
Impact of Ambient Air Pollution Exposure on Long COVID-19 Symptoms: A Cohort Study within the Saudi Arabian Population


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Air Particulate Matter (PM10 and PM2.5 Sampling)
2.3. Statistical Analysis
3. Results
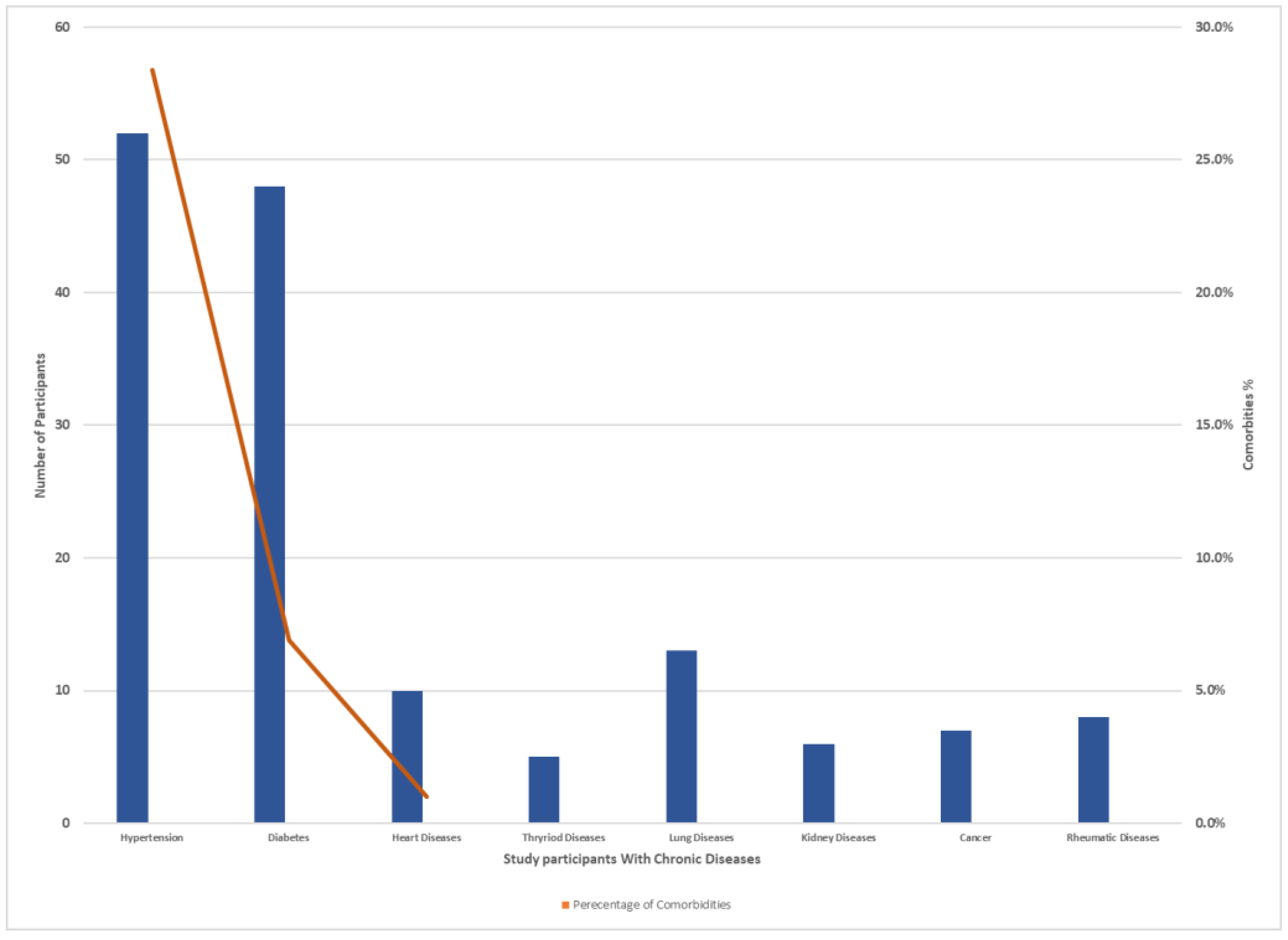
3.1. Participants Demographic Characteristics
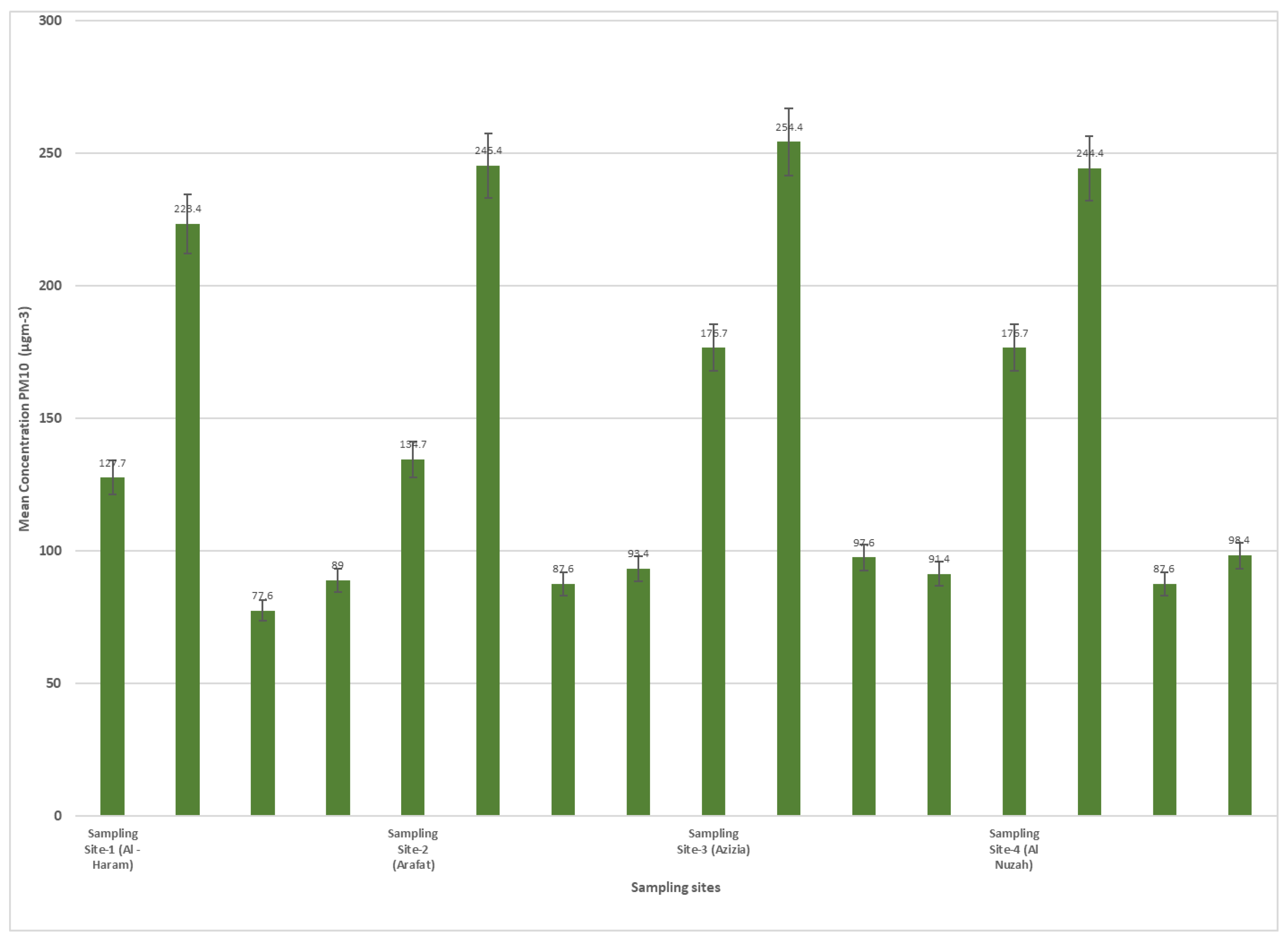
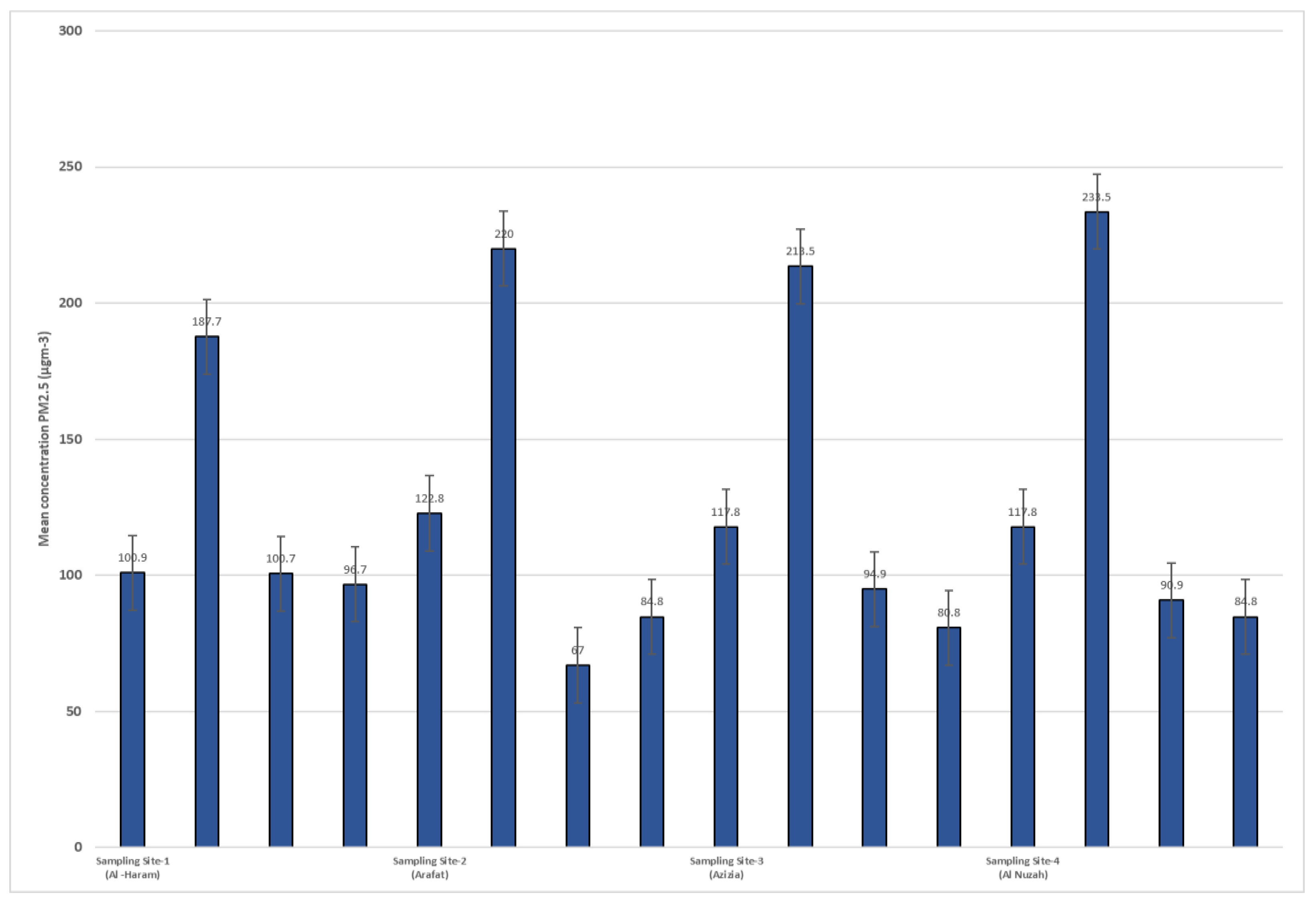
3.2. Air Quality in Sampling Sites
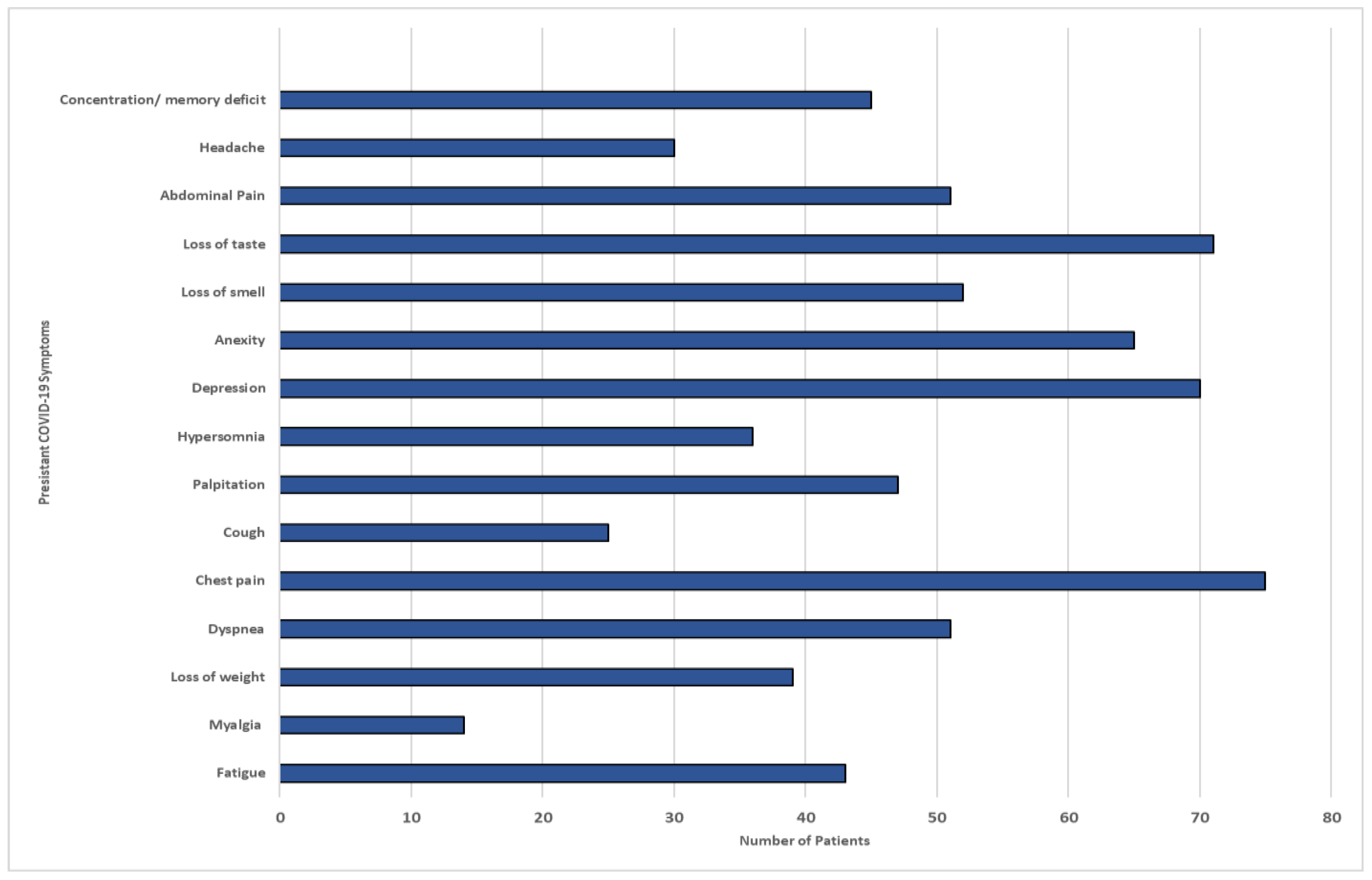
3.3. Characteristics of Post Recovery Long COVID-19 Symptoms
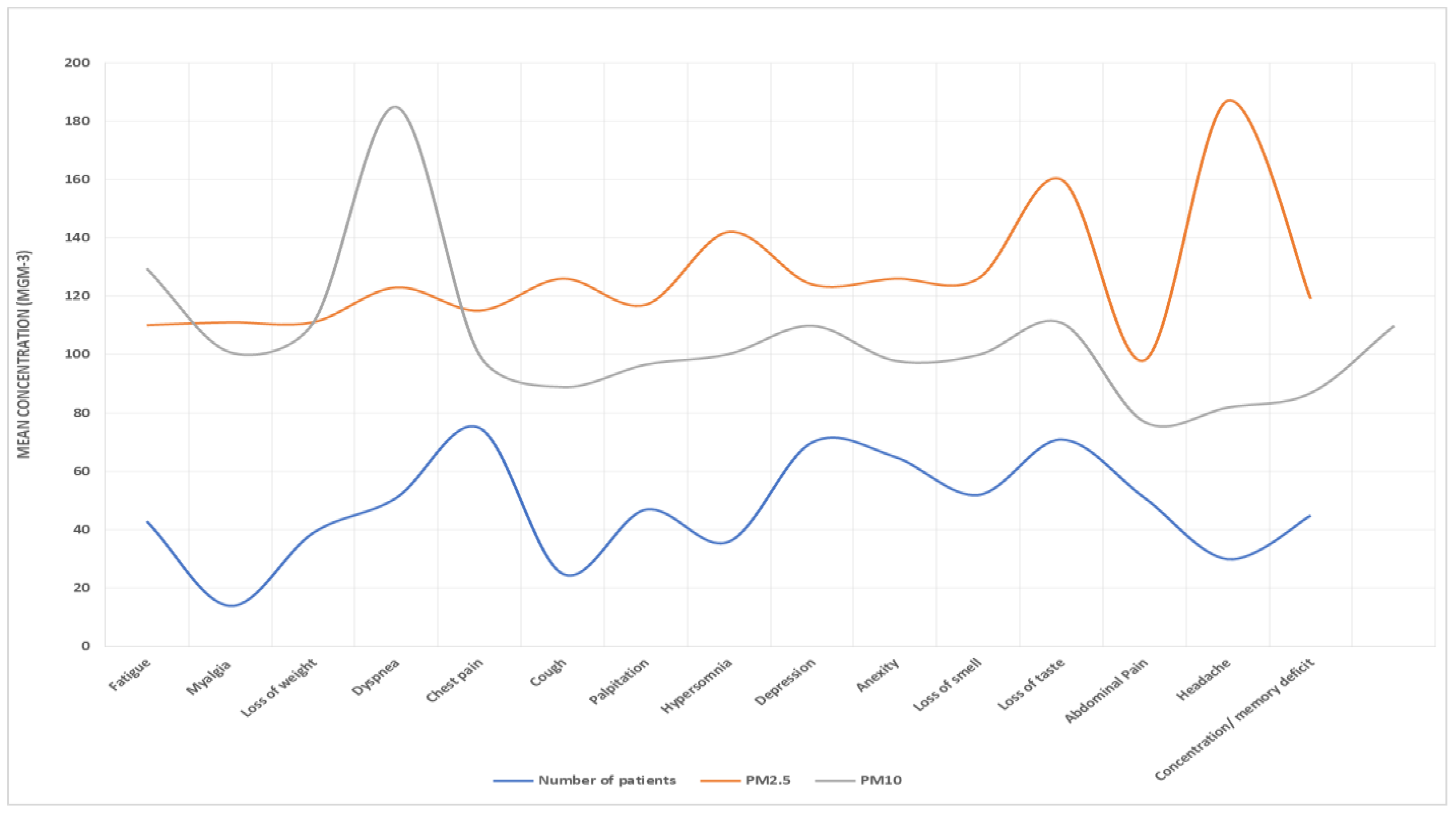
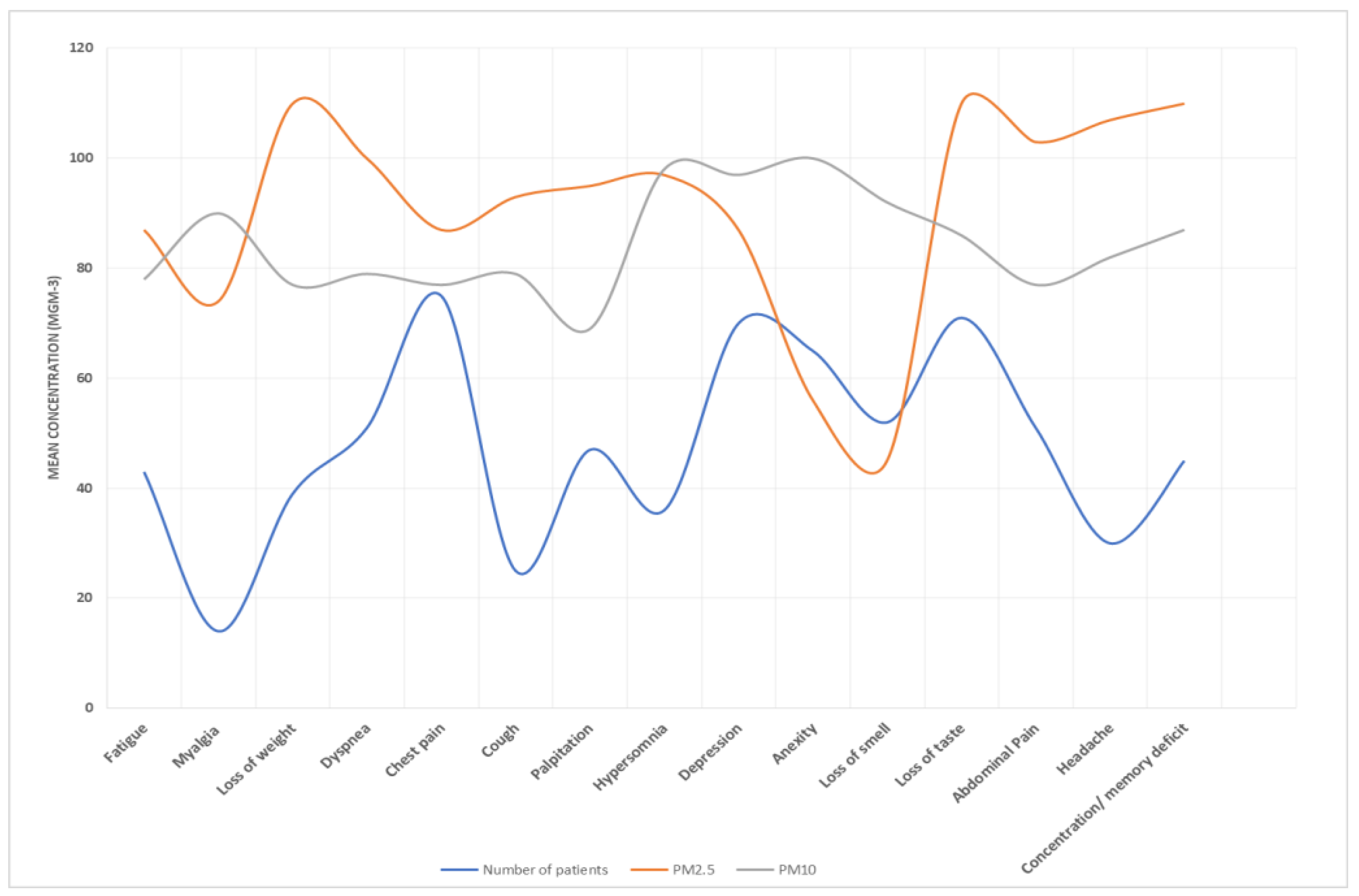
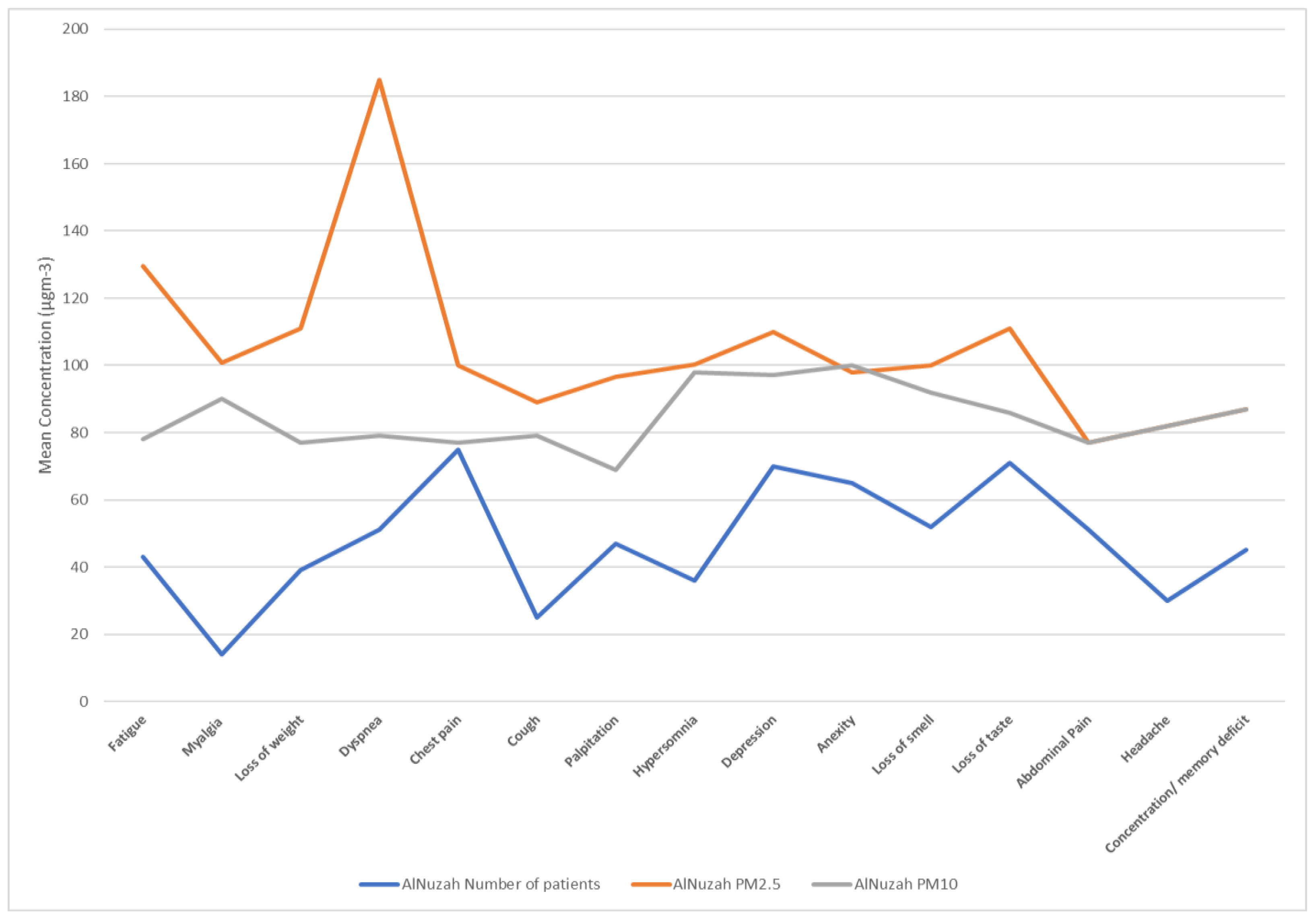
3.4. Association of Air Particulate Matter (PM10, PM2.5) and Long COVID Symptoms
3.5. Multivariate Analysis Addressing Confounding
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Raveendran, A.V.; Jayadevan, R.; Sashidharan, S. Long COVID: An overview. Diabetes Metab. Syndr. 2021, 15, 869–875, Erratum in Diabetes Metab. Syndr. 2022, 16, 102504. Erratum in Diabetes Metab. Syndr. 2022, 16, 102660. [Google Scholar] [CrossRef] [PubMed]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef]
