
Mycobacterium tuberculosis Surgical Site Infection after Cardiac Surgery in the COVID-19 Era: A Case Report



 ,
, 
{kind=link}
{kind=link}
Abstract
:1. Introduction
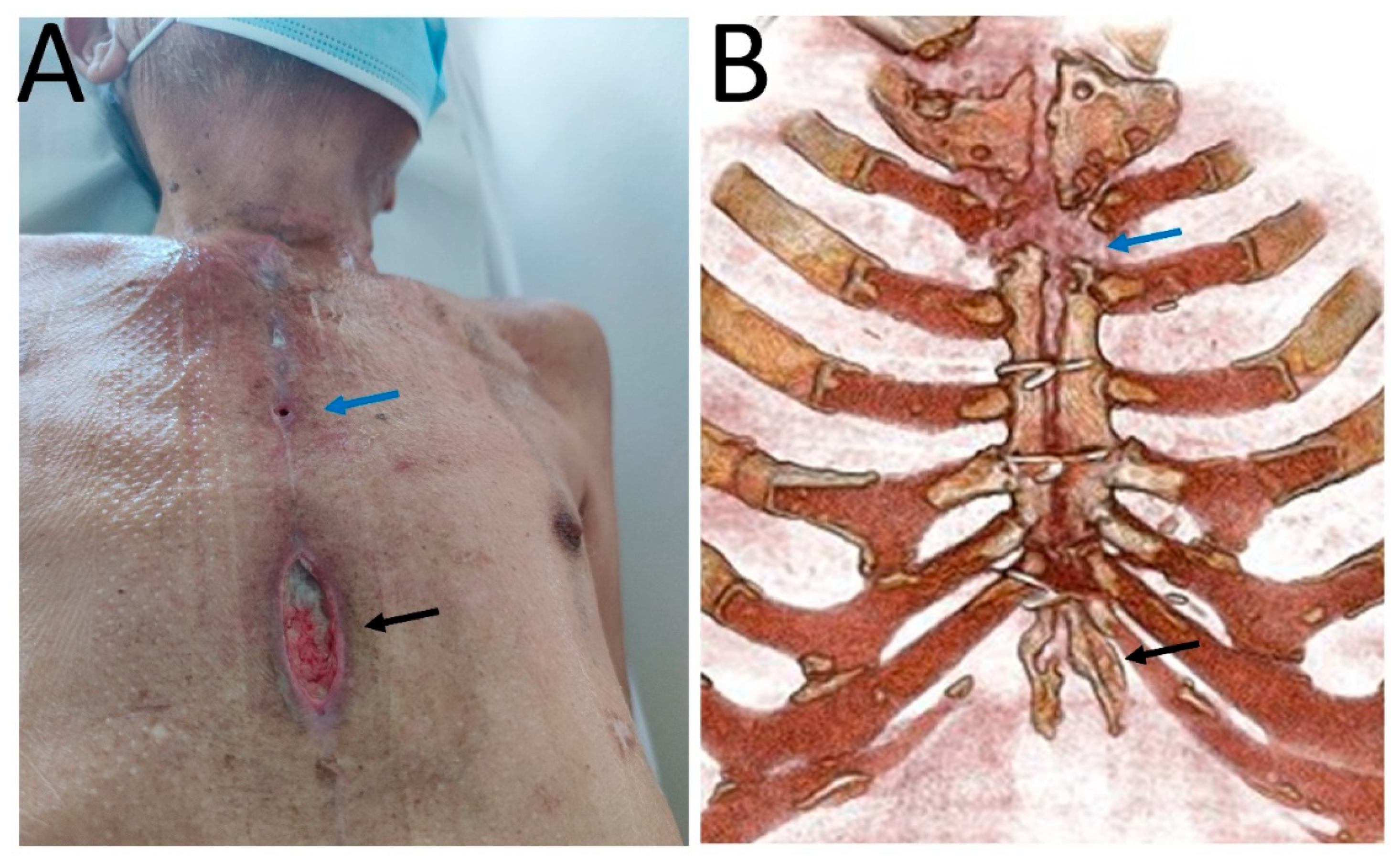
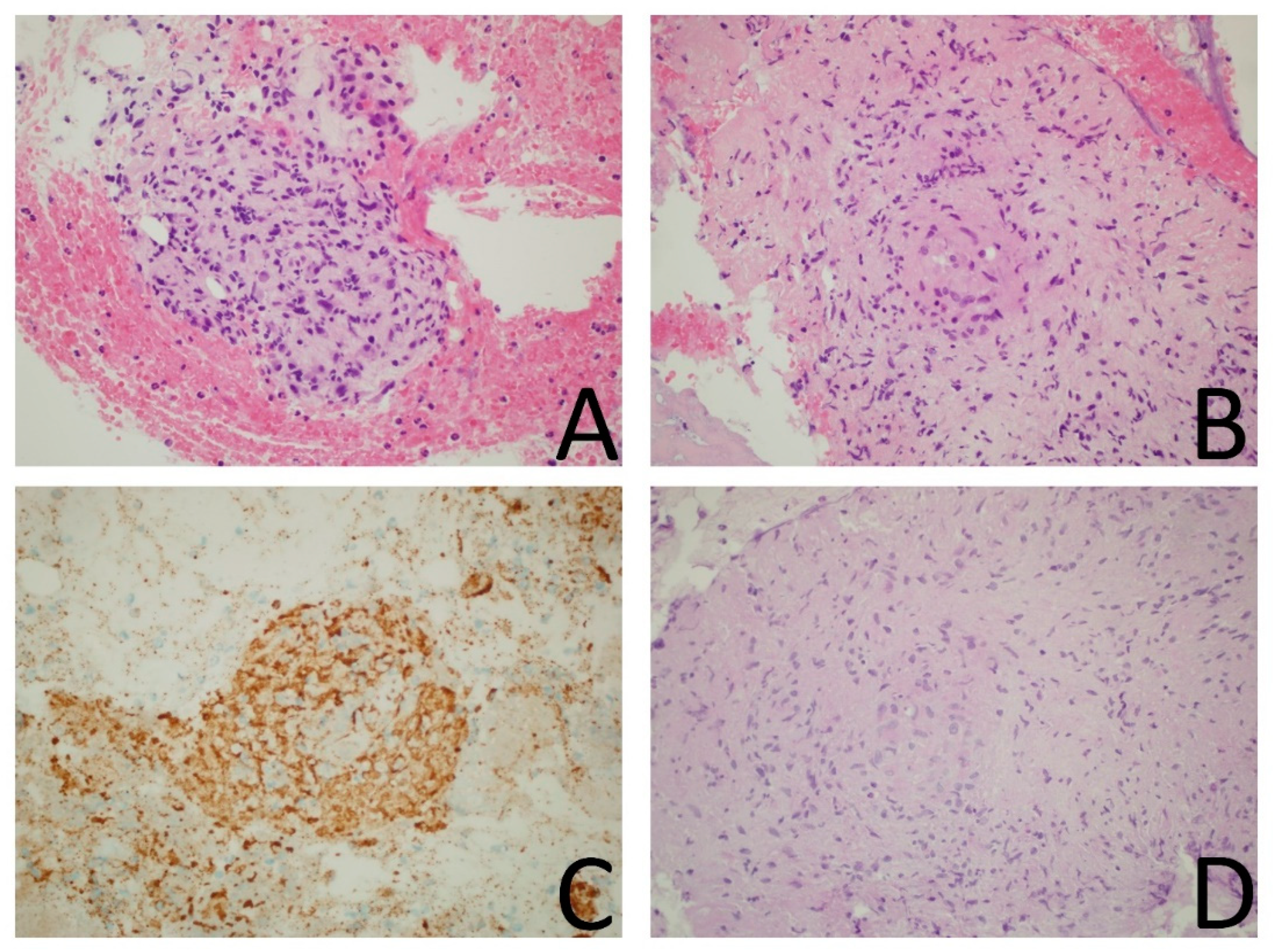
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Ethics Approval and Consent to Participate
References
- Phoon, P.H.Y.; Hwang, N.C. Deep Sternal Wound Infection: Diagnosis, Treatment and Prevention. J. Cardiothorac. Vasc. Anesth. 2020, 34, 1602–1613. [Google Scholar] [CrossRef] [PubMed]
- Yuan, S.M. Sternal wound tuberculosis following cardiac operations: A review. Rev. Bras. Cir. Cardiovasc. 2015, 30, 489–493. [Google Scholar] [CrossRef] [PubMed]
- Tabaja, H.; Hajar, Z.; Kanj, S.S. A review of eleven cases of tuberculosis presenting as sternal wound abscess after open heart surgery. Infect. Dis. 2017, 49, 721–727. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Giacobbe, D.R.; Bruzzi, P.; Barisione, E.; Centanni, S.; Castaldo, N.; Corcione, S.; De Rosa, F.G.; Di Marco, F.; Gori, A.; et al. Clinical Management of Adult Patients with COVID-19 outside Intensive Care Units: Guidelines from the Italian Society of Anti-Infective Therapy (SITA) and the Italian Society of Pulmonology (SIP). Infect. Dis. Ther. 2021, 10, 1837–1885. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, V.; Salmasi, Y.; Hunter, M.; Sidhu, P. Delayed diagnosis of chronic postoperative sternal infection: A rare case of sternal tuberculosis. BMJ Case Rep. 2018, 2018, bcr2017223650. [Google Scholar] [CrossRef] [PubMed]
- Malani, P.N.; McNeil, S.A.; Bradley, S.F.; Kauffman, C.A. Candida albicans Sternal Wound Infections: A Chronic and Recurrent Complication of Median Sternotomy. Clin. Infect. Dis. 2002, 35, 1316–1320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maroz, N. Impact of Renal Failure on Wounds Healing. J. Am. Coll. Clin. Wound Spec. 2018, 8, 12–13. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Tuberculosis Deaths Rise for the First Time in More Than a Decade due to the COVID-19 Pandemic. Available online: https://www.who.int/news/item/14-10-2021-tuberculosis-deaths-rise-for-the-first-time-in-more-than-a-decade-due-to-the-covid-19-pandemic (accessed on 14 January 2022).
