
Adverse Outcomes of Patients with Non-Ventilator-Associated Hospital-Acquired Pneumonia (nvHAP)—A Single Centre Cohort Study


Abstract
1. Introduction
2. Methods
2.1. Study Design, Setting and Patient Population
2.2. Adverse Outcomes and Potential Risk Factors for Adverse Outcome
2.3. Data Analysis
3. Results
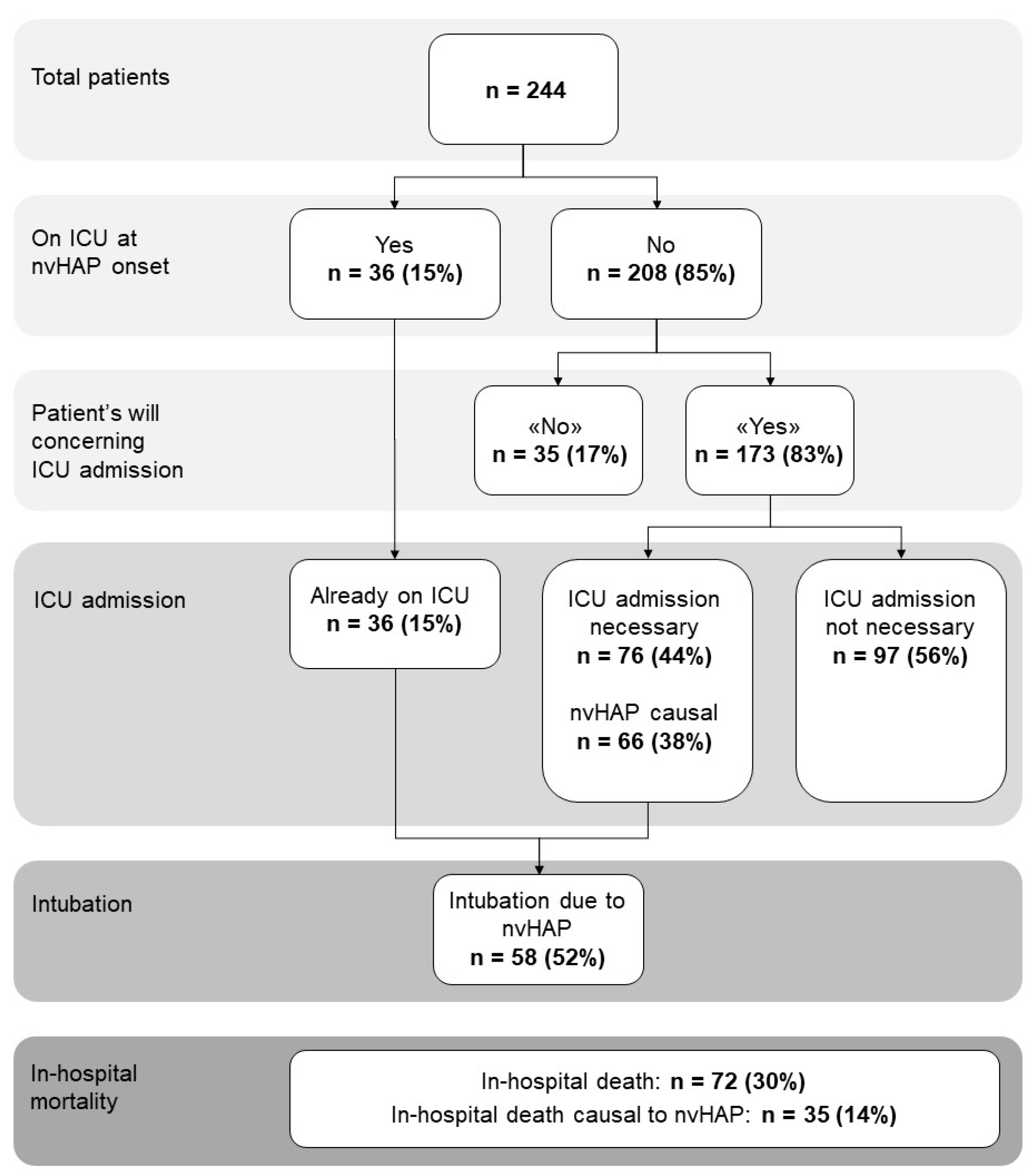
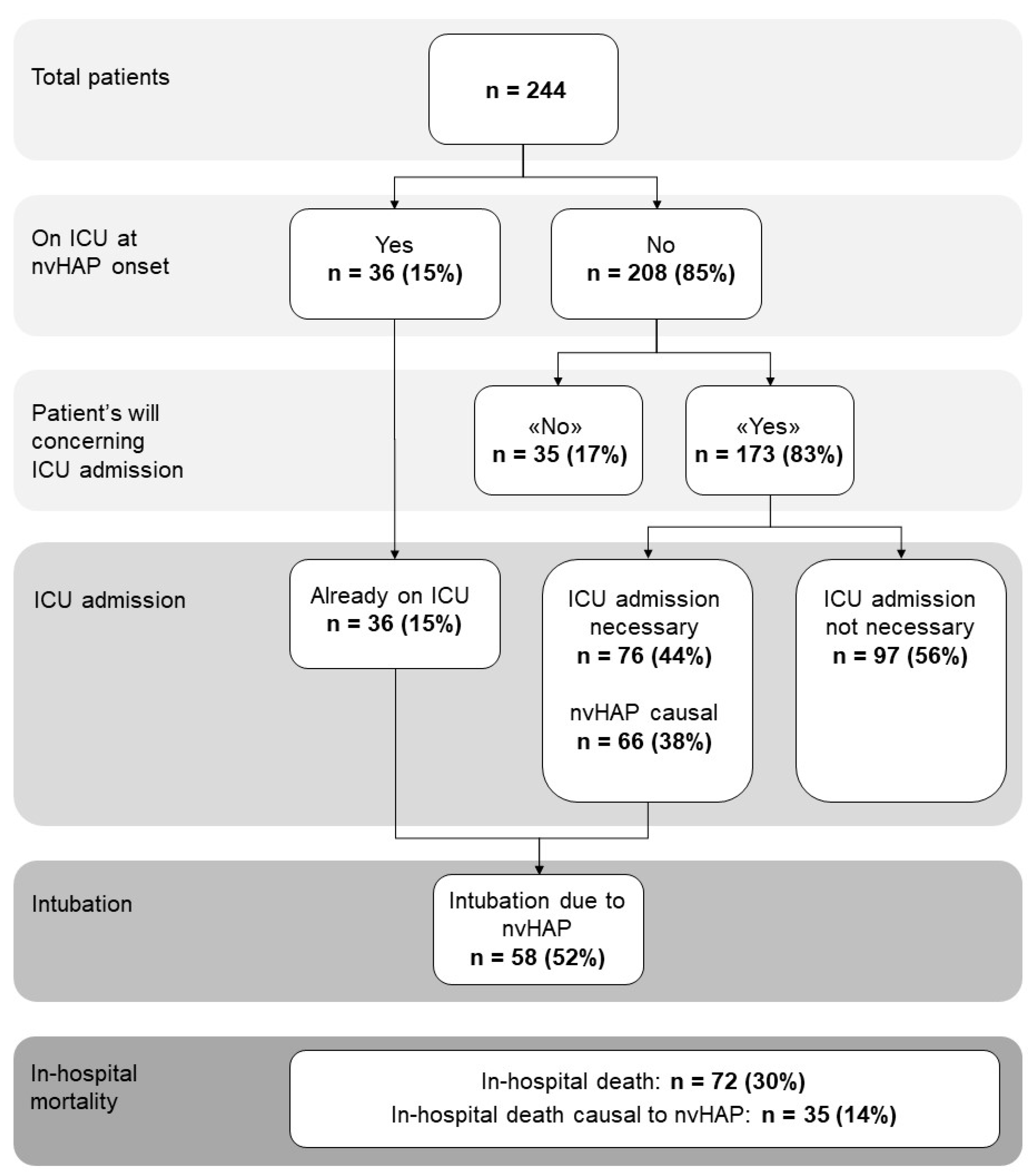
3.1. Frequency of Adverse Events and Associations with nvHAP
3.2. Patient- and Pneumonia-Specific Factors Associated with Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
List of Abbreviations
| ARDS | acute respiratory distress syndrome |
| BMI | body mass index |
| ECDC | European Centre for Disease Prevention and Control |
| EMR | Electronic medical record |
| HAI | healthcare-associated infection |
| HAP | hospital acquired pneumonia |
| ICU | intensive care unit |
| IQR | interquartile range |
| MRDO | multidrug resistant organism |
| nvHAP | non-ventilator-associated hospital-acquired pneumonia |
| qSOFA | quick sequential organ failure assessment score |
| USZ | University hospital Zurich |
| VAP | ventilator-associated pneumonia |
References
- World Health Organization. Global Report on Infection Prevention and Control; World Health Organization: Geneva, Switzerland, 2022; p. 148. Available online: https://www.who.int/publications/i/item/9789240051164 (accessed on 22 December 2023).
