Romay-Barja, M.; Falcón, M.; Ayala, A.; Forjaz, M.J. The COSMO-Spain survey: Three first rounds of the WHO behavioral insights tool. Front. Public Health 2021, 9, 678926. [Google Scholar] [CrossRef] [PubMed]
- Betsch, C.; Wieler, L.H.; Habersaat, K.; COSMO Group. Monitoring behavioural insights related to COVID-19. Lancet 2020, 395, 1255–1256. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Baz, I.; Bullón-Vela, V.; Soldevila, N.; Torner, N.; Palma, D.; García Cenoz, M.; Pérez, G.; Burgui, C.; Castilla, J.; Godoy, P.; et al. Assessment of knowledge and attitudes over time in postacute COVID-19 environments: Protocol for an epidemiological study. JMIR Res. Protoc. 2023, 12, e52114. [Google Scholar] [CrossRef] [PubMed]
- Bullón-Vela, V.; Toledo, D.; Echeverría, A.; Godoy, P.; Cenoz, M.G.; Parrón, I.; Castilla, J.; Domínguez, A.; Martínez-Baz, I. Absence of short-term changes in knowledge and attitudes among household contacts of COVID-19 cases during the post-acute phase of the pandemic in Catalonia and Navarre, Spain. Front. Public Health 2024, 12, 1306284. [Google Scholar] [CrossRef] [PubMed]
- Instituto de Salud Carlos III. Monitorización del Comportamiento y las Actitudes de la Población Relacionadas con la COVID-19 en España (COSMO-SPAIN): Estudio OMS. Available online: https://portalcne.isciii.es/cosmo-spain/ (accessed on 1 July 2024).
- Orden SND/726/2023, de 4 de Julio, por la que se publica el Acuerdo del Consejo de Ministros de 4 de Julio de 2023, por el que se declara la finalización de la situación de crisis sanitaria ocasionada por la COVID-19. Available online: https://www.boe.es/boe/dias/2023/07/05/pdfs/BOE-A-2023-15552.pdf (accessed on 27 June 2024).
- Siddiquea, B.N.; Shetty, A.; Bhattacharya, O.; Afroz, A.; Billah, B. Global epidemiology of COVID-19 knowledge, attitude and practice: A systematic review and meta-analysis. BMJ Open 2021, 11, e051447. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.M.; Marzo, R.R.; Chowdhury, S.; Qalati, S.A.; Hasan, M.N.; Paul, G.K.; Abid, K.; Sheferaw, W.E.; Mariadass, A.; Chandran, D.; et al. Knowledge, attitude and practices toward coronavirus disease (COVID-19) in Southeast and South Asia: A mixed study design approach. Front. Public Health 2022, 10, 875727. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.M.; Mann, S.K.; Negi, A. KAP (Knowledge, Attitude and Practices) analysis during two consecutive waves of COVID-19 in India. GJSFR 2022, 22, 1–7. Available online: https://journalofscience.org/index.php/GJSFR/article/view/101893 (accessed on 15 July 2024).
- World Health Organization (WHO). Pandemic fatigue: Reinvigorating the public to prevent COVID-19: Policy framework for supporting pandemic prevention and management: Revised version November 2020. Copenhagen: WHO Regional Office for Europe. 2020. Available online: https://apps.who.int/iris/bitstream/handle/10665/335820/WHO-EURO-2020-1160-40906-55390-eng.pdf?sequence=3&isAllowed=y (accessed on 1 July 2024).