- Musso, M.; Di Gennaro, F.; Gualano, G.; Mosti, S.; Cerva, C.; Fard, S.N.; Libertone, R.; Di Bari, V.; Cristofaro, M.; Tonnarini, R.; et al. Concurrent cavitary pulmonary tuberculosis and COVID-19 pneumonia with in vitro immune cell anergy. Infection 2021, 49, 1061–1064. [Google Scholar] [CrossRef] [PubMed]
- Petrone, L.; Petruccioli, E.; Vanini, V.; Cuzzi, G.; Gualano, G.; Vittozzi, P.; Nicastri, E.; Maffongelli, G.; Grifoni, A.; Sette, A.; et al. Coinfection of tuberculosis and COVID-19 limits the ability to in vitro respond to SARS-CoV-2. Int. J. Infect. Dis. 2021, 113 (Suppl. 1), S82–S87. [Google Scholar] [CrossRef] [PubMed]
- Tadolini, M.; Codecasa, L.R.; García-García, J.M.; Blanc, F.X.; Borisov, S.; Alffenaar, J.W.; Andréjak, C.; Bachez, P.; Bart, P.-A.; Belilovski, E.; et al. Active tuberculosis, sequelae and COVID-19 co-infection: First cohort of 49 cases. Eur. Respir. J. 2020, 56, 2001398. [Google Scholar] [CrossRef] [PubMed]
- Khayat, M.; Fan, H.; Vali, Y. COVID-19 promoting the development of active tuberculosis in a patient with latent tuberculosis infection: A case report. Respir. Med. Case Rep. 2021, 32, 101344. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parolari, G.; Sepulcri, C.; Salsano, A.; Giacobbe, D.R.; Marchese, A.; Barbieri, R.; Guadagno, A.; Spina, B.; Santini, F.; Bassetti, M. Mycobacterium tuberculosis Surgical Site Infection after Cardiac Surgery in the COVID-19 Era: A Case Report. Infect. Dis. Rep. 2022, 14, 101-105. https://doi.org/10.3390/idr14010013
Parolari G, Sepulcri C, Salsano A, Giacobbe DR, Marchese A, Barbieri R, Guadagno A, Spina B, Santini F, Bassetti M. Mycobacterium tuberculosis Surgical Site Infection after Cardiac Surgery in the COVID-19 Era: A Case Report. Infectious Disease Reports. 2022; 14(1):101-105. https://doi.org/10.3390/idr14010013
Chicago/Turabian StyleParolari, Giulia, Chiara Sepulcri, Antonio Salsano, Daniele Roberto Giacobbe, Anna Marchese, Ramona Barbieri, Antonio Guadagno, Bruno Spina, Francesco Santini, and Matteo Bassetti. 2022. "Mycobacterium tuberculosis Surgical Site Infection after Cardiac Surgery in the COVID-19 Era: A Case Report" Infectious Disease Reports 14, no. 1: 101-105. https://doi.org/10.3390/idr14010013
APA StyleParolari, G., Sepulcri, C., Salsano, A., Giacobbe, D. R., Marchese, A., Barbieri, R., Guadagno, A., Spina, B., Santini, F., & Bassetti, M. (2022). Mycobacterium tuberculosis Surgical Site Infection after Cardiac Surgery in the COVID-19 Era: A Case Report. Infectious Disease Reports, 14(1), 101-105. https://doi.org/10.3390/idr14010013