- Suetens, C.; Latour, K.; Kärki, T.; Ricchizzi, E.; Kinross, P.; Moro, M.L.; Jans, B.; Hopkins, S.; Hansen, S.; Lyytikäinen, O.; et al. Prevalence of healthcare-associated infections, estimated incidence and composite antimicrobial resistance index in acute care hospitals and long-term care facilities: Results from two European point prevalence surveys, 2016 to 2017. Eurosurveillance 2018, 23, 1800516. [Google Scholar] [CrossRef] [PubMed]
- Magill, S.S.; Edwards, J.R.; Bamberg, W.; Beldavs, Z.G.; Dumyati, G.; Kainer, M.A.; Lynfield, R.; Maloney, M.; McAllister-Hollod, L.; Nadle, J.; et al. Multistate Point-Prevalence Survey of Health Care–Associated Infections. N. Engl. J. Med. 2014, 370, 1198–1208. [Google Scholar] [CrossRef] [PubMed]
- Wolfensberger, A.; Jakob, W.; Faes Hesse, M.; Kuster, S.P.; Meier, A.H.; Schreiber, P.W.; Clack, L.; Sax, H. Development and validation of a semi-automated surveillance system-lowering the fruit for non-ventilator-associated hospital-acquired pneumonia (nvHAP) prevention. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2019, 25, e1427–e1428. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Report on the Burden of Endemic Health Care-Associated Infection Worldwide; World Health Organization: Geneva, Switzerland, 2011; Available online: https://apps.who.int/iris/handle/10665/80135 (accessed on 23 December 2023).
- See, I.; Chang, J.; Gualandi, N.; Buser, G.L.; Rohrbach, P.; Smeltz, D.A.; Bellush, M.J.; Coffin, S.E.; Gould, J.M.; Hess, D.; et al. Clinical Correlates of Surveillance Events Detected by National Healthcare Safety Network Pneumonia and Lower Respiratory Infection Definitions-Pennsylvania, 2011-2012. Infect. Control Hosp. Epidemiol. 2016, 37, 818–824. [Google Scholar] [CrossRef] [PubMed]
- Sopena, N.; Heras, E.; Casas, I.; Bechini, J.; Guasch, I.; Pedro-Botet, M.L.; Roure, S.; Sabrià, M. Risk factors for hospital-acquired pneumonia outside the intensive care unit: A case-control study. Am. J. Infect Control. 2014, 42, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Micek, S.T.; Chew, B.; Hampton, N.; Kollef, M.H. A Case-Control Study Assessing the Impact of Nonventilated Hospital-Acquired Pneumonia on Patient Outcomes. Chest 2016, 150, 1008–1014. [Google Scholar] [CrossRef] [PubMed]
- Munro, S.C.; Baker, D.; Giuliano, K.K.; Sullivan, S.C.; Haber, J.; Jones, B.E.; Crist, M.B.; Nelson, R.E.; Carey, E.; Lounsbury, O.; et al. Nonventilator hospital-acquired pneumonia: A call to action. Infect. Control Hosp. Epidemiol. 2021, 42, 991–996. [Google Scholar] [CrossRef]
- Klompas, M. Hospital-Acquired Pneumonia in Nonventilated Patients: The Next Frontier. Infect. Control Hosp. Epidemiol. 2016, 37, 825–826. [Google Scholar] [CrossRef] [PubMed]
- (ECDC), E.C.P.a.C. CDC/NHSN Surveillance Definitions for Specific Types of Infections. 2014. Available online: http://www.socinorte.com/wp-content/uploads/2014/06/17pscNosInfDef_current.pdf (accessed on 23 December 2023).