- Koc, H.C.; Xiao, J.; Liu, W.; Li, Y.; Chen, G. Long COVID and its Management. Int. J. Biol. Sci. 2022, 18, 4768–4780. [Google Scholar] [CrossRef]
- Ali, N.; Fariha, K.A.; Islam, F.; Mishu, M.A.; Mohanto, N.C.; Hosen, M.J.; Hossain, K. Exposure to air pollution and COVID-19 severity: A review of current insights, management, and challenges. Integr. Environ. Assess. Manag. 2021, 17, 1114–1122. [Google Scholar] [CrossRef] [PubMed]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S.; et al. Attributes and predictors of long COVID. Nat. Med. 2021, 27, 626–631. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Wang, J.; Kwong, J.; Kim, J.; van Donkelaar, A.; Martin, R.V.; Hystad, P.; Su, Y.; Lavigne, E.; Kirby-McGregor, M.; et al. Association between long-term exposure to ambient air pollution and COVID-19 severity: A prospective cohort study. CMAJ 2022, 194, E693–E700. [Google Scholar] [CrossRef]
- Dominici, F.; Zanobetti, A.; Schwartz, J.; Braun, D.; Sabath, B.; Wu, X. Assessing Adverse Health Effects of Long-Term Exposure to Low Levels of Ambient Air Pollution: Implementation of Causal Inference Methods. Res Rep Health Eff Inst. 2022, 2022, 211. [Google Scholar]
- Lai, A.; Chang, M.L.; O’Donnell, R.P.; Zhou, C.; Sumner, J.A.; Hsiai, T.K. Association of COVID-19 transmission with high levels of ambient pollutants: Initiation and impact of the inflammatory response on cardiopulmonary disease. Sci. Total Environ. 2021, 779, 146464. [Google Scholar] [CrossRef]
- Paital, B.; Agrawal, P.K. Air pollution by NO2 and PM2.5 explains COVID-19 infection severity by overexpression of angiotensin-converting enzyme 2 in respiratory cells: A review. Environ. Chem. Lett. 2021, 19, 25–42. [Google Scholar] [CrossRef]
- Maheswari, S.; Pethannan, R.; Sabarimurugan, S. Air pollution enhances susceptibility to novel coronavirus (COVID-19) infection—An impact study. Environ. Anal. Health Toxicol. 2020, 35, e2020020. [Google Scholar] [CrossRef]