- Agurto-Ramírez, A.; Pino-Rosón, C.; Ayala, A.; Falcón, M.; Rodríguez-Blázquez, C.; Forjaz, M.J.; Romay-Barja, M. Association between pandemic fatigue and disease knowledge, attitudes, concerns, and vaccination intention at two key moments of the COVID-19 pandemic. Int. J. Public Health 2023, 68, 1606049. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Questions and Values | Age Group | Educational Level | High-Risk Conditions | Previous Infection | ||||
|---|---|---|---|---|---|---|---|---|
| <60 Yrs | ≥60 Yrs | Primary/Secondary | Higher | Yes | No | Yes | No | |
| All people who become ill with COVID-19 will develop into a severe case | ||||||||
| Baseline, % | 79.8 | 72.9 | 68.7 | 86.7 | 72.8 | 84.0 | 78.2 | 76.1 |
| 3-month follow-up, % | 86.2 | 58.0 | 67.0 | 85.2 | 71.1 | 83.1 | 78.0 | 72.9 |
| 6-month follow-up, % | 84.0 | 68.6 | 67.7 | 90.0 | 74.6 | 84.0 | 81.2 | 75.0 |
| AD, % * | 4.2 | −4.3 | −1.0 | 3.3 | 1.8 | 0.0 | 3.0 | −1.1 |
| p-value | 0.400 | 0.577 | 0.879 | 0.486 | 0.764 | 1.000 | 0.600 | 0.861 |
| Asymptomatic persons diagnosed with COVID-19 can transmit the infection | ||||||||
| Baseline, % | 89.1 | 77.1 | 77.8 | 92.2 | 83.3 | 86.7 | 84.2 | 85.2 |
| 3-month follow-up, % | 83.6 | 79.7 | 79.4 | 85.2 | 83.3 | 80.3 | 84.0 | 80.0 |
| 6-month follow-up, % | 86.6 | 80.0 | 78.8 | 90.0 | 86.0 | 81.3 | 84.2 | 84.1 |
| AD, % * | −2.5 | 2.9 | 1.0 | −2.2 | 2.7 | −5.4 | 0.0 | −1.1 |
| p-value | 0.552 | 0.680 | 0.863 | 0.600 | 0.582 | 0.373 | 1.000 | 0.834 |
| Persons diagnosed with COVID-19 can transmit infection despite vaccination | ||||||||
| Baseline, % | 91.6 | 85.7 | 82.8 | 96.7 | 89.5 | 89.3 | 92.1 | 86.4 |
| 3-month follow-up, % | 89.7 | 81.2 | 83.5 | 89.8 | 84.2 | 90.1 | 84.0 | 89.4 |
| 6-month follow-up, % | 93.3 | 77.1 | 77.8 | 97.8 | 86.0 | 89.3 | 90.1 | 84.1 |
| AD, % * | 1.7 | −8.6 | −5.0 | 1.1 | −3.5 | 0.0 | −2.0 | −2.3 |
| p-value | 0.624 | 0.193 | 0.372 | 0.650 | 0.420 | 1.000 | 0.621 | 0.671 |
| The SARS-CoV-2 virus is spread by respiratory droplets from infected individuals when coughing/sneezing/talking/laughing/singing | ||||||||
| Baseline, % | 92.4 | 88.6 | 89.9 | 92.2 | 91.2 | 90.7 | 91.1 | 90.9 |
| 3-month follow-up, % | 91.4 | 89.9 | 86.6 | 95.5 | 91.2 | 90.1 | 95.0 | 85.9 |
| 6-month follow-up, % | 95.0 | 94.3 | 92.9 | 96.7 | 93.9 | 96.0 | 96.0 | 93.2 |
| AD, % * | 2.6 | 5.7 | 3.0 | 4.5 | 2.7 | 5.3 | 4.9 | 2.3 |
| p-value | 0.424 | 0.228 | 0.447 | 0.193 | 0.449 | 0.191 | 0.152 | 0.577 |
| Handwashing is important in reducing the risk of contracting COVID-19 | ||||||||
| Baseline, % | 91.6 | 91.4 | 92.9 | 90.0 | 93.9 | 88.0 | 90.1 | 93.2 |
| 3-month follow-up, % | 90.5 | 92.8 | 92.8 | 89.8 | 91.2 | 91.5 | 90.0 | 92.9 |