- Wolfensberger, A.; Clack, L.; von Felten, S.; Faes Hesse, M.; Saleschus, D.; Meier, M.T.; Kusejko, K.; Kouyos, R.; Held, L.; Sax, H. Prevention of non-ventilator-associated hospital-acquired pneumonia in Switzerland: A type 2 hybrid effectiveness-implementation trial. Lancet. Infect. Dis. 2023, 23, 836–846. [Google Scholar] [CrossRef]
- Marik, P.E.; Taeb, A.M. SIRS, qSOFA and new sepsis definition. J. Thorac. Dis. 2017, 9, 943–945. [Google Scholar] [CrossRef]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Medica 2012, 22, 276–282. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Lancet 2007, 370, 1453–1457. [Google Scholar] [CrossRef] [PubMed]
- De Pauw, B.; Walsh, T.J.; Donnelly, J.P.; Stevens, D.A.; Edwards, J.E.; Calandra, T.; Pappas, P.G.; Maertens, J.; Lortholary, O.; Kauffman, C.A.; et al. Revised definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2008, 46, 1813–1821. [Google Scholar] [CrossRef]
- Greenaway, C.A.; Embil, J.; Orr, P.H.; McLeod, J.; Dyck, B.; Nicolle, L.E. Nosocomial Pneumonia on General Medical and Surgical Wards in a Tertiary-Care Hospital. Infect. Control Hosp. Epidemiol. 1997, 18, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.; Edward, F.; Pennsylvania Patient Safety Authority; ECRI (Organization); Institute for Safe Medication Practices. The Breadth of Hospital-Acquired Pneumonia: Nonventilated versus Ventilated Patients in Pennsylvania. September 2012, Volume 9, No. 3—September 2012. Available online: https://resource.nlm.nih.gov/101591716 (accessed on 24 May 2021).
- Giuliano, K.K.; Baker, D.; Quinn, B. The epidemiology of nonventilator hospital-acquired pneumonia in the United States. Am. J. Infect. Control 2018, 46, 322–327. [Google Scholar] [CrossRef] [PubMed]
- Carey, E.; Blankenhorn, R.; Chen, P.; Munro, S. Non-ventilator associated hospital acquired pneumonia incidence and health outcomes among U.S. veterans from 2016-2020. Am. J. Infect. Control 2022, 50, 116–119. [Google Scholar] [CrossRef] [PubMed]
- Muscedere, J.G.; Day, A.; Heyland1, D.K. Mortality, Attributable Mortality, and Clinical Events as End Points for Clinical Trials of Ventilator-Associated Pneumonia and Hospital-Acquired Pneumonia. Clin. Infect. Dis. 2010, 51, S120–S125. [Google Scholar] [CrossRef] [PubMed]
- Esperatti, M.; Ferrer, M.; Theessen, A.; Liapikou, A.; Valencia, M.; Saucedo, L.M.; Zavala, E.; Welte, T.; Torres, A. Nosocomial pneumonia in the intensive care unit acquired by mechanically ventilated versus nonventilated patients. Am. J. Respir. Crit. Care Med. 2010, 182, 1533–1539. [Google Scholar] [CrossRef] [PubMed]
- Kollef, M.H.; Shorr, A.; Tabak, Y.P.; Gupta, V.; Liu, L.Z.; Johannes, R.S. Epidemiology and outcomes of health-care-associated pneumonia: Results from a large US database of culture-positive pneumonia. Chest 2005, 128, 3854–3862. [Google Scholar] [CrossRef]
- Feng, D.-Y.; Zhou, Y.-Q.; Zou, X.-L.; Zhou, M.; Wu, W.-B.; Chen, X.-X.; Wang, Y.-H.; Zhang, T.-T. Factors influencing mortality in hospital-acquired pneumonia caused by Gram-negative bacteria in China. J. Infect. Public Health 2019, 12, 630–633. [Google Scholar] [CrossRef]