- Bonilla, J.A.; Lopez-Feldman, A.; Pereda, P.C.; Rivera, N.M.; Ruiz-Tagle, J.C. Association between long-term air pollution exposure and COVID-19 mortality in Latin America. PLoS ONE 2023, 18, e0280355. [Google Scholar] [CrossRef] [PubMed]
- Comunian, S.; Dongo, D.; Milani, C.; Palestini, P. Air Pollution and COVID-19: The Role of Particulate Matter in the Spread and Increase of COVID-19’s Morbidity and Mortality. Int. J. Environ. Res. Public Health 2020, 17, 4487. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, J.C.; Moreira, T.C.L.; de Araújo, A.L.; Imamura, M.; Damiano, R.F.; Garcia, M.L.; Sawamura, M.V.; Pinna, F.R.; Guedes, B.F.; Gonçalves, F.A.R.; et al. Clinical, sociodemographic and environmental factors impact post-COVID-19 syndrome. J. Glob. Health 2022, 12, 05029. [Google Scholar] [CrossRef]
- Ali, N.; Islam, F. The Effects of Air Pollution on COVID-19 Infection and Mortality—A Review on Recent Evidence. Front. Public Health 2020, 8, 580057. [Google Scholar] [CrossRef] [PubMed]
- Rahimi, N.R.; Fouladi-Fard, R.; Aali, R.; Shahryari, A.; Rezaali, M.; Ghafouri, Y.; Ghalhari, M.R.; Asadi-Ghalhari, M.; Farzinnia, B.; Conti Gea, O.; et al. Bidirectional association between COVID-19 and the environment: A systematic review. Environ. Res. 2021, 194, 110692. [Google Scholar] [CrossRef]
- Srivastava, A. COVID-19 and air pollution and meteorology-an intricate relationship: A review. Chemosphere 2021, 263, 128297. [Google Scholar] [CrossRef] [PubMed]
- Mario, C. How do low wind speeds and high levels of air pollution support the spread of COVID-19? Atmos. Pollut. Res. 2021, 12, 437–445. [Google Scholar] [CrossRef]
- Semczuk-Kaczmarek, K.; Rys-Czaporowska, A.; Sierdzinski, J.; Kaczmarek, L.D.; Szymanski, F.M.; Platek, A.E. Association between air pollution and COVID-19 mortality and morbidity. Intern. Emerg. Med. 2022, 17, 467–473. [Google Scholar] [CrossRef]
- Aiyegbusi, O.L.; Hughes, S.E.; Turner, G.; Rivera, S.C.; McMullan, C.; Chandan, J.S.; Haroon, S.; Price, G.; Davies, E.H.; Nirantharakumar, K.; et al. Symptoms, complications and management of long COVID: A review. J. R. Soc. Med. 2021, 114, 428–442. [Google Scholar] [CrossRef]
- Sheridan, C.; Klompmaker, J.; Cummins, S.; James, P.; Fecht, D.; Roscoe, C. Associations of air pollution with COVID-19 positivity, hospitalisations, and mortality: Observational evidence from UK Biobank. Environ. Pollut. 2022, 308, 119686. [Google Scholar] [CrossRef]
- Magazzino, C.; Mele, M.; Schneider, N. The relationship between air pollution and COVID-19-related deaths: An application to three French cities. Appl. Energy 2020, 279, 115835. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Clinical Management of COVID-19 (Interim Guidance). 2020. Available online: https://www.who.int/publications-detail/clinicalmanagement-of-covid-19 (accessed on 30 April 2021).
- Environment Protection Agency (USEPA). Method 29-Determination of Metals Emssions from Stationary Sources. Available online: https://www.gpo.gov/fdsys/pkg/FR-2016-08-30/pdf/2016-19642.pdf (accessed on 12 October 2023).