| 6-month follow-up, % | 92.4 | 87.1 | 90.9 | 90.0 | 89.5 | 92.0 | 89.1 | 92.0 |
| AD, % * | 0.8 | −4.3 | −2.0 | 0.0 | −4.4 | 4.0 | −1.0 | −1.2 |
| p-value | 0.811 | 0.412 | 0.602 | 1.000 | 0.231 | 0.414 | 0.818 | 0.773 |
| To prevent transmission of COVID-19, measures such as wearing face masks and avoiding crowds in enclosed spaces should be maintained | ||||||||
| Baseline, % | 89.1 | 97.1 | 92.9 | 91.1 | 94.7 | 88.0 | 93.1 | 90.9 |
| 3-month follow-up, % | 86.2 | 87.0 | 87.6 | 85.2 | 87.7 | 84.5 | 88.0 | 84.7 |
| 6-month follow-up, % | 89.1 | 82.9 | 84.8 | 88.9 | 87.7 | 85.3 | 84.2 | 89.8 |
| AD, % * | 0.0 | −14.2 | −8.1 | −2.2 | −7.0 | −2.7 | −8.9 | −1.1 |
| p-value | 1.000 | 0.005 | 0.070 | 0.619 | 0.061 | 0.631 | 0.046 | 0.779 |
| Questions and Values | Age Group | Educational Level | High-Risk Conditions | Previous Infection | ||||
|---|---|---|---|---|---|---|---|---|
| <60 yrs | ≥60 yrs | Primary/Secondary | Higher | Yes | No | Yes | No | |
| I consider myself susceptible to developing severe disease if I become ill with COVID-19 | ||||||||
| Baseline, % | 42.0 | 42.9 | 40.4 | 44.4 | 21.9 | 73.3 | 37.6 | 47.7 |
| 3-month follow-up, % | 44.8 | 27.5 | 34.0 | 43.2 | 15.8 | 74.6 | 37.0 | 40.0 |
| 6-month follow-up, % | 47.1 | 32.9 | 41.4 | 42.2 | 19.3 | 76.0 | 39.6 | 44.3 |
| AD, % * | 5.1 | −10.0 | 1.0 | −2.2 | −2.6 | 2.7 | 2.0 | −3.4 |
| p-value | 0.434 | 0.223 | 0.885 | 0.764 | 0.623 | 0.707 | 0.773 | 0.650 |
| I consider that my inner circle has complied with the preventive measures to avoid becoming ill with COVID-19 | ||||||||
| Baseline, % | 76.5 | 84.3 | 90.9 | 66.7 | 78.9 | 80.0 | 74.3 | 85.2 |
| 3-month follow-up, % | 80.2 | 91.3 | 92.8 | 75.0 | 86.0 | 81.7 | 80.0 | 89.4 |
| 6-month follow-up, % | 76.5 | 92.9 | 93.9 | 70.0 | 84.2 | 80.0 | 76.2 | 89.8 |
| AD, % * | 0.0 | 8.6 | 3.0 | 3.3 | 5.3 | 0.0 | 1.9 | 4.6 |
| p-value | 1.000 | 0.111 | 0.420 | 0.631 | 0.307 | 1.000 | 0.744 | 0.362 |
| I consider that my inner circle has complied with the vaccination recommendations given by the health authorities | ||||||||
| Baseline, % | 88.2 | 94.3 | 92.9 | 87.8 | 90.4 | 90.7 | 89.1 | 92.0 |
| 3-month follow-up, % | 84.5 | 88.4 | 89.7 | 81.8 | 83.3 | 90.1 | 86.0 | 85.9 |
| 6-month follow-up, % | 79.8 | 90.0 | 91.9 | 74.4 | 83.3 | 84.0 | 80.2 | 87.5 |
| AD, % * | −8.4 | −4.3 | −1.0 | −13.4 | −7.1 | −6.7 | −8.9 | −4.5 |
| p-value | 0.077 | 0.346 | 0.788 | 0.022 | 0.117 | 0.220 | 0.079 | 0.320 |
| I consider that it is better to develop immunity by getting sick with COVID-19 than by being vaccinated | ||||||||
| Baseline, % | 45.4 | 58.6 | 54.5 | 45.6 | 50.9 | 49.3 | 48.5 | 52.3 |
| 3-month follow-up, % | 51.7 | 65.2 | 62.9 | 50.0 | 61.4 | 49.3 | 55.0 | 58.8 |