- Ceccato, A.; Panagiotarakou, M.; Ranzani, O.T.; Martin-Fernandez, M.; Almansa-Mora, R.; Gabarrus, A.; Bueno, L.; Cilloniz, C.; Liapikou, A.; Ferrer, M.; et al. Lymphocytopenia as a Predictor of Mortality in Patients with ICU-Acquired Pneumonia. J. Clin. Med. 2019, 8, 843. [Google Scholar] [CrossRef]
- Di Pasquale, M.; Esperatti, M.; Crisafulli, E.; Ferrer, M.; Bassi, G.L.; Rinaudo, M.; Escorsell, A.; Fernandez, J.; Mas, A.; Blasi, F.; et al. Impact of chronic liver disease in intensive care unit acquired pneumonia: A prospective study. Intensive Care Med. 2013, 39, 1776–1784. [Google Scholar] [CrossRef]
- Ranzani, O.T.; Ferrer, M.; Esperatti, M.; Giunta, V.; Bassi, G.L.; Carvalho, C.R.; Torres, A. Association between systemic corticosteroids and outcomes of intensive care unit-acquired pneumonia. Crit. Care Med. 2012, 40, 2552–2561. [Google Scholar] [CrossRef] [PubMed]
- Rinaudo, M.; Ferrer, M.; Terraneo, S.; De Rosa, F.; Peralta, R.; Fernandez-Barat, L.; Li Bassi, G.; Torres, A. Impact of COPD in the outcome of ICU-acquired pneumonia with and without previous intubation. Chest 2015, 147, 1530–1538. [Google Scholar] [CrossRef]
- Barker, L.A.; Gout, B.S.; Crowe, T.C. Hospital Malnutrition: Prevalence, Identification and Impact on Patients and the Healthcare System. Int. J. Environ. Res. Public Health 2011, 8, 514–527. [Google Scholar] [CrossRef]
- Chen, Z.; Wu, H.; Jiang, J.; Xu, K.; Gao, S.; Chen, L.; Wang, H.; Li, X. Nutritional risk screening score as an independent predictor of nonventilator hospital-acquired pneumonia: A cohort study of 67,280 patients. BMC Infect. Dis. 2021, 21, 313. [Google Scholar] [CrossRef]
- Veronese, N.; Cereda, E.; Solmi, M.; Fowler, S.A.; Manzato, E.; Maggi, S.; Manu, P.; Abe, E.; Hayashi, K.; Allard, J.P.; et al. Inverse relationship between body mass index and mortality in older nursing home residents: A meta-analysis of 19,538 elderly subjects. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2015, 16, 1001–1015. [Google Scholar] [CrossRef]
- Andrès, E.; Serraj, K.; Federici, L.; Vogel, T.; Kaltenbach, G. Anemia in elderly patients: New insight into an old disorder. Geriatr. Gerontol. Int. 2013, 13, 519–527. [Google Scholar] [CrossRef]
- Randi, M.L.; Bertozzi, I.; Santarossa, C.; Cosi, E.; Lucente, F.; Bogoni, G.; Biagetti, G.; Fabris, F. Prevalence and Causes of Anemia in Hospitalized Patients: Impact on Diseases Outcome. J. Clin. Med. 2020, 9, 950. [Google Scholar] [CrossRef]
- Falcone, M.; Russo, A.; Gentiloni Silverj, F.; Marzorati, D.; Bagarolo, R.; Monti, M.; Velleca, R.; D’Angelo, R.; Frustaglia, A.; Zuccarelli, G.C.; et al. Predictors of mortality in nursing-home residents with pneumonia: A multicentre study. Clin. Microbiol. Infect. 2018, 24, 72–77. [Google Scholar] [CrossRef]
- Celis, R.; Torres, A.; Gatell, J.M.; Almela, M.; Rodriguez-Roisin, R.; Agusti-Vidal, A. Nosocomial pneumonia. A multivariate analysis of risk and prognosis. Chest 1988, 93, 318–324. [Google Scholar] [CrossRef]
- Jiang, J.; Yang, J.; Mei, J.; Jin, Y.; Lu, Y. Head-to-head comparison of qSOFA and SIRS criteria in predicting the mortality of infected patients in the emergency department: A meta-analysis. Scand. J. Trauma Resusc. Emerg. Med. 2018, 26, 56. [Google Scholar] [CrossRef] [PubMed]