- Coccia, M. Factors determining the diffusion of COVID-19 and suggested strategy to prevent future accelerated viral infectivity similar to COVID. Sci. Total Environ. 2020, 729, 138474. [Google Scholar] [CrossRef] [PubMed]
- Mendy, A.; Wu, X.; Keller, J.L.; Fassler, C.S.; Apewokin, S.; Mersha, T.B.; Xie, C.; Pinney, S.M. Air pollution and the pandemic: Long-term PM2.5 exposure and disease severity in COVID-19 patients. Respirology 2021, 26, 1181–1187. [Google Scholar] [CrossRef] [PubMed]
- Thangavel, P.; Park, D.; Lee, Y.-C. Recent Insights into Particulate Matter (PM2.5)-Mediated Toxicity in Humans: An Overview. Int. J. Environ. Res. Public Health 2022, 19, 7511. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Liu, S. The Effects and Pathogenesis of PM2.5 and Its Components on Chronic Obstructive Pulmonary Disease. Int. J. Chronic Obstr. Pulm. Dis. 2023, 18, 493–506. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Li, C.; Tang, X. The Impact of PM2.5 on the Host Defense of Respiratory System. Front. Cell Dev. Biol. 2020, 8, 91. [Google Scholar] [CrossRef]
- Wieczfinska, J.; Kleniewska, P.; Pawliczak, R. Oxidative Stress-Related Mechanisms in SARS-CoV-2 Infections. Oxidative Med. Cell. Longev. 2022, 2022, 5589089. [Google Scholar] [CrossRef]
- Yu, Z.; Ekström, S.; Bellander, T.; Ljungman, P.; Pershagen, G.; Eneroth, K.; Kull, I.; Bergström, A.; Georgelis, A.; Stafoggia, M.; et al. BAMSE COVID-19 Study Group. Ambient air pollution exposure linked to long COVID among young adults: A nested survey in a population-based cohort in Sweden. Lancet Reg. Health Eur. 2023, 28, 100608. [Google Scholar] [CrossRef]
- Frontera, A.; Cianfanelli, L.; Vlachos, K.; Landoni, G.; Cremona, G. Severe air pollution links to higher mortality in COVID-19 patients: The “double-hit” hypothesis. J. Infect. 2020, 81, 255–259. [Google Scholar] [CrossRef]
- Hyman, S.; Zhang, J.; Andersen, Z.J.; Cruickshank, S.; Møller, P.; Daras, K.; Williams, R.; Topping, D.; Lim, Y.H. Long-term exposure to air pollution and COVID-19 severity: A cohort study in Greater Manchester, United Kingdom. Environ. Pollut. 2023, 327, 121594. [Google Scholar] [CrossRef]
- Hernandez Carballo, I.; Bakola, M.; Stuckler, D. The impact of air pollution on COVID-19 incidence, severity, and mortality: A systematic review of studies in Europe and North America. Environ. Res. 2022, 215 Pt 1, 114155. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Sidell, M.A.; Huang, B.Z.; Chow, T.; Eckel, S.P.; Martinez, M.P.; Gheissari, R.; Lurmann, F.; Thomas, D.C.; Gilliland, F.D.; et al. Ambient Air Pollutant Exposures and COVID-19 Severity and Mortality in a Cohort of Patients with COVID-19 in Southern California. Am. J. Respir. Crit. Care Med. 2022, 206, 440–448. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sampling Location | Coordinates | Site Description | Land Use Status | Automobile Traffic Volume | Precipitation | Temperature and Humidity | Wind Direction | Wind Speed |
|---|---|---|---|---|---|---|---|---|
| Al-Haram | 21°25′19.2″ N, 39°49′33.6″ E | High traffic volume due to religious significance; extensive construction activities | Urban, construction | High | Sparse, mostly in winter | Urban heat island effect, humid | North-westerly | 10–15 km/h average |
| Arafat | About 20 km from Central Makkah | Rural with seasonal heavy traffic during Hajj | Rural, seasonal pilgrim activities | Heavy (seasonal) | Moderate, winter months | Cooler with high nighttime humidity | North-westerly with occasional shifts | 8–12 km/h average |
| Al-Aziziyah | 32°31′48″ N, 13°0′36″ E | Residential areas with moderate traffic flow | Residential | Moderate | Sparse | Moderate with periodic humidity spikes | North-westerly | 10–14 km/h average |
| Al-Nuzhah | About 5 km from Al-Haram | Residential and commercial with medium-to-high traffic due to local activities | Mixed (Residential and commercial) | Medium-to-high | Sparse, occasional showers | Typical urban climate, moderate humidity | North-westerly | 10–15 km/h average |
| Characteristics of Participants | Value |
|---|---|
| Age, years, n (%) | 18–29, 67 (16.3%) 30–50, 223 (54.5%) ≥50, 120 (29.2%) |
| Gender | Males 204 (49.8%) Females 206 (50.2%) |
| Time since diagnosis (Months, n, %) | ≤3 months, 187 (45.6%) ≥3 months, 64 (15.6%) ≥6 months, 159 (38.8%) |
| Initial symptom severity, n (%) | Asymptomatic 40 (9.8%) Mild-to-moderate 299 (72.9%) Severe to very severe 71 (17.3%) |
| Hospitalization and ICU stay: Non-hospitalized, n (%) | 369 (90%) |
| Hospitalized without ICU stay, n (%) | 36 (8.9%) |
| Hospitalized with ICU stay, n (%) | 5 (1.1%) |
| Comorbidities No comorbidity At least one comorbidity | 261 (63.7%) 284 (38.3%) |
| Vaccination status Had booster dose Two doses | 372 (90.8%) 37 (9.2%) |
| Sampling Sites | Number of Participants | PM10 Concentration Range (µg/m3) | PM10 Average Concentration (µg/m3) | p Value | CI (95%) | PM2.5 Concentration Range (µg/m3) | PM2.5 Average Concentration (µg/m3) | p Value | CI (95%) |