| 6-month follow-up, % | 52.9 | 50.0 | 53.5 | 50.0 | 50.0 | 54.7 | 50.5 | 53.4 |
| AD, % * | 7.5 | −8.6 | −1.0 | 4.4 | −0.9 | 5.4 | 2.0 | 1.1 |
| p-value | 0.244 | 0.311 | 0.887 | 0.551 | 0.895 | 0.513 | 0.778 | 0.880 |
| It is convenient for the general population to wear a face mask correctly (covering the nose and mouth) to prevent COVID-19 in crowded closed environments | ||||||||
| Baseline, % | 92.4 | 91.4 | 92.9 | 91.1 | 93.0 | 90.7 | 90.1 | 94.3 |
| 3-month follow-up, % | 87.9 | 79.7 | 86.6 | 83.0 | 85.1 | 84.5 | 85.0 | 84.7 |
| 6-month follow-up, % | 75.6 | 75.7 | 78.8 | 72.2 | 74.6 | 77.3 | 70.3 | 81.8 |
| AD, % * | −16.8 | −15.7 | −14.1 | −18.9 | −18.4 | −13.4 | −19.8 | −12.5 |
| p-value | <0.001 | 0.012 | 0.004 | 0.001 | <0.001 | 0.026 | <0.001 | 0.011 |
| I consider that COVID-19 had a negative influence on my daily life | ||||||||
| Baseline, % | 51.3 | 52.9 | 49.5 | 54.4 | 54.4 | 48.0 | 44.6 | 60.2 |
| 3-month follow-up, % | 33.6 | 44.9 | 46.4 | 28.4 | 45.6 | 25.4 | 28.0 | 49.4 |
| 6-month follow-up, % | 31.9 | 41.4 | 39.4 | 31.1 | 40.4 | 28.0 | 32.7 | 38.6 |
| AD, % * | −19.4 | −11.5 | −10.1 | −23.3 | −14.0 | −20.0 | −11.9 | −21.6 |
| p-value | 0.002 | 0.176 | 0.153 | 0.002 | 0.034 | 0.012 | 0.083 | 0.004 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vera-Punzano, N.; Bullón-Vela, V.; Miret, C.; Pardos-Plaza, J.; García Cenoz, M.; Godoy, P.; Castilla, J.; Domínguez, À.; Toledo, D.; Martínez-Baz, I. Assessment of Long-Term Changes in Knowledge and Attitudes of Household Contacts of COVID-19 Cases in Northern Spain. Infect. Dis. Rep. 2024, 16, 923-931. https://doi.org/10.3390/idr16050074
Vera-Punzano N, Bullón-Vela V, Miret C, Pardos-Plaza J, García Cenoz M, Godoy P, Castilla J, Domínguez À, Toledo D, Martínez-Baz I. Assessment of Long-Term Changes in Knowledge and Attitudes of Household Contacts of COVID-19 Cases in Northern Spain. Infectious Disease Reports. 2024; 16(5):923-931. https://doi.org/10.3390/idr16050074
Chicago/Turabian StyleVera-Punzano, Noelia, Vanessa Bullón-Vela, Carme Miret, Jéssica Pardos-Plaza, Manuel García Cenoz, Pere Godoy, Jesús Castilla, Àngela Domínguez, Diana Toledo, and Iván Martínez-Baz. 2024. "Assessment of Long-Term Changes in Knowledge and Attitudes of Household Contacts of COVID-19 Cases in Northern Spain" Infectious Disease Reports 16, no. 5: 923-931. https://doi.org/10.3390/idr16050074
APA StyleVera-Punzano, N., Bullón-Vela, V., Miret, C., Pardos-Plaza, J., García Cenoz, M., Godoy, P., Castilla, J., Domínguez, À., Toledo, D., & Martínez-Baz, I. (2024). Assessment of Long-Term Changes in Knowledge and Attitudes of Household Contacts of COVID-19 Cases in Northern Spain. Infectious Disease Reports, 16(5), 923-931. https://doi.org/10.3390/idr16050074