- Giuliano, K.K.; Baker, D. Sepsis in the Context of Nonventilator Hospital-Acquired Pneumonia. Am. J. Crit. Care 2020, 29, 9–14. [Google Scholar] [CrossRef]
- de Assis, M.C.S.; Macedo, A.B.T.; Martins, C.; Konkewicz, L.R.; Viana, L.V.; Tavares, J.P.; Mancuso, A.C.B.; da Rosa, N.G.; Santos, R.P.D. The impact of a bundle to prevent hospital-acquired pneumonia in a cohort of nonventilated patients on enteral nutrition. Infect. Control Hosp. Epidemiol. 2021, 42, 100–102. [Google Scholar] [CrossRef]
- Lacerna, C.C.; Patey, D.; Block, L.; Naik, S.; Kevorkova, Y.; Galin, J.; Parker, M.; Betts, R.; Parodi, S.; Witt, D. A successful program preventing nonventilator hospital-acquired pneumonia in a large hospital system. Infect. Control Hosp. Epidemiol. 2020, 41, 547–552. [Google Scholar] [CrossRef]
- Extermann, M. Measuring comorbidity in older cancer patients. Eur. J. Cancer 2000, 36, 453–471. [Google Scholar] [CrossRef] [PubMed]
- Sundararajan, V.; Henderson, T.; Perry, C.; Muggivan, A.; Quan, H.; Ghali, W.A. New ICD-10 version of the Charlson comorbidity index predicted in-hospital mortality. J. Clin. Epidemiol. 2004, 57, 1288–1294. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]

{kind=link}
| Patient Population n = 244 | |
|---|---|
| Patient Characteristics | |
| Age, median (IQR) | 67 (55–79) |
| Male sex, No. (%) | 162 (66.4%) |
| BMI, median (IQR) 1 | 24.5 (22.0–27.8) |
| Affiliation to non-surgical department, No. (%) | 137 (56.2%) |
| Charlson Comorbidity index, median (IQR) | 5 (4–7) |
| Myocardial infarction, No. (%) | 55 (22.5%) |
| Congestive heart failure, No. (%) | 34 (13.9%) |
| Peripheral vascular disease, No. (%) | 32 (13.1%) |
| Cerebrovascular disease, No. (%) | 47 (19.3%) |
| Dementia, No. (%) | 17 (7.0%) |
| COPD, No. (%) | 25 (10.3%) |
| Connective tissue disease, No. (%) | 15 (6.2%) |
| Ulcer disease, No. (%) | 26 (10.7%) |
| Mild liver disease, No. (%) | 16 (6.6%) |
| Moderate or severe liver disease, No. (%) | 18 (7.4%) |
| Diabetes without complications, No. (%) | 20 (8.2%) |
| Diabetes with end organ damage, No. (%) | 37 (15.2%) |
| Hemiplegia, No. (%) | 3 (1.2%) |
| Moderate or severe renal disease, No. (%) | 43 (17.6%) |
| Solid tumour non metastatic, No. (%) | 40 (16.4%) |
| Second metastatic solid tumour, No. (%) | 11 (4.5%) |
| Leukaemia, No. (%) | 23 (9.4%) |
| Lymphoma, Multiple Myeloma, No. (%) | 18 (7.4%) |
| AIDS, No. (%) | 3 (1.2%) |
| Hb on admission (g/L), median (IQR) | 112 (93–131) |
| Albumin (g/L) on admission, median (IQR) 1 | 33 (27–38) |
| Urea (mmol/L) on admission, median (IQR) 1 | 6.8 (4.8–9.8) |
| Pneumonia Characteristics | |
| Bacterial pneumonia (bacterial pathogen in respiratory sample or BC, except oral flora or CNS), No. (%) | 71 (29.1%) |
| Positive blood culture (except CNS), No. (%) | 22 (9.0%) |
| Positive respiratory sample (except oral flora or CNS), No. (%) | 58 (23.8%) |
| Viral pneumonia, No. (%) | 13 (5.3%) |
| Fungal pneumonia, No. (%) | 14 (5.7%) |
| Infection with MDRO, No. (%) | 13 (5.3%) |
| Bilateral infiltrate, No. (%) | 111 (45.5%) |
| Sepsis, No. (%) | 79 (32.4%) |
| Empyema, No. (%) | 3 (1.2%) |
| ARDS, No. (%) | 12 (5.0%) |
| CRP peak (mg/L), median | 161 (97–270) |