|---|---|---|---|---|---|---|---|---|---|
| Al-Haram high traffic volume | 112 | 127.7 (spring)–176.7 (autumn) | 152.2 | 0.05 | 147.2–157.2 | 100.9 (spring)–122.8 (summer) | 111.85 | 0.02 | 106.2–117.5 |
| Al-Aziziyah residential areas with a moderate level of traffic flow | 86 | 77.6 (spring)–97.6 (autumn) | 87.6 | 0.03 | 82.5–92.7 | 100.7 (spring)–94.9 (autumn) | 97.8 | 0.04 | 92.5–103.1 |
| Al Nuzhah residential and commercial areas, where traffic load ranges from medium to high | 128 | 89 (spring)– 98.4 (winter) | 128 | 0.07 | 88.6–98.8 | 96.7 (spring)–84.8 (summer) | 90.75 | 0.05 | 85.5–95.9 |
| Arafat rural area (seasonal heavy traffic) | 84 | 223.4 (spring)–244.4 (summer) | 233.9 | 0.01 | 228.9–238.9 | 187.7 (spring)–233.5 (autumn) | 210.6 | 0.01 | 205.1–216.1 |
| Post-COVID-19 Symptoms Category | Sampling Sites in Makkah | Total (n = 410) | |||
|---|---|---|---|---|---|
| High Traffic Volume | Residential Areas: Moderate Level of Traffic Flow | Residential and Commercial Areas: Traffic Load Ranges from Medium to High | Rural Area: Seasonal Heavy Traffic | ||
| Al-Haram | Al-Aziziyah | Al Nuzhah | Arafat | ||
| Individuals with persistent symptoms (n, %) | 60 (40%) | 30 (20%) | 45 (30%) | 15 (10%) | 150 (63.5%) |
| Individuals vaccinated at least 2 doses (n, %) | 112 (100%) | 86 (100%) | 128 (100%) | 84 (100%) | 410 (100%) |
| Two or more symptoms (n, %) | 34 (23%) | 17 (11%) | 26 (17%) | 10 (7%) | 87 (58%) |
| Systemic symptoms (n, %) | |||||
| Fatigue | 17 (11.3%) | 8.5 (5.7%) | 13 (8.7%) | 5.5 (3.7%) | 29% |
| Headache | 12 (8%) | 6 (4%) | 9 (6%) | 3 (2%) | 20% |
| Myalgia | 5.7 (3.8%) | 2.8 (1.9%) | 4.3 (2.9%) | 1.4 (0.9%) | 9.5% |
| Respiratory symptoms (n, %) | 25 (16.7%) | 12.5 (8.3%) | 19 (12.7%) | 5.5 (3.7%) | 62 (41.5%) |
| Neuropsychiatric symptoms (n, %) | 15 (10%) | 7.5 (5%) | 11 (7.3%) | 4.5 (3%) | 38 (25.4%) |
| Concentration/memory deficits | 10 (6.7%) | 5 (3.3%) | 7.5 (5%) | 2.5 (1.7%) | 16.7% |
| Headaches | 5.9 (3.9%) | 2.9 (1.9%) | 4.4 (2.9%) | 1.4 (0.9%) | 9.9% |
| Anxiety | 6.1 (4.1%) | 3.05 (2%) | 4.6 (3.1%) | 1.54 (1%) | 10.2% |
| Depression | 5.7 (3.8%) | 2.8 (1.9%) | 4.3 (2.9%) | 1.4 (0.9%) | 9.5% |
| Dermatological symptoms (n, %) | |||||
| Hair loss | 6.9 (4.6%) | 3.45 (2.3%) | 5.2 (3.4%) | 1.74 (1.2%) | 11.5% |
| No post-recovery symptoms (n, %) | 104 (40%) | 52 (20%) | 73 (30%) | 26 (10%) | 260 (63.4%) |
| Pollutant Exposure | Air Pollutant | RR (95% CI) |
|---|---|---|
| Annual exposure average | PM2.5 | 1.32 (1.05, 1.67) |
| PM10 | 1.27 (1.00, 1.61) |
| Variable | Adjusted Odds Ratio | 95% CI | p Value |
|---|---|---|---|
| Age (per 10 years) | 1.25 | (1.10, 1.42) | 0.001 |
| Gender (male vs. female) | 0.85 | (0.70, 1.02) | 0.08 |
| Comorbidity (yes vs. no) | 1.55 | (1.25, 1.92) | <0.001 |
| Air Quality (PM2.5 levels) | 1.35 | (1.20, 1.52) | <0.001 |
| Smoking (yes vs. no) | 0.95 | (0.80, 1.12) | 0.55 |
| Vaccination status (booster vs. two doses) | 1.20 | (1.05, 1.37) | 0.008 |
| Residential area (high traffic vs. low traffic) | 1.45 | (1.32, 1.60) | <0.001 |
| Variable | Adjusted Rate Ratio (RR) | 95% Confidence Interval (CI) |
|---|---|---|
| PM2.5 exposure | 1.28 | 1.06–1.54 |
| PM10 exposure | 1.24 | 0.98–1.56 |
| Age (ref: 18–29 years) | ||
| 1.12 | 0.92–1.37 |
| 1.40 | 1.15–1.70 |
| Gender (ref: males) | ||
| 1.08 | 0.90–1.29 |
| Time since diagnosis (ref: ≤3 months) | ||
| 1.15 | 0.98–1.36 |
| 1.20 | 1.02–1.41 |
| Scenario | Adjusted Odds Ratio | 95% CI | p Value |
|---|---|---|---|
| Excluding participants older than 60 | 1.20 | (1.05, 1.37) | 0.008 |
| Using logistic regression with robust standard errors | 1.25 | (1.10, 1.42) | 0.001 |
| Including only non-smokers | 1.28 | (1.12, 1.46) | 0.0005 |
| Varying PM2.5 exposure definitions (daily vs. annual avg.) | 1.30 | (1.15, 1.48) | 0.0002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saleh, S.A.K.; Adly, H.M. Impact of Ambient Air Pollution Exposure on Long COVID-19 Symptoms: A Cohort Study within the Saudi Arabian Population. Infect. Dis. Rep. 2023, 15, 642-661. https://doi.org/10.3390/idr15050060
Saleh SAK, Adly HM. Impact of Ambient Air Pollution Exposure on Long COVID-19 Symptoms: A Cohort Study within the Saudi Arabian Population. Infectious Disease Reports. 2023; 15(5):642-661. https://doi.org/10.3390/idr15050060
Chicago/Turabian StyleSaleh, Saleh A. K., and Heba M. Adly. 2023. "Impact of Ambient Air Pollution Exposure on Long COVID-19 Symptoms: A Cohort Study within the Saudi Arabian Population" Infectious Disease Reports 15, no. 5: 642-661. https://doi.org/10.3390/idr15050060
APA StyleSaleh, S. A. K., & Adly, H. M. (2023). Impact of Ambient Air Pollution Exposure on Long COVID-19 Symptoms: A Cohort Study within the Saudi Arabian Population. Infectious Disease Reports, 15(5), 642-661. https://doi.org/10.3390/idr15050060