| Parameters (n = 244) | Univariable Analysis Odds Ratio (95%CI), p-Value | Multivariable Analysis Odds Ratio (95%CI), p-Value |
|---|---|---|
| Age | 1.03 (1.00–1.05), p = 0.029 | 1.02 (1.00–1.05), p = 0.063 |
| Male gender | 1.12 (0.52–2.42), p = 0.768 | |
| BMI 1 | 0.90 (0.82–0.98), p = 0.011 | 0.90 (0.82–0.99), p = 0.024 |
| Charlson comorbidity index | 1.13 (1.00–1.29), p = 0.065 | |
| Congestive heart failure | 1.03 (0.37–2.88), p = 0.948 | |
| COPD | 0.49 (0.11–2.18), p = 0.349 | |
| Cerebrovascular disease | 1.86 (0.82–4.20), p = 0.136 | |
| Moderate or severe liver disease | 0.73 (0.16–3.33), p = 0.685 | |
| Moderate or severe renal disease | 0.56 (0.19–1.69), p = 0.304 | |
| Solid tumour | 1.06 (0.41–2.76), p = 0.897 | |
| Immunosupression | 0.72 (0.30–1.74), p = 0.462 | |
| Leukemia, Lymphoma and Multiple Myeloma | 1.38 (0.56–3.43), p = 0.485 | |
| Hb on admission (g/L) | 0.99 (0.97–1.00), p = 0.033 | 0.98 (0.97–1.00), p = 0.049 |
| Albumin (g/L) on admission 1 | 0.92 (0.87–0.98), p = 0.005 | |
| Urea (mmol/L) on admission 1 | 1.05 (1.00–1.09), p = 0.031 | 1.03 (0.98–1.08), p = 0.202 |
| Parameters (n = 244) | Univariable Analysis Odds Ratio (95%CI) p-Value | Multivariable Analysis Odds Ratio (95%CI), p-Value |
|---|---|---|
| Bacterial pneumonia (bacterial pathogen in respiratory sample * or BC, except oral flora or CNS) | 1.33 (0.62–2.84), p = 0.466 | |
| Viral pneumonia | 1.87 (0.49–7.15), p = 0.363 | |
| Fungal pneumonia § | 1.69 (0.45–6.38), p = 0.441 | |
| Infection with MDRO | 1.09 (0.23–5.15), p = 0.912 | |
| Colonisation with MRDO | 0.78 (0.17–3.59), p = 0.754 | |
| Bilateral infiltrate | 3.06 (1.42–6.57), p = 0.004 | 2.31 (1.01–5.25), p = 0.047 |
| Sepsis | 3.91 (1.86–8.19), p = 0.000 | 2.99 (1.36–6.59), p = 0.006 |
| Empyema | 12.61 (1.11–142.96), p = 0.041 | 5.82 (0.47–71.81), p = 0.170 |
| ARDS | 4.81 (1.43–16.13), p = 0.011 | 3.27 (0.81–13.14), p = 0.095 |
| nvHAP acquired on ICU | 0.15 (0.02–1.14), p = 0.067 | 0.14 (0.02–1.13), p = 0.064 |
| CRP peak (mg/L) | 1.00 (1.00–1.00), p = 0.784 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amodio, E.; Schreiber, P.W.; Faes Hesse, M.; Wolfensberger, A. Adverse Outcomes of Patients with Non-Ventilator-Associated Hospital-Acquired Pneumonia (nvHAP)—A Single Centre Cohort Study. Infect. Dis. Rep. 2024, 16, 228-238. https://doi.org/10.3390/idr16020018
Amodio E, Schreiber PW, Faes Hesse M, Wolfensberger A. Adverse Outcomes of Patients with Non-Ventilator-Associated Hospital-Acquired Pneumonia (nvHAP)—A Single Centre Cohort Study. Infectious Disease Reports. 2024; 16(2):228-238. https://doi.org/10.3390/idr16020018
Chicago/Turabian StyleAmodio, Enrica, Peter W. Schreiber, Mirjam Faes Hesse, and Aline Wolfensberger. 2024. "Adverse Outcomes of Patients with Non-Ventilator-Associated Hospital-Acquired Pneumonia (nvHAP)—A Single Centre Cohort Study" Infectious Disease Reports 16, no. 2: 228-238. https://doi.org/10.3390/idr16020018
APA StyleAmodio, E., Schreiber, P. W., Faes Hesse, M., & Wolfensberger, A. (2024). Adverse Outcomes of Patients with Non-Ventilator-Associated Hospital-Acquired Pneumonia (nvHAP)—A Single Centre Cohort Study. Infectious Disease Reports, 16(2), 228-238. https://doi.org/10.3390/idr16020018